

Patients’ Perspectives on the Acceptability and Effectiveness of a Community Health Worker-Led Intervention to Increase Chronic Kidney Disease Knowledge and Screening among Underserved Latine Adults: The CARE 2.0 Study

 ,
,  , , , , , , ,
, , , , , , ,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Intervention Development
2.3. Training of CHWs
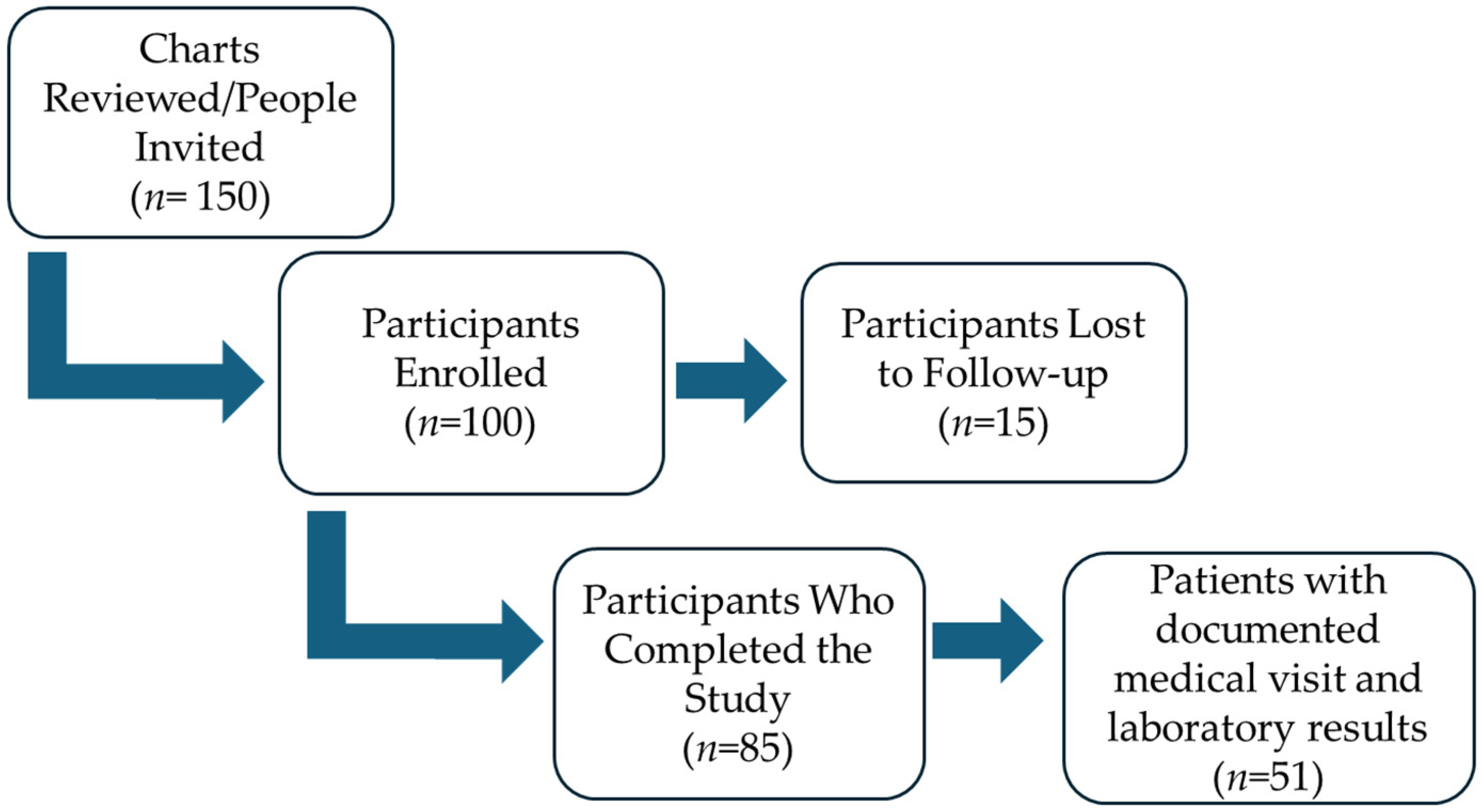
2.4. Recruitment of Patients
2.5. Assessment and Measurements of Acceptability and Effectiveness
2.6. Statistical Analysis
3. Results
3.1. CKD Knowledge Assessment
3.2. Gender Differences in the Impact of Educational Intervention and Risk Perception in Kidney Disease Knowledge
3.3. Patients’ Perspectives on the Acceptability of the CHW-Led Education
3.4. Predictive Capacity of Various Variables for a Patient’s Behavioral Intention to Seek Kidney-HealthCare
3.5. Biochemical Parameters Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention Centers for Disease Control and Prevention. In Chronic Kidney Disease Surveillance System—United States. Available online: https://www.cdc.gov/kidney-disease/php/data-research/index.html (accessed on 10 June 2023).
- Murphy, D.; McCulloch, C.E.; Lin, F.; Banerjee, T.; Bragg-Gresham, J.L.; Eberhardt, M.S.; Morgenstern, H.; Pavkov, M.E.; Saran, R.; Powe, N.R.; et al. Trends in Prevalence of Chronic Kidney Disease in the United States. Ann. Intern. Med. 2016, 165, 473. [Google Scholar] [CrossRef]
- Chu, C.D.; McCulloch, C.E.; Banerjee, T.; Pavkov, M.E.; Burrows, N.R.; Gillespie, B.W.; Saran, R.; Shlipak, M.G.; Powe, N.R.; Tuot, D.S.; et al. CKD Awareness among US Adults by Future Risk of Kidney Failure. Am. J. Kidney Dis. 2020, 76, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Shlipak, M.G.; Tummalapalli, S.L.; Boulware, L.E.; Grams, M.E.; Ix, J.H.; Jha, V.; Kengne, A.-P.; Madero, M.; Mihaylova, B.; Tangri, N.; et al. The Case for Early Identification and Intervention of Chronic Kidney Disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2021, 99, 34–47. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation Inc. Facts about Chronic Kidney Disease. Available online: https://www.kidney.org/atoz/content/about-chronic-kidney-disease (accessed on 23 May 2024).
- Vassalotti, J.; Diamantidis, C.J.; Cook, D.J. Shared Viewpoint—Developing the Future of Kidney Care. J. Gen. Intern. Med. 2022, 37, 947–948. [Google Scholar] [CrossRef] [PubMed]
- Yan, G.; Shen, J.I.; Harford, R.; Yu, W.; Nee, R.; Clark, M.J.; Flaque, J.; Colon, J.; Torre, F.; Rodriguez, Y.; et al. Racial and Ethnic Variations in Mortality Rates for Patients Undergoing Maintenance Dialysis Treated in US Territories Compared with the US 50 States. Clin. J. Am. Soc. Nephrol. 2020, 15, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Fischer, M.J.; Go, A.S.; Lora, C.M.; Ackerson, L.; Cohan, J.; Kusek, J.W.; Mercado, A.; Ojo, A.; Ricardo, A.C.; Rosen, L.K.; et al. CKD in Hispanics: Baseline Characteristics From the CRIC (Chronic Renal Insufficiency Cohort) and Hispanic-CRIC Studies. Am. J. Kidney Dis. 2011, 58, 214–227. [Google Scholar] [CrossRef]
- United States Renal Data System. 2022 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2022. [Google Scholar]
- Desai, N.; Lora, C.M.; Lash, J.P.; Ricardo, A.C. CKD and ESRD in US Hispanics. Am. J. Kidney Dis. 2019, 73, 102–111. [Google Scholar] [CrossRef]
- Norton, J.M.; Moxey-Mims, M.M.; Eggers, P.W.; Narva, A.S.; Star, R.A.; Kimmel, P.L.; Rodgers, G.P. Social Determinants of Racial Disparities in CKD. J. Am. Soc. Nephrol. 2016, 27, 2576–2595. [Google Scholar] [CrossRef]
- Nicholas, S.B.; Kalantar-Zadeh, K.; Norris, K.C. Socioeconomic Disparities in Chronic Kidney Disease. Adv. Chronic Kidney Dis. 2015, 22, 6–15. [Google Scholar] [CrossRef]
- Ortega, A.N.; McKenna, R.M.; Kemmick Pintor, J.; Langellier, B.A.; Roby, D.H.; Pourat, N.; Vargas Bustamante, A.; Wallace, S.P. Health Care Access and Physical and Behavioral Health Among Undocumented Latinos in California. Med. Care 2018, 56, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Ornelas, I.J.; Yamanis, T.J.; Ruiz, R.A. The Health of Undocumented Latinx Immigrants: What We Know and Future Directions. Annu. Rev. Public Health 2020, 41, 289–308. [Google Scholar] [CrossRef]
- Mitchell, T. Unauthorized Immigrant Population Trends for States, Birth Countries and Regions. Available online: https://www.pewresearch.org/race-and-ethnicity/feature/unauthorized-trends/ (accessed on 10 June 2024).
- Estrella, M.L.; Allen-Meares, P.; Ricardo, A.C.; Fischer, M.J.; Gordon, E.J.; Carmona-Powell, E.; Sondheimer, J.; Chen, J.; Horwitz, E.; Wang, X.; et al. Prospective Associations of Health Literacy with Clinical Outcomes in Adults with CKD: Findings from the CRIC Study. Nephrol. Dial. Transplant. 2023, 38, 904–912. [Google Scholar] [CrossRef] [PubMed]
- Lora, C.M.; Gordon, E.J.; Sharp, L.K.; Fischer, M.J.; Gerber, B.S.; Lash, J.P. Progression of CKD in Hispanics: Potential Roles of Health Literacy, Acculturation, and Social Support. Am. J. Kidney Dis. 2011, 58, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Lora, C.M.; Ricardo, A.C.; Chen, J.; Cai, J.; Flessner, M.; Moncrieft, A.; Peralta, C.; Raij, L.; Rosas, S.E.; Talavera, G.A.; et al. Acculturation and Chronic Kidney Disease in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Prev. Med. Rep. 2018, 10, 285–291. [Google Scholar] [CrossRef]
- Crews, D.C.; Kuczmarski, M.F.; Grubbs, V.; Hedgeman, E.; Shahinian, V.B.; Evans, M.K.; Zonderman, A.B.; Burrows, N.R.; Williams, D.E.; Saran, R.; et al. Effect of Food Insecurity on Chronic Kidney Disease in Lower-Income Americans. Am. J. Nephrol. 2014, 39, 27–35. [Google Scholar] [CrossRef]
- Billany, R.E.; Thopte, A.; Adenwalla, S.F.; March, D.S.; Burton, J.O.; Graham-Brown, M.P.M. Associations of Health Literacy with Self-Management Behaviours and Health Outcomes in Chronic Kidney Disease: A Systematic Review. J. Nephrol. 2023, 36, 1267–1281. [Google Scholar] [CrossRef]
- Boulware, L.E.; Carson, K.A.; Troll, M.U.; Powe, N.R.; Cooper, L.A. Perceived Susceptibility to Chronic Kidney Disease among High-Risk Patients Seen in Primary Care Practices. J. Gen. Intern. Med. 2009, 24, 1123–1129. [Google Scholar] [CrossRef]
- Cervantes, L.; Rizzolo, K.; Carr, A.L.; Steiner, J.F.; Chonchol, M.; Powe, N.; Cukor, D.; Hasnain-Wynia, R. Social and Cultural Challenges in Caring for Latinx Individuals With Kidney Failure in Urban Settings. JAMA Netw. Open 2021, 4, e2125838. [Google Scholar] [CrossRef]
- Narva, A.S.; Norton, J.M.; Boulware, L.E. Educating Patients about CKD. Clin. J. Am. Soc. Nephrol. 2016, 11, 694–703. [Google Scholar] [CrossRef]
- Stevens, P.E. Evaluation and Management of Chronic Kidney Disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline. Ann. Intern Med. 2013, 158, 825. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.-J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Kwong, Y.D.; Tuot, D.S. Optimizing Self-Management Programs in Kidney Disease: Implementation of Sick-Day Protocols. Kidney Med. 2022, 4, 100530. [Google Scholar] [CrossRef]
- Kidney Disease Outcomes Quality Initiative. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Diabetes and Chronic Kidney Disease. Am. J. Kidney Dis. 2007, 49, S12–S154. [Google Scholar] [CrossRef] [PubMed]
- Langham, R.G.; Kalantar-Zadeh, K.; Bonner, A.; Balducci, A.; Hsiao, L.L.; Kumaraswami, L.A.; Laffin, P.; Liakopoulos, V.; Saadi, G.; Tantisattamo, E.; et al. Kidney Health for All: Bridging the Gap in Kidney Health Education and Literacy. Clin. Kidney J. 2022, 55, 603–610. [Google Scholar] [CrossRef]
- Cervantes, L.; Robinson, B.M.; Steiner, J.F.; Myaskovsky, L. Culturally Concordant Community-Health Workers: Building Sustainable Community-Based Interventions That Eliminate Kidney Health Disparities. J. Am. Soc. Nephrol. 2022, 33, 1252–1254. [Google Scholar] [CrossRef] [PubMed]
- Kimmel, P.L.; Jefferson, N.; Norton, J.M.; Star, R.A. How Community Engagement Is Enhancing NIDDK Research. Clin. J. Am. Soc. Nephrol. 2019, 14, 768–770. [Google Scholar] [CrossRef]
- Payán, D.; Zawadzki, M.; Song, A. Advancing Community-Engaged Research to Promote Health Equity: Considerations to Improve the Field. Perspect. Public Health 2022, 142, 139–141. [Google Scholar] [CrossRef]
- O’Mara-Eves, A.; Brunton, G.; McDaid, D.; Oliver, S.; Kavanagh, J.; Jamal, F.; Matosevic, T.; Harden, A.; Thomas, J. Community Engagement to Reduce Inequalities in Health: A Systematic Review, Meta-Analysis and Economic Analysis. Public Health Res. 2013, 1, 1–526. [Google Scholar] [CrossRef]
- National Kidney Foundation Community Health Workers. Available online: https://www.kidney.org/NKF-Community-Health-Workers (accessed on 10 June 2024).
- Brownstein, J.N.; Chowdhury, F.M.; Norris, S.L.; Horsley, T.; Jack, L.; Zhang, X.; Satterfield, D. Effectiveness of Community Health Workers in the Care of People with Hypertension. Am. J. Prev. Med. 2007, 32, 435–447. [Google Scholar] [CrossRef]
- Spencer, M.S.; Kieffer, E.C.; Sinco, B.; Piatt, G.; Palmisano, G.; Hawkins, J.; Lebron, A.; Espitia, N.; Tang, T.; Funnell, M.; et al. Outcomes at 18 Months From a Community Health Worker and Peer Leader Diabetes Self-Management Program for Latino Adults. Diabetes Care 2018, 41, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Reininger, B.M.; Lopez, J.; Zolezzi, M.; Lee, M.; Mitchell-Bennett, L.A.; Xu, T.; Park, S.K.; Saldana, M.V.; Perez, L.; Payne, L.Y.; et al. Participant Engagement in a Community Health Worker-Delivered Intervention and Type 2 Diabetes Clinical Outcomes: A Quasiexperimental Study in MexicanAmericans. BMJ Open 2022, 12, e063521. [Google Scholar] [CrossRef] [PubMed]
- Fisher, T.L.; Burnet, D.L.; Huang, E.S.; Chin, M.H.; Cagney, K.A. Cultural Leverage. Med. Care Res. Rev. 2007, 64, 243S–282S. [Google Scholar] [CrossRef]
- Chang, A.; Patberg, E.; Cueto, V.; Li, H.; Singh, B.; Kenya, S.; Alonzo, Y.; Carrasquillo, O. Community Health Workers, Access to Care, and Service Utilization Among Florida Latinos: A Randomized Controlled Trial. Am. J. Public Health 2018, 108, 1249–1251. [Google Scholar] [CrossRef]
- Cass, A.; Cunningham, J.; Wang, Z.; Hoy, W. Regional Variation in the Incidence of End-stage Renal Disease in Indigenous Australians. Med. J. Aust. 2001, 175, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Yadav, A.K.; Sethi, J.; Ghosh, A.; Sahay, M.; Prasad, N.; Varughese, S.; Parameswaran, S.; Gopalakrishnan, N.; Kaur, P.; et al. The Indian Chronic Kidney Disease (ICKD) Study: Baseline Characteristics. Clin. Kidney J. 2022, 15, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.-M.; Yang, C.-W. Chronic Kidney Disease: Global Dimension and Perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Diaz-Martinez, J.; Kallus, L.; Levine, H.M.; Lavernia, F.; Pierre, A.J.; Mancilla, J.; Barthe, A.; Duran, C.; Kotzker, W.; Wagner, E.; et al. Community-Engaged Research (CEnR) to Address Gaps in Chronic Kidney Disease Education among Underserved Latines—The CARE Study. Int. J. Environ. Res. Public Health 2023, 20, 7026. [Google Scholar] [CrossRef]
- Cervantes, L.; Hasnain-Wynia, R.; Steiner, J.F.; Chonchol, M.; Fischer, S. Patient Navigation: Addressing Social Challenges in Dialysis Patients. Am. J. Kidney Dis. 2020, 76, 121–129. [Google Scholar] [CrossRef]
- Aponte, J.; Jackson, T.D.; Wyka, K.; Ikechi, C. Health Effectiveness of Community Health Workers as a Diabetes Self-Management Intervention. Diabetes Vasc. Dis. Res. 2017, 14, 316–326. [Google Scholar] [CrossRef]
- Haboush-Deloye, A.; Marquez, E.; Dunne, R.; Pharr, J.R. The Importance of Community Voice: Using Community-Based Participatory Research to Understand the Experiences of African American, Native American, and Latinx People during a Pandemic. Prev. Chronic Dis. 2023, 20, 220152. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.G.; Pankratz, V.S.; Ghahate, D.M.; Bobelu, J.; Faber, T.; Shah, V.O. Home-Based Kidney Care, Patient Activation, and Risk Factors for CKD Progression in Zuni Indians. Clin. J. Am. Soc. Nephrol. 2018, 13, 1801–1809. [Google Scholar] [CrossRef] [PubMed]
- Walton, J.W.; Snead, C.A.; Collinsworth, A.W.; Schmidt, K.L. Reducing Diabetes Disparities Through the Implementation of a Community Health Worker–Led Diabetes Self-Management Education Program. Fam. Community Health 2012, 35, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.; Oo, M.; Rojas, A.; Damian, A.J. Patients’ Perspectives on the Feasibility, Acceptability, and Impact of a Community Health Worker Program: A Qualitative Study. Health Equity 2021, 5, 160–168. [Google Scholar] [CrossRef]
- Sherman, M.; Covert, H.; Fox, L.; Lichtveld, M. Successes and Lessons Learned From Implementing Community Health Worker Programs in Community-Based and Clinical Settings: Insights From the Gulf Coast. J. Public Health Manag. Pract. 2017, 23, 85–93. [Google Scholar] [CrossRef]
- Lopez, P.M.; Islam, N.; Feinberg, A.; Myers, C.; Seidl, L.; Drackett, E.; Riley, L.; Mata, A.; Pinzon, J.; Benjamin, E.; et al. A Place-Based Community Health Worker Program: Feasibility and Early Outcomes, New York City, 2015. Am. J. Prev. Med. 2017, 52, S284–S289. [Google Scholar] [CrossRef]
- Emery, R.L.; Wimmer, M. Motivational Interviewing. In StatPearls; StatPearls Publishing LLC: Rockville, MD, USA, 2019; Volume 35, p. 21. [Google Scholar]
- Department of Health and Human Services (HHS). Federal Poverty Level (FPL); Department of Health and Human Services (HHS): Washington, DC, USA, 2024. [Google Scholar]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of Healthcare Interventions: An Overview of Reviews and Development of a Theoretical Framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Sanci, L.A.; Coffey, C.M.; Veit, F.C.; Carr-Gregg, M.; Patton, G.C.; Day, N.; Bowes, G. Evaluation of the Effectiveness of an Educational Intervention for General Practitioners in Adolescent Health Care: Randomised Controlled Trial. BMJ 2000, 320, 224–230. [Google Scholar] [CrossRef]
- Johnson, A.M.; Brimhall, A.S.; Johnson, E.T.; Hodgson, J.; Didericksen, K.; Pye, J.; Harmon, G.J.C.; Sewell, K.B. A Systematic Review of the Effectiveness of Patient Education through Patient Portals. JAMIA Open 2023, 6, ooac085. [Google Scholar] [CrossRef]
- Rosenthal, G.E.; Shannon, S.E. The Use of Patient Perceptions in the Evaluation of Health-Care Delivery Systems. Med. Care 1997, 35, NS58–NS68. [Google Scholar] [CrossRef]
- Edmonston, D.; Lydon, E.; Mulder, H.; Chiswell, K.; Lampron, Z.; Marsolo, K.; Goss, A.; Ayoub, I.; Shah, R.C.; Chang, A.R.; et al. Concordance With Screening and Treatment Guidelines for Chronic Kidney Disease in Type 2 Diabetes. JAMA Netw. Open 2024, 7, e2418808. [Google Scholar] [CrossRef]
- Schrauben, S.J.; Cavanaugh, K.L.; Fagerlin, A.; Ikizler, T.A.; Ricardo, A.C.; Eneanya, N.D.; Nunes, J.W. The Relationship of Disease-Specific Knowledge and Health Literacy With the Uptake of Self-Care Behaviors in CKD. Kidney Int. Rep. 2020, 5, 48–57. [Google Scholar] [CrossRef]
- Dudley, W.N.; Benuzillo, J.G.; Carrico, M.S. SPSS and SAS Programming for the Testing of Mediation Models. Nurs. Res. 2004, 53, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Rust, G.; Baltrus, P.; Ye, J.; Daniels, E.; Quarshie, A.; Boumbulian, P.; Strothers, H. Presence of a Community Health Center and Uninsured Emergency Department Visit Rates in Rural Counties. J. Rural. Health 2009, 25, 8–16. [Google Scholar] [CrossRef]
- United States Renal Data System. 2020 USRDS Annual Data Report; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2020. [Google Scholar]
- Szczech, L.A.; Stewart, R.C.; Su, H.-L.; DeLoskey, R.J.; Astor, B.C.; Fox, C.H.; McCullough, P.A.; Vassalotti, J.A. Primary Care Detection of Chronic Kidney Disease in Adults with Type-2 Diabetes: The ADD-CKD Study (Awareness, Detection and Drug Therapy in Type 2 Diabetes and Chronic Kidney Disease). PLoS ONE 2014, 9, e110535. [Google Scholar] [CrossRef] [PubMed]
- Afkarian, M.; Zelnick, L.R.; Hall, Y.N.; Heagerty, P.J.; Tuttle, K.; Weiss, N.S.; de Boer, I.H. Clinical Manifestations of Kidney Disease Among US Adults with Diabetes, 1988–2014. JAMA 2016, 316, 602–610. [Google Scholar] [CrossRef]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global Aetiology and Epidemiology of Type 2 Diabetes Mellitus and Its Complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Blewett, L.A.; Owen, R.A. Accountable Care for the Poor and Underserved: Minnesota’s Hennepin Health Model. Am. J. Public Health 2015, 105, 622–624. [Google Scholar] [CrossRef]
- Brown, L.D.; Vasquez, D.; Salinas, J.J.; Tang, X.; Balcázar, H. Evaluation of Healthy Fit: A Community Health Worker Model to Address Hispanic Health Disparities. Prev. Chronic Dis. 2018, 15, 170347. [Google Scholar] [CrossRef]
- Turner, B.J.; Liang, Y.; Ramachandran, A.; Poursani, R. Telephone or Visit-Based Community Health Worker Care Management for Uncontrolled Diabetes Mellitus: A Longitudinal Study. J. Community Health 2020, 45, 1123–1131. [Google Scholar] [CrossRef]
- Krantz, M.J.; Coronel, S.M.; Whitley, E.M.; Dale, R.; Yost, J.; Estacio, R.O. Effectiveness of a Community Health Worker Cardiovascular Risk Reduction Program in Public Health and Health Care Settings. Am. J. Public Health 2013, 103, e19–e27. [Google Scholar] [CrossRef]
- Lahman, M.; Mendoza, B.; Rodriguez, K.; Schwartz, J. Undocumented Research Participants: Ethics and Protection in a Time of Fear. Hisp. J. Behav. Sci. 2011, 33, 304–322. [Google Scholar] [CrossRef]
- Hernández, M.G.; Nguyen, J.; Casanova, S.; Suárez-Orozco, C.; Saetermoe, C.L. Doing No Harm and Getting It Right: Guidelines for Ethical Research with Immigrant Communities. New Dir. Child Adolesc. Dev. 2013, 2013, 43–60. [Google Scholar] [CrossRef]
- Bachmeier, J.D.; Van Hook, J.; Bean, F.D. Can We Measure Immigrants’ Legal Status? Lessons from Two U.S. Surveys. Int. Migr. Rev. 2014, 48, 538–566. [Google Scholar] [CrossRef]
- Lekas, H.-M.; Pahl, K.; Fuller Lewis, C. Rethinking Cultural Competence: Shifting to Cultural Humility. Health Serv. Insights 2020, 13, 1178632920970580. [Google Scholar] [CrossRef]

{kind=link}
| Covariate | All (n = 100) |
|---|---|
| Age (years)–Mean (SD) | 55.6 ± 10.5 |
| Female | 68.0% |
| Obesity | 33.9% |
| Country of Origin | |
| 43.0% |
| 19% |
| 9.0% |
| 5.0% |
| 4.0% |
| 4.0% |
| 16.0% |
| Former smoker | 19% |
| Alcohol use | |
| 82.0% |
| 16.0% |
| 1.0% |
| 1.0% |
| Medical Diagnosis | |
| 27.0% |
| 75.0% |
| 82.0% |
| 52.0% |
| 9.0% |
| 10.0% |
| 13.0% |
| 5.0% |
| 9.0% |
| 36.0% |
| Literate | 90.0% |
| Semi-literate | 10% |
| Home | |
| 43.0% |
| 26.0% |
| 22.0% |
| 1.0% |
| 8.0% |
| Household members–Mean (SD) | 2.0 ± 1.1 |
| Education | |
| 8.0% |
| 73.0% |
| 6.0% |
| 13.0% |
| Unemployed | 53.0% |
| Income/year–Mean (SD) | $17,993.2 ± $9955.4 |
| Knowledge about the Topic of: | Nothing/Little | A Lot | OR ** | IC95% | p *** | ||
|---|---|---|---|---|---|---|---|
| Kidney Functions | Before | 79.0% | 21.0% | 25.2 | 11.8 | 53.6 | <0.001 |
| After | 12.0% | 88.0% | |||||
| What is Kidney Disease | Before | 79.0% | 21.0% | 25.2 | 11.8 | 53.6 | <0.001 |
| After | 13.0% | 87.0% | |||||
| Who is at Risk | Before | 64.0% | 36.0% | 23.6 | 9.9 | 56.4 | <0.001 |
| After | 7.0% | 93.0% | |||||
| Tests for Kidney Function | Before | 84.0% | 16.0% | 29.7 | 13.8 | 64.0 | <0.001 |
| After | 15.0% | 85.0% | |||||
| Progression/Visit Nephrologist | Before | 87.0% | 13.0% | 32.6 | 14.9 | 71.4 | <0.001 |
| After | 17.0% | 83.0% | |||||
| Diet and Kidney Disease | Before | 84.0% | 16.0% | 29.7 | 13.8 | 64.0 | <0.001 |
| After | 15.0% | 85.0% | |||||
| Therapeutic Goals to Protect Kidneys * | Before | 77.0% | 23.0% | 17.6 | 8.6 | 35.7 | <0.001 |
| After | 16.0% | 84.0% | |||||
| Medicines for Kidney and Heart | Before | 91.0% | 9.0% | 27.3 | 12.1 | 61.7 | <0.001 |
| After | 27.0% | 73.0% | |||||
| Therapies available if Kidney Function Worsens | Before | 83.0% | 17.0% | 20.814 | 10.1 | 42.9 | <0.001 |
| After | 19.0% | 81.0% | |||||
| Median | Q1 | Q3 | |
|---|---|---|---|
| 1. How useful did you find the education about kidney disease? * | 4 | 4 | 5 |
| 2. I learned new things about kidney disease ** | 5 | 4 | 5 |
| 3. The CHWs were well-informed and friendly ** | 5 | 5 | 5 |
| 4. I felt comfortable discussing my concerns about kidney disease ** | 5 | 5 | 5 |
| 5. The words and vocabulary used in the flipchart were easy for me to understand ** | 5 | 5 | 5 |
| 6. The images/photos used in the flipchart helped me understand kidney disease ** | 5 | 5 | 5 |
| 7. Overall, I was satisfied with the support and guidance provided during the education ** | 5 | 5 | 5 |
| 8. The education received will help me with my kidney health and making lifestyle changes ** | 5 | 5 | 5 |
| 9. I will recommend this education to others ** | 5 | 5 | 5 |
| Variable | Before | After | p * | Change | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | Q1 | Q3 | Median | Q1 | Q3 | Median | Q1 | Q3 | ||
| Glycemia | 151.0 | 118.5 | 201.8 | 130.0 | 109.0 | 167.0 | 0.014 | −18.0 | −52.3 | 7.3 |
| HbA1c | 7.4 | 6.5 | 8.1 | 7.4 | 6.8 | 8.5 | 0.509 | 0.2 | −0.7 | 0.9 |
| Chol-LDL | 75.0 | 56.0 | 113.0 | 71.0 | 48.0 | 104.0 | 0.284 | −2.0 | −31.0 | 13.0 |
| Chol-HDL | 47.0 | 40.0 | 55.0 | 47.0 | 38.0 | 53.0 | 0.791 | 0.0 | −4.0 | 4.0 |
| Trig. | 149.0 | 109.0 | 201.5 | 140.0 | 107.0 | 211.0 | 0.035 | −29.0 | −85.8 | 30.5 |
| eGFR | 94.0 | 65.3 | 107.0 | 85.0 | 60.5 | 103.5 | 0.942 | 0.0 | −6.0 | 5.0 |
| uACR | 22.0 | 9.3 | 97.0 | 30.0 | 12.3 | 217.3 | 0.638 | −2.0 | −23.0 | 66.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz-Martinez, J.; Delgado-Enciso, I.; Duran, C.; Kallus, L.; Jean-Pierre, A.; Lopez, B.; Mancilla, J.; Madruga, Y.; Hernandez-Fuentes, G.A.; Kotzker, W.; et al. Patients’ Perspectives on the Acceptability and Effectiveness of a Community Health Worker-Led Intervention to Increase Chronic Kidney Disease Knowledge and Screening among Underserved Latine Adults: The CARE 2.0 Study. Behav. Sci. 2024, 14, 750. https://doi.org/10.3390/bs14090750
Diaz-Martinez J, Delgado-Enciso I, Duran C, Kallus L, Jean-Pierre A, Lopez B, Mancilla J, Madruga Y, Hernandez-Fuentes GA, Kotzker W, et al. Patients’ Perspectives on the Acceptability and Effectiveness of a Community Health Worker-Led Intervention to Increase Chronic Kidney Disease Knowledge and Screening among Underserved Latine Adults: The CARE 2.0 Study. Behavioral Sciences. 2024; 14(9):750. https://doi.org/10.3390/bs14090750
Chicago/Turabian StyleDiaz-Martinez, Janet, Ivan Delgado-Enciso, Carlos Duran, Laura Kallus, Aydeivis Jean-Pierre, Brenda Lopez, Jessica Mancilla, Yoel Madruga, Gustavo A. Hernandez-Fuentes, Wayne Kotzker, and et al. 2024. "Patients’ Perspectives on the Acceptability and Effectiveness of a Community Health Worker-Led Intervention to Increase Chronic Kidney Disease Knowledge and Screening among Underserved Latine Adults: The CARE 2.0 Study" Behavioral Sciences 14, no. 9: 750. https://doi.org/10.3390/bs14090750
APA StyleDiaz-Martinez, J., Delgado-Enciso, I., Duran, C., Kallus, L., Jean-Pierre, A., Lopez, B., Mancilla, J., Madruga, Y., Hernandez-Fuentes, G. A., Kotzker, W., Delgado-Enciso, O., Wagner, E., & Hospital, M. (2024). Patients’ Perspectives on the Acceptability and Effectiveness of a Community Health Worker-Led Intervention to Increase Chronic Kidney Disease Knowledge and Screening among Underserved Latine Adults: The CARE 2.0 Study. Behavioral Sciences, 14(9), 750. https://doi.org/10.3390/bs14090750