

Prospective Analysis of Safety and Efficacy of Tenofovir Alafenamide Fumarate (TAF) in European Real-World Patients with Chronic Hepatitis B: A Single-Centre Real-Word Cohort Study

 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
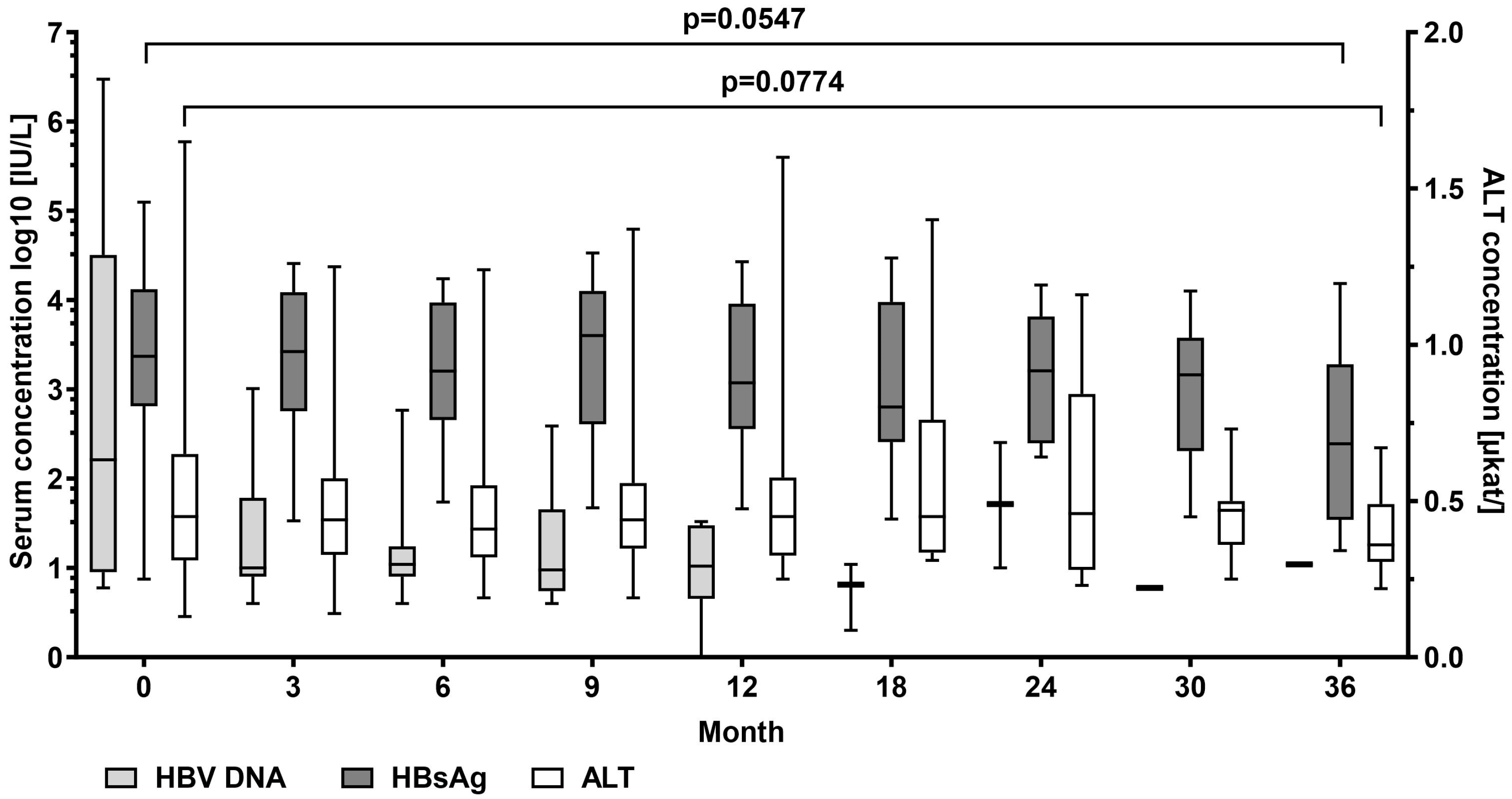
3.2. Virological Response
3.3. Fibrosis Indicators
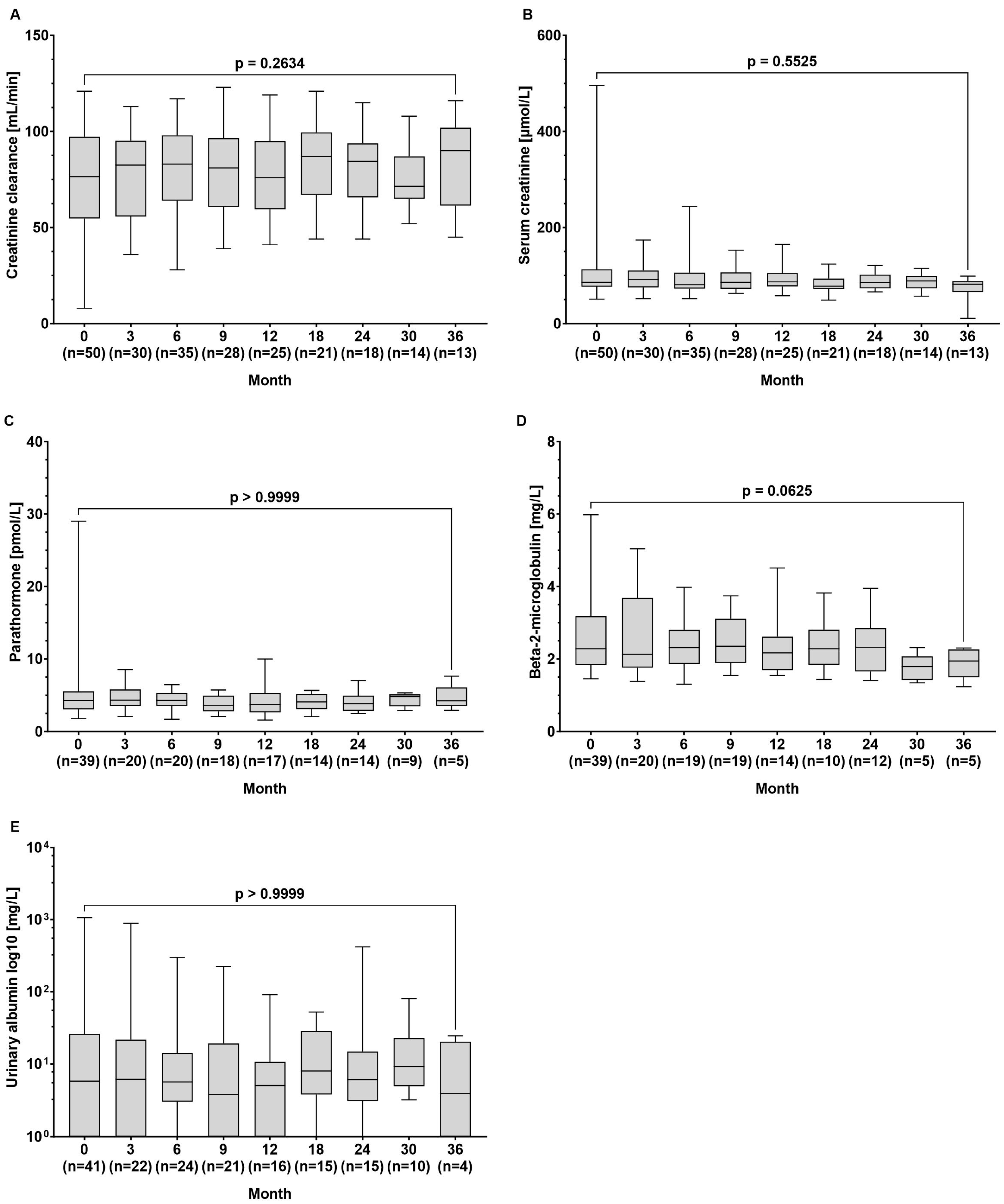
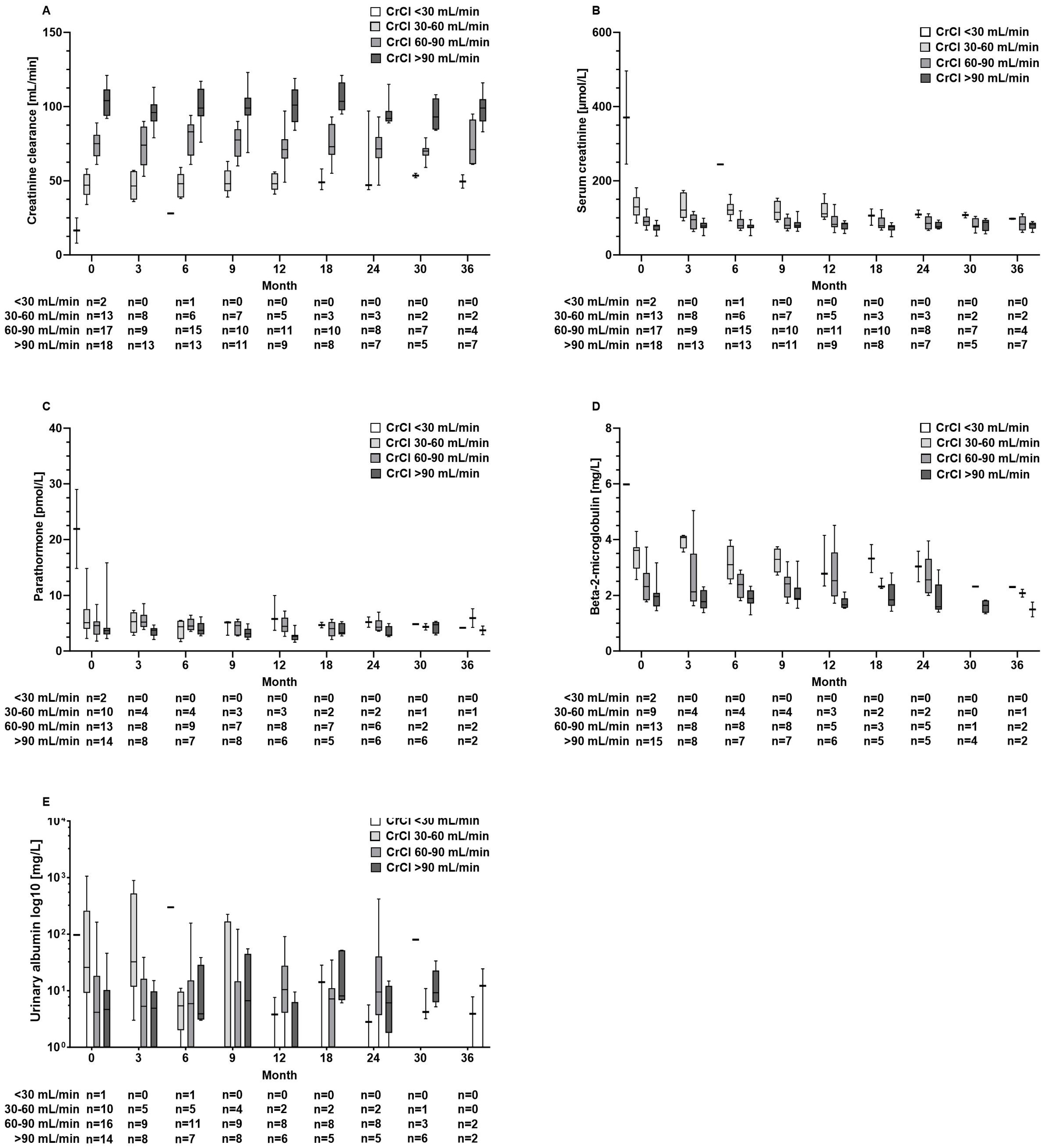
3.4. Renal Function and Bone Metabolism
3.5. Adverse Events
4. Discussion
4.1. Antiviral Efficacy of TAF
4.2. Renal Safety
4.3. Serum Markers of Bone Density
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Terrault, N.A.; Bzowej, N.H.; Chang, K.-M.; Hwang, J.P.; Jonas, M.M.; Murad, M.H. AASLD guidelines for treatment of chronic hepatitis B. Hepatology 2016, 63, 261–283. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef]
- Marcellin, P.; Gane, E.; Buti, M.; Afdhal, N.; Sievert, W.; Jacobson, I.M.; Washington, M.K.; Germanidis, G.; Flaherty, J.F.; Aguilar Schall, R.; et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: A 5-year open-label follow-up study. Lancet 2013, 381, 468–475. [Google Scholar] [CrossRef]
- Schmid, H.; Leo, M.; Thoene, K. Long-term effects of tenofovir on renal function in patients with chronic hepatitis B: A real-life observational study. J. Hepatol. 2016, 64, 227–230. [Google Scholar]
- Buti, M.; Wong, D.K.; Gane, E.; Flisiak, R.; Manns, M.; Kaita, K.; Janssen, H.L.A.; Op den Brouw, M.; Jump, B.; Kitrinos, K. Safety and efficacy of stopping tenofovir disoproxil fumarate in patients with chronic hepatitis B following at least 8 years of therapy: A prespecified follow-up analysis of two randomised trials. Lancet Gastroenterol. Hepatol. 2019, 4, 296–304. [Google Scholar] [CrossRef]
- Chan, H.L.; Fung, S.; Seto, W.K.; Chuang, W.L.; Chen, C.Y.; Kim, H.J.; Hui, A.J.; Janssen, H.L.; Chowdhury, A.; Tsang, T.Y.O.; et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate for the treatment of HBeAg-positive chronic hepatitis B virus infection: A randomised, double-blind, phase 3, non-inferiority trial. Lancet Gastroenterol. Hepatol. 2016, 1, 185–195. [Google Scholar] [CrossRef]
- Agarwal, K.; Brunetto, M.; Seto, W.K.; Lim, Y.S.; Fung, S.; Marcellin, P.; Ahn, S.H.; Izumi, N.; Chuang, W.L.; Bae, H.; et al. 96 weeks treatment of tenofovir alafenamide vs tenofovir disoproxil fumarate for hepatitis B virus infection. J. Hepatol. 2018, 68, 672–681. [Google Scholar] [CrossRef]
- Gane, E.J.; Lim, Y.-S.; Gordon, S.C.; Visvanathan, K.; Sicard, E.; Shouval, D.; Gaggar, A. The effect of tenofovir alafenamide on bone and renal safety compared with tenofovir disoproxil fumarate in patients with chronic hepatitis B virus infection: A randomised controlled trial. Lancet Gastroenterol. Hepatol. 2016, 1, 196–206. [Google Scholar]
- Mena, A.; Mora, M.; Mora, E.; García, F. Treatment of chronic hepatitis B: The role of tenofovir alafenamide. Infect. Drug Resist. 2017, 10, 197–205. [Google Scholar]
- Lampertico, P.; Chan, H.L.; Janssen, H.L.; Strasser, S.I.; Ahn, S.H.; Buti, M. Review article: Treatment of chronic hepatitis B virus infection—Perspectives on the current guidelines. Aliment. Pharmacol. Ther. 2017, 45, 1153–1168. [Google Scholar]
- Sano, T.; Amano, K.; Ide, T.; Kawaguchi, T.; Kuwahara, R.; Arinaga-Hino, T.; Koga, H.; Kuromatsu, R.; Torimura, T. Short-term efficacy after switching from adefovir dipivoxil and tenofovir disoproxil fumarate therapy to tenofovir alaferamide for chronic hepatitis B. Biomed. Rep. 2021, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.R.; Loomba, R.; Berg, T.; Aguilar Schall, R.E.; Yee, L.J.; Dinh, P.; Flaherty, J.F.; Martins, E.B.; Therneau, T.M.; Jacobson, I.; et al. Impact of baseline ALT and viral load on the efficacy of tenofovir disoproxil fumarate in chronic hepatitis B. J. Hepatol. 2021, 75, 67–75. [Google Scholar]
- Ghany, M.G.; Buti, M.; Lampertico, P.; Lee, H.M.; 2022 AASLD-EASL HBV-HDV Treatment Endpoints Conference Faculty. Guidance on treatment endpoints and study design for clinical trials aiming to achieve cure in chronic hepatitis B and D: Report from the 2022 AASLD-EASL HBV-HDV Treatment Endpoints Conference. J. Hepatol. 2023, 79, 1254–1269. [Google Scholar] [CrossRef]
- Lim, J.; Choi, W.M.; Shim, J.H.; Lee, D.; Kim, K.M.; Lim, Y.S.; Lee, H.C.; Choi, J. Efficacy and safety of tenofovir alafenamide versus tenofovir disoproxil fumarate in treatment-naïve chronic hepatitis B. Liver Int. 2022, 42, 1517–1527. [Google Scholar] [CrossRef]
- Nishikawa, T.; Matsui, M.; Onishi, S.; Ushiro, K.; Asai, A.; Kim, S.K.; Nishikawa, H. Long-Term Outcomes after Switching to Tenofovir Alafenamide in Patients with Chronic Hepatitis B. Int. J. Mol. Sci. 2024, 25, 2245. [Google Scholar] [CrossRef]
- Lim, Y.S.; Seto, W.K.; Kurosaki, M.; Fung, S.; Kao, J.H.; Hou, J.; Gordon, S.C.; Flaherty, J.F.; Yee, L.J.; Zhao, Y.; et al. Review article: Switching patients with chronic hepatitis B to tenofovir alafenamide-a review of current data. Aliment Pharmacol. Ther. 2022, 55, 921–943. [Google Scholar] [CrossRef]
- Hall, A.M.; Hendry, B.M.; Nitsch, D.; Connolly, J.O. Tenofovir-associated kidney toxicity in HIV-infected patients: A review of the evidence. Am. J. Kidney Dis. 2011, 57, 773–780. [Google Scholar] [CrossRef]
- Sax, P.E.; Wohl, D.; Yin, M.T.; Post, F.; DeJesus, E.; Saag, M.; Pozniak, A.; Thompson, M.; Podzamczer, D.; Molina, J.M.; et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate, coformulated with elvitegravir, cobicistat, and emtricitabine, for initial treatment of HIV-1 infection: Two randomised, double-blind, phase 3, non-inferiority trials. Lancet 2015, 385, 2606–2615. [Google Scholar] [CrossRef]
- Fernandez-Fernandez, B.; Montoya-Ferrer, A.; Sanz, A.B.; Sanchez-Niño, M.D.; Izquierdo, M.C.; Poveda, J.; Sainz-Prestel, V.; Ortiz-Martin, N.; Parra-Rodriguez, A.; Selgas, R.; et al. Tenofovir nephrotoxicity: 2011 update. AIDS Res. Treat. 2011, 2011, 354908. [Google Scholar] [CrossRef]
- Chan, H.L.Y.; Buti, M.; Lim, Y.S.; Agarwal, K.; Marcellin, P.; Brunetto, M.; Chuang, W.L.; Janssen, H.L.A.; Fung, S.; Izumi, N.; et al. Long-Term Treatment With Tenofovir Alafenamide for Chronic Hepatitis B Results in High Rates of Viral Suppression and Favorable Renal and Bone Safety. Am. J. Gastroenterol. 2024, 119, 486–496. [Google Scholar] [CrossRef]
- Reddy, R.; Curry, M.; Bae, H.; Dieterich, D.; Ankoma-Sey, V.; Pan, C.; Hann, H.W.; Tong, M.; Kim, W.R.; Kwo, P.; et al. Longer-term experience with tenofovir alafenamide (TAF) in HBVinfected patients; changes in EGFR, FIB4, ALT, and DNA suppression. J. Hepatol. 2020, 73, S653–S915. [Google Scholar] [CrossRef]
- Huynh, T.; Bui, D.M.; Zhou, T.X.; Hu, K.Q. Improvement of hepatic fibrosis after tenofovir disoproxil fumarate switching to tenofovir alafenamide for three years. World J. Hepatol. 2024, 16, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Tian, F.; Houle, S.K.D.; Alsabbagh, M.W.; Wong, W.W.L. Cost-Effectiveness of Tenofovir Alafenamide for Treatment of Chronic Hepatitis B in Canada. Pharmacoeconomics 2020, 38, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-H.; Shi, H.-Y.; Tsai, C.-E.; Yang, Y.-C.; Chiu, S.-U.F. Cost–Utility Analysis of Tenofovir Alafenamide and Entecavir in Chronic Hepatitis B Patients: A Markov Decision Model. Cancers 2024, 16, 813. [Google Scholar] [CrossRef]
- Stauffer, J.F.; Goldstein, D.A. Cost-effectiveness of Tenofovir alafenamide versus Tenofovir disoproxil fumarate for treatment of chronic hepatitis B. Clin. Drug Investig. 2015, 35, 315–324. [Google Scholar]
- Charlton, M.R.; Alam, A.; Shukla, A.; Dashtseren, B.; Lesmana, C.R.A.; Duger, D.; Payawal, D.A.; Duy Cuong, D.; Jargalsaikhan, G.; Cua, I.H.Y.; et al. An expert review on the use of tenofovir alafenamide for the treatment of chronic hepatitis B virus infection in Asia. J. Gastroenterol. 2020, 55, 811–823. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Number/Value |
|---|---|
| Male (%) | 35 (70%) |
| Age (years) | 56 (20–83) |
| Ethnicity (%) | |
| Caucasian | 37 (74%) |
| Asian | 8 (16%) |
| Middle East | 4 (8%) |
| African | 1 (2%) |
| BMI (kg/cm2) * | 27.0 (17.2–51.1) |
| Diabetes (%) | 12 (24%) |
| Hyperlipoproteinemia (%) | 9 (18%) |
| Liver cirrhosis (%) | 5 (10%) |
| HCC (%) | 1 (2%) |
| Detectable HBV DNA (%) | 20 (40%) |
| HBV DNA concentration (log10 IU/mL) * | 2.33 (0.76–6.47) |
| HBeAg-positive (%) | 10 (20%) |
| HBsAg concentration (log10 IU/mL) * | 3.38 (0.88–5.10) |
| Previous HBV treatment (%) | 41 (82%) |
| Tenofovir (%) | 26 (63%) |
| Entecavir (%) | 13 (32%) |
| Lamivudine (%) | 1 (2%) |
| Adefovir (%) | 1 (2%) |
| Duration of TAF treatment (month) * | 18 (3–36) |
| ALT (µkat/mL) * | 0.45 (0.13–1.65) |
| AST (µkat/mL) * | 0.49 (0.27–1.32) |
| AP (µkat/mL) * | 1.35 (0.59–3.23) |
| GGT (µkat/mL) * | 0.41 (0.14–7.05) |
| Albumin (g/L) * | 45.9 (36.0–51.5) |
| Bilirubin (µmol/L) * | 8.5 (2.9–27.9) |
| Hemoglobin (mmol/L) * | 8.9 (6.2–10.9) |
| Platelets (×109/L) * | 213 (57–489) |
| Leucocytes (×109/L) * | 6.4 (1.4–17.9) |
| FIB-4 score * | 1.53 (0.35–8.34) |
| APRI score * | 0.391 (0.086–2.250) |
| Creatinine (µmol/L) * | 86 (51–496) |
| Creatinine clearance (mL/min) * | 77 (8–121) |
| CrCl < 30 mL/min (%) | 2 (4%) |
| CrCl 30–60 mL/min (%) | 13 (26%) |
| CrCl 60–90 mL/min (%) | 17 (34%) |
| CrCl > 90 mL/min (%) | 18 (36%) |
| Beta-2-microglobulin (mg/L) * | 2.28 (1.45–5.98) |
| Urinary albumin (mg/L) * | 5.8 (0–1062) |
| Cholesterol (mmol/L) * | 4.20 (2.96–7.40) |
| HDL (mmol/L) * | 1.27 (0.80–2.01) |
| LDL (mmol/L) * | 2.79 (1.49–5.83) |
| Triglyceride (mmol/L) * | 1.23 (0.65–4.49) |
| Bonespecific alkaline phosphatase (µkat/mL) * | 18.5 (6.3–44.6) |
| Parathormon (pmol/L) * | 4.30 (1.79–29.0) |
| 25-Hydroxycholecalciferol (ng/mL) * | 22.5 (6.6–50.7) |
| Adverse Event | Number |
|---|---|
| Mild adverse events (%) | 14 (28%) |
| Exanthema | 2 (14%) |
| Headache | 2 (14%) |
| Fatigue | 3 (21%) |
| Abdominal pain | 3 (21%) |
| Arthalgia | 1 (7%) |
| Non-exertional dyspnea/perspiration | 1 (7%) |
| Dizzines | 1 (7%) |
| CK, AST, and LDH increase | 1 (7%) |
| Severe adverse events | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fülöp, B.; Fischer, J.; Hahn, M.; Böhlig, A.; Matz-Soja, M.; Berg, T.; van Bömmel, F. Prospective Analysis of Safety and Efficacy of Tenofovir Alafenamide Fumarate (TAF) in European Real-World Patients with Chronic Hepatitis B: A Single-Centre Real-Word Cohort Study. Pathogens 2024, 13, 820. https://doi.org/10.3390/pathogens13090820
Fülöp B, Fischer J, Hahn M, Böhlig A, Matz-Soja M, Berg T, van Bömmel F. Prospective Analysis of Safety and Efficacy of Tenofovir Alafenamide Fumarate (TAF) in European Real-World Patients with Chronic Hepatitis B: A Single-Centre Real-Word Cohort Study. Pathogens. 2024; 13(9):820. https://doi.org/10.3390/pathogens13090820
Chicago/Turabian StyleFülöp, Balazs, Janett Fischer, Magdalena Hahn, Albrecht Böhlig, Madlen Matz-Soja, Thomas Berg, and Florian van Bömmel. 2024. "Prospective Analysis of Safety and Efficacy of Tenofovir Alafenamide Fumarate (TAF) in European Real-World Patients with Chronic Hepatitis B: A Single-Centre Real-Word Cohort Study" Pathogens 13, no. 9: 820. https://doi.org/10.3390/pathogens13090820
APA StyleFülöp, B., Fischer, J., Hahn, M., Böhlig, A., Matz-Soja, M., Berg, T., & van Bömmel, F. (2024). Prospective Analysis of Safety and Efficacy of Tenofovir Alafenamide Fumarate (TAF) in European Real-World Patients with Chronic Hepatitis B: A Single-Centre Real-Word Cohort Study. Pathogens, 13(9), 820. https://doi.org/10.3390/pathogens13090820