
Efficacy of Violet-Blue (405 nm) LED Lamps for Disinfection of High-Environmental-Contact Surfaces in Healthcare Facilities: Leading to the Inactivation of Microorganisms and Reduction of MRSA Contamination

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
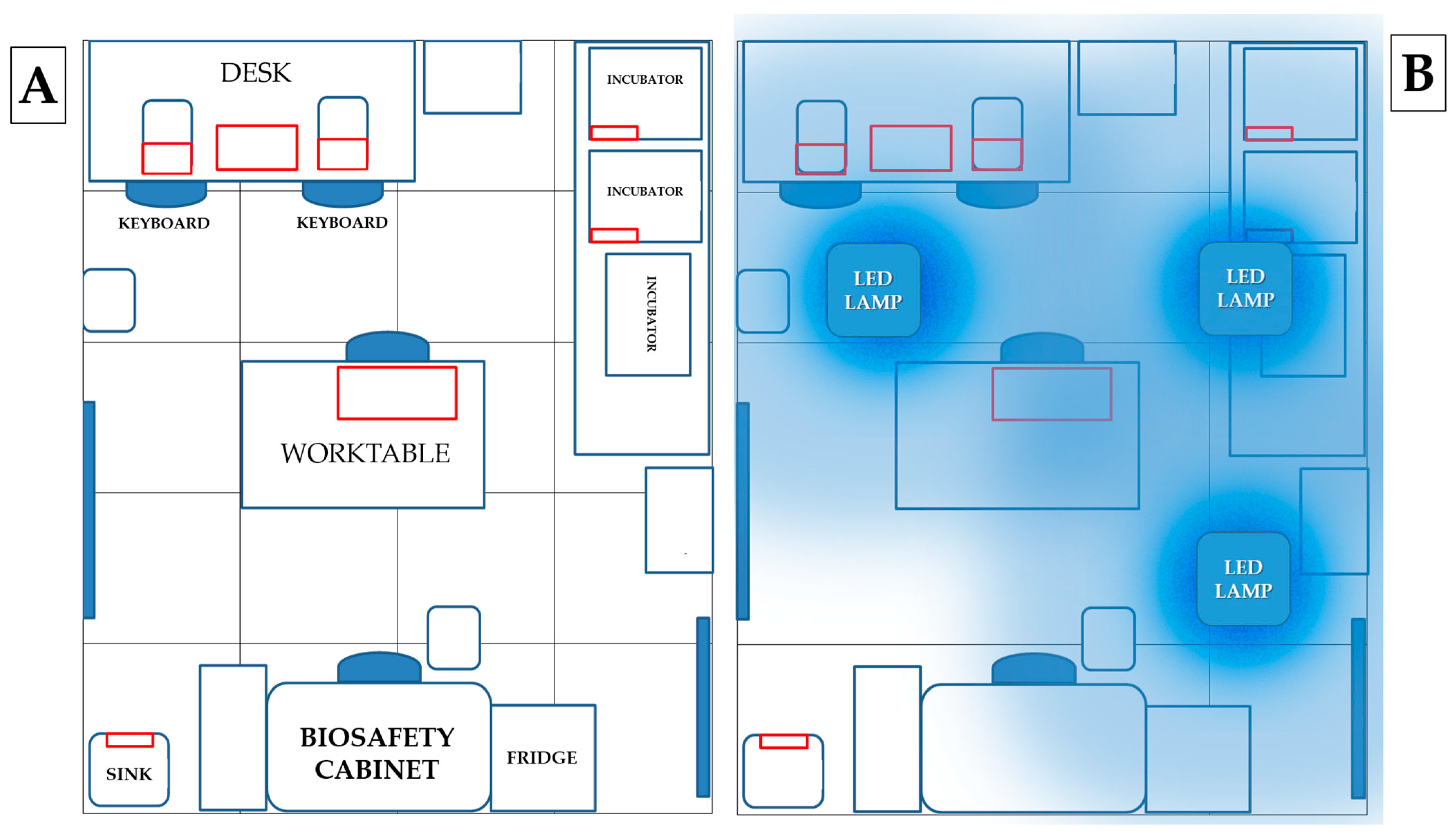
2.2. Simulation Model
2.3. High Touch Surface Sampling
2.4. Sampling of Surfaces Contaminated with MRSA
2.5. Statistical Analysis and Data Processing
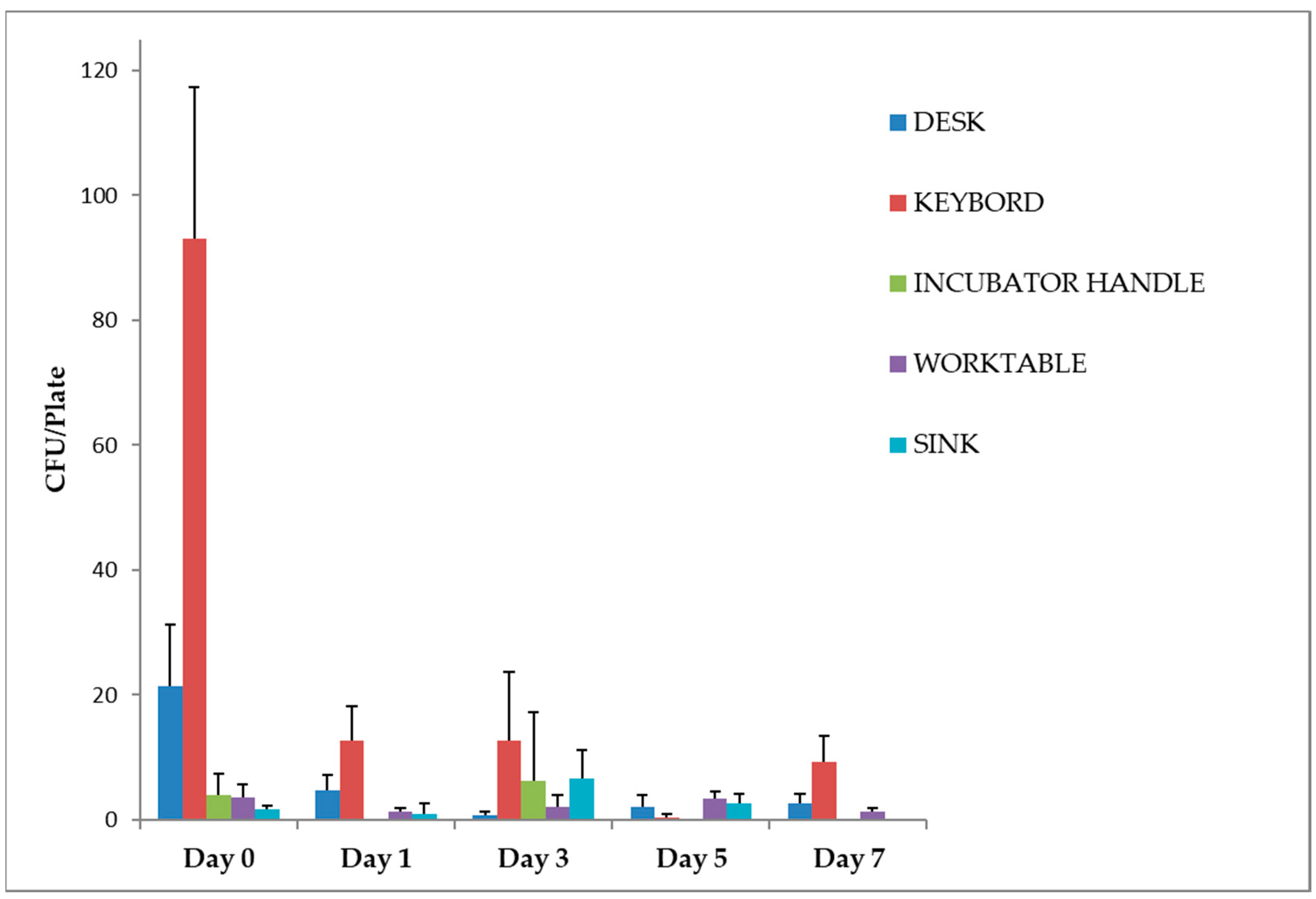
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klevens, R.M.; Edwards, J.R.; Richards, C.L.; Horan, T.C.; Gaynes, R.P.; Pollock, D.A.; Cardo, D.M. Estimating Health Care-Associated Infections and Deaths in U.S. Hospitals, 2002. Public Health Rep. 2007, 122, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Zimlichman, E.; Henderson, D.; Tamir, O.; Franz, C.; Song, P.; Yamin, C.K.; Keohane, C.; Denham, C.R.; Bates, D.W. Health Care-Associated Infections: A Meta-Analysis of Costs and Financial Impact on the US Health Care System. JAMA Intern. Med. 2013, 173, 2039–2046. [Google Scholar] [CrossRef] [PubMed]
- Bearman, G.; Bryant, K.; Leekha, S.; Mayer, J.; Munoz-Price, L.S.; Murthy, R.; Palmore, T.; Rupp, M.E.; White, J. Healthcare Personnel Attire in Non-Operating-Room Settings. Infect. Control Hosp. Epidemiol. 2014, 35, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Wiener-Well, Y.; Galuty, M.; Rudensky, B.; Schlesinger, Y.; Attias, D.; Yinnon, A.M. Nursing and Physician Attire as Possible Source of Nosocomial Infections. Am. J. Infect. Control 2011, 39, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Allegranzi, B.; Pittet, D. Role of Hand Hygiene in Healthcare-Associated Infection Prevention. J. Hosp. Infect. 2009, 73, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Pittet, D.; Allegranzi, B.; Boyce, J. World Health Organization World Alliance for Patient Safety First Global Patient Safety Challenge Core Group of Experts. The World Health Organization Guidelines on Hand Hygiene in Health Care and Their Consensus Recommendations. Infect. Control Hosp. Epidemiol. 2009, 30, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.J.; Diekema, D.J.; Sepkowitz, K.; Perencevich, E.N. Adverse Outcomes Associated with Contact Precautions: A Review of the Literature. Am. J. Infect. Control 2009, 37, 85–93. [Google Scholar] [CrossRef]
- Erasmus, V.; Daha, T.J.; Brug, H.; Richardus, J.H.; Behrendt, M.D.; Vos, M.C.; van Beeck, E.F. Systematic Review of Studies on Compliance with Hand Hygiene Guidelines in Hospital Care. Infect. Control Hosp. Epidemiol. 2010, 31, 283–294. [Google Scholar] [CrossRef]
- Saint, S.; Kowalski, C.P.; Kaufman, S.R.; Hofer, T.P.; Kauffman, C.A.; Olmsted, R.N.; Forman, J.; Banaszak-Holl, J.; Damschroder, L.; Krein, S.L. Preventing Hospital-Acquired Urinary Tract Infection in the United States: A National Study. Clin. Infect. Dis. 2008, 46, 243–250. [Google Scholar] [CrossRef]
- Mody, L.; Meddings, J.; Edson, B.S.; McNamara, S.E.; Trautner, B.W.; Stone, N.D.; Krein, S.L.; Saint, S. Enhancing Resident Safety by Preventing Healthcare-Associated Infection: A National Initiative to Reduce Catheter-Associated Urinary Tract Infections in Nursing Homes. Clin. Infect. Dis. 2015, 61, 86–94. [Google Scholar] [CrossRef]
- Boyce, J.M.; Pittet, D.; Healthcare Infection Control Practices Advisory Committee HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm. Rep. 2002, 51, 1–45, 1-CE4. [Google Scholar] [PubMed]
- World Health Organization. Guidelines on Core Components of Infection Prevention and Control Programmes at the National and Acute Health Care Facility Level; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-154992-9. [Google Scholar]
- Carling, P.C.; Parry, M.F.; Bruno-Murtha, L.A.; Dick, B. Improving Environmental Hygiene in 27 Intensive Care Units to Decrease Multidrug-Resistant Bacterial Transmission. Crit. Care Med. 2010, 38, 1054–1059. [Google Scholar] [CrossRef] [PubMed]
- Manzi, P.; Messina, G.; Falcone, V.; Cevenini, G.; Bernardini, I.; De Lio, C.; Pieri, L.; De Filippis, G.; Violi, S. Permanent environmental disinfection techniques in hospital settings with infectious risk. Ig. Sanita Pubblica 2021, 80, 676–692. [Google Scholar]
- Weber, D.J.; Rutala, W.A.; Miller, M.B.; Huslage, K.; Sickbert-Bennett, E. Role of Hospital Surfaces in the Transmission of Emerging Health Care-Associated Pathogens: Norovirus, Clostridium Difficile, and Acinetobacter Species. Am. J. Infect. Control 2010, 38, S25–S33. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J.M.; Havill, N.L.; Otter, J.A.; McDonald, L.C.; Adams, N.M.T.; Cooper, T.; Thompson, A.; Wiggs, L.; Killgore, G.; Tauman, A.; et al. Impact of Hydrogen Peroxide Vapor Room Decontamination on Clostridium Difficile Environmental Contamination and Transmission in a Healthcare Setting. Infect. Control Hosp. Epidemiol. 2008, 29, 723–729. [Google Scholar] [CrossRef]
- Kowalski, W. Ultraviolet Germicidal Irradiation Handbook: UVGI for Air and Surface Disinfection; Springer: Berlin/Heidelberg, Germany, 2009; ISBN 978-3-642-01998-2. [Google Scholar]
- Messina, G.; Fattorini, M.; Nante, N.; Rosadini, D.; Serafini, A.; Tani, M.; Cevenini, G. Time Effectiveness of Ultraviolet C Light (UVC) Emitted by Light Emitting Diodes (LEDs) in Reducing Stethoscope Contamination. Int. J. Environ. Res. Public Health 2016, 13, 940. [Google Scholar] [CrossRef]
- Russo, C.; Bartolini, D.; Corbucci, C.; Stabile, A.M.; Rende, M.; Gioiello, A.; Cruciani, G.; Mencacci, A.; Galli, F.; Pietrella, D. Effect of a UV-C Automatic Last-Generation Mobile Robotic System on Multi-Drug Resistant Pathogens. Int. J. Environ. Res. Public Health 2021, 18, 13019. [Google Scholar] [CrossRef]
- Casini, B.; Tuvo, B.; Cristina, M.L.; Spagnolo, A.M.; Totaro, M.; Baggiani, A.; Privitera, G.P. Evaluation of an Ultraviolet C (UVC) Light-Emitting Device for Disinfection of High Touch Surfaces in Hospital Critical Areas. Int. J. Environ. Res. Public Health 2019, 16, 3572. [Google Scholar] [CrossRef]
- Yang, J.-H.; Wu, U.-I.; Tai, H.-M.; Sheng, W.-H. Effectiveness of an Ultraviolet-C Disinfection System for Reduction of Healthcare-Associated Pathogens. J. Microbiol. Immunol. Infect. 2019, 52, 487–493. [Google Scholar] [CrossRef]
- Miller, S.L.; Linnes, J.; Luongo, J. Ultraviolet Germicidal Irradiation: Future Directions for Air Disinfection and Building Applications. Photochem. Photobiol. 2013, 89, 777–781. [Google Scholar] [CrossRef]
- Ramos, C.C.R.; Roque, J.L.A.; Sarmiento, D.B.; Suarez, L.E.G.; Sunio, J.T.P.; Tabungar, K.I.B.; Tengco, G.S.C.; Rio, P.C.; Hilario, A.L. Use of Ultraviolet-C in Environmental Sterilization in Hospitals: A Systematic Review on Efficacy and Safety. Int. J. Health Sci. 2020, 14, 52–65. [Google Scholar]
- Maclean, M.; McKenzie, K.; Anderson, J.G.; Gettinby, G.; MacGregor, S.J. 405 Nm Light Technology for the Inactivation of Pathogens and Its Potential Role for Environmental Disinfection and Infection Control. J. Hosp. Infect. 2014, 88, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Amodeo, D.; Lucarelli, V.; De Palma, I.; Puccio, A.; Nante, N.; Cevenini, G.; Messina, G. Efficacy of Violet–Blue Light to Inactive Microbial Growth. Sci. Rep. 2022, 12, 20179. [Google Scholar] [CrossRef] [PubMed]
- Frilli, E.; Amodeo, D.; Cevenini, G.; Nante, N.; Messina, G. Effectiveness of Near-UVA in SARS-CoV-2 Inactivation. Epidemiol. Infect. 2023, 151, e76. [Google Scholar] [CrossRef] [PubMed]
- Hamblin, M.R.; Hasan, T. Photodynamic Therapy: A New Antimicrobial Approach to Infectious Disease? Photochem. Photobiol. Sci. 2004, 3, 436–450. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Wang, Y.; Murray, C.K.; Hamblin, M.R.; Hooper, D.C.; Dai, T. Antimicrobial Blue Light Inactivation of Pathogenic Microbes: State of the Art. Drug Resist. Updates 2017, 33–35, 1–22. [Google Scholar] [CrossRef]
- Shehatou, C.; Logunov, S.L.; Dunman, P.M.; Haidaris, C.G.; Klubben, W.S. Characterizing the Antimicrobial Properties of 405 Nm Light and the Corning® Light-Diffusing Fiber Delivery System. Lasers Surg. Med. 2019, 51, 887. [Google Scholar] [CrossRef]
- Cabral, J.; Ag, R. Blue Light Disinfection in Hospital Infection Control: Advantages, Drawbacks, and Pitfalls. Antibiotics 2019, 8, 58. [Google Scholar] [CrossRef]
- Chen, W.; Yang, H.; Peng, C.; Wu, T. Resolving the “Health vs Environment” Dilemma with Sustainable Disinfection during the COVID-19 Pandemic. Environ. Sci. Pollut. Res. 2023, 30, 24737–24741. [Google Scholar] [CrossRef]
- Sehulster, L.; Chinn, R.Y.; CDC; HICPAC. Guidelines for environmental infection control in health-care facilities. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR Recomm. Rep. 2003, 52, 1–42. [Google Scholar]
- Murrell, L.J.; Hamilton, E.K.; Johnson, H.B.; Spencer, M. Influence of a Visible-Light Continuous Environmental Disinfection System on Microbial Contamination and Surgical Site Infections in an Orthopedic Operating Room. Am. J. Infect. Control 2019, 47, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Maclean, M.; Booth, M.; Anderson, J.; MacGregor, S.; Woolsey, G.; Coia, J.; Hamilton, K.; Gettinby, G. Continuous Decontamination of an Intensive Care Isolation Room during Patient Occupancy Using 405 Nm Light Technology. J. Infect. Prev. 2013, 14, 176–181. [Google Scholar] [CrossRef]
- Bache, S.E.; Maclean, M.; Gettinby, G.; Anderson, J.G.; MacGregor, S.J.; Taggart, I. Universal Decontamination of Hospital Surfaces in an Occupied Inpatient Room with a Continuous 405 Nm Light Source. J. Hosp. Infect. 2018, 98, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.; Schwebke, I.; Kampf, G. How Long Do Nosocomial Pathogens Persist on Inanimate Surfaces? A Systematic Review. BMC Infect. Dis. 2006, 6, 130. [Google Scholar] [CrossRef]
- Walker, P.; Taylor, A.J.; Hitchcock, A.; Webb, J.P.; Green, J.; Weinstein, J.; Kelly, D.J. Exploiting Violet-Blue Light to Kill Campylobacter Jejuni: Analysis of Global Responses, Modeling of Transcription Factor Activities, and Identification of Protein Targets. mSystems 2022, 7, e00454-22. [Google Scholar] [CrossRef]
- Lipovsky, A.; Nitzan, Y.; Friedmann, H.; Lubart, R. Sensitivity of Staphylococcus Aureus Strains to Broadband Visible Light. Photochem. Photobiol. 2009, 85, 255–260. [Google Scholar] [CrossRef]
- Tomb, R.M.; Maclean, M.; Coia, J.E.; MacGregor, S.J.; Anderson, J.G. Assessment of the Potential for Resistance to Antimicrobial Violet-Blue Light in Staphylococcus Aureus. Antimicrob. Resist. Infect. Control 2017, 6, 100. [Google Scholar] [CrossRef]
- Maclean, M.; MacGregor, S.J.; Anderson, J.G.; Woolsey, G. High-Intensity Narrow-Spectrum Light Inactivation and Wavelength Sensitivity of Staphylococcus Aureus. FEMS Microbiol. Lett. 2008, 285, 227–232. [Google Scholar] [CrossRef]
- Enwemeka, C.S.; Williams, D.; Hollosi, S.; Yens, D.; Enwemeka, S.K. Visible 405 Nm SLD Light Photo-Destroys Methicillin-Resistant Staphylococcus Aureus (MRSA) in Vitro. Lasers Surg. Med. 2008, 40, 734–737. [Google Scholar] [CrossRef]
- Soro, A.B.; Ekhlas, D.; Marmion, M.; Scannell, A.G.M.; Whyte, P.; Bolton, D.J.; Burgess, C.M.; Tiwari, B.K. Investigation of Differences in Susceptibility of Campylobacter Jejuni Strains to UV Light-Emitting Diode (UV-LED) Technology. Sci. Rep. 2023, 13, 9459. [Google Scholar] [CrossRef]
- Andrady, A.L.; Hamid, S.H.; Hu, X.; Torikai, A. Effects of Increased Solar Ultraviolet Radiation on Materials. J. Photochem. Photobiol. B 1998, 46, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Irving, D.; Lamprou, D.A.; Maclean, M.; MacGregor, S.J.; Anderson, J.G.; Grant, M.H. A Comparison Study of the Degradative Effects and Safety Implications of UVC and 405 Nm Germicidal Light Sources for Endoscope Storage. Polym. Degrad. Stab. 2016, 133, 249–254. [Google Scholar] [CrossRef]
- Matsumura, Y.; Ananthaswamy, H.N. Toxic Effects of Ultraviolet Radiation on the Skin. Toxicol. Appl. Pharmacol. 2004, 195, 298–308. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Non-Ionizing Radiation Protection (ICNIRP) Guidelines for Limiting Exposure to Electromagnetic Fields (100 kHz to 300 GHz). Health Phys. 2020, 118, 483–524. [CrossRef]
- Dai, T.; Gupta, A.; Huang, Y.-Y.; Yin, R.; Murray, C.K.; Vrahas, M.S.; Sherwood, M.E.; Tegos, G.P.; Hamblin, M.R. Blue Light Rescues Mice from Potentially Fatal Pseudomonas Aeruginosa Burn Infection: Efficacy, Safety, and Mechanism of Action. Antimicrob. Agents Chemother. 2013, 57, 1238–1245. [Google Scholar] [CrossRef]
- Kleinpenning, M.M.; Smits, T.; Frunt, M.H.A.; van Erp, P.E.J.; van de Kerkhof, P.C.M.; Gerritsen, R.M.J.P. Clinical and Histological Effects of Blue Light on Normal Skin. Photodermatol. Photoimmunol. Photomed. 2010, 26, 16–21. [Google Scholar] [CrossRef]
- Ramakrishnan, P.; Maclean, M.; MacGregor, S.J.; Anderson, J.G.; Grant, M.H. Differential Sensitivity of Osteoblasts and Bacterial Pathogens to 405-Nm Light Highlighting Potential for Decontamination Applications in Orthopedic Surgery. J. Biomed. Opt. 2014, 19, 105001. [Google Scholar] [CrossRef]
- Moorhead, S.; Maclean, M.; Coia, J.E.; MacGregor, S.J.; Anderson, J.G. Synergistic Efficacy of 405 Nm Light and Chlorinated Disinfectants for the Enhanced Decontamination of Clostridium Difficile Spores. Anaerobe 2016, 37, 72–77. [Google Scholar] [CrossRef]
- Messina, G.; Bosco, R.; Amodeo, D.; Nante, N.; De Palma, I.; Petri, C.; Cevenini, G. Safer School with Near-UV Technology: Novel Applications for Environmental Hygiene. J. Environ. Health Sci. Eng. 2023, 21, 157–165. [Google Scholar] [CrossRef]
- CEI-CEI EN 62471-5. Available online: https://mycatalogo.ceinorme.it/cei/item/0000014644/ (accessed on 20 July 2023).
- Jing, Z.; Liu, J.; Ibrahim, M.S.; Fan, J.; Fan, X.; Zhang, G. Lifetime Prediction of Ultraviolet Light-Emitting Diodes Using a Long Short-Term Memory Recurrent Neural Network. IEEE Electron Device Lett. 2020, 41, 1817–1820. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Position | Height from Floor | Simulated Irradiance | Energy Dose * |
|---|---|---|---|
| (cm) | (W/m2) | (J/cm2) | |
| Incubator handle | 75 | 10 | 64.8 |
| Desk | 90 | 9.5 | 61.6 |
| Worktable | 130 | 8.5 | 55.1 |
| Keyboards | 92 | 8.5 | 55.1 |
| Sink | 80 | 1.5 | 9.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amodeo, D.; Manzi, P.; De Palma, I.; Puccio, A.; Nante, N.; Barcaccia, M.; Marini, D.; Pietrella, D. Efficacy of Violet-Blue (405 nm) LED Lamps for Disinfection of High-Environmental-Contact Surfaces in Healthcare Facilities: Leading to the Inactivation of Microorganisms and Reduction of MRSA Contamination. Pathogens 2023, 12, 1338. https://doi.org/10.3390/pathogens12111338
Amodeo D, Manzi P, De Palma I, Puccio A, Nante N, Barcaccia M, Marini D, Pietrella D. Efficacy of Violet-Blue (405 nm) LED Lamps for Disinfection of High-Environmental-Contact Surfaces in Healthcare Facilities: Leading to the Inactivation of Microorganisms and Reduction of MRSA Contamination. Pathogens. 2023; 12(11):1338. https://doi.org/10.3390/pathogens12111338
Chicago/Turabian StyleAmodeo, Davide, Pietro Manzi, Isa De Palma, Alessandro Puccio, Nicola Nante, Mariella Barcaccia, Daniele Marini, and Donatella Pietrella. 2023. "Efficacy of Violet-Blue (405 nm) LED Lamps for Disinfection of High-Environmental-Contact Surfaces in Healthcare Facilities: Leading to the Inactivation of Microorganisms and Reduction of MRSA Contamination" Pathogens 12, no. 11: 1338. https://doi.org/10.3390/pathogens12111338
APA StyleAmodeo, D., Manzi, P., De Palma, I., Puccio, A., Nante, N., Barcaccia, M., Marini, D., & Pietrella, D. (2023). Efficacy of Violet-Blue (405 nm) LED Lamps for Disinfection of High-Environmental-Contact Surfaces in Healthcare Facilities: Leading to the Inactivation of Microorganisms and Reduction of MRSA Contamination. Pathogens, 12(11), 1338. https://doi.org/10.3390/pathogens12111338