Abstract
The homeostasis of the skin microbiome can be disrupted by both extrinsic and intrinsic factors, leading to a state of dysbiosis. This imbalance has been observed at the onset of persistent skin diseases that are closely linked to mental health conditions like anxiety and depression. This narrative review explores recent findings on the relationship between the skin microbiome and the pathophysiology of specific skin disorders, including acne vulgaris, atopic dermatitis, psoriasis, and wound infections. Additionally, it examines the psychological impact of these skin disorders, emphasizing their effect on patients’ quality of life and their association with significant psychological consequences, such as anxiety, depression, stress, and suicidal ideation in the most severe cases.
1. Introduction
The skin is a dynamic tissue composed of multiple cells and structures that work together to maintain the integrity of the body against external challenges. The main skin layers are the epidermis and the dermis, which have several roles, such as defense barrier, homeostatic functions, wound repair, support of vitamin D synthesis, and avoidance of colonization by pathogenic organisms [1,2]. Human skin constitutes a true microbial ecosystem, termed the skin microbiome (SM), consisting of bacteria, fungi, and viruses. However, skin varies in its physicochemical and biochemically properties along body sites, giving rise to distinct microenvironments within the SM that promote specific microbial populations [3]. Thus, sebaceous sites of skin have a high density of lipid-rich sebaceous glands, which promote colonization by lipophilic microbial taxa, such as the bacteria Cutibacterium (formerly Propionibacterium) and the fungi Malassezia [1,4]. Moist areas have elevated concentrations of apocrine sweat glands and are primarily populated by the bacterial genera Corynebacterium and Staphylococcus [4]. Conversely, dry skin sites harbor the lowest levels of microbial abundance and diversity, with Corynebacterium, Cutibacterium, and Streptococcus being the dominant bacterial species [5]. However, disruption of the cutaneous barrier, as happens with skin aging, disease, and injuries, can lead to microbial dysbiosis and heighten the risk of skin infections, such as acne vulgaris, atopic dermatitis (AD), psoriasis, and wound infections [6].
The psychological consequences of skin disorders often include elevated levels of anxiety and depression. In this respect, there is a bidirectional relationship between dermatological conditions and mental health, with skin disorders exacerbating psychological distress and vice versa [7].
Therefore, in the present narrative study, we review recent findings on the relationship between the SM and the pathophysiology of various skin diseases, including acne vulgaris, AD, psoriasis, and wound infections. Additionally, we examine the psychological consequences associated with these skin conditions.
2. Human Skin Microbiome
The skin is the largest organ of the human body (average surface area of 30 m2) and harbors 103 to 106 microorganisms in an adult, depending on the sampling site [8]. Most of the bacteria of the human SM are included in four phyla: Actinomycetota, Bacillota, Pseudomonadota, and Bacteroidota, and the dominant genera are Staphylococcus, Cutibacterium, Corynebacterium, Micrococcus, Streptococcus, and Acinetobacter [9]. In addition, fungi belonging to the divisions Ascomycota and Basidiomycota also form part of the SM. The dominant genus is Malassezia, with the species M. restricta, M. globosa, and M. sympodialis, although the highest fungal diversity has been observed on the feet, colonized by the genera Aspergillus, Cryptococcus, Epicoccum, and Rhodotorula [10]. Viruses belonging to the families Papillomaviridae, Polyomaviridae, Poxviridae, and Circoviridae have been reported as common members of the SM [1,11]; although several bacteriophages have also been recently characterized [11,12].
An indicator of a healthy balance between skin microbial communities (eubiosis) is the preservation of skin barrier integrity, which is achieved by the skin cell development [13], the production of antimicrobial peptides by tissue-resident immune cells [14,15], and the prevention of pathogen overgrowth through microbial competitive interactions [16,17]. Perturbation of this balance (dysbiosis) is marked by the excessive growth of certain bacterial species and by a reduction in community diversity. Such dysbiosis can result in compromised wound healing, heightened inflammation, and an increased risk of microbial infections [3,18].
Changes in the SM with Age
The homeostasis of the SM shifts with age because of lifelong changes in skin physiology as the cutaneous immune system develops and hormones stimulate the growth of sweat and sebum glands, affecting the availability of essential nutrients for microorganisms. At birth, the skin, like in the gut, is rapidly colonized from the immediate environment; therefore, the mode of delivery influences the initial composition of the community [19]. For instance, the SM of vaginally delivered neonates is predominantly comprised of vaginal-associated microbiota, mainly Lactobacillus and Prevotella, and shows a higher presence of the yeast Candida albicans. Newborns delivered by cesarean section possess microbiomes that contain microorganisms from maternal skin, such as Corynebacterium, Cutibacterium, Staphylococcus, and Streptococcus [20]. Newborn and infant skin begins to acidify and has a higher water content, elevated pH, reduced sebum production, accelerated epidermal turnover, and enhanced antimicrobial properties [21]. Decreased sebum production early in life is linked to a lower abundance of Corynebacterium, Cutibacterium and Malassezia, to an increase in staphylococci and streptococci, and to a mycobiome predominantly featuring Candida species [5,20,22].
Commensal colonization also promotes the maturation of immune cells, especially the localization of regulatory T cells (Treg) to developing hair follicles shortly after birth [23]. The precise interaction between commensal bacterial antigen and Tregs is necessary to establish immune tolerance, which precludes inflammation directed at the commensals over time [23,24]. Concurrent recognition of several pathogen-related molecules and microbial toxins during initial colonization events restricts the formation of pathogen-specific Tregs [25].
Pubertal hormones (mainly androgens) lead to physical and sexual development that also directly foster functional and structural modifications in the skin, such as sebaceous glands, which increases sebum production, and apocrine sweat gland development, which increases body odor. These changes lead to subsequent shifts in microbial composition [26]. Children in the prepubertal stage exhibit higher relative abundances of Bacteroidota, Pseudomonadota, and Streptococcus, along with greater bacterial and fungal diversity compared to young adults [27,28]. As mentioned previously, the young adult SM is dominated by lipophilic microorganisms, including Corynebacterium, Cutibacterium, and Malassezia [27,28], a profile related to increased sebum production and to elevated serum hormone levels [28]. Estrogen and progesterone strengthen the skin barrier and support wound healing by promoting collagen synthesis and stimulating keratinocyte proliferation. Additionally, they regulate immune function in both pro- and anti-inflammatory manners [3,29]. These hormonal-driven alterations in skin physiology result in changes to the skin microbial communities [28]. Interestingly, androgen-driven development of sebaceous gland and estrogen-induced changes in skin surface lipids [30] fosters the predominance of lipophilic species, such as Cutibacterium acnes and Malassezia restricta [28]. While apocrine gland secretions are initially odorless, body odor in children and adolescents is linked to microbial production of isovaleric and acetic acids (with a sour smell), and of sulfur compounds (with a rotten-egg smell) [31]. In young adults, body odor, particularly from the axillary area [31], is related to the breakdown of sebum by Corynebacterium species into volatile fatty acids (with a cheesy smell) and sulfanyl alkanols (with an oniony smell) [32].
Sex differences in skin microbial composition become increasingly evident as puberty progresses [28]. During this period, the microbial communities in females tend to exhibit reduced diversity and a higher predominance of Cutibacterium, while the SM of males show greater inter-individual variability and increased diversity, characterized by elevated levels of Corynebacterium, Haemophilus, Staphylococcus, and Streptococcus [28]. Furthermore, hormonal changes affecting skin physiology (such as a reduced pH and increased thickness) and immune system modifications during puberty likely contribute to various of the shifts observed in the SM [27]. The adult SM is stable over time, establishing networks of interactions between different microorganisms [33]. Each body site has a unique microenvironment (with a characteristic pH and nutrient pool) and a particular sweat and sebaceous gland density, which determines the prevailing microbial composition [34]. However, the SM may be influenced by the environment, geographic localization, and residence in the same localization [35].
As the skin ages, it undergoes several physiological changes caused by intrinsic and extrinsic factors. Intrinsically aged skin, impacted by genetic, hormonal, and metabolic modifications (e.g., decrease in estradiol levels), is characterized by diminished sebaceous gland activity, reduced blood circulation, and the breakdown of collagenous and fibrous extracellular matrices, resulting in atrophy, decreased lipid content, xerosis, and loss of skin cell regeneration [36,37]. In contrast, extrinsic factors are triggered by environmental factors, mainly UV exposure, and are manifested by telangiectasia, hyperpigmentation, pronounced wrinkles, and a leathery texture [38]. Both intrinsically and extrinsically aged skin exhibits a higher pH, reduced hydration, and lower expression of tight junction proteins compared to youthful skin.
These changes can manifest as impaired wound healing, and as an increase in the production of natural moisturizing factors (NMFs), which are produced as a consequence of the loss of the skin’s ability to retain water. NMFs can foster bacterial growth and adherence to the skin [39] and are also associated with an increased abundance of several microbial taxa, such as Anaerococcus, Corynebacterium, Micrococcus, and Streptococcus [34], and with a reduction in Cutibacterium [34,39]. The decrease in sebocyte area and sebum generation after menopause in women is related to a loss of Cutibacterium and to a higher abundance of Acinetobacter, Corynebacterium, and Streptococcus [32,36,40]. In contrast, men have a significantly slower decline in sebum secretion and maintain a higher Cutibacterium abundance [41].
Elderly subjects maintain a low-grade inflammatory state with elevated systemic levels of pro-inflammatory cytokines [42]. Skin Langerhans cells are progressively lost from the epidermis [43], and cutaneous dendritic cells, in turn, show a diminished capacity for migrating to lymph nodes and present antigens to T cells [44]. This failure in antigen presentation leads to slower immune responses, reduced antimicrobial activity, and compromised wound healing [45]. The weakened immune defenses and higher prevalence of potentially pathogenic bacteria contribute to a significantly greater risk of skin infections in the elderly and to difficulties in resolving these infections [45,46].
3. Skin Microbiome in Disease
A variety of intrinsic and extrinsic factors can influence the shape and composition of the SM, resulting in a state of dysbiosis [47] (Figure 1). While the mechanisms underlying dysbiosis in these diseases remain poorly understood, there is a continuing debate about whether dysbiosis acts as a cause or as a result of the disease [6]. In this situation, the commensal skin microbiota is unable to prevent colonization by pathogenic microorganisms, a phenomenon termed colonization resistance [48]. The mechanisms through which colonization resistance take place have become the focus of current research, involving not only competition for adhesion sites and nutrients but also the role of signaling molecules. A dysbiosis process has been noted at the onset of skin diseases, such as acne vulgaris, AD, psoriasis, and wound infections.
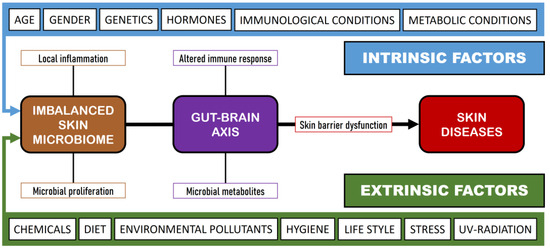
Figure 1.
Influence of intrinsic and extrinsic factors on skin diseases.
3.1. Acne Vulgaris
Increased levels of androgens at the start of puberty can trigger fluctuations in skin cell activity, inflammation, and the colonization of hair follicles by C. acnes, leading to the onset of acne. Acne is a persistent inflammatory condition of the pilosebaceous follicle that affects over 85% of adolescents and young adults. Its pathogenesis encompasses elevated sebum production, follicular hyperkeratinization, clogged hair follicles, painful papules, and inflammation [49]. C. acnes is a lipophilic bacterium that predominantly inhabits sebaceous skin areas. In this regard, each pore is typically governed by a single, nearly clonal lineage [50] and individuals possess a distinctive combination of C. acnes strains [5]. Although acne has been primarily related to C. acnes proliferation, some researchers have reported that the levels of C. acnes do not show significant differences between individuals with acne and those without [51]. Consequently, it seems that the reduction in diversity among the six phylogenetic groups (IA1, IA2, IB1, IC, II, and III), with a predominance of IA1, and to a lesser extent IA2, rather than the proliferation of C. acnes, contributes to the onset of acne [52]. These acne-associated phylotypes tend to release pro-inflammatory cytokines, show increased porphyrin production [53], and exhibit excessive lipase activity, which subsequently attracts neutrophils and promotes hyperkeratosis [54]. In addition, C. acnes can also develop biofilms that elevate its virulence and its resistance to antimicrobial treatment [55]. Interestingly, Staphylococcus epidermidis inhibits C. acnes proliferation by means of the release of succinic acid from glycerol fermentation [56], and also diminishes C. acnes-induced skin inflammation by generating lipoteichoic acid, which suppresses keratinocyte production of Toll-like receptor (TLR) 2, interleukin (IL)-6, and tumor necrosis factor (TNF)-α [57]. In contrast, C. acnes restrains the proliferation of S. epidermidis by maintaining the acidic environment of the pilosebaceous follicle, hydrolyzing sebum triglycerides and releasing propionic acid [58]. On the other hand, other commensal microorganisms such as Malassezia also participate in the pathogenesis of acne, as this genus possesses a lipase more active than that of C. acnes, and may attract neutrophils and stimulate the liberation of pro-inflammatory cytokines from monocytes and keratinocytes [59].
3.2. Atopic Dermatitis
AD (eczema) is an inflammatory skin disease, characterized by dry, inflamed, itchy skin patches, affecting between 15 and 20% of children and 2–10% of adults [60]. AD arises from a sophisticated interplay of genetic susceptibility, barrier dysfunction, both innate and adaptive immune responses, and SM dybiosis [61]. As a result, affected skin areas have increased permeability, decreased water retention, high pH, and disturbed lipid structure [62,63], allowing Staphylococcus aureus to access deeper layers of the skin [60].
Altered keratinocytes and microbial antigens provoke immune responses [64], which further exacerbate barrier defects via the downregulation of filaggrin [65], disruption of tight junctions, and diminishment in stratum corneum lipids, thereby increasing skin susceptibility to S. aureus colonization [65]. Thus, a continuous cycle of impaired barrier function, augmented microbial and irritant infiltration into deeper layers of the skin, and heightened inflammation, followed by itching and additional skin damage, develops. Further alterations in the microbiome associated with AD involve a decrease in C. acnes, Corynebacterium, Dermacoccus, Micrococcus, and coagulase-negative staphylococci (e.g., S. epidermidis and S. hominis), coupled with an increase in Streptococcus and various Malassezia species [62,64,66]. These microbial changes do not seem to be permanent, with a reduction in community diversity and increased S. aureus presence before and during AD flare-ups, followed by a gradual return to baseline levels after the flare resolves [67]. Whether S. aureus initiates AD or prospers as a result of the disease is yet to be clarified. However, toxins and proteases produced by S. aureus exacerbate damage to the skin barrier and stimulate both adaptive and innate immune responses [68].
On the other hand, S. epidermidis seems to be an antagonist of S. aureus [69]. S. epidermidis maintains SM balance by incorporating innate immune mechanisms that regulate effector T-cell activity, and by performing an antimicrobial role via the secretion of IL-1α by dendritic cells and keratinocytes, thus restricting the capacity of pathogens to cause infections [70]. In addition, colonization by Malassezia spp. intensifies with the severity of AD, and its pathophysiological impact may stem from the stimulation of pro-inflammatory cytokines and autoreactive cells. This process can lead to elevated expression of TLR2 and TLR4 via the release of immunogenic proteins [60,68].
3.3. Psoriasis
Psoriasis is a chronic inflammatory disease with worldwide prevalence and a multifactorial etiology, including genetic and non-genetic factors such as diet, drugs, infections, smoking, and stress [71]. These factors induce immune dysregulation and trigger interactions among innate immune cells, adaptive immune cells and keratinocytes, being mediated by cytokines (including IL-6, IL-17, IL-22, IL-23, interferon [IFN], and TNF-α), and leading to the development of erythematous and scaly plaques [72,73,74].
In addition, the breakdown of immune tolerance to cutaneous microorganisms has also been suggested to be involved in the pathogenesis of psoriasis [75], such as species of the genus Staphylococcus (S. aureus, S. pettenkoferi, and S. sciuri) [75,76]. These species colonize psoriatic lesions, secrete enterotoxins and toxic shock syndrome toxin-1, and induce an inflammatory Th17 response responsible for maintaining keratinocyte proliferation [76]. Streptococcus pyogenes infections of the upper respiratory tract are also considered an important etiological factor in psoriasis. These bacterial infections induce T-cell activation and produce IFN-γ, which is elevated in patients with chronic plaque psoriasis lesions [77]. Besides, bacterial superantigens located in the dermal layers bind directly to human leukocyte antigen (HLA)-DR receptors on dendritic cells, macrophages, and keratinocytes, perpetuating inflammation [75].
Diverse studies suggest that the gut is a possible origin of the dysbiosis detected in psoriasis. The most commonly reported findings are a reduction in the gut microbiome of Bacteroides and Akkermansia spp. and an increase in members of the phyla Bacillota and Actinomycetota [72,78]. This intestinal dysbiosis leads to bacterial translocation and induction of inflammation, resulting in the perpetuation of the inflammatory response as seen in inflammatory bowel and Crohn’s diseases [75,79].
3.4. Chronic Wounds
Chronic wounds are typically categorized as burns, diabetic ulcers, malignant ulcers, pressure ulcers, venous ulcers, and pyoderma gangrenosum [80]. The wound healing process involves an interaction among endothelial cells, fibroblasts, keratinocytes, and Langerhans cells, and it is linked to processes such as hemostasis, inflammation, proliferation, and remodeling [81]. Wound healing is regulated by several cytokines and growth factors, including platelet-derived growth factor, transforming growth factors (TGF-β, TGF-α), fibroblast growth factor, and vascular endothelial growth factor, which stimulate angiogenesis, granulation tissue formation, and tissue repair [82]. Multiple bacterial colonization of wounds forms biofilms that delay wound healing by activating neutrophils and pro-inflammatory macrophages, leading to the accumulation of pro-inflammatory cytokines, cytolytic enzymes, and free oxygen radicals [83,84]. The unregulated immune environment of chronic wounds promotes bacterial proliferation, resulting in a vicious cycle of biofilm growth and ongoing inflammation [85]. The major bacterial genera involved in this process are Acinetobacter, Enterobacter, Serratia, and Pseudomonas (Gram-negatives), as well as Staphylococcus, Streptococcus, Enterococcus, and Finegoldia (formerly Peptostreptococcus) (Gram-positives) [86,87].
Chronic wounds are more common in older adults, as well as in patients with chronic mechanical stress, diabetes, malnutrition, obesity, vascular disease, or in those ones with a combination of these aspects [88]. The majority of chronic wounds are colonized by polymicrobial communities, including S. aureus, Pseudomonas aeruginosa, Proteus mirabilis, Escherichia coli, Acinetobacter baumannii and Klebsiella pneumoniae [84]. Anaerobic bacteria in chronic wounds include Prevotella, Peptoniphilus, Finegoldia, and Anaerococcus [89]. In diabetic ulcers S. aureus is the most common infecting species, although other causative organisms include coagulase-negative staphylococci, Streptococcus, Enterococcus, Corynebacterium, members of the Enterobacteriaceae family, P. aeruginosa, Prevotella, Poryphyromonas, and Bacteroides fragilis [86,90]. Some pathogens have been identified in the acute phase after burn injury, including S. aureus, S. pyogenes, E. coli, P. aeruginosa, and coagulase-negative staphylococci [91]. Venous leg ulcers are a common chronic wound condition susceptible to infection by P. aeruginosa, P. mirabilis, Enterococcus, S. aureus, A. baumannii, Klebsiella, and E. coli [84].
4. Association of Skin Diseases with Mental Disorders
The skin plays a central role in the psyche of people affected by external dermatologic disorders, such as acne, dermatitis, or wound ulcers, which can lead to psychological adverse states such as depression, low self-esteem, shame, and social appearance anxiety, thus affecting their quality of life. Quality of life is defined by the World Health Organization as “an individual’s perception of his or her position in life within the context of the culture and value systems in which he or she lives, and in relation to his or her goals, expectations, standards and concerns”, and it includes various aspects such as health status, wealth, freedom, education, safety, and social belonging [92]. Self-esteem is a subjective concept that assesses a person’s self-worth, confidence in their abilities, and qualities. Healthy self-esteem is central for a balanced life, characterized by self-understanding and healthy relationships with oneself and others. The concept of self-esteem is integral to Maslow’s Hierarchy of Needs, which states that self-esteem is essential to human motivation and growth toward self-actualization. Factors such as age, disability, genetics, illness, physical ability, cognition, and socioeconomic status influence self-esteem [93]. Social appearance anxiety is the fear of being judged negatively by others because of one’s appearance. It is associated with social anxiety disorder, which negatively affects the quality of life and is inversely related to self-esteem. Social appearance anxiety involves inconsistent beliefs about one’s appearance, leading to negative body image, personality issues, depression, and affective problems [94]. Therefore, it is plausible to affirm that skin diseases can influence the development of several mental disorders in patients. In the following sections, we have reviewed the major psychological disorders associated with acne, AD, psoriasis, and wound infections.
4.1. Acne Vulgaris
Acne is a risk factor for mental disorders, including anxiety and mood disorders, negative body image, poor individual self-esteem, interpersonal relationships, and even suicide attempts in all age groups [95,96]. In accordance with the literature, acne and stress have a bidirectional relationship. For example, stress can exacerbate the severity of acne, while problems resulting from acne, such as social isolation and lack of self-confidence, can lead to depression [97]. In this respect, diverse studies have pointed out that an increase in stress levels correlates positively with an aggravation of acne severity in a significant proportion of patients with acne [98,99]. However, a different study stated an absence of a direct correlation between self-reported stress levels and the severity of acne, which may highlight variations in how individuals manage stress [100]. The characteristics and main findings of recent studies (2018–2024) on the relationship between acne vulgaris and psychological disorders are depicted in Table 1.

Table 1.
Relationship between acne vulgaris and psychological disorders.
4.2. Atopic Dermatitis
AD is characterized by pruritus and by reappearing eczematous patches and plaques on the skin. It interferes with sleep and its visible nature can be responsible for social stigma, low self-esteem, social withdrawal, reduced quality of life, and psychological distress [118]. AD is also associated with an increased risk of alexithymia, anxiety, depression, obsessive compulsive disorder (OCD), and suicidal ideation [119,120]. Furthermore, Cao et al. [121] investigated the causal relationships between AD and psychiatric disorders by means of a bidirectional two-sample Mendelian randomization analysis and concluded that AD was related to a higher risk of attention deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), anorexia nervosa (AN), and bipolar disorder (BD). Table 2 describes the relationship between AD and mental disorders.
Table 2.
Relationship between atopic dermatitis and psychological disorders.
4.3. Psoriasis
The prevalence of depression is typically greater in individuals with more severe psoriasis compared to those with milder forms of the disease, and is higher in women than in men [135]. Depression in psoriasis significantly reduces quality of life, including aspects such as sexual dysfunction, sleep disturbances, and addictions. The visible lesions associated with the physical burden of this disease can provoke adverse reactions and stigma, resulting in anxiety, depression, diminished self-esteem, and reduced subjective well-being [136].
On the question of whether psoriasis is the underlying cause of psychiatric comorbidities or if, conversely, these psychiatric conditions determine the progression of the skin disorder, Carrasco and Ballesca [137] proposed several explanations: (i) The connection between psoriasis and psychiatric disorders may involve genetic factors that could predispose individuals to both the skin condition and psychological or psychiatric states. Several investigations have identified common alterations in loci and single nucleotide polymorphisms in the HLA region related to depression, psoriasis, and schizophrenia. Nevertheless, given the polygenic nature of psoriasis, such associations may only occur in some patients. (ii) Considering the circumstances inherent to the disease itself (e.g., pain and itching, facial or genital wounds, stigmatization, sleep disturbance, deterioration on self-esteem), it can be recognized within adjustment disorders, a category that includes depressive symptoms caused by a stressor. (iii) The inflammatory state of the patient’s skin, as in psoriasis, might operate to exacerbate psychiatric disorders through synergistic routes present in both processes. Several studies on the relationship between psoriasis and mental disorders are presented in Table 3.
Table 3.
Association of psychological disorders with psoriasis (P) and chronic wounds.
4.4. Chronic Wounds
Depression is a psychological condition commonly comorbid in people that suffer from chronic wounds [155]. Patients with chronic wounds frequently express a sense of lost autonomy in their daily lives due to the external management of their skin condition, and many patients are also pessimistic about their future prospects and about the potential for wound healing [156]. The pathophysiology of depression affects wound healing by modifying immune function, heightening inflammatory responses, and raising stress hormone levels, all of which collectively disrupt the natural capacity of the body for effective tissue repair [80]. The neuroendocrine system plays a central role in modulating how psychological stress affects wound healing. The secretion of stress hormones, including cortisol and catecholamines, as a reaction to psychological stress, can substantially hinder the healing process. Evidence indicates that cortisol can slow down wound repair by suppressing the inflammatory response, which is pivotal for the early stages of wound healing. Similarly, catecholamines impair healing by reducing blood circulation to the wound area [80,157]. Table 3 reviews various studies that link psychological disorders to chronic wounds.
5. Discussion and Remarks
The SM is formed by the association of several microbial taxa, including bacteria, fungi, and viruses. These microbial species shift during life and are located along body sites depending on the skin’s physicochemical and biochemical properties, forming distinct microenvironments or niches and establishing specific ecological relationships through trophic, competitive, and quorum-sensing mechanisms [6]. Compared to other microbiomes, such as the gut, the biomass, abundance, and biodiversity of the SM is relatively low [158,159] and varies significantly with individuality and ethnicity, which may be explained by endogenous (immune status, sweat, and sebum composition) and/ or exogenous (dietary and hygiene preferences) factors [5]. While distinct variations have been observed among different ethnic groups, it is still uncertain whether race and genetics determine the composition of the SM or whether it is a consequence of diet and lifestyle [160,161]. In this sense, the dietary habits prevalent in several geographical regions (such as the Western, Mediterranean, or vegetarian diets) influence the gut microbiome [162], a fact that can be hypothesized to occur also in the case of the SM.
The eubiosis of the SM may be altered by several extrinsic and intrinsic factors (Figure 1), provoking an imbalance in the SM and the production of skin diseases. In this sense, it is interesting to establish the role of commensal microorganisms in the SM, since these same microorganisms can act as opportunistic pathogens and initiate an infectious process under certain conditions and among immunocompromised subjects [4]. For example, S. epidermidis has been implicated in AD and in Netherton syndrome [163]; Corynebacterium spp. has been reported in various skin diseases such as erythrasma, keratolysis, and trichobacteriosis [164]; and Malassezia spp. has been associated with head and neck dermatitis, seborrheic dermatitis, pityriasis versicolor, and folliculitis [165]. All these opportunistic microorganisms promote immune tolerance while also eliciting pro-inflammatory responses [166]. The human innate immune system can be stimulated against S. epidermidis via Toll-like receptors that enhance antibacterial reactions, trigger inflammation, and result in the stimulation of immune system effectors, including type-1 interferon (IFN-α and IFN-β), pro-inflammatory cytokines (IL-1, IL-6, and TNF-α), and nitric oxide [167]. In the case of Corynebacterium spp. infection, particularly C. accolens, there is an increase in the number and activation of a defined subset of γδ T cells and IL-23 [168]. Finally, Malassezia spp. infection presents an immunological paradox; in some circumstances, it acts as an adjuvant, activating the complement cascade and eliciting both cellular and humoral immune responses in healthy individuals. In contrast, it also seems to have the ability not only to evade the immune system but also to suppress the response directed against it [169].
Therefore, questions arise such as: is it appropriate to call these microorganisms commensals, is there such a thing as a healthy SM, or what are the factors that trigger the commensal–pathogen shift? To provide answers, it is pivotal that forthcoming research focus on the investigation of understudied species and their molecular and biochemical mechanisms of interaction within their ecosystems [4]. Several skin diseases have already been associated with dysbiosis in the SM, where is a predominance of some microorganisms to the detriment of others is produced through the secretion of mediators that inhibit pathogen signaling systems, preventing their colonization and damage to host tissues. According to Townsend et al. [3], future work on the SM will likely continue to explore: (i) the age evolution of the SM and the factors involved; (ii) the complex interactions between microorganisms and the immune system and how they change over the lifespan; (iii) the pathogenesis of SM dysbiosis; and (iv) the development of new therapeutic strategies to effectively modulate the microbial balance.
In this review, we have shown that certain skin diseases (i.e., acne, AD, psoriasis, and chronic wounds) have a substantial impact on the patient’s quality of life and psychological wellness (Table 1, Table 2 and Table 3). Most of the studies point out that these skin diseases are closely linked to distressing mental states, including anxiety, depression, and stress, while in severe cases, suicidal ideation has also been reported as a consequence [105,119,120]. These results could be related to the fact that skin conditions, particularly those that are visible and chronic, can constitute a stigma, and that have profound social consequences for the affected individuals. Indeed, during adolescence, a critical life period for social and emotional development, these conditions may increase the risk of victimization through harassment dynamics (e.g., mocking, social exclusion). The visible nature of skin disorders such as acne, AD, or psoriasis can lead to negative peer reactions expressed through bullying, which can elicit adverse self-conscious emotional responses such as humiliation or shame, perturbing the personal and social well-being of individuals [170]. Thus, this kind of stigmatization is not merely superficial, especially because it intersects with the psychological vulnerability of these developmental stages, potentially contributing to lasting emotional trauma. In addition, the recalcitrant symptoms of these skin conditions may exacerbate the distress experienced, leading to a process where stress worsens the skin pathology, which in turn heightens the emotional and social burden. In this respect, overwhelming stress and isolation might drive affected youth toward maladaptive coping mechanisms, including the initiation of risky behaviors, in order to escape from reality, such as continued substance use [171]. Consequently, the psychosocial impact of skin diseases should be considered a pivotal component of patient care, emphasizing the need for holistic treatment approaches. Understanding the full scope of these interactions highlights the importance of integrating dermatological care with psychological support, particularly in pediatric and adolescent populations.
Psychodermatology is recognized to be a collaborative approach between dermatologists, psychiatrists, and psychologists to help those individuals with mental disorders that arise from a skin disease, and also those with a skin disease that is influenced by mental disorders. This multidisciplinary framework is thought to yield better outcomes compared to medical treatment individually [172]. Psychodermatologic conditions can be divided into three groups: psychophysiological disorders, psychiatric disorders with dermatologic symptoms, and dermatologic disorders with psychiatric symptoms. The term “psychophysiological disorder” describes skin conditions that are exacerbated by emotional stress (e.g., acne, eczema, and psoriasis). In cases of primary psychiatric disorders, the primary issue is psychological, with skin manifestations being secondary and sometimes self-induced. In cases of secondary psychiatric disorders, the skin lesions themselves lead to negative effects on the patient’s body image, mood, and self-esteem. This can result in feelings of frustration, shame, and social anxiety [173]. The effect of the skin disease on the patient’s quality of life is considered a stronger predictor of psychiatric morbidity than the clinical severity of the skin condition. On the other hand, it is crucial to consider the side effects of skin medication on the psychological well-being of patients. For instance, Ding et al. [174] studied isotretinoin, a vitamin A derivative employed for the treatment of acne, in relation to the potential psychological consequences experienced by patients due to its use. These authors concluded that these side effects remain unclear and do not seem to differ significantly from the psychological effects caused by acne itself.
Reported risk factors for skin disease include socioeconomic aspects such as bacterial infections, dietary variables, excess of body weight, frequent skin touching, humid environments, stress, tobacco use, topical oily products that obstruct pores, as well as genetic and hormonal factors [175]. The “hygiene hypothesis” postulates that insufficient exposure to a diverse array of skin microbiota during childhood may impair the proper “training” of the immune system [176]. This lack of exposure is thought to diminish the immune system’s resistance to microbial pathogens, thereby increasing susceptibility to infections and to other diseases. AD and other atopic skin diseases may be associated with an overly sterile (abiotic) environment [177].
There is a bidirectional relationship between gut and skin dysbiosis, with imbalances in the gut microbiome influencing the pathophysiology of various inflammatory skin conditions [178]. Therefore, in the future, the treatment of skin diseases and their psychological consequences can be based on the adjustment of human skin and gut microbiomes with healthy dietary patterns and with probiotics, prebiotics, synbiotics, and fecal microbiota transplantation [179,180,181], as well as with other strategies that are providing promising results (e.g., skin microbiota transplantation) [182]. In this regard, engineering and restoration of skin microbiota could emerge as a potent strategy for treating skin diseases in the future [183]. Finally, it is important to highlight that the prevalence of skin diseases has increased in recent years, with fungal infections being major contributors to skin and subcutaneous diseases worldwide [184]. Additionally, several environmental factors and food additives appear to be directly or indirectly involved in the rising incidence of these health conditions [185,186].
Author Contributions
Conceptualization, A.B.-R. and J.J.B.; investigation, J.J.B.; writing—original draft preparation, J.J.B.; writing—review and editing, A.B.-R.; supervision, J.J.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Byrd, A.L.; Belkaid, Y.; Segre, J.A. The human skin microbiome. Nat. Rev. Microbiol. 2018, 16, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Smythe, P.; Wilkinson, H.N. The skin microbiome: Current landscape and future opportunities. Int. J. Mol. Sci. 2023, 24, 3950. [Google Scholar] [CrossRef] [PubMed]
- Townsend, E.C.; Kalan, L.R. The dynamic balance of the skin microbiome across the lifespan. Biochem. Soc. Trans. 2023, 51, 71–86. [Google Scholar] [CrossRef]
- Flowers, L.; Grice, E.A. The skin microbiota: Balancing risk and reward. Cell Host Microbe 2020, 28, 190–200. [Google Scholar] [CrossRef]
- Oh, J.; Byrd, A.L.; Deming, C.; Conlan, S.; Kong, H.H.; Segre, J.A. Biogeography and individuality shape function in the human skin metagenome. Nature 2014, 514, 59–64. [Google Scholar] [CrossRef]
- Glatthardt, T.; Lima, R.D.; de Mattos, R.M.; Ferreira, R.B.R. Microbe interactions within the skin microbiome. Antibiotics 2024, 13, 49. [Google Scholar] [CrossRef]
- Balieva, F.; Abebe, D.S.; Dalgard, F.J.; Lien, L. Risk of developing psychiatric disease among adult patients with skin disease: A 9-year national register follow-up study in Norway. Skin Health Dis. 2023, 3, e294. [Google Scholar] [CrossRef]
- Skowron, K.; Bauza-Kaszewska, J.; Kraszewska, Z.; Wiktorczyk-Kapischke, N.; Grudlewska-Buda, K.; Kwiecińska-Piróg, J.; Wałecka-Zacharska, E.; Radtke, L.; Gospodarek-Komkowska, E. Human skin microbiome: Impact of intrinsic and extrinsic factors on skin microbiota. Microorganisms 2021, 9, 543. [Google Scholar] [CrossRef] [PubMed]
- Cundell, A.M. Microbial ecology of the human skin. Microb. Ecol. 2018, 76, 113–120. [Google Scholar] [CrossRef]
- Nguyen, U.T.; Kalan, L.R. Forgotten fungi: The importance of the skin mycobiome. Curr. Opin. Microbiol. 2022, 70, 102235. [Google Scholar] [CrossRef]
- Hannigan, G.D.; Meisel, J.S.; Tyldsley, A.S.; Zheng, Q.; Hodkinson, B.P.; SanMiguel, A.J.; Minot, S.; Bushman, F.D.; Grice, E.A. The human skin double-stranded DNA virome: Topographical and temporal diversity, genetic enrichment, and dynamic associations with the host microbiome. mBio 2015, 6, e01578-15. [Google Scholar] [CrossRef] [PubMed]
- Natarelli, N.; Gahoonia, N.; Sivamani, R.K. Bacteriophages and the microbiome in dermatology: The role of the phageome and a potential therapeutic strategy. Int. J. Mol. Sci. 2023, 24, 2695. [Google Scholar] [CrossRef] [PubMed]
- Uberoi, A.; Bartow-McKenney, C.; Zheng, Q.; Flowers, L.; Campbell, A.; Knight, S.A.B.; Chan, N.; Wei, M.; Lovins, V.; Bugayev, J.; et al. Commensal microbiota regulates skin barrier function and repair via signaling through the aryl hydrocarbon receptor. Cell Host Microbe 2021, 29, 1235–1248.e8. [Google Scholar] [CrossRef] [PubMed]
- Lunjani, N.; Ahearn-Ford, S.; Dube, F.S.; Hlela, C.; O’Mahony, L. Mechanisms of microbe-immune system dialogue within the skin. Genes Immun. 2021, 22, 276–288. [Google Scholar] [CrossRef]
- Takahashi, T.; Gallo, R.L. The critical and multifunctional roles of antimicrobial peptides in dermatology. Dermatol. Clin. 2017, 35, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Claesen, J.; Spagnolo, J.B.; Ramos, S.F.; Kurita, K.L.; Byrd, A.L.; Aksenov, A.A.; Melnik, A.V.; Wong, W.R.; Wang, S.; Hernandez, R.D.; et al. A Cutibacterium acnes antibiotic modulates human skin microbiota composition in hair follicles. Sci. Transl. Med. 2020, 12, eaay5445. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, J.N.; Rea, M.C.; O’Connor, P.M.; Hill, C.; Ross, R.P. Human skin microbiota is a rich source of bacteriocin-producing staphylococci that kill human pathogens. FEMS Microbiol. Ecol. 2019, 95, fiy241. [Google Scholar] [CrossRef]
- Verbanic, S.; Shen, Y.; Lee, J.; Deacon, J.M.; Chen, I.A. Microbial predictors of healing and short-term effect of debridement on the microbiome of chronic wounds. NPJ Biofilms Microbiomes 2020, 6, 21. [Google Scholar] [CrossRef]
- Borrego-Ruiz, A.; Borrego, J.J. Neurodevelopmental disorders associated with gut microbiome dysbiosis in children. Children 2024, 11, 796. [Google Scholar] [CrossRef]
- Chu, D.M.; Ma, J.; Prince, A.L.; Antony, K.M.; Seferovic, M.D.; Aagaard, K.M. Maturation of the infant microbiome community structure and function across multiple body sites and in relation to mode of delivery. Nat. Med. 2017, 23, 314–326. [Google Scholar] [CrossRef]
- Visscher, M.O.; Carr, A.N.; Winget, J.; Huggins, T.; Bascom, C.C.; Isfort, R.; Lammers, K.; Narendran, V. Biomarkers of neonatal skin barrier adaptation reveal substantial differences compared to adult skin. Pediatr. Res. 2021, 89, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.; Duan, Y.Y.; Kong, F.Q.; Galzote, C.; Quan, Z.X. Dynamics of skin mycobiome in infants. Front. Microbiol. 2020, 11, 1790. [Google Scholar] [CrossRef] [PubMed]
- Scharschmidt, T.C.; Vasquez, K.S.; Pauli, M.L.; Leitner, E.G.; Chu, K.; Truong, H.A.; Lowe, M.M.; Sanchez Rodriguez, R.; Ali, N.; Laszik, Z.G.; et al. Commensal microbes and hair follicle morphogenesis coordinately drive Treg migration into neonatal skin. Cell Host Microbe 2017, 21, 467–477.e5. [Google Scholar] [CrossRef] [PubMed]
- Scharschmidt, T.C.; Vasquez, K.S.; Truong, H.A.; Gearty, S.V.; Pauli, M.L.; Nosbaum, A.; Gratz, I.K.; Otto, M.; Moon, J.J.; Liese, J.; et al. A wave of regulatory T cells into neonatal skin mediates tolerance to commensal microbes. Immunity 2015, 43, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Leech, J.M.; Dhariwala, M.O.; Lowe, M.M.; Chu, K.; Merana, G.R.; Cornuot, C.; Weckel, A.; Ma, J.M.; Leitner, E.G.; Gonzalez, J.R.; et al. Toxin-triggered interleukin-1 receptor signaling enables early-life discrimination of pathogenic versus commensal skin bacteria. Cell Host Microbe 2019, 26, 795–809.e5. [Google Scholar] [CrossRef]
- Gratton, R.; Del Vecchio, C.; Zupin, L.; Crovella, S. Unraveling the role of sex hormones on keratinocyte functions in human inflammatory skin diseases. Int. J. Mol. Sci. 2022, 23, 3132. [Google Scholar] [CrossRef]
- Oh, J.; Conlan, S.; Polley, E.C.; Segre, J.A.; Kong, H.H. Shifts in human skin and nares microbiota of healthy children and adults. Genome Med. 2012, 4, 77. [Google Scholar] [CrossRef]
- Park, J.; Schwardt, N.H.; Jo, J.H.; Zhang, Z.; Pillai, V.; Phang, S.; Brady, S.M.; Portillo, J.A.; MacGibeny, M.A.; Liang, H.; et al. Shifts in the skin bacterial and fungal communities of healthy children transitioning through puberty. J. Investig. Dermatol. 2022, 142, 212–219. [Google Scholar] [CrossRef]
- Wilkinson, H.N.; Hardman, M.J. The role of estrogen in cutaneous ageing and repair. Maturitas 2017, 103, 60–64. [Google Scholar] [CrossRef]
- Yang, M.; Zhou, M.; Li, Y.; Huang, H.; Jia, Y. Lipidomic analysis of facial skin surface lipid reveals the causes of pregnancy-related skin barrier weakness. Sci. Rep. 2021, 11, 3229. [Google Scholar] [CrossRef]
- Lam, T.H.; Verzotto, D.; Brahma, P.; Ng, A.H.Q.; Hu, P.; Schnell, D.; Tiesman, J.; Kong, R.; Ton, T.M.U.; Li, J.; et al. Understanding the microbial basis of body odor in pre-pubescent children and teenagers. Microbiome 2018, 6, 213. [Google Scholar] [CrossRef] [PubMed]
- Emter, R.; Natsch, A. The sequential action of a dipeptidase and a β-lyase is required for the release of the human body odorant 3-methyl-3-sulfanylhexan-1-ol from a secreted cys-gly-(S) conjugate by corynebacteria. J. Biol. Chem. 2008, 283, 20645–20652. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Byrd, A.L.; Park, M.; Kong, H.H.; Segre, J.A. Temporal stability of the human skin microbiome. Cell 2016, 165, 854–866. [Google Scholar] [CrossRef]
- Howard, B.; Bascom, C.C.; Hu, P.; Binder, R.L.; Fadayel, G.; Huggins, T.G.; Jarrold, B.B.; Osborne, R.; Rocchetta, H.L.; Swift, D.; et al. Aging-associated changes in the adult human skin microbiome and the host factors that affect skin microbiome composition. J. Investig. Dermatol. 2022, 142, 1934–1946.e21. [Google Scholar] [CrossRef]
- Cho, H.W.; Eom, Y.B. Forensic analysis of human microbiome in skin and body fluids based on geographic location. Front. Cell. Infect. Microbiol. 2021, 11, 695191. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, J.J.; Myeong, N.R.; Kim, T.; Kim, D.; An, S.; Kim, H.; Park, T.; Jang, S.I.; Yeon, J.H.; et al. Segregation of age-related skin microbiome characteristics by functionality. Sci. Rep. 2019, 9, 16748. [Google Scholar] [CrossRef]
- Wilkinson, H.N.; Hardman, M.J. A role for estrogen in skin ageing and dermal biomechanics. Mech. Ageing Dev. 2021, 197, 111513. [Google Scholar] [CrossRef]
- Fang, J.Y.; Wang, P.W.; Huang, C.H.; Chen, M.H.; Wu, Y.R.; Pan, T.L. Skin aging caused by intrinsic or extrinsic processes characterized with functional proteomics. Proteomics 2016, 16, 2718–2731. [Google Scholar] [CrossRef]
- Feuillie, C.; Vitry, P.; McAleer, M.A.; Kezic, S.; Irvine, A.D.; Geoghegan, J.A.; Dufrêne, Y.F. Adhesion of Staphylococcus aureus to corneocytes from atopic dermatitis patients is controlled by natural moisturizing factor levels. mBio 2018, 9, e01184-18. [Google Scholar] [CrossRef]
- Kim, H.J.; Oh, H.N.; Park, T.; Kim, H.; Lee, H.G.; An, S.; Sul, W.J. Aged related human skin microbiome and mycobiome in Korean women. Sci. Rep. 2022, 12, 2351. [Google Scholar] [CrossRef]
- Alkema, W.; Boekhorst, J.; Eijlander, R.T.; Schnittger, S.; De Gruyter, F.; Lukovac, S.; Schilling, K.; Kortman, G.A.M. Charting host-microbe co-metabolism in skin aging and application to metagenomics data. PLoS ONE 2021, 16, e0258960. [Google Scholar] [CrossRef] [PubMed]
- Brodin, P.; Davis, M.M. Human immune system variation. Nat. Rev. Immunol. 2017, 17, 21–29. [Google Scholar] [CrossRef]
- Hasegawa, T.; Feng, Z.; Yan, Z.; Ngo, K.H.; Hosoi, J.; Demehri, S. Reduction in human epidermal Langerhans cells with age is associated with decline in CXCL14-mediated recruitment of CD14+ monocytes. J. Investig. Dermatol. 2020, 140, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Pilkington, S.M.; Ogden, S.; Eaton, L.H.; Dearman, R.J.; Kimber, I.; Griffiths, C.E.M. Lower levels of interleukin-1 β gene expression are associated with impaired Langerhans’ cell migration in aged human skin. Immunology 2018, 153, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Chambers, E.S.; Vukmanovic-Stejic, M. Skin barrier immunity and ageing. Immunology 2020, 160, 116–125. [Google Scholar] [CrossRef]
- Haran, J.P.; Wilsterman, E.; Zeoli, T.; Beaudoin, F.L.; Tjia, J.; Hibberd, P.L. Elderly patients are at increased risk for treatment failure in outpatient management of purulent skin infections. Am. J. Emerg. Med. 2017, 35, 249–254. [Google Scholar] [CrossRef]
- Iebba, V.; Totino, V.; Gagliardi, A.; Santangelo, F.; Cacciotti, F.; Trancassini, M.; Mancini, C.; Cicerone, C.; Corazziari, E.; Pantanella, F.; et al. Eubiosis and dysbiosis: The two sides of the microbiota. New Microbiol. 2016, 39, 1–12. [Google Scholar]
- Buffie, C.G.; Pamer, E.G. Microbiota-mediated colonization resistance against intestinal pathogens. Nat. Rev. Immunol. 2013, 13, 790–801. [Google Scholar] [CrossRef]
- Carmona-Cruz, S.; Orozco-Covarrubias, L.; Sáez-de-Ocariz, M. The human skin microbiome in selected cutaneous diseases. Front. Cell. Infect. Microbiol. 2022, 12, 834135. [Google Scholar] [CrossRef]
- Conwill, A.; Kuan, A.C.; Damerla, R.; Poret, A.J.; Baker, J.S.; Tripp, A.D.; Alm, E.J.; Lieberman, T.D. Anatomy promotes neutral coexistence of strains in the human skin microbiome. Cell Host Microbe 2022, 30, 171–182.e7. [Google Scholar] [CrossRef]
- Li, C.X.; You, Z.X.; Lin, Y.X.; Liu, H.Y.; Su, J. Skin microbiome differences relate to the grade of acne vulgaris. J. Dermatol. 2019, 46, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Dagnelie, M.A.; Corvec, S.; Saint-Jean, M.; Nguyen, J.M.; Khammari, A.; Dréno, B. Cutibacterium acnes phylotypes diversity loss: A trigger for skin inflammatory process. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2340–2348. [Google Scholar] [CrossRef] [PubMed]
- Barnard, E.; Johnson, T.; Ngo, T.; Arora, U.; Leuterio, G.; McDowell, A.; Li, H. Porphyrin production and regulation in cutaneous propionibacteria. mSphere 2020, 5, e00793-19. [Google Scholar] [CrossRef]
- Sanford, J.A.; O’Neill, A.M.; Zouboulis, C.C.; Gallo, R.L. Short-chain fatty acids from Cutibacterium acnes activate both a canonical and epigenetic inflammatory response in human sebocytes. J. Immunol. 2019, 202, 1767–1776. [Google Scholar] [CrossRef]
- Hazarika, N. Acne vulgaris: New evidence in pathogenesis and future modalities of treatment. J. Dermatolog. Treat. 2021, 32, 277–285. [Google Scholar] [CrossRef]
- Claudel, J.P.; Auffret, N.; Leccia, M.T.; Poli, F.; Corvec, S.; Dréno, B. Staphylococcus epidermidis: A potential new player in the physiopathology of acne? Dermatology 2019, 235, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Skabytska, Y.; Biedermann, T. Staphylococcus epidermidis sets things right again. J. Investig. Dermatol. 2016, 136, 559–560. [Google Scholar] [CrossRef]
- Dréno, B.; Dagnelie, M.A.; Khammari, A.; Corvec, S. The skin microbiome: A new actor in inflammatory acne. Am. J. Clin. Dermatol. 2020, 21, 18–24. [Google Scholar] [CrossRef]
- Lee, Y.B.; Byun, E.J.; Kim, H.S. Potential role of the microbiome in acne: A comprehensive review. J. Clin. Med. 2019, 8, 987. [Google Scholar] [CrossRef]
- Langan, S.M.; Irvine, A.D.; Weidinger, S. Atopic dermatitis. Lancet 2020, 396, 345–360. [Google Scholar] [CrossRef]
- Byrd, A.L.; Deming, C.; Cassidy, S.K.B.; Harrison, O.J.; Ng, W.I.; Conlan, S.; NISC Comparative Sequencing Program; Belkaid, Y.; Segre, J.A.; Kong, H.H. Staphylococcus aureus and Staphylococcus epidermidis strain diversity underlying pediatric atopic dermatitis. Sci. Transl. Med. 2017, 9, eaal4651. [Google Scholar] [CrossRef] [PubMed]
- Baurecht, H.; Rühlemann, M.C.; Rodríguez, E.; Thielking, F.; Harder, I.; Erkens, A.S.; Stölzl, D.; Ellinghaus, E.; Hotze, M.; Lieb, W.; et al. Epidermal lipid composition, barrier integrity, and eczematous inflammation are associated with skin microbiome configuration. J. Allergy Clin. Immunol. 2018, 141, 1668–1676.e16. [Google Scholar] [CrossRef] [PubMed]
- Tsakok, T.; Woolf, R.; Smith, C.H.; Weidinger, S.; Flohr, C. Atopic dermatitis: The skin barrier and beyond. Br. J. Dermatol. 2019, 180, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Fyhrquist, N.; Muirhead, G.; Prast-Nielsen, S.; Jeanmougin, M.; Olah, P.; Skoog, T.; Jules-Clement, G.; Feld, M.; Barrientos-Somarribas, M.; Sinkko, H.; et al. Microbe-host interplay in atopic dermatitis and psoriasis. Nat. Commun. 2019, 10, 4703. [Google Scholar] [CrossRef]
- Hönzke, S.; Wallmeyer, L.; Ostrowski, A.; Radbruch, M.; Mundhenk, L.; Schäfer-Korting, M.; Hedtrich, S. Influence of Th2 cytokines on the cornified envelope, tight junction proteins, and β-defensins in filaggrin-deficient skin equivalents. J. Investig. Dermatol. 2016, 136, 631–639. [Google Scholar] [CrossRef]
- Bjerre, R.D.; Holm, J.B.; Palleja, A.; Sølberg, J.; Skov, L.; Johansen, J.D. Skin dysbiosis in the microbiome in atopic dermatitis is site-specific and involves bacteria, fungus and virus. BMC Microbiol. 2021, 21, 256. [Google Scholar] [CrossRef]
- Kwon, S.; Choi, J.Y.; Shin, J.W.; Huh, C.H.; Park, K.C.; Du, M.H.; Yoon, S.; Na, J.I. Changes in lesional and non-lesional skin microbiome during treatment of atopic dermatitis. Acta Derm. Venereol. 2019, 99, 284–290. [Google Scholar] [CrossRef]
- Lunjani, N.; Hlela, C.; O’Mahony, L. Microbiome and skin biology. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 328–333. [Google Scholar] [CrossRef]
- Woo, T.E.; Sibley, C.D. The emerging utility of the cutaneous microbiome in the treatment of acne and atopic dermatitis. J. Am. Acad. Dermatol. 2020, 82, 222–228. [Google Scholar] [CrossRef]
- Paller, A.S.; Kong, H.H.; Seed, P.; Naik, S.; Scharschmidt, T.C.; Gallo, R.L.; Luger, T.; Irvine, A.D. The microbiome in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 143, 26–35. [Google Scholar] [CrossRef]
- Zeng, J.; Luo, S.; Huang, Y.; Lu, Q. Critical role of environmental factors in the pathogenesis of psoriasis. J. Dermatol. 2017, 44, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Chen, Z.M.; Fan, X.Y.; Jin, Y.L.; Li, X.; Wu, S.R.; Ge, W.W.; Lv, C.H.; Wang, Y.K.; Chen, J.G. Gut-brain-skin axis in psoriasis: A review. Dermatol. Ther. 2021, 11, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Ghoreschi, K.; Balato, A.; Enerbäck, C.; Sabat, R. Therapeutics targeting the IL-23 and IL-17 pathway in psoriasis. Lancet 2021, 397, 754–766. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.M.; Ascenso, A.; Ribeiro, H.M.; Marto, J. The brain-skin connection and the pathogenesis of psoriasis: A review with a focus on the serotonergic system. Cells 2020, 9, 796. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.J.; Chan, W.H.; Hinojosa, T.; Hsu, S.; Feldman, S.R. Mechanisms of microbial pathogenesis and the role of the skin microbiome in psoriasis: A review. Clin. Dermatol. 2019, 37, 160–166. [Google Scholar] [CrossRef]
- Chang, H.W.; Yan, D.; Singh, R.; Liu, J.; Lu, X.; Ucmak, D.; Lee, K.; Afifi, L.; Fadrosh, D.; Leech, J.; et al. Alteration of the cutaneous microbiome in psoriasis and potential role in Th17 polarization. Microbiome 2018, 6, 154. [Google Scholar] [CrossRef]
- De Jesús-Gil, C.; Sans-de San Nicolás, L.; Ruiz-Romeu, E.; Ferran, M.; Soria-Martinez, L.; Chiriac, A.; Celada, A.; Pujol, R.M.; Santamaria-Babí, L.F. Specific IgA and CLA+ T-cell IL-17 response to Streptococcus pyogenes in psoriasis. J. Investigat. Dermatol. 2020, 140, 1364–1370.e1. [Google Scholar] [CrossRef]
- Zhu, Q.; Wu, K.; Yang, Q.; Meng, B.; Niu, Y.; Zhao, F. Advances in psoriasis and gut microorganisms with co-metabolites. Front. Microbiol. 2023, 14, 1192543. [Google Scholar] [CrossRef]
- Visser, M.J.E.; Kell, D.B.; Pretorius, E. Bacterial dysbiosis and translocation in psoriasis vulgaris. Front. Cell. Infect. Microbiol. 2019, 9, 7. [Google Scholar] [CrossRef]
- Frasier, K.; Li, V.; Christoforides, S.; Daly, K.; Loperfito, A.; Stech, K.; Dragovic, M. The impact of psychosocial influences on chronic wound healing. Open J. Med. Psychol. 2024, 13, 39–57. [Google Scholar] [CrossRef]
- Serra, R.; Grande, R.; Butrico, L.; Rossi, A.; Settimio, U.F.; Caroleo, B.; Amato, B.; Gallelli, L.; de Franciscis, S. Chronic wound infections: The role of Pseudomonas aeruginosa and Staphylococcus aureus. Expert Rev. Anti. Infect. Ther. 2015, 13, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Babenko, N.M.; Litvinova, O.B.; Pavlov, S.B.; Kumechko, M.V.; Komarchuk, V.V. Problems of healing chronic wounds. Mod. Med.Techn. 2023, 3, 66–70. [Google Scholar] [CrossRef]
- Wilkinson, H.N.; Hardman, M.J. Wound healing: Cellular mechanisms and pathological outcomes. Open Biol. 2020, 10, 200223. [Google Scholar] [CrossRef] [PubMed]
- Di Domenico, E.G.; Farulla, I.; Prignano, G.; Gallo, M.T.; Vespaziani, M.; Cavallo, I.; Sperduti, I.; Pontone, M.; Bordignon, V.; Cilli, L.; et al. Biofilm is a major virulence determinant in bacterial colonization of chronic skin ulcers independently from the multidrug resistant phenotype. Int. J. Mol. Sci. 2017, 18, 1077. [Google Scholar] [CrossRef] [PubMed]
- Raziyeva, K.; Kim, Y.; Zharkinbekov, Z.; Kassymbek, K.; Jimi, S.; Saparov, A. Immunology of acute and chronic wound healing. Biomolecules 2021, 11, 700. [Google Scholar] [CrossRef]
- Ding, X.; Tang, Q.; Xu, Z.; Xu, Y.; Zhang, H.; Zheng, D.; Wang, S.; Tan, Q.; Maitz, J.; Maitz, P.K.; et al. Challenges and innovations in treating chronic and acute wound infections: From basic science to clinical practice. Burn. Trauma 2022, 10, tkac014. [Google Scholar] [CrossRef]
- Matei, S.C.; Dumitru, C.S.; Fakhry, A.M.; Ilijevski, N.; Pešić, S.; Petrović, J.; Crăiniceanu, Z.P.; Murariu, M.-S.; Olariu, S. Bacterial species involved in venous leg ulcer infections and their sensitivity to antibiotherapy—An alarm signal regarding the seriousness of chronic venous insufficiency C6 stage and its need for prompt treatment. Microorganisms 2024, 12, 472. [Google Scholar] [CrossRef]
- Tomic-Canic, M.; Burgess, J.L.; O’Neill, K.E.; Strbo, N.; Pastar, I. Skin microbiota and its interplay with wound healing. Am. J. Clin. Dermatol. 2020, 21, 36–43. [Google Scholar] [CrossRef]
- Johnson, T.R.; Gómez, B.I.; McIntyre, M.K.; Dubick, M.A.; Christy, R.J.; Nicholson, S.E.; Burmeister, D.M. The cutaneous microbiome and wounds: New molecular targets to promote wound healing. Int. J. Mol. Sci. 2018, 19, 2699. [Google Scholar] [CrossRef]
- Kalan, L.R.; Brennan, M.B. The role of the microbiome in nonhealing diabetic wounds. Ann. N.Y. Acad. Sci. 2019, 1435, 79–92. [Google Scholar] [CrossRef]
- Bertesteanu, S.; Triaridis, S.; Stankovic, M.; Lazar, V.; Chifiriuc, M.C.; Vlad, M.; Grigore, R. Polymicrobial wound infections: Pathophysiology and current therapeutic approaches. Int. J. Pharm. 2014, 463, 119–126. [Google Scholar] [CrossRef] [PubMed]
- WHO. Measuring Quality of Life. Available online: https://www.who.int/tools/whoqol (accessed on 13 August 2024).
- von Soest, T.; Wagner, J.; Hansen, T.; Gerstorf, D. Self-esteem across the second half of life: The role of socioeconomic status, physical health, social relationships, and personality factors. J. Pers. Soc. Psychol. 2018, 114, 945–958. [Google Scholar] [CrossRef] [PubMed]
- Göbel, P.; Şanlıer, N.; Yılmaz, S.; Kocabaş, Ş. Social appearance anxiety and self-esteem in women: Could body mass index have a mediating role? Behav. Psychol. 2023, 31, 25–37. [Google Scholar] [CrossRef]
- Gupta, M.A.; Pur, D.R.; Vujcic, B.; Gupta, A.K. Suicidal behaviors in the dermatology patient. Clin. Dermatol. 2017, 35, 302–311. [Google Scholar] [CrossRef]
- Lukaviciute, L.; Ganceviciene, R.; Navickas, P.; Navickas, A.; Grigaitiene, J.; Zouboulis, C.C. Anxiety, depression, and suicidal ideation amongst patients with facial dermatoses (acne, rosacea, perioral dermatitis, and folliculitis) in Lithuania. Dermatology 2020, 236, 314–322. [Google Scholar] [CrossRef]
- Jović, A.; Marinović, B.; Kostović, K.; Čeović, R.; Basta-Juzbašić, A.; Bukvić Mokos, Z. The impact of pyschological stress on acne. Acta Dermatovenerol. Croat. 2017, 25, 1133–1141. [Google Scholar] [PubMed]
- Samuels, D.V.; Rosenthal, R.; Lin, R.; Chaudhari, S.; Natsuaki, M.N. Acne vulgaris and risk of depression and anxiety: A meta-analytic review. J. Am. Acad. Dermatol. 2020, 83, 532–541. [Google Scholar] [CrossRef]
- Tasneem, T.; Begum, A.; Chowdhury, M.R.K.; Rahman, S.; Macassa, G.; Manzoor, J.; Rashid, M. Effects of acne severity and acne-related quality of life on depressive symptoms among adolescents and young adults: A cross-sectional study in Bangladesh. Front. Psychol. 2023, 14, 1153101. [Google Scholar] [CrossRef]
- Karaagaç, M.; Akça, H.M.; Acat, Ö. Lack of association of acne severity with depression, anxiety, stress, and eating attitudes: A cross-sectional study. J. Pers. Med. 2024, 14, 133. [Google Scholar] [CrossRef]
- Eyüboglu, M.; Kalay, I.; Eyüboglu, D. Evaluation of adolescents diagnosed with acne vulgaris for quality of life and psychosocial challenges. Indian J. Dermatol. 2018, 63, 131–135. [Google Scholar] [CrossRef]
- Kodra, V.; Shehu, E.; Xhaja, A. Self-esteem and mental health in adolescents with acne vulgaris. Eur. Neuropsychopharmacol. 2018, 28, S44–S45. [Google Scholar] [CrossRef]
- How, K.N.; Shamsudin, N. The psychological impact and functional disability of patients with acne vulgaris in Hospital Serdang, Malaysia: A cross sectional analysis. Malays. J. Med. Health Sci. 2019, 15, 56–61. [Google Scholar]
- Mostafa, S.S.; El Malky, M.I.; Al-Barky, S.T.; Ibrahim, S.R. Psychological problems among adolescents with acne vulgaris. Egypt. J. Health Care 2019, 10, 127–141. [Google Scholar] [CrossRef]
- Altunay, I.K.; Özkur, E.; Dalgard, F.J.; Gieler, U.; Tomas Aragones, L.; Lien, L.; Poot, F.; Jemec, G.B.; Misery, L.; Szabó, C.; et al. Psychosocial aspects of adult acne: Data from 13 European countries. Acta Derm. Venereol. 2020, 100, adv00051. [Google Scholar] [CrossRef]
- D Kandre, D.; Kariya, M.M.; Patel, A.V. Prevalence of stress, anxiety and depression in patients of acne vulgaris. IP Indian J. Clin. Exp. Dermatol. 2020, 6, 243–248. [Google Scholar] [CrossRef]
- Rafiq, Z.; Mehdi, S.M. Frequency of depression, anxiety and stress in patients with acne vulgaris. J. Pak. Assoc. Dermatol. 2020, 30, 598–603. [Google Scholar]
- Molla, A.; Alrizqi, H.; Alharbi, E.; Alsubhi, A.; Alrizqi, S.; Shahada, O. Assessment of anxiety and depression in patients with acne vulgaris in Medina: A case-control study. Clin. Cosmet. Investig. Dermatol. 2021, 14, 999–1007. [Google Scholar] [CrossRef]
- Khan, A.S.; Almulhim, A.F.; Alqattan, M.H.; Almakhaitah, N.F.; Alomair, F.I.; Alkhateeb, A.A. Psychological impact of acne vulgaris among young females in the Eastern province, Saudi Arabia. Cureus 2022, 14, e29378. [Google Scholar] [CrossRef] [PubMed]
- Rayapureddy, S.; Benerji, T.; Kodali, M.; Pallekona, R.; Enamurthy, H.; Ravi Kumar, M.S. Anxiety and depression in patients with acne vulgaris at tertiary care hospital: A cross-sectional study. J. Dr. NTR Univ. Health Sci. 2022, 11, 351–355. [Google Scholar] [CrossRef]
- Agarwal, D.; Mathur, D.K.; Paliwal, V. Psychological morbidity in young adults with acne vulgaris: A hospital-based study. J. Clin. Diagn. Res. 2023, 17, WC01–WC04. [Google Scholar] [CrossRef]
- Kunjumon, S.P.; Najad, N.; Faizal, M. Depression and social anxiety among patients with presenting acne vulgaris. J. Cardiovasc. Dis. Res. 2023, 14, 1740–1747. [Google Scholar]
- Morshed, A.S.M.; Noor, T.; Uddin Ahmed, M.A.; Mili, F.S.; Ikram, S.; Rahman, M.; Ahmed, S.; Uddin, M.B. Understanding the impact of acne vulgaris and associated psychological distress on self-esteem and quality of life via regression modeling with CADI, DLQI, and WHOQoL. Sci. Rep. 2023, 13, 21084. [Google Scholar] [CrossRef] [PubMed]
- Noor, T.; Morshed, A.S.M.; Ahmed, A.; Haque, F.; Bhuiyan, M.S.I.; Hasan, A.; Guha, A.; Rahman, T. Association of depression, anxiety and stress in acne vulgaris in Bangladesh. J. Pak. Assoc. Dermatol. 2023, 33, 424–428. [Google Scholar]
- Sharma, R.; Dogra, N.; Arora, M. Psychosocial impact of acne vulgaris on the quality of life among adolescents versus adults. Clin. Med. 2023, 23, 35. [Google Scholar] [CrossRef]
- Leskelä, M.; Jokelainen, J.; Huilaja, L.; Sinikumpu, S.P. Adult acne in middle-age: Effects on mental health in general population of the Northern Finland birth cohort 1966. Acta Derm. Venereol. 2024, 104, adv14733. [Google Scholar] [CrossRef]
- Shakir, W.; Tariq, M.; Khalid, F.; Sahar. Self-esteem, social appearance anxiety and quality of life among adolescents with acne. J. Health Rehabil. Res. 2024, 4, 577–584. [Google Scholar] [CrossRef]
- Courtney, A.; Su, J.C. The psychology of atopic dermatitis. J. Clin. Med. 2024, 13, 1602. [Google Scholar] [CrossRef]
- Hartono, S.P.; Chatrath, S.; Aktas, O.N.; Kubala, S.A.; Capozza, K.; Myles, I.A.; Silverberg, J.I.; Schwartz, A. Interventions for anxiety and depression in patients with atopic dermatitis: A systematic review and meta-analysis. Sci. Rep. 2024, 14, 8844. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, J.K.; Wu, K.K.; Bui, T.L.; Armstrong, A.W. Association between atopic dermatitis and suicidality: A systematic review and meta-analysis. JAMA Dermatol. 2019, 155, 178–187. [Google Scholar] [CrossRef]
- Cao, S.; Zhang, Z.; Liu, L.; Li, Y.; Li, W.; Li, Y.; Wu, D. Causal relationships between atopic dermatitis and psychiatric disorders: A bidirectional two-sample Mendelian randomization study. BMC Psychiatry 2024, 24, 16. [Google Scholar] [CrossRef]
- Kim, S.H.; Hur, J.; Jang, J.Y.; Park, H.S.; Hong, C.H.; Son, S.J.; Chang, K.J. Psychological distress in young adult males with atopic dermatitis: A cross-sectional study. Medicine 2015, 94, e949. [Google Scholar] [CrossRef] [PubMed]
- Catal, F.; Topal, E.; Soylu, N.; Ozel Ozcan, O.; Celiksoy, M.H.; Babayiğit, A.; Karakoç, H.T.; Erge, D.; Sancak, R. Psychiatric disorders and symptoms severity in preschool children with atopic eczema. Allergol. Immunopathol. 2016, 44, 120–124. [Google Scholar] [CrossRef]
- Eckert, L.; Gupta, S.; Gadkari, A.; Mahajan, P.; Gelfand, J.M. Burden of illness in adults with atopic dermatitis: Analysis of National Health and Wellness Survey data from France, Germany, Italy, Spain, and the United Kingdom. J. Am. Acad. Dermatol. 2019, 81, 187–195. [Google Scholar] [CrossRef]
- Ring, J.; Zink, A.; Arents, B.W.M.; Seitz, I.A.; Mensing, U.; Schielein, M.C.; Wettemann, N.; de Carlo, G.; Fink-Wagner, A. Atopic eczema: Burden of disease and individual suffering—Results from a large EU study in adults. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1331–1340. [Google Scholar] [CrossRef]
- Schonmann, Y.; Mansfield, K.E.; Hayes, J.F.; Abuabara, K.; Roberts, A.; Smeeth, L.; Langan, S.M. Atopic eczema in adulthood and risk of depression and anxiety: A population-based cohort study. J. Allergy Clin. Immunol. Pract. 2020, 8, 248–257.e16. [Google Scholar] [CrossRef] [PubMed]
- Talamonti, M.; Galluzzo, M.; Silvaggio, D.; Lombardo, P.; Tartaglia, C.; Bianchi, L. Quality of life and psychological impact in patients with atopic dermatitis. J. Clin. Med. 2021, 10, 1298. [Google Scholar] [CrossRef] [PubMed]
- Keller, W.; Vogel, M.; Prenzel, F.; Genuneit, J.; Jurkutat, A.; Hilbert, C.; Hiemisch, A.; Kiess, W.; Poulain, T. Atopic diseases in children and adolescents are associated with behavioural difficulties. BMC Pediatr. 2021, 21, 197. [Google Scholar] [CrossRef]
- Kern, C.; Wan, J.; LeWinn, K.Z.; Ramirez, F.D.; Lee, Y.; McCulloch, C.E.; Langan, S.M.; Abuabara, K. Association of atopic dermatitis and mental health outcomes across childhood: A longitudinal cohort study. JAMA Dermatol. 2021, 157, 1200–1208. [Google Scholar] [CrossRef]
- Muzzolon, M.; Muzzolon, S.R.B.; Lima, M.; Canato, M.; Carvalho, V.O. Mental disorders and atopic dermatitis in children and adolescents. Postepy. Derm. Alergol. 2021, 38, 1099–1104. [Google Scholar] [CrossRef]
- Iannone, M.; Janowska, A.; Panduri, S.; Morganti, R.; Davini, G.; Romanelli, M.; Dini, V. Impact of psychiatric comorbidities in psoriasis, hidradenitis suppurativa and atopic dermatitis: The importance of a psychodermatological approach. Exp. Dermatol. 2022, 31, 956–961. [Google Scholar] [CrossRef]
- Vinh, N.M.; Trang, V.T.T.; Dac Thuy, L.N.; Tam, H.T.X.; Hang, L.T.T.; Bac, P.V. The anxiety and depression disorder in adults with atopic dermatitis: Experience of a dermatology hospital. Dermatol. Rep. 2022, 15, 9524. [Google Scholar] [CrossRef]
- Ferrucci, S.M.; Tavecchio, S.; Nicolini, G.; Angileri, L.; Ceresa, A.; Del Tordello, G.; Berti, E.; Marzano, A.V.; Buoli, M. Mental health in patients affected by atopic dermatitis: Which effects of treatment with dupilumab? Int. Clin. Psychopharmacol. 2024, 39, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.K.; Loiselle, A.; Chatrath, S.; Smith Begolka, W. Patient and caregiver perspectives on the relationship between atopic dermatitis symptoms and mental health. Dermatitis 2024, 35, 386–391. [Google Scholar] [CrossRef]
- Luna, P.C.; Chu, C.Y.; Fatani, M.; Borlenghi, C.; Adora, A.; Llamado, L.Q.; Wee, J. Psychosocial burden of psoriasis: A systematic literature review of depression among patients with psoriasis. Dermatol. Ther. 2023, 13, 3043–3055. [Google Scholar] [CrossRef]
- Snast, I.; Reiter, O.; Atzmony, L.; Leshem, Y.A.; Hodak, E.; Mimouni, D.; Pavlovsky, L. Psychological stress and psoriasis: A systematic review and meta-analysis. Br. J. Dermatol. 2018, 178, 1044–1055. [Google Scholar] [CrossRef]
- Carrascosa, J.M.; Ballesca, F. Psoriasis and psychiatric disorders: The next frontier. Actas Dermosifiliogr. 2017, 108, 502–505. [Google Scholar] [CrossRef]
- Jensen, P.; Zachariae, C.; Skov, L.; Zachariae, R. Sleep disturbance in psoriasis: A case-controlled study. Br. J. Dermatol. 2018, 179, 1376–1384. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Thyssen, J.P.; Wu, J.J.; Skov, L. Risk of first-time and recurrent depression in patients with psoriasis: A population-based cohort study. Br. J. Dermatol. 2019, 180, 116–121. [Google Scholar] [CrossRef]
- Aguayo-Carreras, P.; Ruiz-Carrascosa, J.C.; Molina-Leyva, A. Type D personality is associated with poor quality of life, social performance, and psychological impairment in patients with moderate to severe psoriasis: A cross-sectional study of 130 patients. Indian J. Dermatol. Venereol. Leprol. 2020, 86, 375–381. [Google Scholar] [CrossRef]
- Mohapatra, B.; Chakraborty, K.; Sinha, N.; Mondal, A.; Mukherjee, P.; Chatterjee, M. Prevalence of psychiatric comorbidities in patients with psoriasis: A cross-sectional study from a tertiary care hospital in Eastern India. Ind. J. Priv. Psychiatry 2020, 14, 68–74. [Google Scholar] [CrossRef]
- Bakar, R.S.; Jaapar, S.Z.S.; Azmi, A.F.; Aun, Y.C. Depression and anxiety among patients with psoriasis: A correlation with quality of life and associated factors. J. Taibah Univ. Med. Sci. 2021, 16, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Jung, K.J.; Kim, T.G.; Kim, H.W.; Jee, S.H.; Lee, M.G. Risk of psychiatric diseases among patients with psoriasis in Korea: A 12-year nationwide population-based cohort study. J. Dermatol. 2021, 48, 1763–1771. [Google Scholar] [CrossRef] [PubMed]
- Pollo, C.F.; Miot, H.A.; Matos, T.D.S.; de Souza, J.M.; Jorge, M.F.S.; Miot, L.D.B.; Meneguin, S. Prevalence and factors associated with depression and anxiety in patients with psoriasis. J. Clin. Nurs. 2021, 30, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Badaiki, W.; Penney, M.; Pyper, E.; Lester, K.; Skeard, J.; Shin, J.; Fisher, B.; Gulliver, S.; Gulliver, W.; Rahman, P. Real world studies of psoriasis and mental illness in Newfoundland and Labrador. J. Cutan. Med. Surg. 2022, 26, 494–501. [Google Scholar] [CrossRef] [PubMed]
- da Silva, N.; Augustin, M.; Hilbring, C.; Braren-von Stülpnagel, C.C.; Sommer, R. Psychological (co)morbidity in patients with psoriasis: The impact of pruritus and anogenital involvement on symptoms of depression and anxiety and on body dysmorphic concerns—A cross-sectional study. BMJ Open 2022, 12, e055477. [Google Scholar] [CrossRef] [PubMed]
- Schuster, B.; Peifer, C.; Ziehfreund, S.; Tizek, L.; Biedermann, T.; Zink, A.; Schielein, M.C. Happiness and depression in psoriasis: A cross-sectional study in Germany. Qual. Life Res. 2022, 31, 1761–1773. [Google Scholar] [CrossRef]
- Adesanya, E.I.; Henderson, A.D.; Matthewman, J.; Bhate, K.; Hayes, J.F.; Mulick, A.; Mathur, R.; Smith, C.; Carreira, H.; Rathod, S.D.; et al. Severe mental illness among adults with atopic eczema or psoriasis: Population-based matched cohort studies within UK primary care. Clin. Epidemiol. 2023, 15, 363–374. [Google Scholar] [CrossRef]
- Finlayson, K.; Miaskowski, C.; Alexander, K.; Liu, W.H.; Aouizerat, B.; Parker, C.; Maresco-Pennisi, D.; Edwards, H. Distinct wound healing and quality-of-life outcomes in subgroups of patients with venous leg ulcers with different symptom cluster experiences. J. Pain Symptom Manag. 2017, 53, 871–879. [Google Scholar] [CrossRef]
- Walburn, J.; Weinman, J.; Norton, S.; Hankins, M.; Dawe, K.; Banjoko, B.; Vedhara, K. Stress, illness perceptions, behaviors, and healing in venous leg ulcers: Findings from a prospective observational study. Psychosom. Med. 2017, 79, 585–592. [Google Scholar] [CrossRef]
- Fauziyah, H.; Gayatri, D. Pain, stress, and sleep quality in chronic wound patients. Enferm. Clin. 2018, 28, 176–179. [Google Scholar] [CrossRef]
- Fino, P.; Di Taranto, G.; Pierro, A.; Kacjulite, J.; Codolini, L.; Onesti, M.G.; Toscani, M.; Tarallo, M. Depression risk among patients with chronic wounds. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 4310–4312. [Google Scholar] [CrossRef] [PubMed]
- Dantas, J.S.; Silva, A.C.O.; Augusto, F.S.; Agra, G.; Oliveira, J.S.; Ferreira, L.M.; Sawada, N.O.; Freire, M.E.M. Health-related quality of life in people with chronic wounds and associated factors. Texto Contexto Enferm. 2022, 31, e20220010. [Google Scholar] [CrossRef]
- Spoer, D.L.; Huffman, S.S.; Rogers, A.E.; Berger, L.E.; Foshag, A.C.; Park, R.H.; Marable, J.K.; Lava, C.X.; Cunningham, M.H.; Evans, K.K. Examining the unmet needs of chronic wound patients with common mental disorders. J. Plast. Reconstr. Aesthet. Surg. 2023, 82, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.; Jia, P. Depressive symptoms in patients with wounds: A cross-sectional study. Wound Repair Regen. 2016, 24, 1059–1065. [Google Scholar] [CrossRef]
- Renner, R.; Erfurt-Berge, C. Depression and quality of life in patients with chronic wounds: Ways to measure their influence and their effect on daily life. Chronic Wound Care Manag. Res. 2017, 4, 143–151. [Google Scholar] [CrossRef]
- Almaqhawi, A.; Morrison, A.E.; Berrington, R.; Kong, M.F. Anxiety and depression among patients attending a multidisciplinary foot clinic. Pract. Diabetes 2023, 40, 14–18a. [Google Scholar] [CrossRef]
- Borrego-Ruiz, A.; Borrego, J.J. An updated overview on the relationship between human gut microbiome dysbiosis and psychiatric and psychological disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 2024, 128, 110861. [Google Scholar] [CrossRef]
- Perez Perez, G.I.; Gao, Z.; Jourdain, R.; Ramirez, J.; Gany, F.; Clavaud, C.; Demaude, J.; Breton, L.; Blaser, M.J. Body site is a more determinant factor than human population diversity in the healthy skin microbiome. PLoS ONE 2016, 11, e0151990. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Budding, A.E.; van der Lugt-Degen, M.; Du-Thumm, L.; Vandeven, M.; Fan, A. The influence of age, gender and race/ethnicity on the composition of the human axillary microbiome. Int. J. Cosmet. Sci. 2019, 41, 371–377. [Google Scholar] [CrossRef]
- Wang, Y.; Yu, Q.; Zhou, R.; Feng, T.; Hilal, M.G.; Li, H. Nationality and body location alter human skin microbiome. Appl. Microbiol. Biotechnol. 2021, 105, 5241–5256. [Google Scholar] [CrossRef]
- Borrego-Ruiz, A.; Borrego, J.J. Human gut microbiome, diet, and mental disorders. Int. Microbiol. 2024; Epub ahead of print. [Google Scholar] [CrossRef]
- Brown, M.M.; Horswill, A.R. Staphylococcus epidermidis—Skin friend or foe? PLoS Pathog. 2020, 16, e1009026. [Google Scholar] [CrossRef] [PubMed]
- Pinto, M.; Hundi, G.K.; Bhat, R.M.; Bala, N.K.; Dandekeri, S.; Martis, J.; Kambil, S.M. Clinical and epidemiological features of coryneform skin infections at a tertiary hospital. Indian. Dermatol. Online J. 2016, 7, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Saunte, D.M.L.; Gaitanis, G.; Hay, R.J. Malassezia-associated skin diseases, the use of diagnostics and treatment. Front. Cell. Infect. Microbiol. 2020, 10, 112. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.V.; Soulika, A.M. The dynamics of the skin’s immune system. Int. J. Mol. Sci. 2019, 20, 1811. [Google Scholar] [CrossRef]
- Rasoul, M.; Rokhsareh, M.; Mohammad, S.M.; Sajad, K.; Ahmadreza, M. The human immune system against Staphylococcus epidermidis. Crit. Rev. Immunol. 2019, 39, 151–163. [Google Scholar] [CrossRef]
- Ridaura, V.K.; Bouladoux, N.; Claesen, J.; Chen, Y.E.; Byrd, A.L.; Constantinides, M.G.; Merrill, E.D.; Tamoutounour, S.; Fischbach, M.A.; Belkaid, Y. Contextual control of skin immunity and inflammation by Corynebacterium. J. Exp. Med. 2018, 215, 785–799. [Google Scholar] [CrossRef] [PubMed]
- Ashbee, H.R.; Evans, E.G. Immunology of diseases associated with Malassezia species. Clin. Microbiol. Rev. 2002, 15, 21–57. [Google Scholar] [CrossRef]
- Borrego-Ruiz, A.; Fernández, S. Humiliation and its relationship with bullying victimization: A narrative review. Psychol. Soc. Educ. 2024, 16, 42–51. [Google Scholar] [CrossRef]
- Borrego-Ruiz, A. Intrinsic motivation and drug consumption: A review of studies on curiosity and expansion motives. Health Addict. 2024, 24, 47–67. [Google Scholar] [CrossRef]
- Bewley, A. The neglected psychological aspects of skin disease. BMJ 2017, 358, j3208. [Google Scholar] [CrossRef]
- Mufaddel, A.; Abdelgani, A. Psychiatric comorbidity in patients with psoriasis, vitiligo, acne, eczema and group of patients with miscellaneous dermatological diagnoses. Open J. Psychiatry 2014, 4, 168–175. [Google Scholar] [CrossRef]
- Ding, R.L.; Zheng, Y.; Bu, J. Physiological and psychological effects of isotretinoin in the treatment of patients with acne: A narrative review. Clin. Cosmet. Investigat. Dermatol. 2023, 16, 1843–1854. [Google Scholar] [CrossRef] [PubMed]
- Heng, A.H.S.; Chew, F.T. Systematic review of the epidemiology of acne vulgaris. Sci. Rep. 2020, 10, 5754. [Google Scholar] [CrossRef] [PubMed]
- Gensollen, T.; Iyer, S.S.; Kasper, D.L.; Blumberg, R.S. How colonization by microbiota in early life shapes the immune system. Science 2016, 352, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, E.A.; Connolly, J.; Hourihane, J.O.; Fallon, P.G.; McLean, W.H.I.; Murray, D.; Jo, J.H.; Segre, J.A.; Kong, H.H.; Irvine, A.D. Skin microbiome before development of atopic dermatitis: Early colonization with commensal staphylococci at 2 months is associated with a lower risk of atopic dermatitis at 1 year. J. Allergy Clin. Immunol. 2017, 139, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.R.; Boland, C.R.; Patel, M.; Thrash, B.; Menter, A. Cutaneous manifestations of gastrointestinal disease: Part I. J. Am. Acad. Dermatol. 2013, 68, 189.e1-210. [Google Scholar] [CrossRef]
- Borrego-Ruiz, A.; Borrego, J.J. Psychobiotics: A new perspective on the treatment of stress, anxiety, and depression. Anxiety Stress 2024, 30, 79–93. [Google Scholar] [CrossRef]
- Alves, E.; Gregório, J.; Rijo, P.; Rosado, C.; Monteiro Rodrigues, L. Kefir and the gut-skin axis. Int. J. Environ. Res. Public Health 2022, 19, 13791. [Google Scholar] [CrossRef]
- Ellis, S.R.; Nguyen, M.; Vaughn, A.R.; Notay, M.; Burney, W.A.; Sandhu, S.; Sivamani, R.K. The skin and gut microbiome and its role in common dermatologic conditions. Microorganisms 2019, 7, 550. [Google Scholar] [CrossRef]
- Yang, Y.; Qu, L.; Mijakovic, I.; Wei, Y. Advances in the human skin microbiota and its roles in cutaneous diseases. Microb. Cell Fact. 2022, 21, 176. [Google Scholar] [CrossRef]
- Johns, N.I.; Blazejewski, T.; Gomes, A.L.; Wang, H.H. Principles for designing synthetic microbial communities. Curr. Opin. Microbiol. 2016, 31, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Yakupu, A.; Aimaier, R.; Yuan, B.; Chen, B.; Cheng, J.; Zhao, Y.; Peng, Y.; Dong, J.; Lu, S. The burden of skin and subcutaneous diseases: Findings from the global burden of disease study 2019. Front. Public Health 2023, 11, 1145513. [Google Scholar] [CrossRef] [PubMed]
- Faraz, K.; Seely, M.; Marano, A.L. The role of the environment in allergic skin disease. Curr. Allergy Asthma Rep. 2024, 24, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Witkowski, M.; Grajeta, H.; Gomułka, K. Hypersensitivity reactions to food additives-preservatives, antioxidants, flavor enhancers. Int. J. Environ. Res. Public Health 2022, 19, 11493. [Google Scholar] [CrossRef]
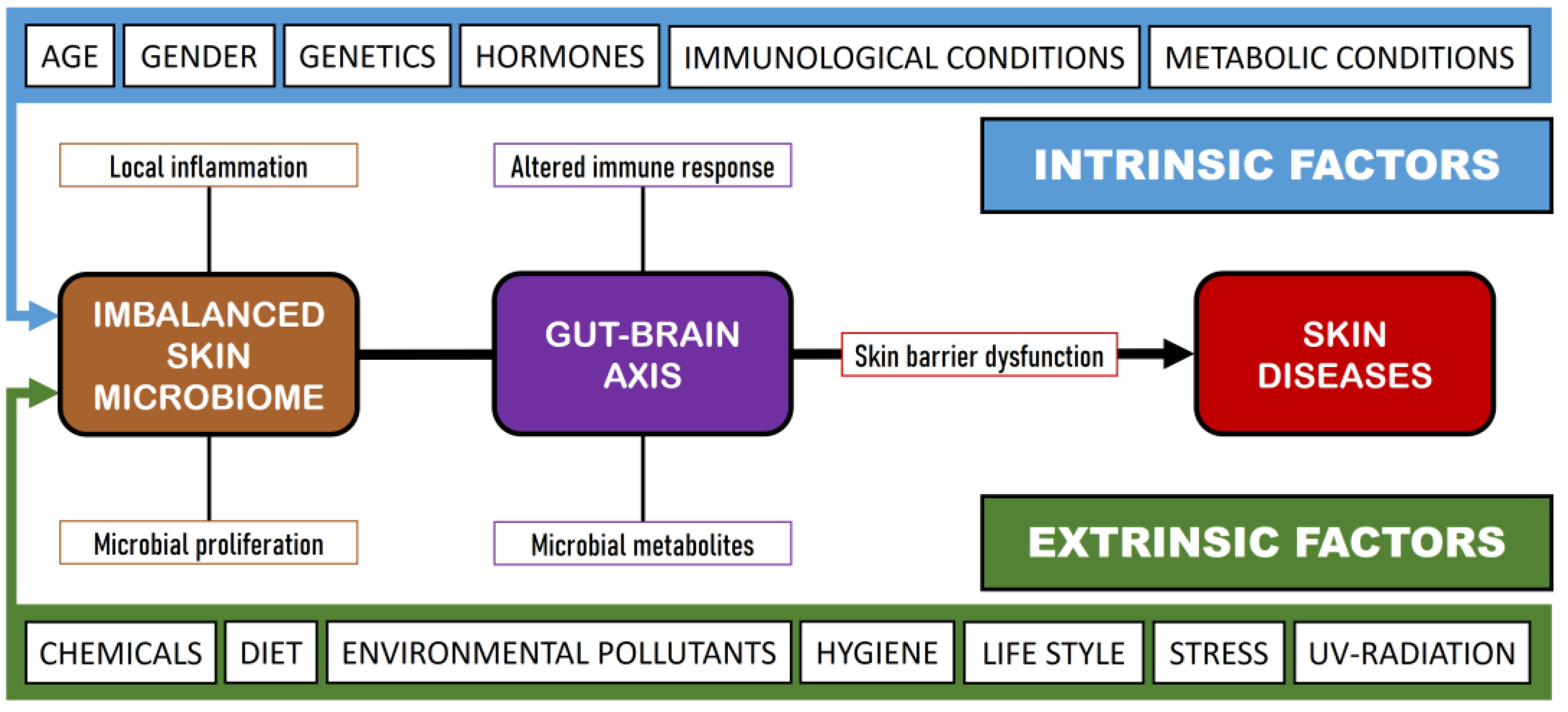
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).