
Psychological Impact of the COVID-19 Pandemic on Pregnant Women: A Scoping Review

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
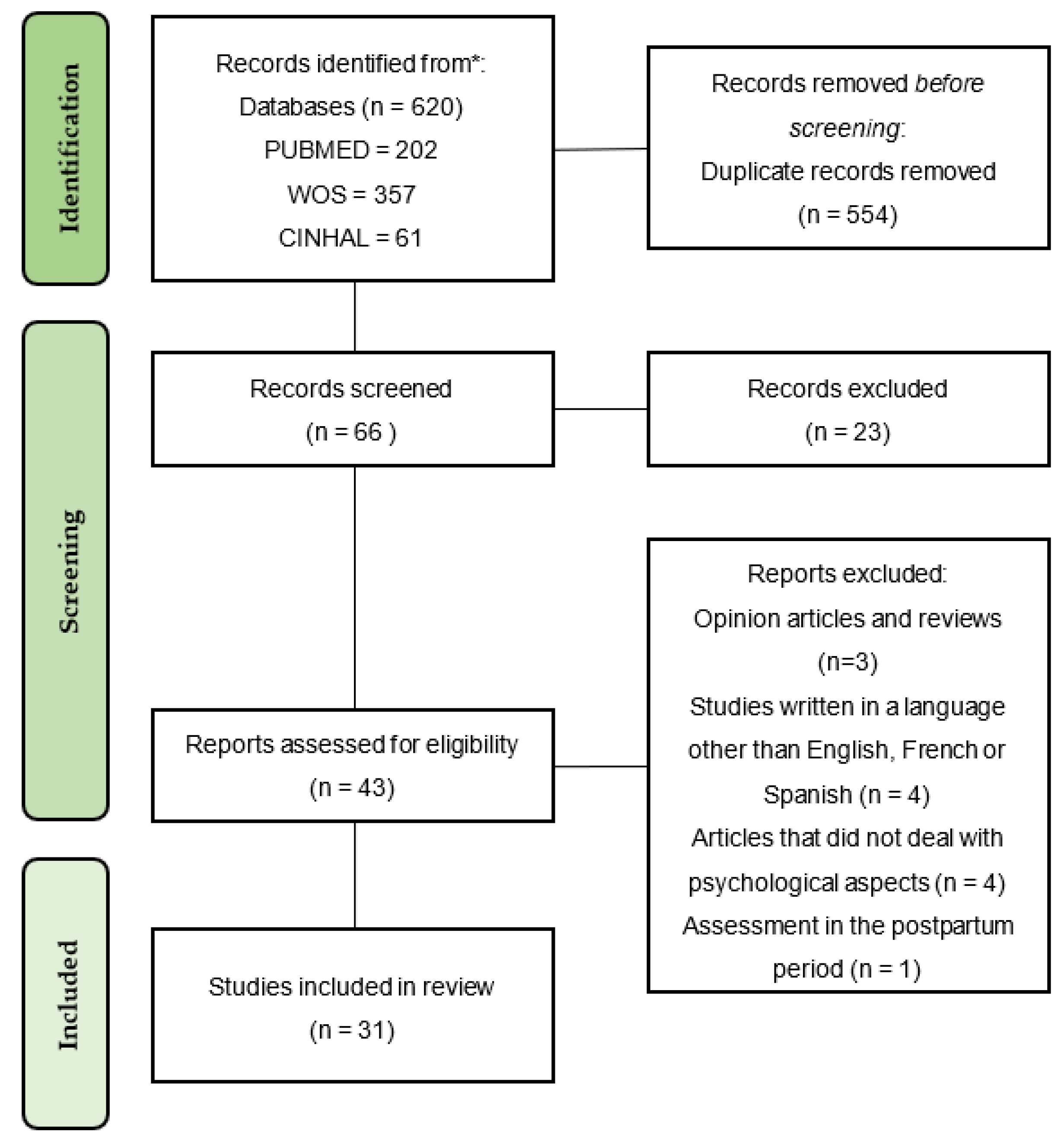
2.1. Literature Search and Selection of Studies
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Analysis
2.4. Data Extraction and Management
2.5. Quality Assessment Tool
3. Results
3.1. Study Characteristics
3.2. Symptoms of Depression
3.3. Symptoms of Anxiety
3.4. Stress Levels
3.5. Mood and Psychopathological Symptoms
4. Discussion
4.1. Limitations
4.2. Strengths
4.3. Implications for Practice and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Alanagreh, L.; Alzoughool, F.; Atoum, M. The Human Coronavirus Disease COVID-19: Its Origin, Characteristics, and Insights into Potential Drugs and Its Mechanisms. Pathogens 2020, 9, 331. [Google Scholar] [CrossRef] [PubMed]
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Abrahao-Machado, L.F.; Dahal, S.; Kumar, H.; Kv, D. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med. J. 2020, 96, 753–758. [Google Scholar] [PubMed]
- Ministerio de Sanidad, Consumo y Bienestar Social—Profesionales—Situación actual Coronavirus. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/situacionActual.htm (accessed on 2 September 2021).
- Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?adgroupsurvey=%7Badgroupsurvey%7D&gclid=Cj0KCQjw7MGJBhD-ARIsAMZ0eeuXa_sAMir7JGEFInKKfby2BZSNQQiICNxjCOYt-lF_nBdn5wD0lkEaAkKXEALw_wcB (accessed on 2 September 2021).
- Kakodkar, P.; Kaka, N.; Baig, M. A Comprehensive Literature Review on the Clinical Presentation, and Management of the Pandemic Coronavirus Disease 2019 (COVID-19). Cureus 2020, 12, e7560. [Google Scholar] [CrossRef]
- Han, Q.; Zheng, B.; Agostini, M.; Bélanger, J.J.; Gützkow, B.; Kreienkamp, J.; Reitsema, A.M.; van Breen, J.A.; Collaboration, P.; Leander, N.P. Associations of risk perception of COVID-19 with emotion and mental health during the pandemic. J. Affect. Disord. 2021, 284, 247–255. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain. Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Bjelica, A.; Cetkovic, N.; Trninic-Pjevic, A.; Mladenovic-Segedi, L. The phenomenon of pregnancy—A psychological view. Ginekol. Pol. 2018, 89, 102–106. [Google Scholar] [CrossRef]
- Nagandla, K.; Nalliah, S.; Yin, L.; Majeed, Z.; Ismail, I.; Zubaidah, S.; Ragavan, U.; Krishnan, S. Prevalence and associated risk factors of depression, anxiety and stress in pregnancy. Int. J. Reprod. Contracept. Obstet. Gynecol. 2016, 5, 2380–2388. [Google Scholar] [CrossRef]
- Guimaraes, F.J.; Da Silva Santos, F.J.; Bern Leite, A.F.; De Holanda, V.R.; De Sousa, G.S.; Alburquerque Perrelli, J.G. Preferencias Enfermedad mental en mujeres embarazadas. Enfermería Glob. 2018, 18, 499–534. [Google Scholar] [CrossRef]
- Kassada, D.S.; Waidman, M.A.P.; Miasso, A.I.; Marcon, S.S. Prevalência de transtornos mentais e fatores associados em gestantes. Acta Paul. Enferm. 2015, 28, 495–502. [Google Scholar] [CrossRef]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef]
- Auger, N.; Potter, B.J.; Healy-Profitós, J.; He, S.; Schnitzer, M.E.; Paradis, G. Mood disorders in pregnant women and future cardiovascular risk. J. Affect. Disord. 2020, 266, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Accortt, E.E.; Cheadle, A.C.D.; Dunkel Schetter, C. Prenatal depression and adverse birth outcomes: An updated systematic review. Matern. Child Health J. 2015, 19, 1306–1337. [Google Scholar] [CrossRef]
- Caparros-Gonzalez, R.A.; Perra, O.; Alderdice, F.; Lynn, F.; Lobel, M.; García-García, I.; Peralta-Ramírez, M.I. Psychometric validation of the Prenatal Distress Questionnaire (PDQ) in pregnant women in Spain. Women Health 2019, 59, 937–952. [Google Scholar] [CrossRef] [PubMed]
- Knight, M.; Bunch, K.; Vousden, N.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J.; et al. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: National population based cohort study. BMJ 2020, 369, m2107. [Google Scholar] [CrossRef]
- Sapkota, B.; Mali, N.S.; Singh, R.D. Prenatal Anxiety among Pregnant Women Visiting in Antenatal Care Outpatient Department at Paropakar Maternity and Women’s Hospital. Int. J. Health Sci. Res. 2019, 9, 173–181. [Google Scholar]
- Ravaldi, C.; Ricca, V.; Wilson, A.; Homer, C.; Vannacci, A. Previous psychopathology predicted severe COVID-19 concern, anxiety, and PTSD symptoms in pregnant women during “lockdown” in Italy. Arch. Women’s Ment. Heals 2020, 23, 783–786. [Google Scholar] [CrossRef]
- Caparros-Gonzalez, R.A.; Luque-Fernández, M.Á. Mental health in the perinatal period and maternal stress during the Covid-19 pandemic: Influence on fetal development. Rev. Esp. Salud Publica 2020, 94, e1–e2. [Google Scholar]
- Caparros-Gonzalez, R.A.; Ganho-Ávila, A.; Torre-Luque, A. de la The COVID-19 Pandemic Can Impact Perinatal Mental Health and the Health of the Offspring. Behav. Sci. 2020, 10, 162. [Google Scholar] [CrossRef] [PubMed]
- Naurin, E.; Markstedt, E.; Stolle, D.; Enström, D.; Wallin, A.; Andreasson, I.; Attebo, B.; Eriksson, O.; Martinsson, K.; Elden, H.; et al. Pregnant under the pressure of a pandemic: A large-scale longitudinal survey before and during the COVID-19 outbreak. Eur. J. Public Health 2021, 31, 7–13. [Google Scholar] [CrossRef]
- Shayganfard, M.; Mahdavi, F.; Haghighi, M.; Sadeghi Bahmani, D.; Brand, S. Health Anxiety Predicts Postponing or Cancelling Routine Medical Health Care Appointments among Women in Perinatal Stage during the Covid-19 Lockdown. Int. J. Environ. Res. Public Health 2020, 17, 8272. [Google Scholar] [CrossRef]
- Pacheco, F.; Sobral, M.; Guiomar, R.; de la Torre-Luque, A.; Caparros-Gonzalez, R.A.; Ganho-ávila, A. Breastfeeding during covid-19: A narrative review of the psychological impact on mothers. Behav. Sci. 2021, 11, 34. [Google Scholar] [CrossRef] [PubMed]
- Brik, M.; Sandonis, M.A.; Fernández, S.; Suy, A.; Parramon-Puig, G.; Maiz, N.; Dip, M.E.; Ramos-Quiroga, J.A.; Carreras, E. Psychological impact and social support in pregnant women during lockdown due to SARS-CoV2 pandemic: A cohort study. Acta obstetricia et gynecologica Scandinavica 2021, 100, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Ren, J.; Luo, B.; Xiang, J.; Wang, G.; Gu, L.; Chen, P. Women’s Psychological Health, Family Function, and Social Support During Their Third Trimester of Pregnancy Within the COVID-19 Epidemic: A Cross-sectional Survey. Disaster Med. Public Health Prep. 2021, 1–5, Advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Effati-Daryani, F.; Zarei, S.; Mohammadi, A.; Hemmati, E.; Ghasemi Yngyknd, S.; Mirghafourvand, M. Depression, stress, anxiety and their predictors in Iranian pregnant women during the outbreak of COVID-19. BMC Psychol. 2020, 8, 99. [Google Scholar] [CrossRef]
- Jiang, H.; Jin, L.; Qian, X.; Xiong, X.; La, X.; Chen, W.; Yang, X.; Yang, F.; Zhang, X.; Abudukelimu, N.; et al. Maternal Mental Health Status and Approaches for Accessing Antenatal Care Information During the COVID-19 Epidemic in China: Cross-Sectional Study. J. Med. Internet Res. 2021, 23, e18722. [Google Scholar] [CrossRef] [PubMed]
- Matsushima, M.; Horiguchi, H. The COVID-19 Pandemic and Mental Well-Being of Pregnant Women in Japan: Need for Economic and Social Policy Interventions. Disaster Med. Public Health Prep. 2020, 1–6. [Google Scholar] [CrossRef]
- Shahid, A.; Javed, A.; Rehman, S.; Tariq, R.; Ikram, M.; Suhail, M. Evaluation of psychological impact, depression, and anxiety among pregnant women during the COVID-19 pandemic in Lahore, Pakistan. Int. J. Gynaecol. Obstet. 2020, 151, 462–465. [Google Scholar] [CrossRef]
- Sun, G.; Wang, Q.; Lin, Y.; Li, R.; Yang, L.; Liu, X.; Peng, M.; Wang, H.; Yang, X.; Ren, W.; et al. Perinatal Depression of Exposed Maternal Women in the COVID-19 Pandemic in Wuhan, China. Front. Psychiatry 2020, 11, 551812. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, C.; Liu, H.; Duan, C.; Li, C.; Fan, J.; Li, H.; Chen, L.; Xu, H.; Li, X.; et al. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am. J. Obstet. Gynecol. 2020, 223, e1–e240. [Google Scholar] [CrossRef] [PubMed]
- Romero-Gonzalez, B.; Puertas-Gonzalez, J.A.; Mariño-Narvaez, C.; Peralta-Ramirez, M.I. Variables del confinamiento por COVID-19 predictoras de sintomatología ansiosa y depresiva en mujeres embarazadas. Med. Clin. 2021, 156, 172–176. [Google Scholar] [CrossRef]
- Puertas-Gonzalez, J.A.; Mariño-Narvaez, C.; Peralta-Ramirez, M.I.; Romero-Gonzalez, B. The psychological impact of the COVID-19 pandemic on pregnant women. Psychiatry Res. 2021, 301, 113978. [Google Scholar] [CrossRef] [PubMed]
- Yirmiya, K.; Yakirevich-Amir, N.; Preis, H.; Lotan, A.; Atzil, S.; Reuveni, I. Women’s Depressive Symptoms during the COVID-19 Pandemic: The Role of Pregnancy. Int. J. Environ. Res. Public Health 2021, 18, 4298. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef]
- Moyer, C.A.; Compton, S.D.; Kaselitz, E.; Muzik, M. Pregnancy-related anxiety during COVID-19: A nationwide survey of 2740 pregnant women. Arch. Womens. Ment. Health 2020, 23, 757–765. [Google Scholar] [CrossRef]
- Ng, Q.J.; Koh, K.M.; Tagore, S.; Mathur, M. Perception and Feelings of Antenatal Women during COVID-19 Pandemic: A Cross-Sectional Survey. Ann. Acad. Med. Singapore 2020, 49, 543–552. [Google Scholar] [CrossRef]
- Zhou, Y.; Shi, H.; Liu, Z.; Peng, S.; Wang, R.; Qi, L.; Li, Z.; Yang, J.; Ren, Y.; Song, X.; et al. The prevalence of psychiatric symptoms of pregnant and non-pregnant women during the COVID-19 epidemic. Transl. Psychiatry 2020, 10, 319. [Google Scholar] [CrossRef]
- Akgor, U.; Fadıloglu, E.; Soyak, B.; Unal, C.; Cagan, M.; Temiz, B.E.; Erzenoglu, B.E.; Ak, S.; Gultekin, M.; Ozyuncu, O. Anxiety, depression and concerns of pregnant women during the COVID-19 pandemic. Arch. Gynecol. Obstet. 2021, 304, 125–130. [Google Scholar] [CrossRef]
- Farrell, T.; Reagu, S.; Mohan, S.; Elmidany, R.; Qaddoura, F.; Ahmed, E.E.; Corbett, G.; Lindow, S.; Abuyaqoub, S.M.; Alabdulla, M.A. The impact of the COVID-19 pandemic on the perinatal mental health of women. J. Perinat. Med. 2020, 48, 971–976. [Google Scholar] [CrossRef]
- Khoury, J.E.; Atkinson, L.; Bennett, T.; Jack, S.M.; Gonzalez, A. COVID-19 and mental health during pregnancy: The importance of cognitive appraisal and social support. J. Affect. Disord. 2021, 282, 1161–1169. [Google Scholar] [CrossRef]
- López-Morales, H.; Del Valle, M.V.; Canet-Juric, L.; Andrés, M.L.; Galli, J.I.; Poó, F.; Urquijo, S. Mental health of pregnant women during the COVID-19 pandemic: A longitudinal study. Psychiatry Res. 2021, 295, 113567. [Google Scholar] [CrossRef]
- Kahyaoglu Sut, H.; Kucukkaya, B. Anxiety, depression, and related factors in pregnant women during the COVID-19 pandemic in Turkey: A web-based cross-sectional study. Perspect. Psychiatr. Care 2021, 57, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Ayaz, R.; Hocaoğlu, M.; Günay, T.; Yardımcı, O.D.; Turgut, A.; Karateke, A. Anxiety and depression symptoms in the same pregnant women before and during the COVID-19 pandemic. J. Périnat. Med. 2020, 48, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Taubman-Ben-Ari, O.; Chasson, M.; Abu Sharkia, S.; Weiss, E. Distress and anxiety associated with COVID-19 among Jewish and Arab pregnant women in Israel. J. Reprod. Infant Psychol. 2020, 38, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Drouin-Maziade, C.; Martel, É.; Maziade, M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet. Gynecol. Scand. 2020, 99, 848–855. [Google Scholar] [CrossRef]
- Kassaw, C.; Pandey, D. The prevalence of general anxiety disorder and its associated factors among women’s attending at the perinatal service of Dilla University referral hospital, Dilla town, Ethiopia, April, 2020 in Covid pandemic. Heliyon 2020, 6, e05593. [Google Scholar] [CrossRef]
- Liu, X.; Chen, M.; Wang, Y.; Sun, L.; Zhang, J.; Shi, Y.; Wang, J.; Zhang, H.; Sun, G.; Baker, P.; et al. Prenatal anxiety and obstetric decisions among pregnant women in Wuhan and Chongqing during the COVID-19 outbreak: A cross-sectional study. BJOG An. Int. J. Obstet. Gynaecol. 2020, 127, 1229–1240. [Google Scholar] [CrossRef]
- Sinaci, S.; Ozden Tokalioglu, E.; Ocal, D.; Atalay, A.; Yilmaz, G.; Keskin, H.L.; Erdinc, S.O.; Sahin, D.; Moraloglu Tekin, O. Does having a high-risk pregnancy influence anxiety level during the COVID-19 pandemic? Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 255, 190–196. [Google Scholar] [CrossRef]
- Colli, C.; Penengo, C.; Garzitto, M.; Driul, L.; Sala, A.; Degano, M.; Preis, H.; Lobel, M.; Balestrieri, M. Prenatal Stress and Psychiatric Symptoms During Early Phases of the COVID-19 Pandemic in Italy. Int. J. Womens. Health 2021, 13, 653–662. [Google Scholar] [CrossRef]
- Preis, H.; Mahaffey, B.; Heiselman, C.; Lobel, M. Vulnerability and resilience to pandemic-related stress among U.S. women pregnant at the start of the COVID-19 pandemic. Soc. Sci. Med. 2020, 266, 113348. [Google Scholar] [CrossRef]
- Chaves, C.; Marchena, C.; Palacios, B.; Salgado, A.; Duque, A. Effects of the COVID-19 pandemic on perinatal mental health in Spain: Positive and negative outcomes. Women Birth 2021, in press. [Google Scholar] [CrossRef]
- Davenport, M.H.; Meyer, S.; Meah, V.L.; Strynadka, M.C.; Khurana, R. Moms Are Not OK: COVID-19 and Maternal Mental Health. Front. Glob. Women’s Health 2020, 1. [Google Scholar] [CrossRef]
- Mappa, I.; Distefano, F.A.; Rizzo, G. Effects of coronavirus 19 pandemic on maternal anxiety during pregnancy: A prospectic observational study. J. Perinat. Med. 2020, 48, 545–550. [Google Scholar] [CrossRef]
- Saccone, G.; Florio, A.; Aiello, F.; Venturella, R.; De Angelis, M.C.; Locci, M.; Bifulco, G.; Zullo, F.; Di Spiezio Sardo, A. Psychological impact of coronavirus disease 2019 in pregnant women. Am. J. Obstet. Gynecol. 2020, 223, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wu, W.; Zhao, X.; Zhang, W. Recommended psychological crisis intervention response to the 2019 novel coronavirus pneumonia outbreak in China: A model of West China Hospital. Precis. Clin. Med. 2020, 3, 3–8. [Google Scholar] [CrossRef]
- O’Connor, C.; Murphy, M. Going viral: Doctors must tackle fake news in the covid-19 pandemic. BMJ 2020, 369, m1587. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, R.; Garon-Bissonnette, J.; Loiselle, M.; Martel, É.; Drouin-Maziade, C.; Berthelot, N. Association entre la fréquence de consultation des médias d’information et la détresse psychologique chez les femmes enceintes durant la pandémie de COVID-19: Association between news media consulting frequency and psychological distress in pregnant women. Can. J. Psychiatry 2021, 66, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Shao, B.; Mo, M.; Xin, X.; Jiang, W.; Wu, J.; Huang, M.; Wang, S.; Muyiduli, X.; Si, S.; Shen, Y.; et al. The interaction between prepregnancy BMI and gestational vitamin D deficiency on the risk of gestational diabetes mellitus subtypes with elevated fasting blood glucose. Clin. Nutr. 2020, 39, 2265–2273. [Google Scholar] [CrossRef]
- Basu, A.; Kim, H.H.; Basaldua, R.; Choi, K.W.; Charron, L.; Kelsall, N.; Hernandez-Diaz, S.; Wyszynski, D.F.; Koenen, K.C. A cross-national study of factors associated with women’s perinatal mental health and wellbeing during the COVID-19 pandemic. PLoS ONE 2021, 16, e0249780. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Weston, D.; Greenberg, N. Psychological impact of infectious disease outbreaks on pregnant women: Rapid evidence review. Public Health 2020, 189, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Rogozińska, E.; Marlin, N.; Jackson, L.; Rayanagoudar, G.; Ruifrok, A.E.; Dodds, J.; Molyneaux, E.; van Poppel, M.N.M.; Poston, L.; Vinter, C.A.; et al. Effects of antenatal diet and physical activity on maternal and fetal outcomes: Individual patient data meta-analysis and health economic evaluation. Health Technol. Assess. 2017, 21, 1–158. [Google Scholar] [CrossRef]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- Braunack-Mayer, A.; Tooher, R.; Collins, J.E.; Street, J.M.; Marshall, H. Understanding the school community’s response to school closures during the H1N1 2009 influenza pandemic. BMC Public Heals 2013, 13, 344. [Google Scholar] [CrossRef]
- Aknin, L.; De Neve, J.-E.; Dunn, E.; Fancourt, D.; Goldberg, E.; Helliwell, J.; Jones, S.P.; Karam, E.; Layard, R.; Lyubomirsky, S.; et al. Mental Health During the First Year of the COVID-19 Pandemic: A Review and Recommendations for Moving Forward. PsyArXiv 2021. [Google Scholar] [CrossRef]
- Cannella, D.; Lobel, M.; Monheit, A. Knowing is believing: Information and attitudes towards physical activity during pregnancy. J. Psychosom. Obstet. Gynecol. 2010, 31, 236–242. [Google Scholar] [CrossRef]
- Sun, S.; Goldberg, S.B.; Lin, D.; Qiao, S.; Operario, D. Psychiatric symptoms, risk, and protective factors among university students in quarantine during the COVID-19 pandemic in China. Global. Health 2021, 17, 15. [Google Scholar] [CrossRef]
- Puertas-Gonzalez, J.A.; Mariño-Narvaez, C.; Romero-Gonzalez, B.; Peralta-Ramirez, M.I. Stress and Psychopathology Reduction in Pregnant Women through Online Cognitive Behavioural Therapy during COVID-19: A Feasibility Study. Behav. Sci. 2021, 11, 100. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.P. Fetal programming of coronary heart disease. Trends Endocrinol. Metab. 2002, 13, 364–368. [Google Scholar] [CrossRef]
- Helgertz, J.; Bengtsson, T. The Long-Lasting Influenza: The Impact of Fetal Stress During the 1918 Influenza Pandemic on Socioeconomic Attainment and Health in Sweden, 1968–2012. Demography 2019, 56, 1389–1425. [Google Scholar] [CrossRef] [PubMed]
- Caparros-Gonzalez, R.A.; de la Torre-Luque, A.; Romero-Gonzalez, B.; Quesada-Soto, J.M.; Alderdice, F.; Peralta-Ramírez, M.I. Stress During Pregnancy and the Development of Diseases in the offspring: A Systematic-Review and Meta-Analysis. Midwifery 2021, 97, 102939. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion criteria | |
|---|---|
| Language | Studies written in Spanish, English or French |
| Design | Observational studies |
| Population | Pregnant women |
| Risk factor | Studies which considered the psychological issues of pregnant women during the COVID-19 pandemic |
| Year of publication | Articles published between 2020 and September 2021 |
| Exclusion criteria | |
| Design | Literature reviews and editorials |
| Author, Year | Country | Study Design | Assessment Tool | N | Age Mean (Years) | Gestational Age (Weeks) | Main Results | Conclusions | Quality of the Study * |
|---|---|---|---|---|---|---|---|---|---|
| Effati-Daryani et al., 2020 [29] | Iran | Cross sectional study | Questionnaire: DASS-21 | 205 | 29.3 (SD = 5.5) | NR | Pregnant women: 32.7% Depression 32.7% Anxiety 43.9% Stress (Prevalence) | Maintaining high partner satisfaction, possessing a high level of education (the couple) and a stable income level, decreases the levels of depression, anxiety and stress | 8/10 |
| Jiang et al., 2020 [30] | China | Cross sectional study | Questionnaire: PSS SAS EDS | 1873 | 29 (SD = 4.10) | NR | Pregnant women: 45.9% Depression 18.1% Anxiety 89.1% Stress (Prevalence) | Using the informational tools provided by the hospital, decreases the risk of depression anxiety and stress. | 6/10 |
| Matsushima et al., 2020 [31] | Japan | Cross sectional | EPDS | 1777 | NR | Third trimester: 45.08% (SD= 0.50) | EPDS ≥ 13 17% (0.38), Depression: 1.82 (2.05), Anxiety: 3.68 (2.28) | A high percentage of pregnant women showed depressive symptoms | 5/10 |
| Shahid et al., 2020 [32] | Pakistan | Cross sectional | EPDS | 552 | NR | NR | 39% stated that the pandemic had caused them depression and anxiety; 33% were found to have possible depression (EPDS > 10) and 6% scored EPDS = 30 (maximum depression) | Pregnancy is a determinant factor for negative perceptions of the COVID-19 pandemic | 6/10 |
| Sun et al., 2020 [33] | China | Cross sectional | EPDS | 2883, Prenatal: 26.08%, Postnatal: 73.92% | 25–29 aged: 41.42% | NR | The prevalence of maternal depression was increased from 30.99% to 42.98% | Prenatal depression in the beginning of the epidemic and postnatal depression in the end of the epidemic should be noticed | 7/10 |
| Wu et al., 2020 [34] | China | Cross sectional | EPDS | 4124 | 30 (27-32) | NR | Overall, the prevalence of depressive symptoms was 26.0–29.6%. | The risk for mental illness among pregnant women have increased including thoughts of self-harm | 9/10 |
| Romero-Gonzalez et al., 2021 [35] | Spain | Cross sectional | SCL-90-R, PDQ, PSS, CD-RISC, AIS | 131 | 32.95 (SD = 4.75) | 27.20 (SD = 8.74) | Depressive symptomatology in confinement increases with loneliness, fear of contagion and perceived stress as well as anxiety, perceived stress and insomnia, increase with feelings of loneliness and fear of contagion | Perceived stress, pregnancy-specific stress, as well as insomnia are predictor variables in most anxious and depressive symptoms related to COVID-19. | 3/10 |
| Puertas-Gonzalez et al., 2021 [36] | Spain | Cross sectional | SCL-90-R, PSS, PDQ, AIS | Pregnant women during (PG) and prior (PPG) the pandemic (n = 100 respectively) | 33.20 (SD = 4.71) and 33.04 (SD = 4.45) | 26.47 (SD = 9.12) and 27.26 (SD = 8.70) | PG obtained higher scores than PPG with an average effect size in the depression dimension of the SCL-90, and with a small effect size in the phobic anxiety dimension of the SCL-90 and in the PSS | Women who were pregnant during the pandemic showed higher levels of depression and phobic anxiety than a group of pregnant women assessed before the COVID-19 pandemic | 3/10 |
| Yirmiya et al., 2021 [37] | Israel | Cross sectional | PHQ-2, PREPS, GAD-7 | Pregnant (N = 1114), Non-Pregnant (N = 256) | 31.88 (SD = 4.22), 35.71 (SD = 5.42) | NR | Pregnant women reported significantly fewer depressive symptoms than non-pregnant women. Non significant differences were observed between pregnant and non-pregnant women in levels of stress and anxiety | During the first wave of the COVID-19 pandemic, non-pregnant women had higher depressive symptoms than pregnant women. | 4/10 |
| Lebel et al., 2020 [38] | Canada | Cross sectional study | Questionnaire: EDS PROMIS SSEQ ISEL GSLTPAQ | 1987 | 32.4 (SD = 4.2) | 22.5 (SD = 8.4) | Pregnant women: 37% Depression 57% Anxiety (Prevalence) | Having high social support, staying physically active, is associated with lower levels of anxiety and depression in pregnant women during the pandemic. | 5/10 |
| Moyer et al., 2020 [39] | USA | Cross sectional study | Questionnaire: VAS PRaS | 2740 | 32.7 | NR | Pregnant women: PRaS score: pre-COVID-19: 20.6. Pregnant women: COVID-19: 23.9. (Prevalence) | The main concerns of pregnant women during the pandemic were: the fear of food shortages, the risk of contagion from work, the likelihood of not receiving care for the baby, etc. | 6/10 |
| QJ Ng et al., 2020 [40] | Singapur | Cross sectional | Questionnaire: DASS-21 | 324 | 31.8 (SD = 4.2) | 23.4 (SD = 10) | Pregnant women: 18.2% Depression 35.8% Anxiery 11.1% Stress | Online platforms are the main source of information for pregnant women. | 5/10 |
| Zhou et al., 2020 [41] | China | Cross sectional | Questionnaire: PHQ-9, GAD-7, PCL-5, SCL-90, ISI | 859 (544 pregnant;315 not pregnant) | Not pregnant: 35.4 (SD = 5.7). Pregnant: 31.1 (SD = 3.9) | NR | Pregnant women: 5.3% Depression. 6.8% Anxiety, 2.4% somatic symptoms, 2.6% insomnia, 0.9% post-traumatic stress | During the pandemic, pregnant women are less likely to suffer from anxiety and depression than women who are not. | 5/10 |
| Akgor et al., 2020 [42] | Turkey | Cohort | Questionnaire: HADS | 297 | 27.64 (SD = 5.27) | 27.04 (SD= 8.85) | HADS-A 7.94 (SD = 4.03), HADS-D 7.23 (SD = 3.84) | Anxiety and depresion were associated with concern about the inability to reach obstetrician and being in advanced age. | 3/9 |
| Farrell et al., 2020 [43] | Qatar | Cross sectional | GAD-7, PHQ-9 | 288 | 30,5 (SD = 5.3) | 26.1 (SD= 14.3) | Prevalence of anxiety and depression was 34.4% and 39.2% respectively. | More than a third of women scored anxiety and depression ratings. | 3/10 |
| Khoury et al., 2021 [44] | Canada | Cross sectional | CWS, CES-D, ISI, and MSPSS | 303 | 32.13 (SD = 4.22) | 21.47 (SD = 8.92) | CWS 1.94 (SD = 0.97), CES-D: 11.50 (SD = 6.36), ISI score ≥ 15: 19.2% (clinical insomnia) | Pregnant women are experiencing high levels of anxiety and depressive symptoms during the COVID-19 pandemic | 5/10 |
| López-Morales et al., 2021 [45] | Argentina | Cohort | BAI, STAI-T | Pregnant women: 102, non-pregnant women: 102 | 32.56 (SD = 4.71) | 32.56 (SD= 4.71) | Time 1 vs. Time 3: Pregnant women: BDI-II: 8.71 (6.08) vs. 15.42 (8.50), STAI-T: 22.66 (9.48) vs. 28.10 (9.60), Non pregnant women: BDI-II: 7.92 (4.53) vs. 10.83 (6.79), STAI-T: 21.51 (8.44) vs. 23.97 (9.27) | Pregnant women showed a more pronounced increase in depression, anxiety than the non-pregnant women. | 7/9 |
| Kahyaoglu -Sut and Kucukkaya, 2020 [46] | Turkey | Cross sectional | Questionnaire: HADS | 403 | 28.2 (SD = 4.5) | 27.9 (SD = 8.8) | Pregnant women: 64.5% Anxiety, 56.3% Depression | Being an active worker during the pandemic, maintaining a sports routine, information from a healthcare professional, are some of the beneficial factors related to anxiety and depression. | 3/10 |
| Ayaz et al., 2020 [47] | Turkey | Cross sectional | Questionnaire: BAI IDAS-II | 63 | 30.35 (SD = 5.27) | 32.7 | Pregnant women: IDAS II: pre-COVID-19: Pre184.7 (SD = 49.67), COVID-19: 202.57 (SD = 52.90). BAI: ANYTHING: pre-COVID n = 10, COVID n = 6. SEVERE: Pre-COVID-19 n = 2, COVID-19 n = 8 | Stress and anxiety levels in pregnant women have increased as a result of the COVID-19 pandemic | 9/10 |
| Taubman-Ben-Ari et al., 2020 [48] | Israel | Cross sectional | Questionnaire: HI-5 | 336 | 30.31 (SD = 4.7) | 25.40 (SD = 9.6) | Causes of anxiety in pregnant women during the pandemic were the fear of being infected when attending gynecological appointments, using public transports or when walking in public places; fear of COVID-19 infection by a family member; worries about the fetus health; and the birth time. | Arab pregnant women showed higher levels of anxiety than Jewish women. In addition, suffering from poor health, being in the 3rd trimester of pregnancy and being primiparity were the factors that contributed to high anxiety levels. | 4/10 |
| Berthelot et al., 2020 [49] | Canada | Cohort | Questionnaire: K10 PCL-5 PANAS | 1754 | 29.27 (SD = 4.23) | 24.80 (SD = 9.40) | Pregnant women: Anxiety/depression: pre-COVID-19: -0.39 (SD = 0.04), COVID-19: 0.15 (SD = 0.03). Post-traumatic stress: pre-COVID-19: -0.12 (SD = 0.04). COVID-19: 0.06 (SD = 0.03). | Pregnant women surveyed during the pandemic suffer from higher levels of psychological events (anxiety and depression) than those surveyed before the pandemic. | 5/9 |
| Kassaw et al., 2020 [50] | Ethiopia | Cross sectional study | Interview GAD-7 OSLO-3 | 178 | 28 (SD = 5.6) | NR | Pregnant women: 32.2% Anxiety prevalence | Living in an urban environment, primiparity, secondary education and low social support, are risk factors for suffering from anxious symptoms. | 10/10 |
| Liu et al., 2020 [51] | China | Cross sectional study | Questionnaire: SAS | 1947 | NR | NR | Pregnant women: 17.2% Anxiety (Prevalence) | In Wuhan, more pregnant people suffered from anxiety than in Chongqing. Staying at home, having subjective symptoms increased anxious episodes. | 6/10 |
| Sinaci et al., 2020 [52] | Turkey | Cross sectional | Questionnaire: STAI-T, BAI | 446 | 28.9 (SD = 5.7) | 24.5 (SD = 7.7) | Pregnant women: Anxiety pre-pandemia: Total 39.34 (SD = 6.39), Anxiety during the pandemic: Total: 44.57 (SD = 9.55). | High-risk pregnant women suffer more anxiety than those without risk. | 4/10 |
| Colli et al., 2021 [53] | Italy | Cross sectional | PREPS, PSS, GAD-7, PHQ-2, OCD Screening | 258 | 32.5 (SD = 5.12) | NR | 32.6% reported clinically relevant anxiety levels and 11.2% was positive for OCD problems. Pandemic-related stress predicts the development of anxiety, depressive, and obsessive-compulsive symptoms. | The COVID-19 pandemic onset contributed to poor mental health, especially anxiety among Italian pregnant women | 5/10 |
| Preis et al., 2020 [54] | USA | Cross sectional | Questionnaire: PREPS | 4451 | 30.8 (SD = 4.7) | 27 | Prenatal preparation stress: 27.2% Prenatal risk stress: 29.1%. | Having access to open spaces, not canceling prenatal appointments and leading a healthy life protect against stress | 5/10 |
| Chaves et al., 2021 [55] | Spain | Cross sectional | Questionnaire: EPDS and PANAS | N = 450 pregnancy, N = 274 postpartum | 33.36 (SD = 4.12) | NR | Total EPDS: 12 (SD = 5.19); EPDS-Anxiety: 7.36 (SD = 2.47); PANAS Positive: 28.71 (SD = 6.81); PANAS Negative: 22.61 (SD = 7.18). | 58% and 51% of women reported depressive and anxiety symptoms respectively. | 2/10 |
| Davenport et al., 2020 [56] | Canada | Cross sectional | EPDS, STAI-State | N = 520 pregnancy, N = 380 postpartum | 33 (SD = 8) | NR | Pre-pandemia vs. Pandemia: EPDS: 7.5 ± 4.9 vs. 11.2 ± 6.3; STAI = 34.5 ± 11.4 vs. 48.1 ± 13.6 | 40.7% and 72% of women reported an indicative of depression and moderate to high anxiety respectively. | 3/10 |
| Mappa et al., 2020 [57] | Italy | Cross sectional | STAI-T | 200 | 33 (IQR 30–36) | 18 (IQR 15–23) | STAI-T: 37 (IQR 20–43) STAI-T ≥ 40: 38.2% CI 31.3–45.5) | COVID 19 induced a significant increase in maternal anxiety | 3/10 |
| Saccone et al., 2020 [58] | Italy | Cross sectional | STAI, IES-R | 100 | IES-R: 36.9 (10.1), STAI 45.2 (14.6) | COVID-19 outbreak had a moderate to severe psychological impact on pregnant women. | 3/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campos-Garzón, C.; Riquelme-Gallego, B.; de la Torre-Luque, A.; Caparrós-González, R.A. Psychological Impact of the COVID-19 Pandemic on Pregnant Women: A Scoping Review. Behav. Sci. 2021, 11, 181. https://doi.org/10.3390/bs11120181
Campos-Garzón C, Riquelme-Gallego B, de la Torre-Luque A, Caparrós-González RA. Psychological Impact of the COVID-19 Pandemic on Pregnant Women: A Scoping Review. Behavioral Sciences. 2021; 11(12):181. https://doi.org/10.3390/bs11120181
Chicago/Turabian StyleCampos-Garzón, Celia, Blanca Riquelme-Gallego, Alejandro de la Torre-Luque, and Rafael A. Caparrós-González. 2021. "Psychological Impact of the COVID-19 Pandemic on Pregnant Women: A Scoping Review" Behavioral Sciences 11, no. 12: 181. https://doi.org/10.3390/bs11120181
APA StyleCampos-Garzón, C., Riquelme-Gallego, B., de la Torre-Luque, A., & Caparrós-González, R. A. (2021). Psychological Impact of the COVID-19 Pandemic on Pregnant Women: A Scoping Review. Behavioral Sciences, 11(12), 181. https://doi.org/10.3390/bs11120181