Abstract
Candida spp. are ubiquitous yeasts that are part of most mammals’ microbiota and can become opportunistic pathogens under predisposing conditions. Interestingly, recent studies in human medicine report an increased abundance of Candida spp. in association with inflammatory bowel disease (IBD). Gastrointestinal candidiasis has been primarily reported in neonatal foals, but not in adult horses. The aim of this study is to describe the morphological, histopathological, and microbiological features of gastric lesions associated with Candida infiltration in five horses referred to two tertiary hospitals for different reasons. Clinical features, findings from gastroscopy, gastric, and duodenal biopsies, as well as fungal and bacterial cultures obtained from gastric lesions will be reported. Macroscopically, gastric lesions showed a characteristic yellow/white pseudo-membranous appearance, similar to lesions reported in foals. The presence of Candida spp. was confirmed by positive culture and/or histopathological evidence of fungal infiltration on the gastric epithelium. Three out of five horses showed histopathological changes in duodenal biopsies, potentially suggesting IBD. These results demonstrate that gastric candidiasis can occur in adult horses. Further research is needed to elucidate the pathogenesis, predisposing factors, and clinical relevance of Candida spp. infections in the equine stomach, as well as their potential impact on gastrointestinal health and overall performance.
Keywords:
equine; Candida; stomach; yeast; gastrointestinal; colic; ulcer; omeprazole; inflammatory bowel disease; microbiota 1. Introduction
Candida spp. are ubiquitous yeasts that naturally colonize the skin and mucosal surfaces of the gastrointestinal, upper respiratory, and lower urogenital tracts in most mammals [1,2]. Under normal conditions, an individual’s microbiota prevents excessive proliferation.
However, certain risk factors may predispose the host to Candida spp. overgrowth and colonization. These include immunosuppressive treatments, prolonged antibiotic therapy, severe illness, primary or acquired immunodeficiency, nutritional deficiencies, and the disruption of the cutaneous and gastrointestinal barriers [1,3,4,5]. Interestingly, recent studies in human medicine report an increased abundance of Candida spp. in association with inflammatory bowel disease (IBD), although further research is necessary to clarify the potential role of fungi in this condition [6].
The gastrointestinal tract is one of the anatomical locations where candidiasis most commonly develops in humans, together with the skin and the genitourinary tract [7]. In other animal species, gastrointestinal cases have also been described [8,9,10]. In adult horses, cases of candidiasis affecting the eyes, respiratory tract, urogenital system, and joints have been documented, primarily in individuals that are immunocompromised or receiving antimicrobial treatment [11,12,13,14]. In the equine species, gastrointestinal candidiasis has only been reported in foals, affecting different locations such as the mouth, esophagus, and stomach [15]. Other manifestations of candidiasis described in foals include diarrhea, meningitis, omphalophlebitis, and, less frequently, systemic infections [1,16].
Five horses were referred for different reasons to two tertiary referral hospitals, the CEU Veterinary Clinical Hospital in Spain (Case 1) and the Equine Hospital of the University of Liège in Belgium (Cases 2–5) between July 2023 and July 2024. As part of the individual work-up of each case, a gastroscopy was performed, and gastric candidiasis was confirmed by culture and/or histopathology. This case series aims to describe the morphological, histopathological, and microbiological features of this condition which, to our knowledge, has not previously been described in adult horses. The clinical findings, diagnosis, and management of the five cases, as well as potential predisposing factors for the fungal infection, will be discussed.
2. Case Description
2.1. Case 1
A 10-year-old KWPN gelding used for dressage was referred to a veterinary hospital for an investigation of chronic weight loss. The clinical examination was within normal limits, and its body condition score (BCS) was 4/9 following the Henneke scale [17].
Initial blood work revealed mild neutropenia and lymphopenia, as well as a mild increase in gamma-glutamyl transferase (GGT) serum enzyme activity. An abdominal ultrasound revealed distended and moderately thickened (4–6 mm) small intestine loops in both inguinal regions and a mild accumulation of peritoneal fluid. Fecal culture and fecal egg count, abdominal radiology, thymidine kinase, and a glucose absorption test (85%) were within normal limits.
As part of the weight loss work-up, a gastroscopy was performed, and atypical, white, easily detachable cotton-like patches on the squamous gastric mucosa were observed (Figure 1). Grade 2 ulcers were observed on the squamous gastric mucosa, and diffuse hyperemic areas were visible in the glandular portion and duodenum (Table 1) [18].
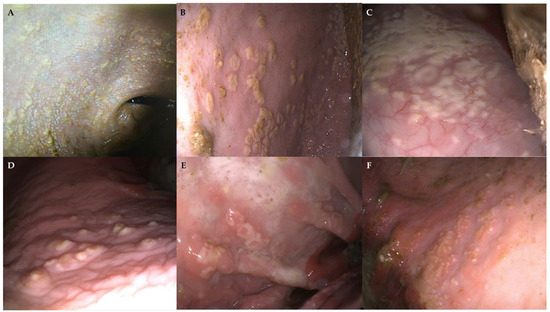
Figure 1.
Gastroscopic images showing white, cotton-like material on the squamous mucosa of horses with gastric candidiasis, forming pseudo-membranous multifocal to coalescing plaques (A–C). In some cases, fungal lesions appeared punctiform (D), ring-shaped (E) or with a miliary appearance (F), close to the greater curvature. An underlying hyperemic area, extending beyond the plaques, is visible in some lesions (E,F).

Table 1.
Detailed macroscopic findings found in the squamous mucosa, glandular mucosa, and the duodenum during gastroscopies performed to the 5 horses.
Gastric and duodenal biopsies were obtained as part of the weight loss investigation. Histopathologic evaluation revealed moderate gastritis and mild lymphoplasmacytic enteritis (Table 2). The culture of the gastric lesions was positive for Candida spp., along with Klebsiella pneumoniae, Pseudomonas mendocina, and Acinetobacter baumannii.
Table 2.
Detailed fungal culture and histopathology results performed from gastric and duodenal biopsies in the five horses.
The horse was diagnosed with equine gastric ulcer syndrome (EGUS) and potential lymphoplasmacytic enteritis. It was discharged under treatment with omeprazole, sucralfate, and probiotics (Menarini Consumer Health, Barcelona, Spain; TRM, Newbridge, Ireland) as well as the recommendation of a controlling gastroscopy one month later. Additional treatment with fluconazole was recommended but was never administered by the owner. A tapering protocol with corticosteroids was recommended after gastric candidiasis resolved.
After discharge, the horse left the country and was lost to follow-up. When contacted one year later, the owner reported that the follow-up gastroscopy had been performed five months after discharge at another clinic. Complete resolution of the gastric ulcers was observed, with no remaining evidence of the initial fungal, cotton-like lesions.
2.2. Case 2
A 3-year-old miniature stallion was admitted to the veterinary hospital with signs of lethargy that had been developing for one week. There was also a history of progressive weight loss in the last 2 years. On arrival, the pony was dull and hypothermic (36.9 °C) with an estimated BCS of 3/9.
Blood analysis showed mild anaemia, hypoalbuminemia and hyperlactatemia.
After initial stabilisation (Lactated Ringer’s, intravenous glucose, and plasma, B. Braun, Melsungen, Germany), several ancillary tests were performed during hospitalization to investigate the cause of weight loss, including dental examination, fecal egg count, abdominal/thoracic radiology and ultrasound, peritoneal fluid cytology, oral glucose tolerance test (OGGT), and a gastroscopy (day 10), including duodenal biopsies. Given its poor appetite, the horse had been started on proton pump inhibitors (omeprazole 2 mg/kg PO q24 h, Norbrook Laboratories, Monaghan, Ireland) one day before gastroscopy.
The gastroscopy revealed mainly atypical large multifocal coalescent plaques of a friable white pseudo-membranous material located on the squamous gastric mucosa (Figure 1B,C). A complete description of gastroscopic findings can be found in Table 1. The aspect of the plaques evoked lesions of oral candidiasis, so a fungal aetiology was suspected. Biopsies were performed and sent for fungal culture and histopathology, yielding positive results for Candida spp. Duodenal biopsies were obtained as well, and the results confirmed a mild lymphoplasmacytic infiltrate. Detailed histopathological results are described in Table 2.
A presumptive diagnosis of lymphoplasmacitic enteritis associated with partial malabsorption (45%) was concluded. Given the strong suspicion of IBD, a decreasing protocol of corticosteroids (initially dexamethasone (Dechra Veterinary Products, Herentals, Belgium) starting at 0.1 mg/kg IM q24 h for 15 days and prednisolone (Le Vet.B.V., Oudewater, The Netherlands) at 2 mg/kg PO q24 h over several weeks) was implemented, and omeprazole therapy was continued.
One week later, before leaving the hospital (day 18), a second gastroscopy was performed, revealing the complete resolution of the fungal plaques.
2.3. Case 3
An 11-year-old crossbred mare was referred to the veterinary hospital due to an acute onset of hyperthermia (41 °C) 2 weeks earlier, followed by inappetence. Weight loss had been noticed over the last few months, taking place after the mare moved to a new barn. Suspecting piroplasmosis, the referring veterinarian had administered corticosteroids and imidocarb 5 days prior to admission.
On clinical examination, the mare showed a BCS of 3/9 with generalised muscular atrophy. Mild icterus, a heart rate of 48 bpm, and a rectal temperature of 36.9 °C were also noticed.
The blood analysis revealed moderate neutrophilic leucocytosis, mild hypoalbuminemia, increased serum amyloid A (SAA), and hypovitaminosis E. Direct polymerase chain reaction (PCR) blood testing for Theileria equi and Babesia caballi yielded negative results. A left dorsal displacement of the large colon was identified on the rectal examination. The weight loss work-up revealed no abnormalities on dental examination, fecal egg count, thoracic/abdominal imaging (US and X-Ray), or abdominal fluid cytology.
On gastroscopy, the stomach showed a few atypical pearl-shaped patches on the non-glandular mucosa (Table 1). Biopsies of the patches were performed, and, despite no growth on the fungal culture, the histopathology confirmed fungal infiltration (Figure 2). Duodenal biopsies were obtained as well. Detailed histopathological results can be found in Table 2.
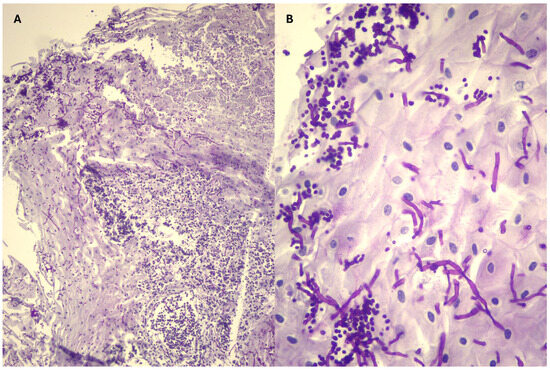
Figure 2.
Histopathological images of the endoscopic biopsies taken from the white plaques on the squamous mucosa of horses with gastric candidiasis. Periodic acid-Schiff stain. (A) Squamous epithelium with fungal spores and hyphae, pyocytes, and bacteria (10×). (B) Numerous spores and hyphae colonizing the squamous epithelium of the equine stomach (40×).
No more fever was noted, and the mare gained weight during hospitalization, so a presumptive diagnosis of transient viral infection and inadequate food intake were concluded. The mare left the clinic without any treatment except for dietary recommendations.
No further gastroscopies were performed in this case. Several months after hospitalisation, the mare had recovered an adequate body condition (6/9) and was reported to be clinically normal.
2.4. Case 4
A 9-year-old Friesian crossbred mare was referred to the veterinary hospital with signs of colic.
The mare had a BCS of 7/9 and presented tachycardia (58 bpm) and reduced borborygmi on admission.
Clinical chemistry evaluation revealed hyperlactatemia and a moderate neutrophilic leucocytosis. The large colon felt tympanic and was displaced caudally to the right on rectal examination. A right colon displacement was diagnosed and treated successfully with intravenous (Lactated Ringer’s, B. Braun, Melsungen, Germany) and enteral fluid therapy and 24 h of food withholding. On day 2, the mare presented a transient phase of soft feces, fever, and neutropenic leukopenia without further clinical signs. A Fecal PCR was positive for Salmonella spp. Activated charcoal (Vinoferm, Beverlo, Belgium), smectite (Platinum Performance, Buellton, CA, USA), flunixin meglumine (0.25 mg/kg q6 h, Syva, León, Spain), and enoxaparin (Sanofi-Aventis, Argenteuil, France) were added to the treatment.
The mare presented poor appetite during refeeding. Suspecting EGUS, omeprazole (Norbrook Laboratories, Monaghan, Ireland) and sucralfate (EXOD, Saint-Cloud, France) were started on day 4, and a gastroscopy was performed on day 6. Atypical white, ring-shaped plaques were visible in the squamous gastric mucosa, some of them surrounded by an erythematous halo (Table 1). Biopsies of the plaques were performed and sent for fungal culture and histopathology, confirming the presence of Candida spp. in the lesions. Significant pyloric ulcers were confirmed and biopsied as well. Detailed results of the histopathological exam can be found in Table 2.
The horse was discharged on treatment with omeprazole (4 mg/kg PO q24 h) and sucralfate (12 mg/kg PO 12 h) for 3 weeks, and a follow up gastroscopy was planned.
The appetite of the mare had normalized during treatment, and the second gastroscopy showed a significant improvement of the pyloric and squamous lesions. Although the white plaques were mostly gone, some of the initial erythematous lesions remained on the squamous mucosa. The nature and clinical significancy of the remaining lesions not being clear, the owner’s consent was obtained to take additional gastric and duodenal biopsies. Detailed histopathological results can be found in Table 2. The treatment with omeprazole and sucralfate was continued for 3 additional weeks to ensure the complete resolution of the pyloric ulcers.
2.5. Case 5
A 2-year-old purebred Lusitanian mare was found stuck in a flooded field contaminated by fuel after local torrential rains. The first veterinarian who cared for it washed the skin and the stomach, administered activated charcoal and mineral oil by nasogastric tubing, and referred the mare to the veterinary hospital for further care and follow up.
On arrival, the mare showed a BCS of 5/9 and was agitated, tachycardic (56 bpm), and presented several superficial wounds all over the body.
Blood analysis showed neutrophilic leucocytosis and increased creatine phospho-kinase (CPK) activity. Thoracic radiology was normal, but lung ultrasonography showed abnormal B-lines, so early-stage pneumonia could not be excluded. Abdominal ultrasound showed no abnormalities.
The mare was placed on intravenous fluid therapy with Lactated Ringer’s (B. Braun, Melsungen, Germany), large spectrum antimicrobials (natrium penicillin 22,000 IU/kg IV q6 h (Kela, Hoogstraten, Belgium) and gentamicin 6.6 mg/kg IV q24 h (Emdoka bvba, Hoogstraten, Belgium)), NSAIDs (flunixin meglumine 1.1 mg/kg IV q12 h, Syva, León, Spain), enoxaparin (Sanofi-Aventis, Argenteuil, France), activated charcoal (Vinoferm, Beverlo, Belgium), smectite (Platinum Performance, Buellton, CA, USA), and appropriate wound care. The stomach and the skin showed fuel residues and were washed further, and the mare was kept hospitalized under observation for several days. Evolution was good, with no abnormal clinical signs except for transient soft feces.
On day 8, a gastroscopy was carried out to evaluate for potential gastrointestinal injury secondary to hydrocarbon ingestion. Squamous and glandular gastric ulcers were found (see detailed description in Table 1). Furthermore, atypical multifocal miliary white vesicles surrounded by an erythematous halo were observed on the squamous mucosa, which were not related to the more “classical” gastric ulcers (Figure 1F). Biopsies were performed on those atypical lesions and on the duodenum (see detailed description in Table 2). Fungal culture confirmed the presence of Candida glabrata.
A treatment with omeprazole (4 mg/kg PO q24 h) and sucralfate (12 mg/kg PO q12 h) was started, and the mare was discharged (Day 10).
A follow-up gastroscopy was performed 4 weeks later by the referral veterinarian. The gastric ulcers had almost resolved, and the whitish lesions were no longer visible.
3. Discussion
This study describes for the first time the findings associated with gastric candidiasis in adult horses. Previously, equine gastrointestinal candidiasis had only been reported in foals. In the five cases described in this report, all adult horses exhibited similar lesions (cotton-like plaques, easily detachable) on the non-glandular gastric mucosa, very similar to lesions observed in the oral or gastrointestinal mucosa of neonatal foals [1,16,19,20]. Despite the extensive experience of the authors in equine gastroscopic examination, such lesions had never been previously observed in adult horses. For that reason, cases were analyzed regarding literature and to look for common features or predisposing factors.
Candida spp. is a microorganism that naturally exists within the saprophytic mycobiome but can act as an opportunistic pathogen in favorable conditions. In human medicine, studies describe the presence of candidiasis in patients with imbalances in saprophytic flora, antibiotic therapy, chemotherapy, radiotherapy, stress, or immunosuppression therapy [5]. An increased incidence of candidiasis has been reported in adult horses treated with antibiotics or corticosteroids or that were in states of immunosuppression, as well as in foals with a failure of passive immunity transfer [19,21]. Three cases were presented for weight loss, although in at least one of them, the cause was found to be malnutrition. Only one horse out of the five (Case 5) had received antimicrobials (penicillin and gentamicin) before gastroscopic examination. Additionally, another horse (Case 3) had received a single dose of corticosteroids. In which degree these treatments may have helped Candida overgrowth in these two cases remains unknown.
Some articles in human medical literature have investigated the potential relationship between the use of gastric acid suppressors and gastrointestinal fungal overgrowth. Gastric acid is considered a main barrier for the inhibition of fungal and bacterial overgrowth of the stomach and small bowel, and its absence has been associated with gastroenteritis caused by Clostridium difficile, Salmonella, and Campylobacter as well as with rapid increases in Candida concentrations in gastrointestinal content [22]. It has been shown that the use of gastric acid suppressor therapy may promote increased Candida colonization in the esophagus and stomach [22,23,24]. Interestingly, the concurrent use of proton pump inhibitors and steroids in the same patient substantially increased the risk of esophageal candidiasis compared to the effect of each medication alone, suggesting a synergistic effect [25]. In animals, few studies have been published on the relationship of gastric acid inhibition and gastrointestinal colonization by Candida spp. A study in rats showed that previous treatment with antisecretory agents or non-steroidal anti-inflammatory drugs allowed persistent colonization with Candida after experimental inoculation [26]. From the five horses included in this study, only two (Case 2 and Case 4) had received gastric protectants or gastric acid suppression prior to gastroscopy. Given the short course of the therapy before gastroscopy in both cases (1 and 4 days, respectively), it is unlikely that they played a major role in the development of the gastric lesions observed. Furthermore, it is interesting to notice that gastric fungal lesions resolved in three of the five horses while receiving antiulcer treatment (omeprazole and/or sucralfate) for the prevention or treatment of concomitant EGUS.
Traditionally, the stomach was considered a sterile environment; however, it is now known that both in humans and animals there is a gastric microbiota [27]. It is important to note that the composition of the gastric microbiota can vary based on external factors such as diet, transportation, thermal stress, high performance, age, geographic location, medical treatments, and the presence of diseases. These factors can significantly influence the microbial balance of the gastrointestinal tract [28]. Although the gastric microbiota in horses has not been widely characterized, the presence of genera such as Lactobacillus spp., Streptococcus spp., Actinobacillus spp., Moraxella spp., Prevotella spp., and Porphyromonas spp. has been demonstrated through samples taken from healthy patients. In the gastrointestinal tract, Candida spp. can overgrow alongside other pathogenic microorganisms such as Clostridium difficile, Pseudomonas spp., Helicobacter spp., Enterobacter spp., and Escherichia coli [29]. In Case 1, a bacteriologic study of gastric white plaques was performed, and the growths of Klebsiella pneumoniae, Pseudomonas mendocina, and Acinetobacter baumannii were observed. Despite no bacterial cultures of gastric lesions being performed in Cases 2–5, histopathology revealed often a suppurative gastritis, including neutrophilic infiltration and the presence of bacteria. The interpretation of this data in relation to the presence of fungal lesions is difficult. Despite the fact that some of those bacteria could be merely contaminants, in humans, it has been observed that the excessive growth of Actinobacillus spp, Pseudomona spp., and Helicobacter spp. under certain conditions may be associated with gastric disorders, and something similar could happen in horses. This finding opens the door to future research in veterinary medicine that could explore the role of these pathogens in the gastric health of animals [27,28]. Stomach and gastric feeding tubes have been frequently found colonized by oral Candida spp. in human patients [30]. Candida spp. have been identified as part of the normal nasal microbiota in healthy horses [2]. This raises the question of whether nasogastric intubation could promote Candida spp. proliferation in horses. Four out of the five patients reported in this study underwent nasogastric tubing for enteral fluid therapy for less than 24 h prior to the identification of gastric lesions associated with Candida spp. Mechanical irritation from the tube could have acted as an initial insult, facilitating fungal proliferation. Although this hypothesis cannot be entirely ruled out, it seems unlikely to account for the extent and distribution of the fungal lesions observed in these cases.
The diagnosis of Candida spp. infections is usually confirmed through histopathology or fungal culture of affected tissues and exudates. Among the species responsible for candidiasis, Candida albicans remains the most prevalent etiological agent, followed by C. glabrata, C. tropicalis, C. parapsilosis, and C. krusei [1,6,31]. Depending on the species, different morphological forms—yeasts, pseudo-hyphae, or hyphae—can be observed [8,32]. From the five cases reported here, C. glabrata was isolated in one of them (Case 5). Unfortunately, the laboratories did not go further in the species identification of the other isolated Candida. Case 3 yielded negative fungal culture results, but histopathological findings supported fungal infection of the lesions (Table 2).
Human research has identified an association between Candida albicans colonization and various inflammatory disorders of the gastrointestinal tract, suggesting that such colonization might hinder the resolution of inflammatory responses [7]. Findings from animal model studies indicate that Candida colonization impairs the healing of inflammatory lesions, while inflammation itself can enhance fungal colonization. In human medicine, fungal growth has commonly been described in both non-glandular and glandular (peptic) gastric ulcers [33]. Gastric candidiasis in foals has also been associated with gastric ulcers in the non-glandular mucosa [15,20]. Inflammation of the gastric mucosa may be linked to a decline in local bacterial populations, facilitating fungal proliferation [7]. In the present report, two horses had grade-2 squamous ulcers (Cases 1 and 5), and three horses had different kinds of glandular ulcers (Cases 1, 4, and 5), but mycotic lesions did not seem associated with those ulcerative lesions in any of the five cases. Interestingly, erythematous mucosa underlying Candida lesions has been described in human oral candidiasis when the characteristic white plaques are wiped away [34]. In some of the cases reported here, we observed an erythematous halo surrounding the fungal lesions (Figure 1E,F).
Inflammatory bowel diseases (IBDS) are a group of gastrointestinal tract disorders characterized by the infiltration of the mucosa and submucosa with inflammatory cells [35]. Consequently, there may be an alteration in the microbiome, which can contribute to an overgrowth of fungal elements [36]. In human medicine, indeed, IBD has been associated with the increased growth of Candida spp., which can further compromise the gastrointestinal barrier, heighten inflammation, and slow down tissue healing [7]. Only one of the five horses (Case 1) presented macroscopic lesions in the duodenal area; however, duodenal biopsies were taken in all of them to investigate the potential presence of IBD together with Candida spp. colonization. In three of them, there was a history of weight loss and histological duodenal findings of mild to moderate lymphoplasmacytic inflammatory bowel disease (Cases 1, 2, and 3). One of them presented distended and thickened small intestinal loops as well (Case 1). However, in the other two cases (Cases 4 and 5), IBD was not supported by either clinical or laboratory findings; thus, the link between Candidiasis and this gastrointestinal disorder currently seems weak in horses, and a potential cause-and-effect relationship remains to be elucidated.
Finally, it is interesting to notice that, in all five horses, we had evidence of improvement or even complete resolution of the fungal lesions without the need to administer any antifungal treatment. An absence of fungi in the squamous mucosa was also confirmed histologically in the control gastroscopy of one case (Case 4). Four of the five horses received antiulcer treatment (one omeprazole only and three omeprazole + sucralfate) for the prevention or treatment of concomitant EGUS. Human literature is controversial regarding the response of gastric Candida infection to acid suppression therapy. As already mentioned, some studies consider gastric acid suppression as a predisposing factor for fungal development [22,23,24], while others report the healing of gastric ulcers colonized by Candida after 6 weeks of proton pump inhibitor therapy only without antifungal medication [37]. Some limitations of the present case series include the lack of information about Candida spp. subspecies and the absence of follow-up gastroscopy in some cases.
4. Conclusions
In conclusion, gastric candidiasis occurs in adult horses and seems to exclusively affect the squamous gastric mucosa. Macroscopical findings look fairly similar to gastrointestinal candidiasis in foals. Diagnosis can be achieved by the observation of characteristic cotton-like multifocal plaques in gastroscopic examination or through fungal identification in culture or biopsy. No direct association with EGUS lesions has been found despite the fact that concomitant EGUS lesions may be present in affected horses. A potential association with gastric bacterial dysbiosis or intestinal inflammation in horses deserves further study. Based on the five cases presented in this series, no clear predisposing factors can be suggested for gastric candidiasis in adult horses, but the condition seems benign and resolves without need of antifungal therapy.
Author Contributions
Conceptualization, C.C. and M.d.l.C.-T.; investigation, P.N.-E. and C.A.M.; resources, S.J., V.V. and C.C.; writing—original draft preparation, P.N.-E. and C.A.M.; writing—review and editing, C.B.-E., M.d.l.C.-T., V.V., and C.C.; funding acquisition, C.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all owners of animals involved in this study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
The authors want to thank Marine Lopes and Ludivine Marczewski for their detailed follow up information concerning Case 5.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BCS | Body Condition Score |
| KWPN | Koninklijk Warmbloed Paardenstamboek Nederland |
| EGUS | Equine Gastric Ulcer Syndrome |
| PCR | Polymerase Chain Reaction |
| NSAIDs | Non-Steroidal Anti-inflammatory Drugs |
| GGT | Gamma-Glutamyl Transferase |
| CPK | Creatin Phosphokinase |
| IBD | Inflammatory Bowel Disease |
References
- Sellon, D.C.; Long, M.T. Equine Infectious Diseases, 2nd ed.; Saunders/Elsevier: St. Louis, MO, USA, 2014; pp. 408–411. [Google Scholar]
- Cordeiro, R.D.A.; Bittencourt, P.V.; Brilhante, R.S.N.; Teixeira, C.E.C.; Castelo-Branco, D.D.S.C.M.; Silva, S.T.D.C.; De Alencar, L.P.; Souza, E.R.Y.; Bandeira, T.d.J.P.G.; Monteiro, A.J.; et al. Species of Candida as a component of the nasal microbiota of healthy horses. Med. Mycol. 2013, 51, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Linder, N.; Levit, O.; Klinger, G.; Kogan, I.; Levy, I.; Shalit, I.; Ashkenazi, S.; Sirota, L. Risk factors associated with candidaemia in the neonatal intensive care unit: A case–control study. J. Hosp. Infect. 2004, 57, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Pirrone, A.; Castagnetti, C.; Mariella, J.; Bonoli, C.; Stancampiano, L.; Tampieri, M.P.; Galuppi, R. Yeast Flora in Oropharyngeal and Rectal Mucous Membranes of Healthy and Critically Ill Neonatal Foals. J. Equine Vet. Sci. 2012, 32, 93–98. [Google Scholar] [CrossRef]
- Jawhara, S. How Gut Bacterial Dysbiosis Can Promote Candida albicans Overgrowth during Colonic Inflammation. Microorganisms 2022, 10, 1014. [Google Scholar] [CrossRef]
- Poulain, D. Candida albicans, plasticity and pathogenesis. Crit. Rev. Microbiol. 2013, 41, 208–217. [Google Scholar] [CrossRef]
- Kumamoto, C.A. Inflammation and gastrointestinal Candida colonization. Curr. Opin. Microbiol. 2011, 14, 386–391. [Google Scholar] [CrossRef]
- Bradford, K.; Meinkoth, J.; McKeirnen, K.; Love, B. Candida peritonitis in dogs: Report of 5 cases. Vet. Clin. Pathol. 2013, 4, 227–233. [Google Scholar] [CrossRef]
- Nadăş, G.C.; Taulescu, M.A.; Ciobanu, L.; Fiţ, N.I.; Flore, C.; Răpuntean, S.; Bouari, C.M.; Catoi, C. The Interplay Between NSAIDs and Candida albicans on the Gastrointestinal Tract of Guinea Pigs. Mycopathologia 2013, 175, 221–230. [Google Scholar] [CrossRef]
- Randolph, N.K.; Her, J.; McAloney, C.A.; Wellman, M. Gastrointestinal colonization by Diutina (Candida) rugosa in a 6-year-old Siberian Husky. Vet. Clin. Pathol. 2024, 53, 255–260. [Google Scholar] [CrossRef]
- Doyle, A.; López, A.; Pack, L.; Muckle, A. Candida osteomyelitis in a gelding. Can. Vet. J. 2013, 54, 176. [Google Scholar] [PubMed]
- Montes, A.J.; Montes, L.F.; Vaughan, J.; Wilborn, W.H.; Bado, G.; Comero, A.; Blaquier, P.C. Vulvo vaginal candidiasis in thoroughbred mares following progestogen administration intravaginal treatment with clotrimazole. J. Equine Vet. Sci. 2001, 21, 68–70. [Google Scholar] [CrossRef]
- Cafarchia, C.; Figueredo, L.A.; Otranto, D. Fungal diseases of horses. Vet. Microbiol. 2013, 167, 215–234. [Google Scholar] [CrossRef] [PubMed]
- Stefanetti, V.; Marenzoni, M.L.; Lepri, E.; Coletti, M.; Proietti, P.C.; Agnetti, F.; Crotti, S.; Pitzurra, L.; Del Sero, A.; Passamonti, F. A case of Candida guilliermondii abortion in an Arab mare. Med. Mycol. Case Rep. 2014, 4, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Gross, T.; Matyhew, I. Gastroesophageal ulceration and candidiasis in foals. J. Am. Vet. Med. Assoc. 1983, 15, 1370–1373. [Google Scholar] [CrossRef] [PubMed]
- Reilly, L.K.; Palmer, J.E. Systemic candidiasis in four foals. J. Am. Vet. Med. Assoc. 1994, 205, 464–466. [Google Scholar] [CrossRef] [PubMed]
- Henneke, D.R.; Potter, G.D.; Kreider, J.L.; Yeates, B.F. Relationship between condition score, physical measurements and body fat percentage in mares. Equine Vet. J. 1983, 15, 371–372. [Google Scholar] [CrossRef]
- Sykes, B.W.; Hewetson, M.; Hepburn, R.J.; Luthersson, N.; Tamzali, Y. European College of Equine Internal Medicine Consensus Statement—Equine Gastric Ulcer Syndrome in Adult Horses. J. Vet. Intern. Med. 2015, 29, 1288–1299. [Google Scholar] [CrossRef]
- McClure, J.J.; Addison, J.D.; Miller, R.I. Immunodeficiency manifested by oral candidiasis and bacterial septicemia in foals. J. Am. Vet. Med. Assoc. 1985, 186, 1195–1197. [Google Scholar] [CrossRef] [PubMed]
- Preis, I.S.; Silva, R.O.S.; Pires, P.S.; Lobato, F.C.F.; Palhares, M.S.; Maranhão, R.P.A.; Ecco, R. Enteritis associated with Clostridium difficile and opportunistic candidiasis in a foal. Braz. J. Vet. Path. 2012, 5, 10–12. Available online: https://bjvp.org.br/wp-content/uploads/2015/07/DOWNLOAD-FULL-ARTICLE-2-20881_2012_3_30_8_11.pdf (accessed on 15 May 2024).
- Cohen, J.M.; Ross, M.W.; Busschers, E. Diagnosis and management of Candida utilis infectious arthritis in a Standardbred filly. Equine Vet. Educ. 2008, 20, 348–352. [Google Scholar] [CrossRef]
- Daniell, H.W. Acid suppressing therapy as a risk factor for Candida esophagitis. Dis. Esophagus 2016, 29, 479–483. [Google Scholar] [CrossRef]
- Larner, A.J.; Lendrum, R. Oesophageal candidiasis after omeprazole therapy. Gut 1992, 33, 860–861. [Google Scholar] [CrossRef]
- Mottaghi, B.; Emami, M.H.; Riahi, P.; Fahim, A.; Rahimi, H. Candida colonization of the esophagus and gastric mucosa; a comparison of patients taking proton pump inhibitors and those taking histamine receptor antagonist drugs. Gastroenterol. Hepatol. Bed Bench 2021, 14, 349–355. [Google Scholar] [PubMed] [PubMed Central]
- Shah, M.D.N.; Cavanagh, Y.; Shulik, O.; Patel, P.; DeBari, V.A.; Baddoura, W. Proton pump inhibitors and corticosteroids as synergistic risk factors for Candida esophagitis. J. Adv. Med. Res. 2015, 10, 1–6. [Google Scholar] [CrossRef]
- Brzozowski, T.; Zwolinska-Wcislo, M.; Konturek, P.C.; Kwiecien, S.; Drozdowicz, D.; Konturek, S.J.; Stachura, J.; Budak, A.; Bogdal, J.; Pawlik, W.W.; et al. Influence of gastric colonization with Candida albicans on ulcer healing in rats: Effect of ranitidine, aspirin and probiotic therapy. Scand. J. Gastroenterol. 2005, 40, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.A.; Bakker, H.C.D.; Burton, A.J.; Erb, H.N.; McDonough, S.P.; McDonough, P.L.; Parker, J.; Rosenthal, R.L.; Wiedmann, M.; Dowd, S.E.; et al. Equine Stomachs Harbor an Abundant and Diverse Mucosal Microbiota. Appl. Environ. Microbiol. 2012, 78, 2522–2532. [Google Scholar] [CrossRef]
- Boucher, L.; Leduc, L.; Leclère, M.; Costa, M.C. Current Understanding of Equine Gut Dysbiosis and Microbiota Manipulation Techniques: Comparison with Current Knowledge in Other Species. Animals 2024, 14, 758. [Google Scholar] [CrossRef]
- Pinto, N.C.; Bosch, J.N.; Ng-Wong, Y.K.; Menowsky, M.; Shine, R.; Moya, M.; Galindo, J.; Serna, S.; Ii, M.M.; Malcolm, J. A Case Report of Candida-Induced Emphysematous Gastritis. Cureus 2023, 15, 47870. [Google Scholar] [CrossRef]
- Gottlieb, K.; Iber, F.L.; Livak, A.; Leya, J.; Mobarhan, S. Oral Candida Colonizes the Stomach and Gastrostomy Feeding Tubes. J. Parenter. Enter. Nutr. 1994, 18, 264–267. [Google Scholar] [CrossRef]
- Kreulen, I.A.M.; De Jonge, W.J.; Van Den Wijngaard, R.M.; Van Thiel, I.A.M. Candida spp. in Human Intestinal Health and Disease: More than a Gut Feeling. Mycopathologia 2023, 188, 845–862. [Google Scholar] [CrossRef]
- Veses, V.; Gow, N.A.R. Pseudohypha budding patterns of Candida albicans. Med. Mycol. 2009, 47, 268–275. [Google Scholar] [CrossRef]
- Sasaki, K. Candida-associated gastric ulcer relapsing in a different position with a different appearance. World J. Gastroenterol. 2012, 18, 4450. [Google Scholar] [CrossRef]
- Akpan, A.; Morgan, R. Oral candidiasis. Postgrad. Med. J. 2002, 78, 455–459. [Google Scholar] [CrossRef]
- Vitale, V. Inflammatory bowel diseases in horses: What do we know? Equine Vet. Educ. 2022, 34, 493–500. [Google Scholar] [CrossRef]
- Patnaik, S.; Durairajan, S.S.K.; Singh, A.K.; Krishnamoorthi, S.; Iyaswamy, A.; Mandavi, S.P.; Jeewon, R.; Williams, L.L. Role of Candida Species in Pathogenesis, Immune Regulation, and Prognostic Tools for Managing Ulcerative Colitis and Crohn’s Disease. World J. Gastroenterol. 2024, 30, 5212–5220. [Google Scholar] [CrossRef]
- Di Febo, G.; Miglioli, M.; Calò, G.; Biasco, G.; Luzza, F.; Gizzi, G.; Cipollini, F.; Rossi, A.; Barbara, L. Candida albicans infection of gastric ulcer frequency and correlation with medical treatment: Results of a multicenter study. Dig. Dis. Sci. 1985, 30, 178–181. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).