
The Association between Cesarean Section Delivery and Child Behavior: Is It Mediated by Maternal Post-Traumatic Stress Disorder and Maternal Postpartum Depression?

 , ,
, , 
Abstract
1. Introduction
1.1. Background
1.1.1. Child Behavior
1.1.2. C-Section and Child Behavior
1.1.3. C-Section as Predictor of Maternal PPD and PTSD
1.1.4. Other Predictors of Children’s Behavioral Problems
2. Materials and Methods
2.1. Study Design and Sample
2.2. Measures
2.2.1. Predictor: Delivery Type
2.2.2. Outcome: Child Internalizing and Externalizing
2.2.3. Mediator: Maternal Postpartum Depressive Symptoms and Maternal PTSD
2.2.4. Covariates
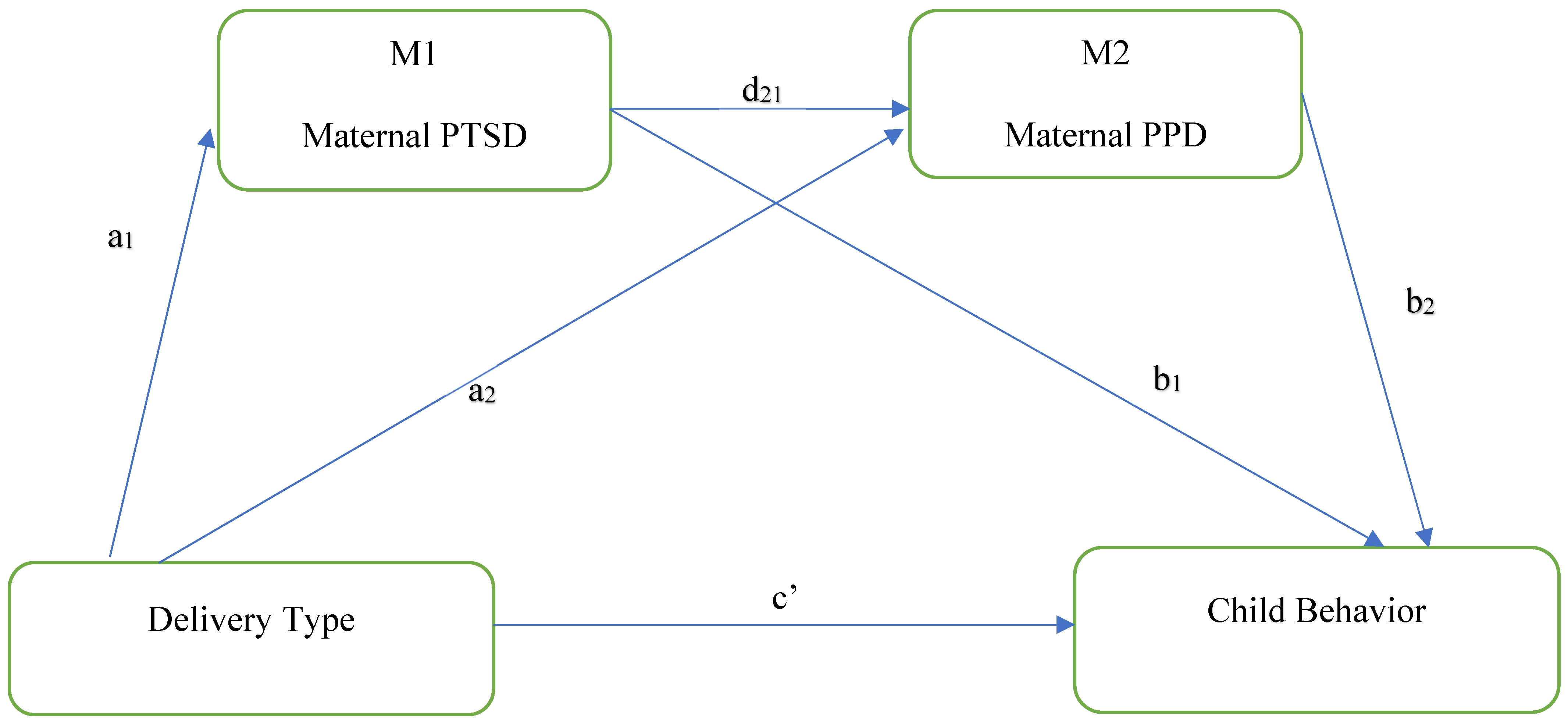
2.3. Data Analysis
3. Results
3.1. Descriptive Findings
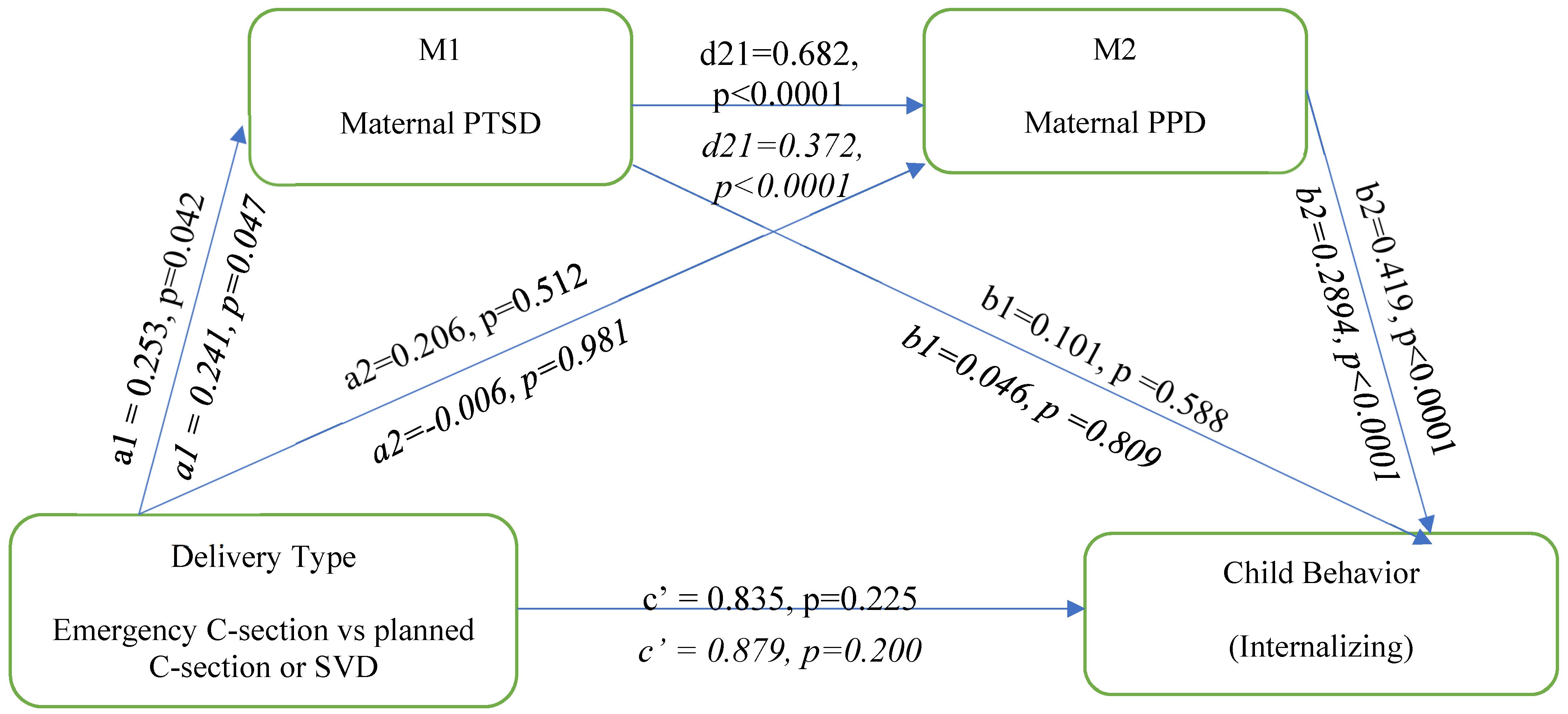
3.2. Internalizing Behaviors
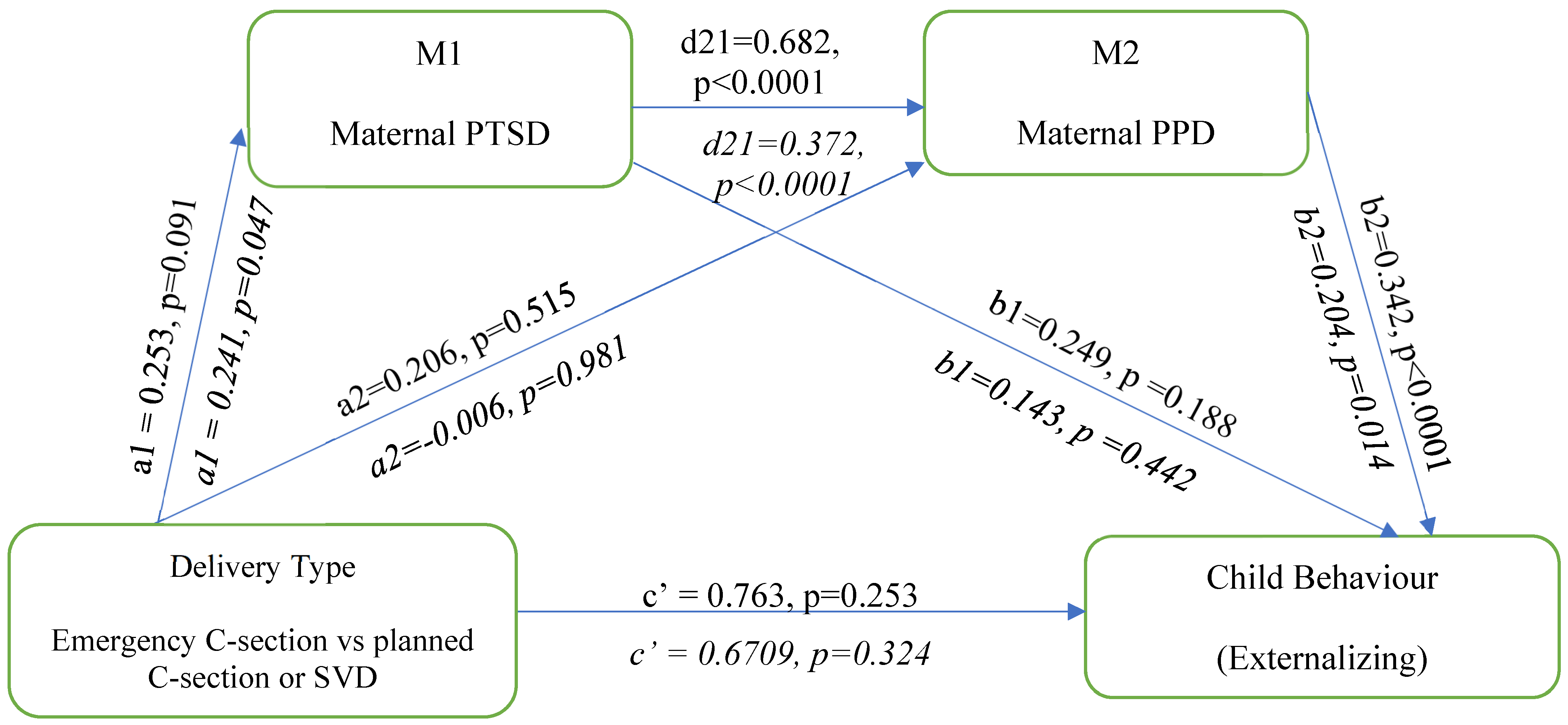
3.3. Externalizing Behaviors
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Betran, A.P.; Ye, J.; Moller, A.B.; Souza, J.P.; Zhang, J. Trends and projections of caesarean section rates: Global and regional estimates. BMJ Glob. Health 2021, 6, e005671. [Google Scholar] [CrossRef] [PubMed]
- Caughey, A.B.; Cahill, A.G.; Guise, J.M.; Rouse, D.J. Safe prevention of the primary cesarean delivery. Am. J. Obstet. Gynecol. 2014, 210, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Rutayisire, E.; Wu, X.; Huang, K.; Tao, S.; Chen, Y.; Tao, F. Childhood emotional and behavior problems and their associations with cesarean delivery. Rev. Bras. Psiquiatr. 2018, 40, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Sirvinskiene, G.; Zemaitiene, N.; Jusiene, R.; Markuniene, E. Predictors of emotional and behavioral problems in 1-year-old children: A longitudial perspective. Infant Ment. Health J. 2016, 37, 401–410. [Google Scholar] [CrossRef]
- Stein, A.; Pearson, R.M.; Goodman, S.H.; Rapa, E.; Rahman, A.; McCallum, M.; Howard, L.M.; Pariante, C.M. Effects of perinatal mental disorders on the fetus and child. Lancet 2014, 384, 1800–1819. [Google Scholar] [CrossRef]
- Liu, X.; Wang, S.; Wang, G. Prevalence and Risk Factors of Postpartum Depression in Women: A Systematic Review and Meta-analysis. J. Clin. Nurs. 2022, 31, 2665–2677. [Google Scholar] [CrossRef]
- Carter, F.; Frampton, C.; Mulder, R. Cesarean section and postpartum depression: A review of the evidence examining the link. Psychosom. Med. 2006, 68, 321–330. [Google Scholar] [CrossRef]
- Chang, S.-R.; Chen, K.-H.; Ho, H.-N.; Lai, Y.-H.; Lin, M.-I.; Lee, C.-N.; Lin, W.-A. Depressive symptoms, pain, and sexual dysfunction over the first year following vaginal or cesarean delivery: A prospective longitudinal study. Int. J. Nurs. Stud. 2015, 52, 1433–1444. [Google Scholar] [CrossRef]
- Meltzer-Brody, S.; Maegbaek, M.L.; Medland, S.E.; Miller, W.C.; Sullivan, P.; Munk-Olsen, T. Obstetrical, pregnancy and socio-economic predictors for new-onset severe postpartum psychiatric disorders in primiparous women. Psychol. Med. 2017, 47, 1427–1441. [Google Scholar] [CrossRef]
- Verreault, N.; Da Costa, D.; Marchand, A.; Ireland, K.; Banack, H.; Dritsa, M.; Khalife, S. PTSD following childbirth: A prospective study of incidence and risk factors in Canadian women. J. Psychosom. Res. 2012, 73, 257–263. [Google Scholar] [CrossRef]
- White, T.; Matthey, S.; Boyd, K.; Barnett, B. Postnatal depression and post-traumatic stress after childbirth: Prevalence, course and co-occurrence. J. Reprod. Infant Psychol. 2006, 24, 107–120. [Google Scholar] [CrossRef]
- Grisbrook, M.A.; Dewey, D.; Cuthbert, C.; McDonald, S.; Ntanda, H.; Giesbrecht, G.F.; Letourneau, N. Associations among Caesarean Section Birth, Post-Traumatic Stress, and Postpartum Depression Symptoms. Int. J. Environ. Res. Public Health 2022, 19, 4900. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.; Grant, S.; Morlock, L. The teacher-student relationship as a developmental context for children with internalizing or externalizing behavior problems. Sch. Psychol. Q 2008, 23, 3–15. [Google Scholar] [CrossRef]
- Breslau, J.; Miller, E.; Breslau, N.; Bohnert, K.; Lucia, V.; Schweitzer, J. The impact of early behavior disturbances on academic achievement in high school. Pediatrics 2009, 123, 1472–1476. [Google Scholar] [CrossRef] [PubMed]
- Solem, M.; Christophersen, K.; Martinussen, M. Predicting parenting stress: Children’s behavioural problems and parents’ coping. Infant Child Dev. 2011, 20, 162–180. [Google Scholar] [CrossRef]
- Canadian Paediatric Society. Child and Youth Mental Health. Available online: https://cps.ca/en/strategic-priorities/child-and-youth-mental-health#:~:text=Twenty%20per%20cent%20of%20Canadian,and%20timely%20care%20when%20needed (accessed on 15 December 2023).
- Ghandour, R.M.; Sherman, L.J.; Vladutiu, C.J.; Ali, M.M.; Lynch, S.E.; Bitsko, R.H.; Blumberg, S.J. Prevalence and Treatment of Depression, Anxiety, and Conduct Problems in US Children. J. Pediatr. 2019, 206, 256–267.e253. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Amminger, G.P.; Aguilar-Gaxiola, S.; Alonso, J.; Lee, S.; Ustün, T.B. Age of onset of mental disorders: A review of recent literature. Curr. Opin. Psychiatry 2007, 20, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Canadian Institute of Health Information. Care for Children and Youth With Mental Disorders: Data Table. Available online: https://www.cihi.ca/en/search?query-all=children+and+youth+mental+health&Search+Submit= (accessed on 10 April 2023).
- Hoffmann, J.; Stack, A.; Samnaliev, M.; Monuteaux, M.; Lee, L. Trends in visits and costs of mental health emergencies in a pediatric emergency department: 2010–2016. Acad. Pediatr. 2019, 19, 386–393. [Google Scholar] [CrossRef]
- Jasiulione, J.; Jusiene, R. Delivery mode, maternal characteristics, and developmental trajectories of toddlers’ emotional and behavioral problems. Child Youth Care Forum 2019, 48, 405–425. [Google Scholar] [CrossRef]
- Li, H.T.; Ye, R.; Achenbach, T.M.; Ren, A.; Pei, L.; Zheng, X.; Liu, J.M. Caesarean delivery on maternal request and childhood psychopathology: A retrospective cohort study in China. BJOG 2011, 118, 42–48. [Google Scholar] [CrossRef]
- Al Khalaf, S.Y.; O’Neill, S.M.; O’Keeffe, L.M.; Henriksen, T.B.; Kenny, L.C.; Cryan, J.F.; Khashan, A.S. The impact of obstetric mode of delivery on childhood behavior. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1557–1567. [Google Scholar] [CrossRef]
- Lobel, M.; DeLuca, R.S. Psychosocial sequelae of cesarean delivery: Review and analysis of their causes and implications. Soc. Sci. Med. 2007, 64, 2272–2284. [Google Scholar] [CrossRef] [PubMed]
- Clout, D.; Brown, R. Sociodemographic, pregnancy, obstetric, and postnatal predictors of postpartum stress, anxiety and depression in new mothers. J. Affect. Disord. 2015, 188, 60–67. [Google Scholar] [CrossRef]
- Hanlon, A.; Beckmann, M. Mode of birth and early postnatal psychological morbidity. Aust. N. Z. J. Obstet. Gynaecol. 2015, 55, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Rauh, C.; Beetz, A.; Burger, P.; Engel, A.; Haberle, L.; Fasching, P.A.; Kornhuber, J.; Beckmann, M.W.; Goecke, T.W.; Faschingbauer, F. Delivery mode and the course of pre- and postpartum depression. Arch. Gynecol. Obstet. 2012, 286, 1407–1412. [Google Scholar] [CrossRef]
- Youn, H.; Lee, S.; Han, S.W.; Kim, L.Y.; Lee, T.S.; Oh, M.J.; Jeong, H.G.; Cho, G.J. Obstetric risk factors for depression during the postpartum period in South Korea: A nationwide study. J. Psychosom. Res. 2017, 102, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Waldenstrom, U.; Schytt, E. A longitudinal study of women’s memory of labour pain--from 2 months to 5 years after the birth. BJOG 2009, 116, 577–583. [Google Scholar] [CrossRef]
- Bell, A.; Andersson, E. The birth experience and women’s postnatal depression: A systematic review. Midwifery 2016, 39, 112–123. [Google Scholar] [CrossRef]
- Goecke, T.W.; Voigt, F.; Faschingbauer, F.; Spangler, G.; Beckmann, M.W.; Beetz, A. The association of prenatal attachment and perinatal factors with pre- and postpartum depression in first-time mothers. Arch. Gynecol. Obstet. 2012, 286, 309–316. [Google Scholar] [CrossRef]
- Sword, W.; Landy, C.K.; Thabane, L.; Watt, S.; Krueger, P.; Farine, D.; Foster, G. Is mode of delivery associated with postpartum depression at 6 weeks: A prospective cohort study. BJOG 2011, 118, 966–977. [Google Scholar] [CrossRef]
- Elmir, R.; Schmied, V.; Wilkes, L.; Jackson, D. Women’s perceptions and experiences of a traumatic birth: A meta-ethnography. J. Adv. Nurs. 2010, 66, 2142–2153. [Google Scholar] [CrossRef]
- Soderquist, J.; Wijma, B.; Wijma, K. The longitudinal course of post-traumatic stress after childbirth. J. Psychosom. Obstet. Gynaecol. 2006, 27, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Beck, C.; Gable, R.; Sakala, C.; Declercq, E. Posttraumatic stress disorder in new mothers: Results from a two-stage U.S. national survey. Birth 2011, 38, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Quarini, C.; Pearson, R.M.; Stein, A.; Ramchandani, P.G.; Lewis, G.; Evans, J. Are female children more vulnerable to the long-term effects of maternal depression during pregnancy? J. Affect. Disord. 2016, 189, 329–335. [Google Scholar] [CrossRef]
- Kaplan, B.J.; Giesbrecht, G.F.; Leung, B.M.; Field, C.J.; Dewey, D.; Bell, R.C.; Manca, D.P.; O’Beirne, M.; Johnston, D.W.; Pop, V.J.; et al. The Alberta Pregnancy Outcomes and Nutrition (APrON) cohort study: Rationale and methods. Matern. Child Nutr. 2014, 10, 44–60. [Google Scholar] [CrossRef]
- Letourneau, N.; Aghajafari, F.; Bell, R.C.; Deane, A.J.; Dewey, D.; Field, C.; Giesbrecht, G.; Kaplan, B.; Leung, B.; Ntanda, H. The Alberta Pregnancy Outcomes and Nutrition (APrON) longitudinal study: Cohort profile and key findings from the first three years. BMJ Open 2022, 12, e047503. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Preschool Forms & Profiles; Research Center for Children, Youth, and Families: Burlington, VT, USA; University of Vermont: Burlington, VT, USA, 2000. [Google Scholar]
- Kristensen, S.; Henriksen, T.B.; Bilenberg, N. The Child Behavior Checklist for Ages 1.5-5 (CBCL/1(1/2)-5): Assessment and analysis of parent- and caregiver-reported problems in a population-based sample of Danish preschool children. Nord. J. Psychiatry 2010, 64, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.; Holden, J.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Cox, J.; Holden, J.; Henshaw, C. Perinatal Mental Health: The Edinburgh Postnatal Depression Scale (EPDS) Manual; RCPsych Publications: London, UK, 2014. [Google Scholar]
- Murray, D.; Cox, J. Screening for depression during pregnancy with the edinburgh depression scale. J. Reprod. Infant Psychol. 1990, 8, 99–107. [Google Scholar] [CrossRef]
- Leung, B.; Letourneau, N.; Bright, K.; Giesbrecht, G.; Ntanda, H.; Gagnon, L. Appraisal of the psychiatric diagnostic screening questionnaire in a perinatal cohort: The APrON study. Scand. J. Public Health 2017, 45, 658–665. [Google Scholar] [CrossRef]
- Üstündağ Budak, A.M.; Harris, G.; Blissett, J. Perinatal trauma with and without loss experiences. J. Reprod. Infant Psychol. 2016, 34, 413–425. [Google Scholar] [CrossRef]
- Zimmerman, M.; Mattia, J. The Psychiatric Diagnostic Screening Questionnaire: Development, reliability and validity. Compr. Psychiatry 2001, 42, 175–189. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. National Population Health Survey: Household Component. Available online: https://www23.statcan.gc.ca/imdb-bmdi/pub/document/3225_D10_T9_V3-eng.pdf (accessed on 26 April 2023).
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Maher, G.M.; Khashan, A.S.; McCarthy, F.P. Obstetrical mode of delivery and behavioural outcomes in childhood and adolescence: Findings from the Millennium Cohort Study. Soc. Psychiatry Psychiatr. Epidemiol. 2022, 57, 1697–1709. [Google Scholar] [CrossRef] [PubMed]
- Curran, E.A.; Khashan, A.S.; Dalman, C.; Kenny, L.C.; Cryan, J.F.; Dinan, T.G.; Kearney, P.M. Obstetric mode of delivery and attention-deficit/hyperactivity disorder: A sibling-matched study. Int. J. Epidemiol. 2016, 45, 532–542. [Google Scholar] [CrossRef] [PubMed]
- Dachew, B.A.; Tessema, G.A.; Alati, R. Association between obstetric mode of delivery and emotional and behavioural problems in children and adolescents: The children of the 90s health study. Soc. Psychiatry Psychiatr. Epidemiol. 2022, 58, 949–960. [Google Scholar] [CrossRef]
- Robson, S.J.; Vally, H.; Abdel-Latif, M.E.; Yu, M.; Westrupp, E. Childhood Health and Developmental Outcomes After Cesarean Birth in an Australian Cohort. Pediatrics 2015, 136, e1285–e1293. [Google Scholar] [CrossRef] [PubMed]
- Takács, L.; Putnam, S.P.; Monk, C.; Dahlen, H.G.; Thornton, C.; Bartoš, F.; Topalidou, A.; Peters, L.L. Associations Between Mode of Birth and Neuropsychological Development in Children Aged 4 Years: Results from a Birth Cohort Study. Child Psychiatry Hum. Dev. 2021, 52, 1094–1105. [Google Scholar] [CrossRef]
- Beck, C. Birth Trauma: In the Eye of the Beholder. Nurs. Res. 2004, 53, 28–35. [Google Scholar] [CrossRef]
- Seng, J.S.; Sperlich, M.; Low, L.K.; Ronis, D.L.; Muzik, M.; Liberzon, I. Childhood abuse history, posttraumatic stress disorder, postpartum mental health, and bonding: A prospective cohort study. J. Midwifery Women’s Health 2013, 58, 57–68. [Google Scholar] [CrossRef]
- Bagner, D.M.; Pettit, J.W.; Lewinsohn, P.M.; Seeley, J.R. Effect of maternal depression on child behavior: A sensitive period? J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Carter, A.; Garrity-Rokous, F.; Chazan-Cohen, R.; Little, C.; Briggs-Gowan, M. Maternal depression and comorbidity: Predicting early parenting, attachment security, and toddler social-emotional problems and competencies. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Letourneau, N.; Dennis, C.; Benzies, K.; Duffett-Leger, L.; Stewart, M.; Tryphonopoulos, P.; Este, D.; Watson, W. Postpartum depression is a family affair: Addressing the impact on mothers, fathers, and children. Issues Ment. Health Nurs. 2012, 33, 445–457. [Google Scholar] [CrossRef]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.Y.; Bruyere, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Womens Health 2019, 15, 1745506519844044. [Google Scholar] [CrossRef]
- Hernández-Martínez, A.; Rodríguez-Almagro, J.; Molina-Alarcón, M.; Infante-Torres, N.; Donate Manzanares, M.; Martínez-Galiano, J.M. Postpartum post-traumatic stress disorder: Associated perinatal factors and quality of life. J. Affect. Disord. 2019, 249, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Dikmen-Yildiz, P.; Ayers, S.; Phillips, L. Longitudinal trajectories of post-traumatic stress disorder (PTSD) after birth and associated risk factors. J. Affect. Disord. 2018, 229, 377–385. [Google Scholar] [CrossRef]
- Gluska, H.; Shiffman, N.; Mayer, Y.; Margalit, S.; Daher, R.; Elyasyan, L.; Sharon Weiner, M.; Miremberg, H.; Kovo, M.; Biron-Shental, T.; et al. Postpartum Depression in COVID-19 Days: Longitudinal Study of Risk and Protective Factors. J. Clin. Med. 2022, 11, 3488. [Google Scholar] [CrossRef]
- O’Connor, E.; Rossom, R.C.; Henninger, M.; Groom, H.C.; Burda, B.U. Primary Care Screening for and Treatment of Depression in Pregnant and Postpartum Women: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 315, 388–406. [Google Scholar] [CrossRef]
- Kettunen, P.; Koistinen, E.; Hintikka, J. Is postpartum depression a homogenous disorder: Time of onset, severity, symptoms and hopelessness in relation to the course of depression. BMC Pregnancy Childbirth 2014, 14, 402. [Google Scholar] [CrossRef]
- Munk-Olsen, T.; Laursen, T.M.; Pedersen, C.B.; Mors, O.; Mortensen, P.B. New parents and mental disorders: A population-based register study. JAMA 2006, 296, 2582–2589. [Google Scholar] [CrossRef]
- Hahn-Holbrook, J.; Cornwell-Hinrichs, T.; Anaya, I. Economic and Health Predictors of National Postpartum Depression Prevalence: A Systematic Review, Meta-analysis, and Meta-Regression of 291 Studies from 56 Countries. Front. Psychiatry 2017, 8, 248. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency (n) | Percentage |
|---|---|---|
| Maternal education | ||
| Below university degree | 227 | 24.3 |
| University degree or more | 705 | 75.7 |
| Marital status | ||
| Single | 24 | 2.6 |
| Married | 914 | 97.4 |
| Parity | ||
| 0 | 509 | 54.3 |
| 1 | 330 | 35.2 |
| 2 or more | 99 | 10.6 |
| Household Income | ||
| Less than 70k | 147 | 15.9 |
| 70k or more | 779 | 84.1 |
| Delivery Type | ||
| Spontaneous Vaginal Birth/Planned C-section | 764 | 81.5 |
| Unplanned C-section | 174 | 18.6 |
| Gestational age at birth | ||
| <37 weeks | 59 | 6.3 |
| 37 or more weeks | 879 | 93.7 |
| Child sex | ||
| Male | 487 | 51.9 |
| Female | 451 | 48.1 |
| PTSD score | ||
| 0 | 702 | 74.8 |
| 1 | 129 | 13.8 |
| 2 | 49 | 5.2 |
| 3 | 32 | 3.4 |
| 4 | 13 | 1.4 |
| 5 or more | 13 | 1.4 |
| Mean (SD) | Range | |
| Maternal age | 32.1 (4.2) | 17–44 |
| Prenatal depression symptoms | 6.6 (4) | 0–22 |
| PPD symptoms | 4.8 (3.9) | 0–20 |
| Prenatal social support | 14.8 (2.24) | 4–16 |
| PTSD symptoms | 0.6 (1.45) | 0–11 |
| Internalizing behavior | 44.8 (8.3) | 29–73 |
| Externalizing behavior | 45.8 (8.2) | 28–68 |
| Indirect Effect | Effect | Bootstrap SE | 95% CI |
|---|---|---|---|
| Total Indirect Effect | 0.185 0.034 | 0.164 0.106 | −0.102, 0.550 −0.148, 0.282 |
| Ind 1 (a): delivery type→maternal PTSD→child internalizing | 0.026 −0.001 | 0.065 0.060 | −0.058, 0.232 −0.078, 0.186 |
| Ind 2 (b): delivery type→maternal PPD→child internalization | 0.087 −0.002 | 0.135 0.080 | −0.171, 0.364 −0.164, 0.162 |
| Ind 3 (c1): delivery type→maternal PTSD→maternal PPD→child internalization | 0.072 0.026 | 0.050 0.023 | 0.000, 0.202 0.000, 0.096 |
| Indirect Effect | Effect | Bootstrap SE | 95% CI |
|---|---|---|---|
| Total Indirect Effect | 0.192 0.052 | 0.143 0.087 | −0.054, 0.512 −0.092, 0.260 |
| Ind 1 (a): delivery type→maternal PTSD→child internalization | 0.063 0.035 | 0.064 0.056 | −0.014, 0.269 −0.031, 0.216 |
| Ind 2 (b): delivery type→maternal PPD→child internalization | 0.071 −0.001 | 0.011 0.059 | −0.132, 0.312 −0.121, 0.123 |
| Ind 3 (c1): delivery type→maternal PTSD→maternal PPD→child internalization | 0.059 0.018 | 0.041 0.017 | 0.002, 0.173 0.000, 0.076 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grisbrook, M.-A.; Dewey, D.; Cuthbert, C.; McDonald, S.; Ntanda, H.; Letourneau, N. The Association between Cesarean Section Delivery and Child Behavior: Is It Mediated by Maternal Post-Traumatic Stress Disorder and Maternal Postpartum Depression? Behav. Sci. 2024, 14, 61. https://doi.org/10.3390/bs14010061
Grisbrook M-A, Dewey D, Cuthbert C, McDonald S, Ntanda H, Letourneau N. The Association between Cesarean Section Delivery and Child Behavior: Is It Mediated by Maternal Post-Traumatic Stress Disorder and Maternal Postpartum Depression? Behavioral Sciences. 2024; 14(1):61. https://doi.org/10.3390/bs14010061
Chicago/Turabian StyleGrisbrook, Marie-Andrée, Deborah Dewey, Colleen Cuthbert, Sheila McDonald, Henry Ntanda, and Nicole Letourneau. 2024. "The Association between Cesarean Section Delivery and Child Behavior: Is It Mediated by Maternal Post-Traumatic Stress Disorder and Maternal Postpartum Depression?" Behavioral Sciences 14, no. 1: 61. https://doi.org/10.3390/bs14010061
APA StyleGrisbrook, M.-A., Dewey, D., Cuthbert, C., McDonald, S., Ntanda, H., & Letourneau, N. (2024). The Association between Cesarean Section Delivery and Child Behavior: Is It Mediated by Maternal Post-Traumatic Stress Disorder and Maternal Postpartum Depression? Behavioral Sciences, 14(1), 61. https://doi.org/10.3390/bs14010061