
The Natural Course of Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, and Mycoplasma genitalium in Pregnant and Post-Delivery Women in Pemba Island, Tanzania

 ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Population Characteristics
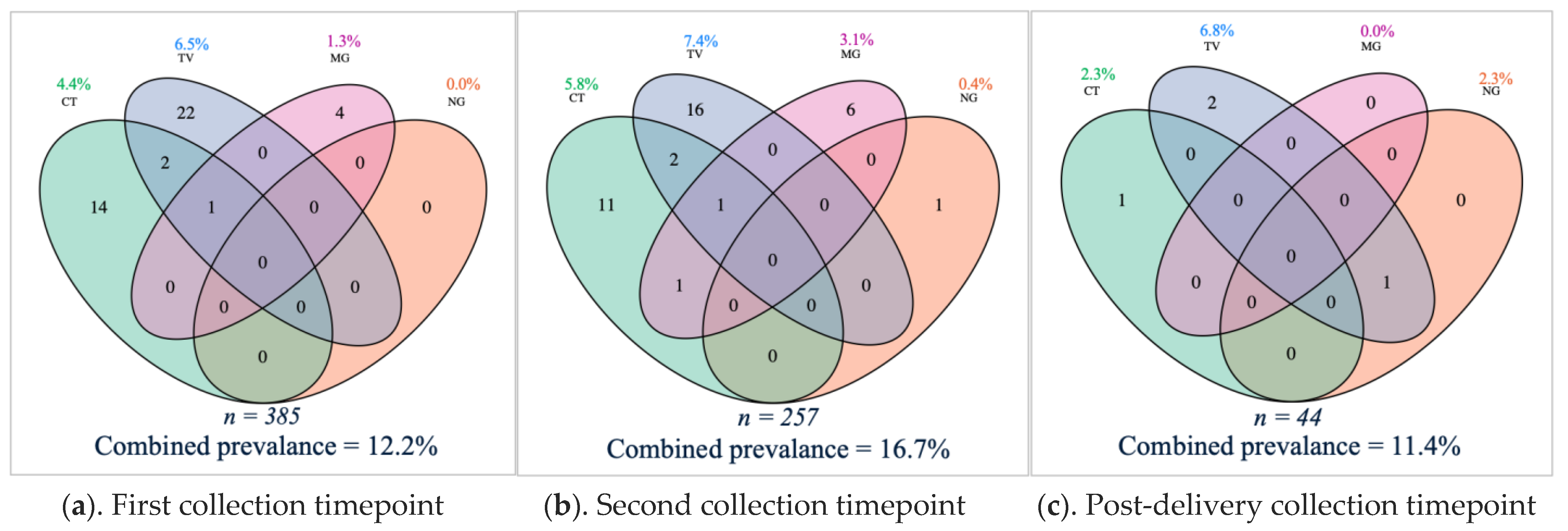
3.2. Sexually Transmitted Infections Prevalence and Symptomatology
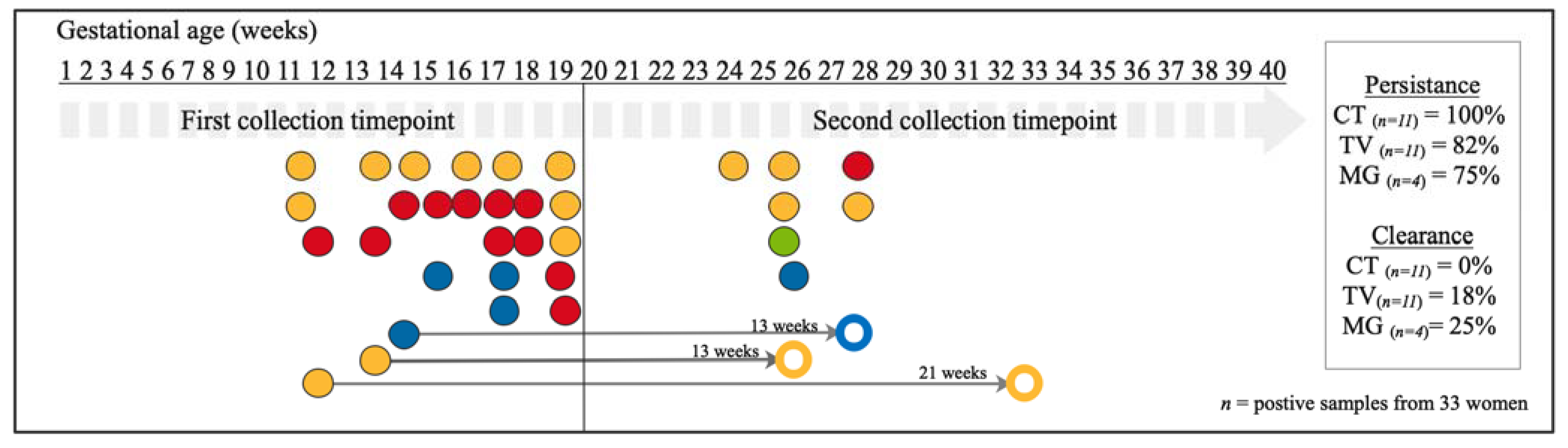
3.3. Sexually Transmitted Infections Persistence and Clearance during Pregnancy
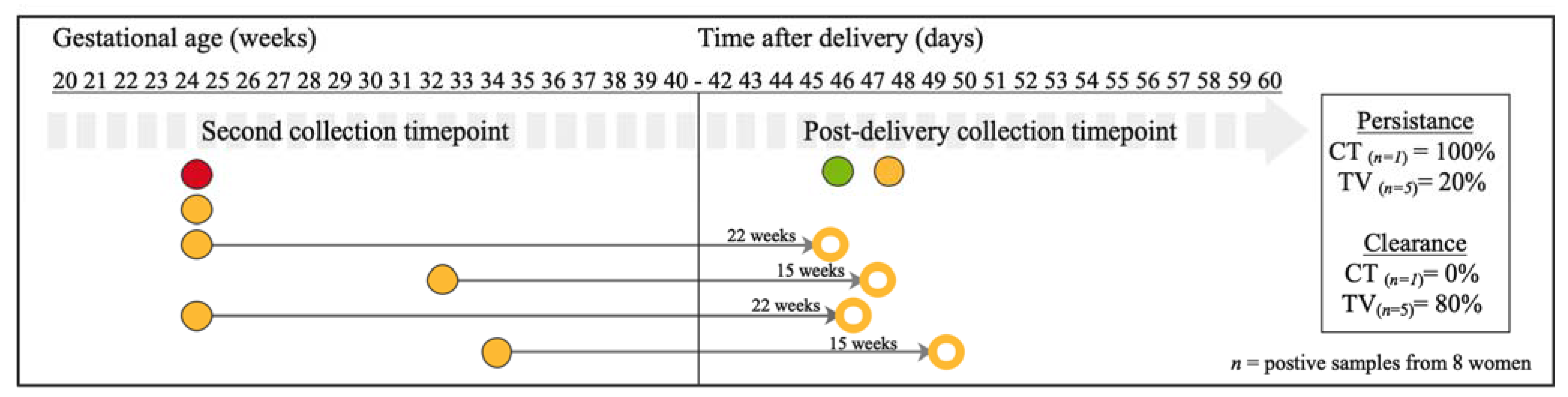
3.4. Sexually Transmitted Infections Persistence and Clearance after Pregnancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Newman, L.; Rowley, J.; Vander Hoorn, S.; Wijesooriya, N.S.; Unemo, M.; Low, N.; Stevens, G.; Gottlieb, S.; Kiarie, J.; Temmerman, M. Global estimates of the prevalence and incidence of four curable sexually transmitted infections in 2012 based on systematic review and global reporting. PLoS ONE 2015, 10, e0143304. [Google Scholar] [CrossRef] [PubMed]
- Adachi, K.; Nielsen-Saines, K.; Klausner, J.D. Chlamydia trachomatis infection in pregnancy: The global challenge of preventing adverse pregnancy and infant outcomes in Sub-Saharan Africa and Asia. Biomed. Res. Int. 2016, 2016, 9315757. [Google Scholar] [CrossRef] [PubMed]
- Rowley, J.; Vander Hoorn, S.; Korenromp, E.; Low, N.; Unemo, M.; Abu-Raddad, L.J.; Chico, R.M.; Smolak, A.; Newman, L.; Gottlieb, S.; et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: Global prevalence and incidence estimates. Bull. World Health Organ. 2019, 97, 548. [Google Scholar] [CrossRef]
- Nodjikouambaye, Z.A.; Compain, F.; Sadjoli, D.; Mboumba Bouassa, R.S.; Péré, H.; Veyer, D.; Robin, L.; Adawaye, C.; Tonen-Wolyec, S.; Moussa, A.M.; et al. Accuracy of curable sexually transmitted infections and genital mycoplasmas screening by multiplex real-time PCR using a self-collected veil among adult women in Sub-Saharan Africa. Infect. Dis. Obstet. Gynecol. 2019, 2019, 15. [Google Scholar] [CrossRef]
- Taylor-Robinson, D.; Lamont, R. Mycoplasmas in pregnancy. BJOG An. Int. J. Obstet. Gynaecol. 2011, 118, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Creighton, S. Gonorrhoea. BMJ Clin. Evid. 2014, 2014, 1604. [Google Scholar]
- Watson-Jones, D.; Weiss, H.A.; Changalucha, J.M.; Todd, J.; Gumodoka, B.; Bulmer, J.; Balira, R.; Ross, D.; Mugeye, K.; Hayes, R.; et al. Adverse birth outcomes in United Republic of Tanzania—Impact and prevention of maternal risk factors. Bull. World Health Organ. 2007, 85, 9–18. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Desmyter, J.; De Wet, D.H.; Van Assche, F.A. The association of gonorrhoea and syphilis with premature birth and low birthweight. Genitourin. Med. 1993, 69, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Gravett, M.G.; Nelson, H.P.; Derouen, T.; Critchlow, C.; Eschenbach, D.A.; Holmes, K.K. Independent associations of bacterial vaginosis and Chlamydia trachomatis infection with adverse pregnancy outcome. JAMA J. Am. Med. Assoc. 1986, 256, 1899–1903. [Google Scholar] [CrossRef]
- Cotch, M.F.; Pastorek, J.G.; Nugent, R.P.; Hillier, S.L.; Gibbs, R.S.; Martin, D.H.; Eschenbach, D.A.; Edelman, R.; Carey, J.C.; Regan, J.A.; et al. Trichomonas vaginalis associated with low birth weight and preterm delivery. The vaginal infections and prematurity study group. Sex. Transm. Dis. 1997, 24, 353–360. [Google Scholar] [CrossRef]
- Heumann, C.L.; Quilter, L.A.S.; Eastment, M.C.; Heffron, R.; Hawes, S.E. Adverse birth outcomes and maternal Neisseria gonorrhoeae infection: A population-based cohort study in Washington State. Sex. Transm. Dis. 2017, 44, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Martius, J.; Krohn, M.A.; Millier, S.L.; Stamm, W.E.; Holmes, K.K.; Eschenbach, D.A. Relationships of vaginal lactobacillus species, cervical Chlamydia trachomatis, and bacterial vaginosis to preterm birth. Obstet. Gynecol. 1988, 71, 89–95. [Google Scholar]
- Dubbink, J.H.; De Waaij, D.J.; Bos, M.; Van Der Eem, L.; Bébéar, C.; Mbambazela, N.; Ouburg, S.; Peters, R.P.H.; Morré, S.A. Microbiological characteristics of chlamydia trachomatis and neisseria gonorrhoeae infections in South African women. J. Clin. Microbiol. 2016, 54, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Geisler, W.M. Duration of untreated, uncomplicated Chlamydia trachomatis genital infection and factors associated with chlamydia resolution: A review of human studies. J. Infect. Dis. 2010, 201, 104–113. [Google Scholar] [CrossRef]
- Van Der Pol, B. Trichomonas vaginalis infection: The most prevalent nonviral sexually transmitted infection receives the least public health attention. Clin. Infect. Dis. 2007, 44, 23–25. [Google Scholar] [CrossRef]
- Stupiansky, N.W.; Van Der Pol, B.; Williams, J.A.; Weaver, B.; Taylor, S.E.; Fortenberry, J.D. The natural history of incident gonococcal infection in adolescent women. Sex. Transm. Dis. 2011, 38, 750–754. [Google Scholar] [CrossRef]
- Sheffield, J.S.; Andrews, W.W.; Klebanoff, M.A.; MacPherson, C.; Carey, J.C.; Ernest, J.M.; Wapner, R.J.; Trout, W.; Moawad, A.; Miodovnik, M.; et al. Spontaneous resolution of asymptomatic Chlamydia trachomatis in pregnancy. Obstet. Gynecol. 2005, 105, 557–562. [Google Scholar] [CrossRef]
- Vandepitte, J.; Weiss, H.A.; Kyakuwa, N.; Nakubulwa, S.; Muller, E.; Buvé, A.; Van Der Stuyft, P.; Hayes, R.; Grosskurth, H. Natural history of mycoplasma genitalium infection in a cohort of female sex workers in Kampala, Uganda. Sex. Transm. Dis. 2013, 40, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Bowden, F.J.; Garnett, G.P. Trichomonas vaginalis epidemiology: Parameterising and analysing a model of treatment interventions. Sex Transm Infect. 2000, 76, 248. [Google Scholar] [CrossRef]
- Van Der Pol, B.; Williams, J.A.; Orr, D.P.; Batteiger, B.E.; Fortenberry, J.D. Prevalence, incidence, natural history, and response to treatment of Trichomonas vaginalis infection among adolescent women. J. Infect. Dis. 2005, 192, 2039–2044. [Google Scholar] [CrossRef] [PubMed]
- Lovett, A.; Duncan, J.A. Human immune response and the natural history of neisseria gonorrhoeae infection. Front. Immunol. 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Molano, M.; Meijer, C.J.L.M.; Weiderpass, E.; Arslan, A.; Posso, H.; Franceschi, S.; Ronderos, M.; Muñoz, N.; Van Den Brule, A.J.C. The natural course of Chlamydia trachomatis infection in asymptomatic Colombian women: A 5-year follow-up study. J. Infect. Dis. 2005, 191, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Morré, S.A.; Van den Brule, A.J.C.; Rozendaal, L.; Boeke, A.J.P.; Voorhorst, F.J.; De Blok, S.; Meijer, C.J.L.M. The natural course of asymptomatic Chlamydia trachomatis infections: 45% Clearance and no development of clinical PID after one-year follow-up. Int. J. STD AIDS 2002, 13, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Cardenas, I. The immune system in pregnancy: A unique complexity. Am. J. Reprod. Immunol. 2010, 63, 425–433. [Google Scholar] [CrossRef]
- Robinson, D.P.; Klein, S.L. Pregnancy and pregnancy-associated hormones alter immune responses and disease pathogenesis. Horm. Behav. 2012, 62, 263–271. [Google Scholar] [CrossRef]
- Francis, S.C.; Ao, T.T.; Vanobberghen, F.M.; Chilongani, J.; Hashim, R.; Andreasen, A.; Watson-Jones, D.; Changalucha, J.; Kapiga, S.; Hayes, R.J. Epidemiology of curable sexually transmitted infections among women at increased risk for HIV in Northwestern Tanzania: Inadequacy of syndromic management. PLoS ONE 2014, 9, e101221. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Country Cooperation Strategy at a Glance: Tanzania (United Republic of); WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Ministry of Health Community Development Gender Elderly and Childeren (MoHCDGEC). Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015–2016. Available online: https://dhsprogram.com/pubs/pdf/FR321/FR321.pdf (accessed on 3 July 2020).
- Alliance for Maternal and Newborn Health Improvement; Baqui, A.H.; Khanam, R.; Rahman, M.S.; Ahmed, A.; Rahman, H.H.; Moin, M.I.; Ahmed, S.; Jehan, F.; Nisar, I.; et al. Understanding biological mechanisms underlying adverse birth outcomes in developing countries: Protocol for a prospective cohort (AMANHI bio-banking) study. J. Glob. Health 2017, 7, 021201. [Google Scholar]
- Ahmed, I.; Ali, S.M.; Amenga-Etego, S.; Ariff, S.; Bahl, R.; Baqui, A.H.; Begum, N.; Bhandari, N.; Bhatia, K.; Bhutta, Z.A.; et al. Population-based rates, timing, and causes of maternal deaths, stillbirths, and neonatal deaths in south Asia and sub-Saharan Africa: A multi-country prospective cohort study. Lancet Glob. Heal. 2018, 6, e1297–e1308. [Google Scholar] [CrossRef]
- Juliana, N.C.A.; Deb, S.; Ouburg, S.; Chauhan, A.; Pleijster, J.; Ali, S.M.; Morré, S.A.; Sazawal, S.; Ambrosino, E. The prevalence of chlamydia trachomatis and three other non-viral sexually transmitted infections among pregnant women in Pemba Island Tanzania. Pathogens 2020, 9, 625. [Google Scholar] [CrossRef]
- Dols, J.A.M.; Molenaar, D.; van der Helm, J.J.; Caspers, M.P.M.; de Angelino-Bart, A.K.; Schuren, F.H.J.; Speksnijder, A.G.C.L.; Westerhoff, H.V.; Richardus, J.H.; Boon, M.E.; et al. Molecular assessment of bacterial vaginosis by Lactobacillus abundance and species diversity. BMC Infect. Dis. 2016, 180, 1–8. [Google Scholar] [CrossRef]
- de Waaij, D.J.; Ouburg, S.; Dubbink, J.H.; Peters, R.P.H.; Morré, S.A. Evaluation of prestoplus assay and LightMix kit Trichomonas vaginalis assay for detection of Trichomonas vaginalis in dry vaginal swabs. J. Microbiol. Methods 2016, 127, 102–104. [Google Scholar] [CrossRef] [PubMed][Green Version]
- de Waaij, D.J.; Dubbink, J.H.; Peters, R.P.H.; Ouburg, S.; Morré, S.A. Comparison of GMT presto assay and Roche cobas® 4800 CT/NG assay for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in dry swabs. J. Microbiol. Methods 2015, 118, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Müller, E.E.; Venter, J.M.E.; Magooa, M.P.; Morrison, C.; Lewis, D.A.; Mavedzenge, S.N. Development of a rotor-gene real-time PCR assay for the detection and quantification of Mycoplasma genitalium. J. Microbiol. Methods 2012, 88, 311–315. [Google Scholar] [CrossRef]
- Golden, M.; Schillinger, J.; Markowitz, L. Duration of untreated genital infections with Chlamydia trachomatis: A review of the literature. Sex. Transm. Dis. 2000, 6, 329–337. [Google Scholar] [CrossRef]
- Masha, S.C.; Cools, P.; Descheemaeker, P.; Reynders, M.; Sanders, E.J.; Vaneechoutte, M. Urogenital pathogens, associated with Trichomonas vaginalis, among pregnant women in Kilifi, Kenya: A nested case-control study. BMC Infect. Dis. 2018, 18, 549. [Google Scholar] [CrossRef] [PubMed]
- van de Wijgert, J.H.H.M. The vaginal microbiome and sexually transmitted infections are interlinked: Consequences for treatment and prevention. PLoS Med. 2017, 2017. 14, e1002478. [Google Scholar] [CrossRef]
- Malogajski, J.; Brankovic, I.; Verweij, S.P.; Ambrosino, E.; Van Agtmael, M.A.; Brand, A.; Ouburg, S.; Morré, S.A. Translational potential into health care of basic genomic and genetic findings for human immunodeficiency virus, chlamydia trachomatis, and human papilloma virus. Biomed. Res. Int. 2013, 2013. [Google Scholar] [CrossRef]
- Serrano, M.G.; Parikh, H.I.; Brooks, J.P.; Edwards, D.J.; Arodz, T.J.; Edupuganti, L.; Huang, B.; Girerd, P.H.; Bokhari, Y.A.; Bradley, S.P.; et al. Racioethnic diversity in the dynamics of the vaginal microbiome during pregnancy. Nat. Med. 2019, 25, 1001–1011. [Google Scholar] [CrossRef]
- van de Wijgert, J.H.H.M.; Jespers, V. The global health impact of vaginal dysbiosis. Res. Microbiol. 2017. [Google Scholar] [CrossRef]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.K.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108, 4680–4687. [Google Scholar] [CrossRef]
- Romero, R.; Hassan, S.S.; Gajer, P.; Tarca, A.L.; Fadrosh, D.W.; Nikita, L.; Galuppi, M.; Lamont, R.F.; Chaemsaithong, P.; Miranda, J.; et al. The composition and stability of the vaginal microbiota of normal pregnant women is different from that of non-pregnant women. Microbiome 2014, 2, 4. [Google Scholar] [CrossRef]
- Howie, S.; Horner, P.; Horne, A. Chlamydia trachomatis infection during pregnancy—Known unknowns. Discov. Med. 2011, 12, 57–64. [Google Scholar]
- Gustafsson, C.; Mjösberg, J.; Matussek, A.; Geffers, R.; Matthiesen, L.; Berg, G.; Sharma, S.; Buer, J.; Ernerudh, J. Gene expression profiling of human decidual macrophages: Evidence for immunosuppressive phenotype. PLoS ONE 2008, 3, e2078. [Google Scholar] [CrossRef] [PubMed]
- Houser, B.L.; Tilburgs, T.; Hill, J.; Nicotra, M.L.; Strominger, J.L. Two unique human decidual macrophage populations. J. Immunol. 2011, 186, 2633–2642. [Google Scholar] [CrossRef] [PubMed]
- Szarka, A.; Rigó, J.; Lázár, L.; Beko, G.; Molvarec, A. Circulating cytokines, chemokines and adhesion molecules in normal pregnancy and preeclampsia determined by multiplex suspension array. BMC Immunol. 2010, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Mjösberg, J.; Berg, G.; Jenmalm, M.C.; Ernerudh, J. FOXP3+ regulatory T cells and T helper 1, T helper 2, and T helper 17 cells in human early pregnancy decidua. Biol. Reprod. 2010, 82, 698–705. [Google Scholar] [CrossRef]
- Witkin, S.S.; Linhares, I.M.; Bongiovanni, A.M.; Herway, C.; Skupski, D. Unique alterations in infection-induced immune activation during pregnancy. BJOG An. Int. J. Obstet. Gynaecol. 2011, 118, 145–153. [Google Scholar] [CrossRef]
- Erlebacher, A. Immune surveillance of the maternal/fetal interface: Controversies and implications. Trends Endocrinol. Metab. 2010, 21, 428–434. [Google Scholar] [CrossRef]
- Seavey, M.M.; Mosmann, T.R. Immunoregulation of fetal and anti-paternal immune responses. Immunol. Res. 2008, 40, 97–113. [Google Scholar] [CrossRef]
- Al-Nasiry, S.; Ambrosino, E.; Schlaepfer, M.; Morré, S.A.; Wieten, L.; Voncken, J.W.; Spinelli, M.; Mueller, M.; Kramer, B.W. The interplay between reproductive tract microbiota and immunological system in human reproduction. Front. Immunol. 2020, 11, 378. [Google Scholar] [CrossRef]
- Horne, A.W.; Stock, S.J.; King, A.E. Innate immunity and disorders of the female reproductive tract. Reproduction 2008, 135, 739–749. [Google Scholar] [CrossRef]
- Nobbenhuis, M.A.E.; Helmerhorst, T.J.M.; Van den Brule, A.J.C.; Rozendaal, L.; Bezemer, P.D.; Voorhorst, F.J.; Meijer, C.J.L.M. High-risk human papillomavirus clearance in pregnant women: Trends for lower clearance during pregnancy with a catch-up postpartum. Br. J. Cancer 2002, 87, 75–80. [Google Scholar] [CrossRef]
- Sethi, S.; Muller, M.; Schneider, A.; Blettner, M.; Smith, E.; Turek, L.; Wahrendorf, J.; Gissmann, L.; Chang-Claude, J. Serologic response to the E4, E6, and E7 proteins of human papillomavirus type 16 in pregnant women. Am. J. Obstet. Gynecol. 1998, 178, 360–364. [Google Scholar] [CrossRef]
- Contini, C.; Rotondo, J.C.; Seraceni, S.; Maritati, M. Investigation on Silent Bacterial Infections in Specimens from Pregnant Women Affected by Spontaneous Miscarriage. The role of chlamydia in ocular lymphoma view project silent intracellular infections during pregnancy view project. Artic. J. Cell. Physiol. 2018, 2018. 234, 100–107. [Google Scholar]
- Dukers-Muijrers, N.H.T.M.; Van Liere, G.A.F.S.; Wolffs, P.F.G.; Heijer, C.D.; Werner, M.I.L.S.; Hoebea, C.J.P.A. Antibiotic use before chlamydia and gonorrhea genital and extragenital screening in the sexually transmitted infection clinical setting. Antimicrob. Agents Chemother. 2015, 59, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Ginige, S.; Chen, M.Y.; Hocking, J.S.; Read, T.R.H.; Fairley, C.K. Antibiotic consumption and chlamydia prevalence in international studies. Sex. Health 2006, 3, 221–224. [Google Scholar] [CrossRef]
- Berg, E.; Benson, D.M.; Haraszkiewicz, P.; Grieb, J.; McDonald, J. High prevalence of sexually transmitted diseases in women with urinary infections. Acad. Emerg. Med. 1996, 3, 1030–1034. [Google Scholar] [CrossRef] [PubMed]
- Davey, D.L.J.; Shull, H.I.; Billings, J.D.; Wang, D.; Adachi, K.; Klausner, J.D. Prevalence of curable sexually transmitted infections in pregnant women in low–and middle-income countries from 2010 to 2015: A systematic review. Sex. Transm. Dis. 2016, 43, 450–458. [Google Scholar] [CrossRef]
- Seale, A.; Broutet, N.; Narasimhan, M. Assessing process, content, and politics in developing the global health sector strategy on sexually transmitted infections 2016–2021: Implementation opportunities for policymakers. PLoS Med. 2017, 14, e1002330. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for the Treatment of Chlamydia Trachomatis; WHO: Geneva, Switzerland, 2016; ISBN 978-9241549714. [Google Scholar]
- World Health Organization. Global Health Sector Strategy on Sexually Transmitted Infections 2016–2021; Towards Ending STIs. Report; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- WHO; UNICEF; UNFPA; World Bank Group; United Nations Population Division Global Health Observatory. Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030). Available online: https://www.who.int/reproductivehealth/publications/maternal-mortality-2000-2017/en/ (accessed on 27 July 2020).
- Jensen, J.S.; Bradshaw, C.S.; Tabrizi, S.N.; Fairley, C.K.; Hamasuna, R. Azithromycin treatment failure in Mycoplasma genitalium-positive patients with nongonococcal urethritis is associated with induced macrolide resistance. Clin. Infect. Dis. 2008, 47, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Ison, C.A.; Dillon, J.A.R.; Tapsall, J.W. The epidemiology of global antibiotic resistance among Neisseria gonorrhoeae and Haemophilus ducreyi. Lancet 1998, 351, 8–11. [Google Scholar] [CrossRef]
- Horner, P.J. Azithromycin antimicrobial resistance and genital Chlamydia trachomatis infection: Duration of therapy may be the key to improving efficacy. Sex. Transm. Infect. 2012, 88, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Stamm, L.V. Global challenge of antibiotic-resistant Treponema pallidum. Antimicrob. Agents Chemother. 2010, 54, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Krupp, K.; Madhivanan, P. Antibiotic resistance in prevalent bacterial and protozoan sexually transmitted infections. Indian J. Sex. Transm. Dis. AIDS 2015, 36, 3. [Google Scholar] [PubMed]



 are compared with two pregnancy studies (Sheffield et al.
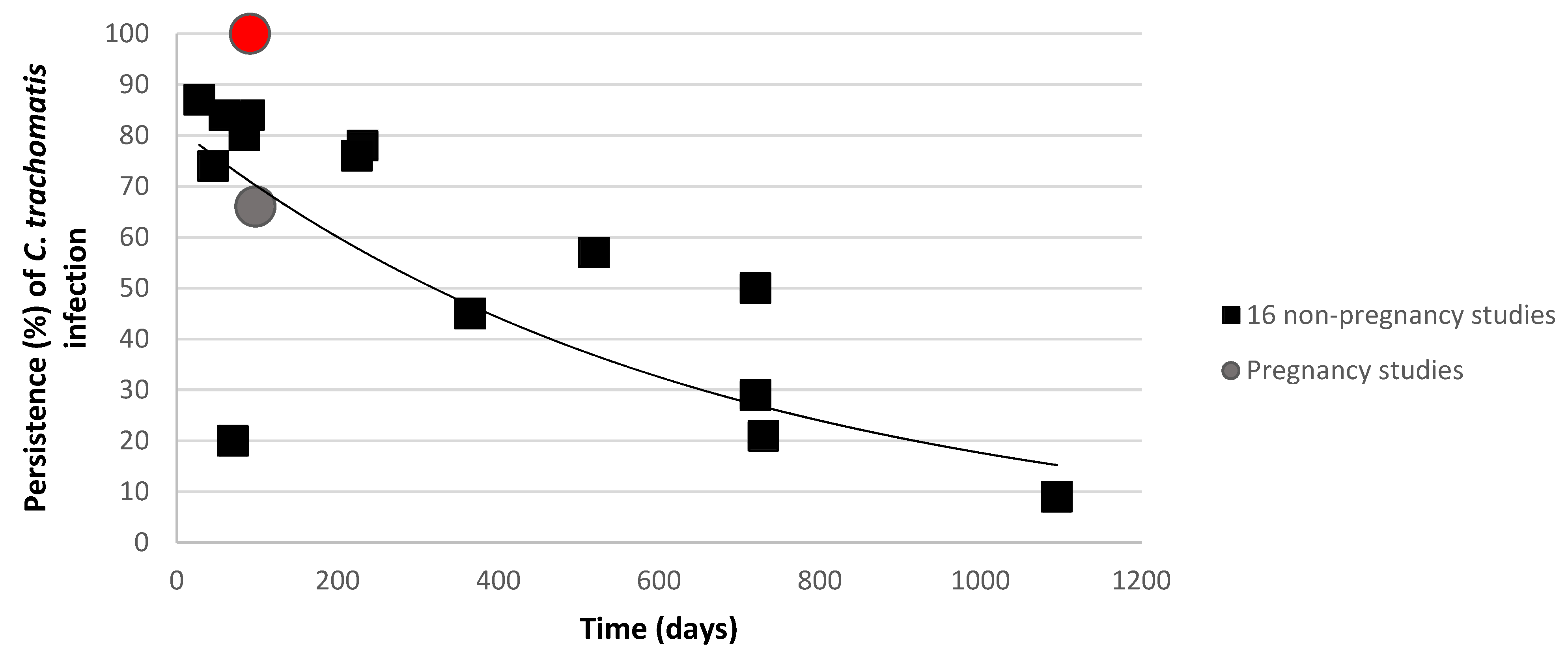
are compared with two pregnancy studies (Sheffield et al.  and the present study
and the present study  ) [14,17,36]. The curve shows the trend as calculated by the sixteen non-pregnant studies.
are compared with two pregnancy studies (Sheffield et al. and the present study ) [14,17,36]. The curve shows the trend as calculated by the sixteen non-pregnant studies.
) [14,17,36]. The curve shows the trend as calculated by the sixteen non-pregnant studies.
are compared with two pregnancy studies (Sheffield et al. and the present study ) [14,17,36]. The curve shows the trend as calculated by the sixteen non-pregnant studies.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juliana, N.C.A.; Omar, A.M.; Pleijster, J.; Aftab, F.; Uijldert, N.B.; Ali, S.M.; Ouburg, S.; Sazawal, S.; Morré, S.A.; Deb, S.; et al. The Natural Course of Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, and Mycoplasma genitalium in Pregnant and Post-Delivery Women in Pemba Island, Tanzania. Microorganisms 2021, 9, 1180. https://doi.org/10.3390/microorganisms9061180
Juliana NCA, Omar AM, Pleijster J, Aftab F, Uijldert NB, Ali SM, Ouburg S, Sazawal S, Morré SA, Deb S, et al. The Natural Course of Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, and Mycoplasma genitalium in Pregnant and Post-Delivery Women in Pemba Island, Tanzania. Microorganisms. 2021; 9(6):1180. https://doi.org/10.3390/microorganisms9061180
Chicago/Turabian StyleJuliana, Naomi C. A., Abdulla Mbaruk Omar, Jolein Pleijster, Fahad Aftab, Nina B. Uijldert, Said M. Ali, Sander Ouburg, Sunil Sazawal, Servaas A. Morré, Saikat Deb, and et al. 2021. "The Natural Course of Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, and Mycoplasma genitalium in Pregnant and Post-Delivery Women in Pemba Island, Tanzania" Microorganisms 9, no. 6: 1180. https://doi.org/10.3390/microorganisms9061180
APA StyleJuliana, N. C. A., Omar, A. M., Pleijster, J., Aftab, F., Uijldert, N. B., Ali, S. M., Ouburg, S., Sazawal, S., Morré, S. A., Deb, S., & Ambrosino, E. (2021). The Natural Course of Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, and Mycoplasma genitalium in Pregnant and Post-Delivery Women in Pemba Island, Tanzania. Microorganisms, 9(6), 1180. https://doi.org/10.3390/microorganisms9061180