Switching to Integrase Inhibitors Unlinked to Weight Increase in Perinatally HIV-Infected Young Adults and Adolescents: A 10-Year Observational Study

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
3. Statistical Methods
4. Results
4.1. Weight Gain in the Whole Study Population
4.2. Comparison of Weight Change in INSTI vs. Non-INSTI-Treated Patients
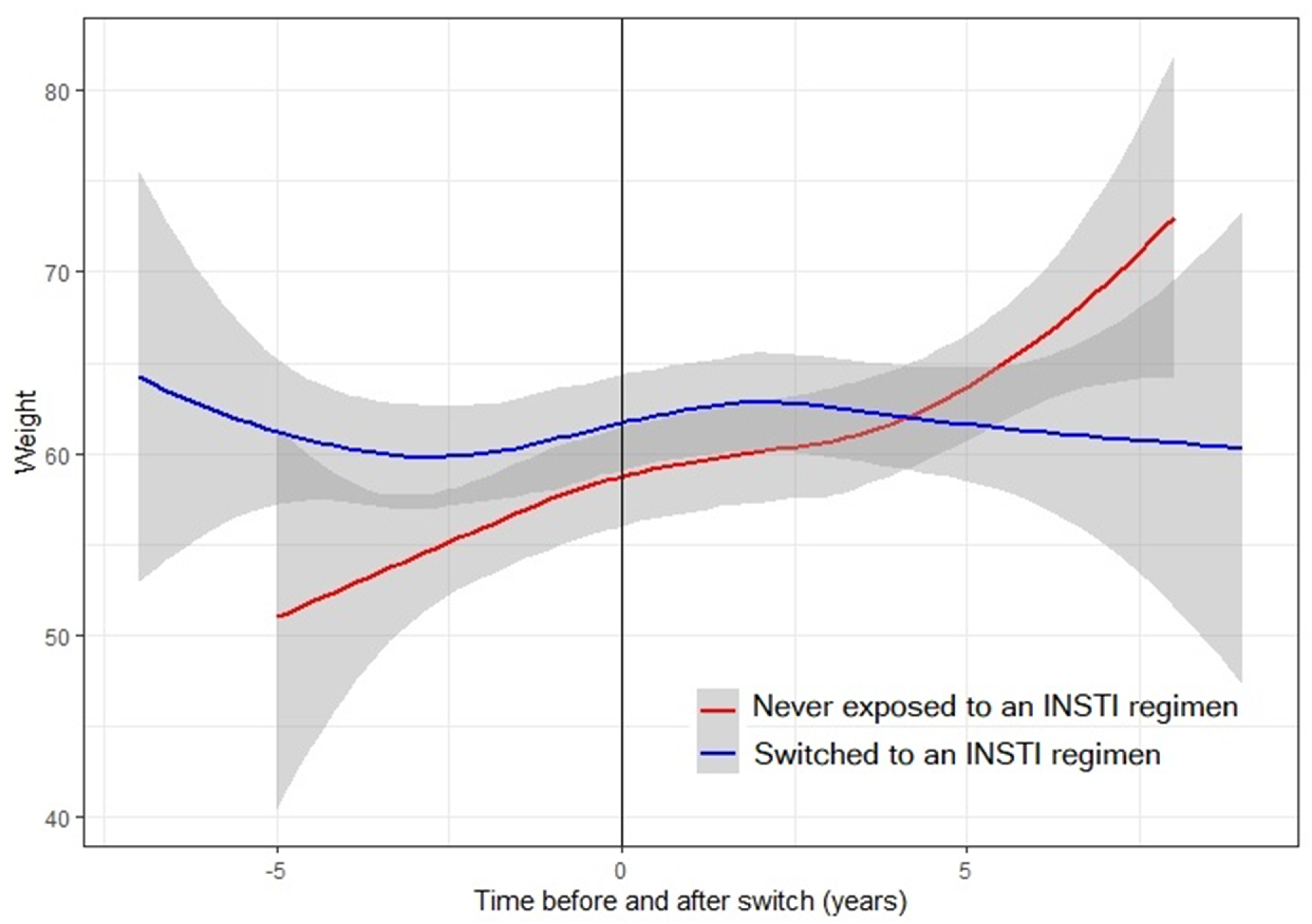
4.3. Trend of Weight in INSTI Treated Patients
5. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Taramasso, L.; Ricci, E.; Menzaghi, B.; Orofino, G.; Passerini, S.; Madeddu, G.; Martinelli, C.V.; De Socio, G.V.; Squillace, N.; Rusconi, S.; et al. Weight Gain: A Possible Side Effect of All Antiretrovirals. Open Forum Infect. Dis. 2017, 4, ofx239. [Google Scholar] [CrossRef] [PubMed]
- Erlandson, K.M.; Kitch, U.; Tierney, C.; Sax, P.E.; Daar, E.S.; Tebas, P.; Melbourne, K.; Ha, B.; Jahed, N.C.; Mccomsey, G.A. Weight and lean body mass change with antiretroviral initiation and impact on bone mineral density. AIDS 2013, 27, 2069–2079. [Google Scholar] [CrossRef] [PubMed]
- Bourgi, K.; Rebeiro, P.F.; Turner, M.; Castilho, J.L.; Hulgan, T.; Raffanti, S.P.; Koethe, J.R.; Sterling, T.R. Greater Weight Gain in Treatment Naïve Persons Starting Dolutegravir-Based Antiretroviral Therapy. Clin. Infect. Dis. 2019, 70, 1267–1274. [Google Scholar] [CrossRef]
- NAMSAL ANRS 12313 Study Group; Kouanfack, C.; Mpoudi-Etame, M.; Bassega, P.O.; Eymard-Duvernay, S.; Leroy, S.; Boyer, S.; Peeters, M.; Calmy, A.; Delaporte, E.; et al. Dolutegravir-Based or Low-Dose Efavirenz-Based Regimen for the Treatment of HIV-1. N. Engl. J. Med. 2019, 381, 816–826. [Google Scholar] [CrossRef]
- Venter, W.D.F.; Moorhouse, M.; Sokhela, S.; Fairlie, L.; Mashabane, N.; Masenya, M.; Serenata, C.; Akpomiemie, G.; Qavi, A.; Chandiwana, N.; et al. Dolutegravir plus Two Different Prodrugs of Tenofovir to Treat HIV. N. Engl. J. Med. 2019, 381, 803–815. [Google Scholar] [CrossRef] [PubMed]
- Bourgi, K.; Jenkins, C.A.; Rebeiro, P.F.; Lake, J.E.; Moore, R.D.; Mathews, W.C. Greater weight gain among treatment-naïve persons starting integrase inhibtors. J. Int. AIDS Soc. 2020, 23, e25484. [Google Scholar] [CrossRef]
- Kerchberger, A.M.; Sheth, A.N.; Angert, C.D.; Mehta, C.C.; A Summers, N.; Ofotokun, I.; Gustafson, D.; Weiser, S.D.; Sharma, A.; Adimora, A.; et al. Weight Gain Associated with Integrase Stand Transfer Inhibitor Use in Women. Clin. Infect. Dis. 2019, ciz853. [Google Scholar] [CrossRef]
- Lake, J.E.; Wu, K.; Erlandson, K.M.; Bares, S.H.; Debroy, P.; Godfrey, C. Risk factors for excess weight gain following switch to integrase inhibitor-based antiretroviral Therapy. Clin. Infect. Dis. 2020, ciaa177. [Google Scholar] [CrossRef]
- Mccomsey, G.A.; Eron, J.J.; Santiago, S.; Mounzer, K.; Moyle, G.; Vanig, T. Weight gain during treatment among 3468 treatment-experienced adults with HIV. In Proceedings of the Conference on Retroviruses and Opportunistic Infections (CROI), Seattle, WA, USA, 4–7 March 2019. [Google Scholar]
- Williams, D.W.; Elahi, S. Profound immune consequences for young adults infected with HIV perinatally or during childhood. AIDS 2019, 33, 2251–2252. [Google Scholar] [CrossRef]
- Fastenackels, S.; Sauce, D.; Vigouroux, C.; Avettand-Fènoël, V.; Bastard, J.-P.; Fellahi, S.; Nailler, L.; Arezes, E.; Rouzioux, C.; Warszawski, J.; et al. HIV-mediated immune aging in young adults infected perinatally or during childhood. AIDS 2019, 33, 1705–1710. [Google Scholar] [CrossRef]
- Horvath, S.; Stein, D.J.; Phillips, N.J.; Heany, S.J.; Kobor, M.S.; Lin, D.T.; Myer, L.; Zar, H.J.; Levine, A.J.; Hoare, J. Perinatally acquired HIV infection accelerates epigenetic aging in South African adolescents. AIDS 2018, 32, 1465–1474. [Google Scholar] [CrossRef] [PubMed]
- Chiappini, E.; Bianconi, M.; Dalzini, A.; Petrara, M.R.; Galli, L.; Giaquinto, C.; De Rossi, A. Accelerated aging in perinatally HIV-infected children: Clinical manifestations and pathogenetic mechanisms. Aging 2018, 10, 3610–3625. [Google Scholar] [CrossRef] [PubMed]
- Padmapriyadarsini, C.; Shet, A.; Srinivasan, R.; Ramachandran, G.; Sanjeeva, G.N.; Devi, P.; Ramesh, K.; Bhavani, P.K.; Reddy, D.; Suresh, E.; et al. High Prevalence of Lipid Abnormalities and Insulin Resistance Among Antiretroviral Naïve HIV-infected Children in India. Pediatr. Infect. Dis. J. 2018, 37, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Alam, N.; Cortina-Borja, M.; Goetghebuer, T.; Marczyńska-Stolarek, M.; Vigano, A.; Thorne, C.; European Paediatric HIV and Lipodystrophy Study Group in EuroCoord. Body fat abnormality in HIV-infected children and adolescents living in Europe: Prevalence and risk factors. JAIDS J. Acquir. Immune Defic. Syndr. 2012, 59, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Dapena, M.; Jiménez, B.; Noguera-Julian, A.; Soler-Palacín, P.; Fortuny, C.; Lahoz, R.; Aracil, F.J.; Figueras, C.; De José, M.I. Metabolic disorders in vertically HIV-infected children: Future adults at risk for cardiovascular disease. J. Pediatr. Endocrinol. Metab. 2012, 25, 529–535. [Google Scholar] [CrossRef]
- Pantelic, M.; Casale, M.; Cluver, L.; Toska, E.; Moshabela, M. Multiple forms of discrimination and internalized stigma compromise retention in HIV care among adolescents: Findings from a South African cohort. J. Int. AIDS Soc. 2020, 23, e25488. [Google Scholar] [CrossRef]
- Ungaro, R.; Taramasso, L.; Bruzzone, B.; Vicenti, I.; Galli, L.; Borghi, V.; Francisci, D.; Pecorari, M.; Zoncada, A.; Callegaro, A.P.; et al. Prevalence of acquired resistance mutations in a large cohort of perinatally infected HIV-1 patients. Clin. Microbiol. Infect. 2019, 25, 1443–1446. [Google Scholar] [CrossRef]
- Dirajlal-Fargo, S.; Shan, L.; Sattar, A.; Bowman, E.; Gabriel, J.; Kulkarni, M.; Funderburg, N.; Nazzinda, R.; Musiime, V.; Mccomsey, G.A. Insulin resistance and intestinal integrity in children with and without HIV infection in Uganda. HIV Med. 2019, 21, 119–127. [Google Scholar] [CrossRef]
- Viganò, A.; Zuccotti, G.V.; Cerini, C.; Stucchi, S.; Puzzovio, M.; Giacomet, V.; Mora, S. Lipodystrophy, insulin resistance, and adiponectin concentration in HIV-infected children and adolescents. Curr. HIV Res. 2011, 9, 321–326. [Google Scholar] [CrossRef]
- Taramasso, L.; Di Biagio, A.; Riccardi, N.; Briano, F.; Di Filippo, E.; Comi, L.; Mora, S.; Giacomini, M.; Gori, A.; Maggiolo, F. Lipid profile changings after switching from rilpivirine/tenofovir disoproxil fumarate/emtricitabine to rilpivirine/tenofovir alafenamide/emtricitabine: Different effects in patients with or without baseline hypercholesterolemia. PLoS ONE 2019, 14, e0223181. [Google Scholar] [CrossRef]
- Tassiopoulos, K.; Williams, P.L.; Seage, G.R.; Crain, M.; Oleske, J.; Farley, J.; International Maternal Pediatric Adolescent AIDS Clinical Trials 219C Team. Association of Hypercholesterolemia Incidence With Antiretroviral Treatment, Including Protease Inhibitors, Among Perinatally HIV-Infected Children. J. Acquir. Immune Defic. Syndr. 2008, 47, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Rosso, R.; Di Biagio, A.; Maggiolo, F.; Nulvesu, L.; Callegaro, A.P.; Taramasso, L.; Bruzzone, B.; Viscoli, C. Patient-reported outcomes and low-level residual HIV-RNA in adolescents perinatally infected with HIV-1 after switching to one-pill fixed-dose regimen. AIDS Care 2011, 24, 54–58. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Fraccaro, P.; Pupella, V.; Gazzarata, R.; Dentone, C.; Cenderello, G.; De Leo, P.; Bozzano, F.; Finocchio, G.C.; De Maria, A.; Fenoglio, D.; et al. The ligurian human immunodeficiency virus clinical network: A web tool to manage patients with human immunodeficiency virus in primary care and multicenter clinical trials. Med 2 0. 2013, 2, e5. [Google Scholar] [CrossRef] [PubMed]
- The European Pregnancy and Paediatric HIV Cohort Collaboration (EPPICC) Study Group; European Pregnancy and Paediatric HIV Cohort Collaboration (EPPICC) study group; Crichton, S.; Belfrage, E.; Collins, I.J.; Doerholt, K.; Judd, A.; Le Coeur, S.; Spoulou, V.; Scherpbier, H.; et al. Height and timing of growth spurt during puberty in young people living with vertically acquired HIV in Europe and Thailand. AIDS 2019, 33, 1897–1910. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Growth Reference 5–19 Years. Available online: https://www.who.int/growthref/who2007_height_for_age/en/ (accessed on 15 April 2020).
- Malhotra, R.; Østbye, T.; Riley, C.M.; Finkelstein, E.A. Young adult weight trajectories through midlife by body mass category. Obesity 2013, 21, 1923–1934. [Google Scholar] [CrossRef] [PubMed]
- Sax, P.; Erlandson, K.M.; Lake, J.; McComsey, G.; Orkin, C.; Esser, S.; Brown, T.T.; Rockstroh, J.K.; Wei, X.; Carter, C.; et al. Weight Gain Following Initiation of Antiretroviral Therapy: Risk Factors in Randomized Comparative Clinical Trials. Clin. Infect. Dis. 2019, 32, 1–32. [Google Scholar] [CrossRef]
- Taramasso, L.; Berruti, M.; Briano, F.; Di Biagio, A. The Switch from TDF to TAF Determines Weight Gain in Patients on Rilpivirine-Based Regimen. AIDS 2020, 34, 877–881. [Google Scholar] [CrossRef]
- Menard, A.; Meddeb, L.; Tissot-Dupont, H.; Ravaux, I.; Dhiver, C.; Mokhtari, S.; Tomei, C.; Brouqui, P.; Colson, P.; Stein, A. Dolutegravir and weight gain. AIDS 2017, 31, 1499–1500. [Google Scholar] [CrossRef]
- Seidell, J.; Visscher, T. Body weight and weight change and their health implications for the elderly. Eur. J. Clin. Nutr. 2000, 54, S33–S39. [Google Scholar] [CrossRef]
- Yarnell, J.W.G.; Patterson, C.C.; Thomas, H.F.; Sweetnam, P.M. Comparison of weight in middle age, weight at 18 years, and weight change between, in predicting subsequent 14 year mortality and coronary events: Caerphilly Prospective Study. J. Epidemiol. Community Health 2000, 54, 344–348. [Google Scholar] [CrossRef]
- Miller, T.L.; Orav, E.J.; Lipshultz, S.E.; Arheart, K.L.; Duggan, C.; Weinberg, G.A.; Bechard, L.; Furuta, L.; Nicchitta, J.; Gorbach, S.L.; et al. Risk Factors for Cardiovascular Disease in Children Infected with Human Immunodeficiency Virus-1. J. Pediatr. 2008, 153, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Sharma, T.S.; Somarriba, G.; Arheart, K.L.; Neri, D.A.; Mathew, M.S.; Graham, P.L.; Scott, G.B.; Miller, T.L. Longitudinal Changes in Body Composition by Dual-energy Radiograph Absorptiometry Among Perinatally HIV-infected and HIV-uninfected Youth. Pediatr. Infect. Dis. J. 2018, 37, 1002–1007. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.E.; Stirrup, O.; Dunn, D.; Runcie-Unger, I.; Milinkovic, A.; Candfield, S.; Lukha, H.; Severn, A.; Waters, L.; Edwards, S.; et al. No overall change in the rate of weight gain after switching to an integrase-inhibitor in virologically suppressed adults with HIV. AIDS 2020, 34, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Taramasso, L.; Bonfanti, P.; Ricci, E.; Orofino, G.; Squillace, N.; Menzaghi, B.; De Socio, G.V.; Madeddu, G.; Pellicanò, G.F.; Pagnucco, L.; et al. Factors associated with weight gain in people treated with dolutegravir. Open Forum Infect. Dis. 2020, ofaa195. [Google Scholar] [CrossRef]
- Liu, Y.; Galárraga, O. Do national drug policies influence antiretroviral drug prices? Evidence from the Southern African Development community. Heal. Policy Plan. 2016, 32, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Iyun, V.; Technau, K.-G.; Eley, B.; Rabie, H.; Boulle, A.; Fatti, G.; Egger, M.; Tanser, F.; Wood, R.; Fairlie, L.; et al. Earlier Antiretroviral Therapy Initiation and Decreasing Mortality Among HIV-infected Infants Initiating Antiretroviral Therapy Within 3 Months of Age in South Africa, 2006–2017. Pediatr. Infect. Dis. J. 2020, 39, 127–133. [Google Scholar] [CrossRef]
- Di Biagio, A.; Taramasso, L.; Gustinetti, G.; Burastero, G.; Giacomet, V.; La Rovere, D.; Genovese, O.; Giaquinto, C.; Rampon, O.; Carloni, I.; et al. Missed opportunities to prevent mother-to-child transmission of HIV in Italy. HIV Med. 2019, 20, 330–336. [Google Scholar] [CrossRef]


{kind=link}
| Variables | All Patients | INSTI Group | Non-INSTI Group | p-Value |
|---|---|---|---|---|
| Number of patients (%) | 66 (100) | 45 (68.18) | 21 (31.82) | |
| Mean Age (±SD), years | 26.67 (±4.79) | 26.53 (±4.79) | 26.95 (±4.90) | 0.853 |
| Male Gender (%) | 33 (50.00) | 23 (51.11) | 10 (47.62) | 0.792 |
| Mean weight (±SD), kg | 58.65 (12.51) | 59.63 (13.66) | 56.56 (9.54) | 0.711 |
| Caucasian ethnicity | 61 (92.42) | 42 (93.33) | 19 (90.48) | 0.683 |
| Mean Born weight (±SD), grams | 2863.40 (±725.64) N = 47 | 2845.15 (±636.62) N = 33 | 2906.43 (±928.83) N = 14 | 0.972 |
| Mean CD4+T-cell count, cells/mm3 (at last clinical evaluation) | 817.68 (±335.21) N = 65 | 770.98 (±348.18) N = 44 | 915.52 (±289.94) | 0.059 |
| Weight Change in kg/Year | All Patients * (N = 66) | Female ** (N = 33) | Male ** (N = 33) |
|---|---|---|---|
| Pre-T0 (p-value) | +0.47 (0.14–0.77) (0.006) | +0.52 (0.08–0.95) (0.020) | +0.42 (−0.06–0.91) (0.126) |
| Post-T0 (p-value) | +0.77 (0.44–1.10) (<0.0001) | +0.97 (0.54–1.41) (<0.0001) | +0.57 (0.09–1.06) (0.086) |
| Pre-post Difference (p-value) | +0.30 (−0.16–0.77) (0.200) | +0.46 (−0.16–1.07) (0.141) | +0.15 (−0.54–0.84) (0.660) |
| Weight Change in kg/Year | Non-INSTI Group * (N = 21) | INSTI Group * (N = 45) |
|---|---|---|
| Pre-T0 (p-value) | +0.38 (−0.21–0.97) (0.204) | +0.51 (0.11–0.91) (0.014) |
| Post- T0 (p-value) | +0.74 (0.15–1.34) (<.0001) | +0.79 (0.38–1.19) (0.0002) |
| Pre-post Difference (p-value) | +0.36 (−0.47–1.20) (0.391) | +0.28 (−0.29–0.85) (0.338) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taramasso, L.; Di Biagio, A.; Bovis, F.; Forlanini, F.; Albani, E.; Papaioannu, R.; Giacomet, V. Switching to Integrase Inhibitors Unlinked to Weight Increase in Perinatally HIV-Infected Young Adults and Adolescents: A 10-Year Observational Study. Microorganisms 2020, 8, 864. https://doi.org/10.3390/microorganisms8060864
Taramasso L, Di Biagio A, Bovis F, Forlanini F, Albani E, Papaioannu R, Giacomet V. Switching to Integrase Inhibitors Unlinked to Weight Increase in Perinatally HIV-Infected Young Adults and Adolescents: A 10-Year Observational Study. Microorganisms. 2020; 8(6):864. https://doi.org/10.3390/microorganisms8060864
Chicago/Turabian StyleTaramasso, Lucia, Antonio Di Biagio, Francesca Bovis, Federica Forlanini, Elena Albani, Rebecka Papaioannu, and Vania Giacomet. 2020. "Switching to Integrase Inhibitors Unlinked to Weight Increase in Perinatally HIV-Infected Young Adults and Adolescents: A 10-Year Observational Study" Microorganisms 8, no. 6: 864. https://doi.org/10.3390/microorganisms8060864
APA StyleTaramasso, L., Di Biagio, A., Bovis, F., Forlanini, F., Albani, E., Papaioannu, R., & Giacomet, V. (2020). Switching to Integrase Inhibitors Unlinked to Weight Increase in Perinatally HIV-Infected Young Adults and Adolescents: A 10-Year Observational Study. Microorganisms, 8(6), 864. https://doi.org/10.3390/microorganisms8060864