
Cryptococcal Meningitis in Kidney Transplant Recipients: A Two-Decade Cohort Study in France

 , ,
, ,  , , , ,
, , , ,  , ,
, ,  , , , , , ,
, , , , , ,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Definitions
2.3. Inclusion Criteria
2.4. Clinical Symptoms and Laboratory Studies
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. General Characteristics of Patients with CM
3.1.1. Clinical Features
3.1.2. Biological Characteristics
3.1.3. Immunosuppressive Regimen
3.1.4. Therapeutic Management
3.1.5. Determinants of CM
3.2. Prognosis of CM vs. Non-CM Cryptococcosis
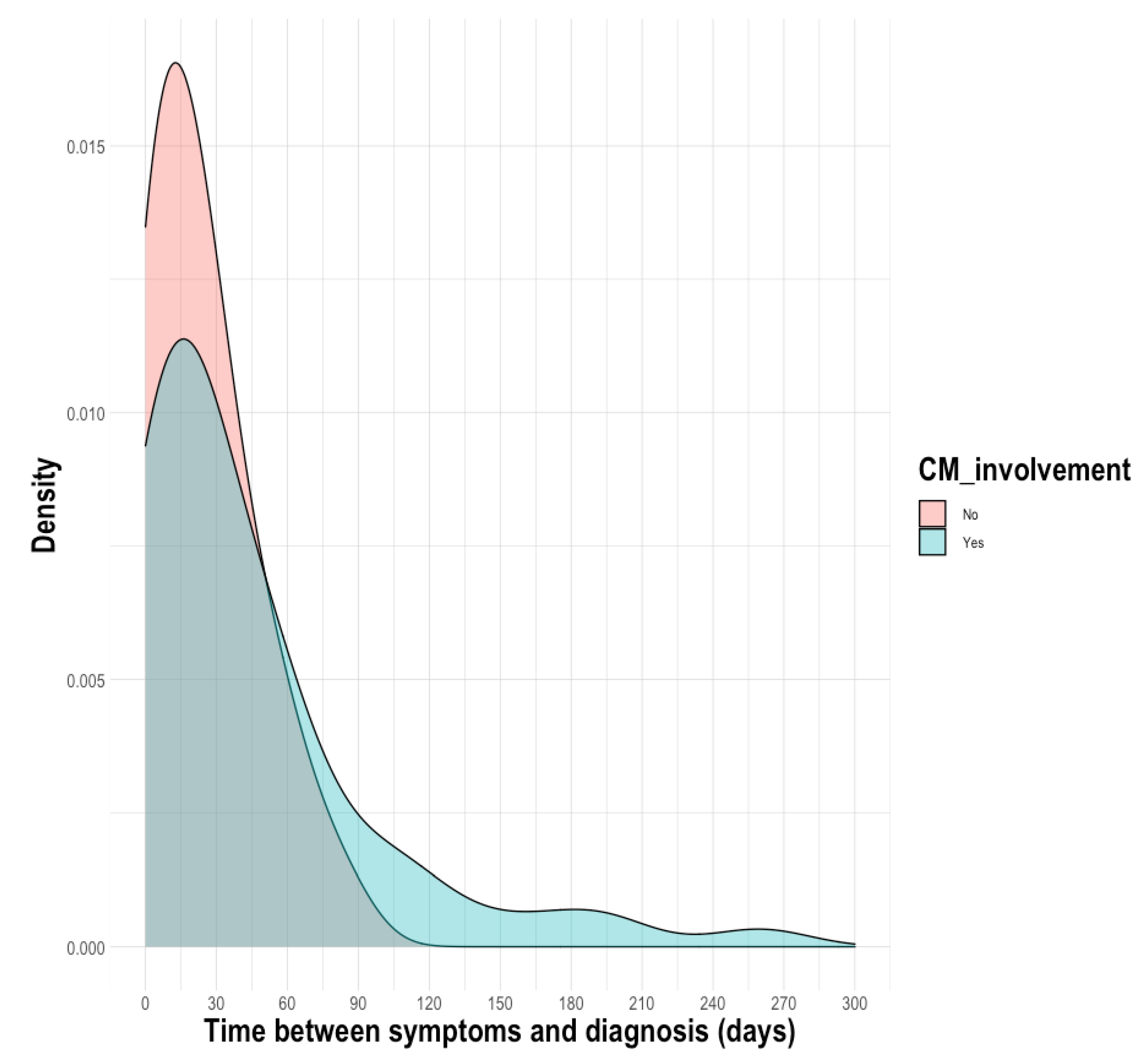
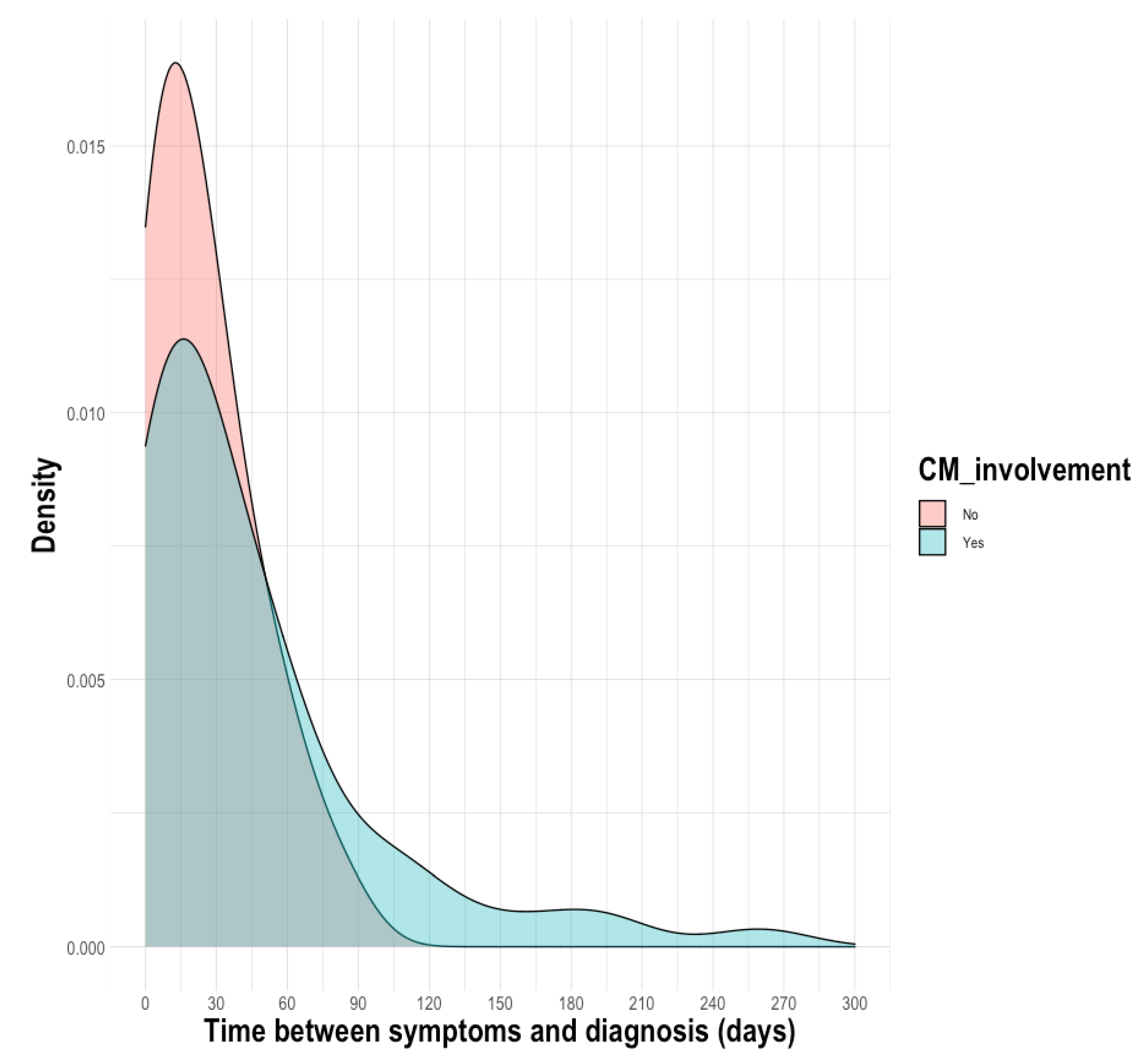
3.2.1. Diagnostic Delay
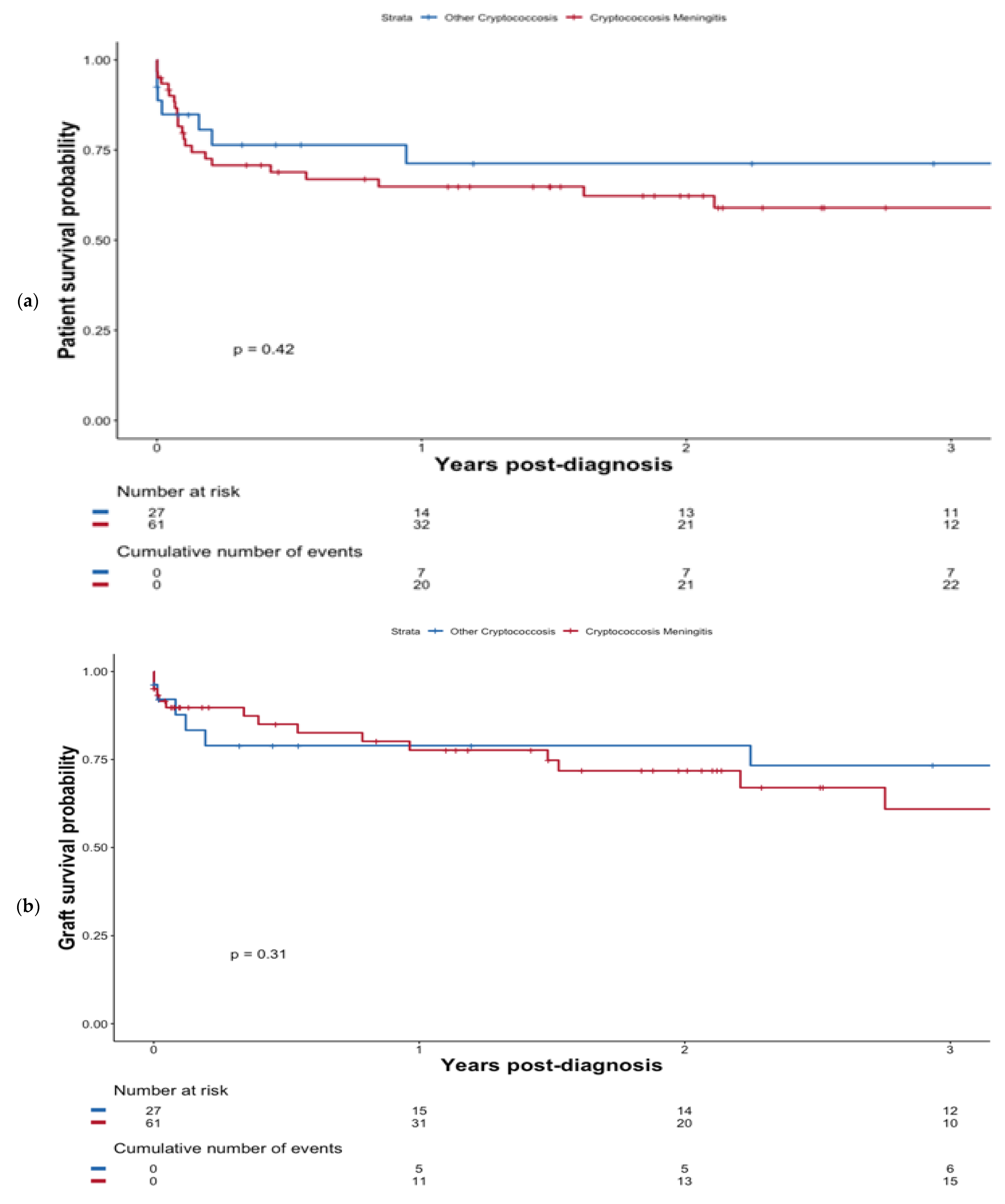
3.2.2. Patient Outcomes
3.2.3. Graft Survival
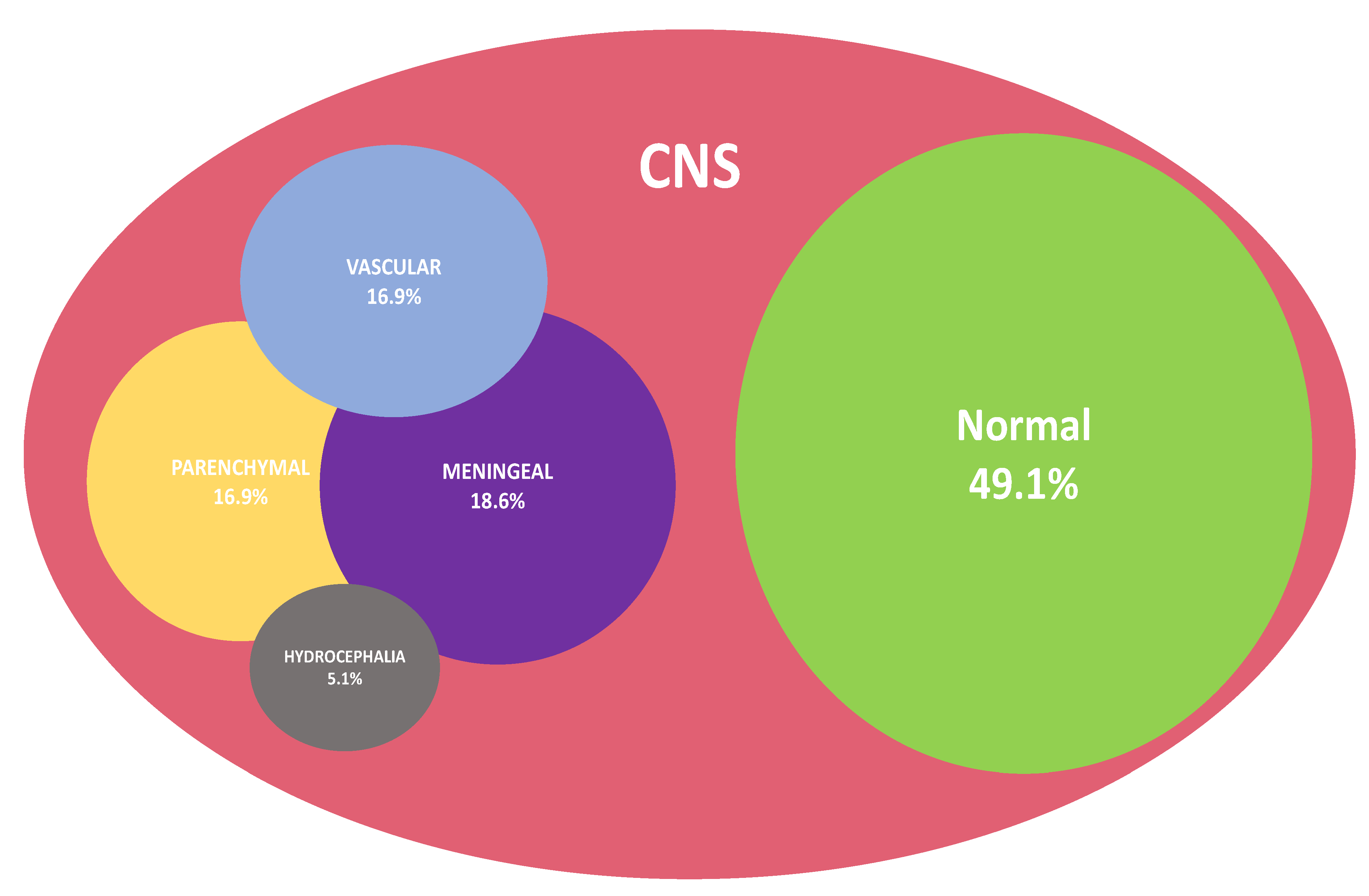
3.3. CM-Associated Features in Brain Imaging
3.3.1. Radiological Characteristics
3.3.2. Clinical Presentation According to Brain Injury Pattern
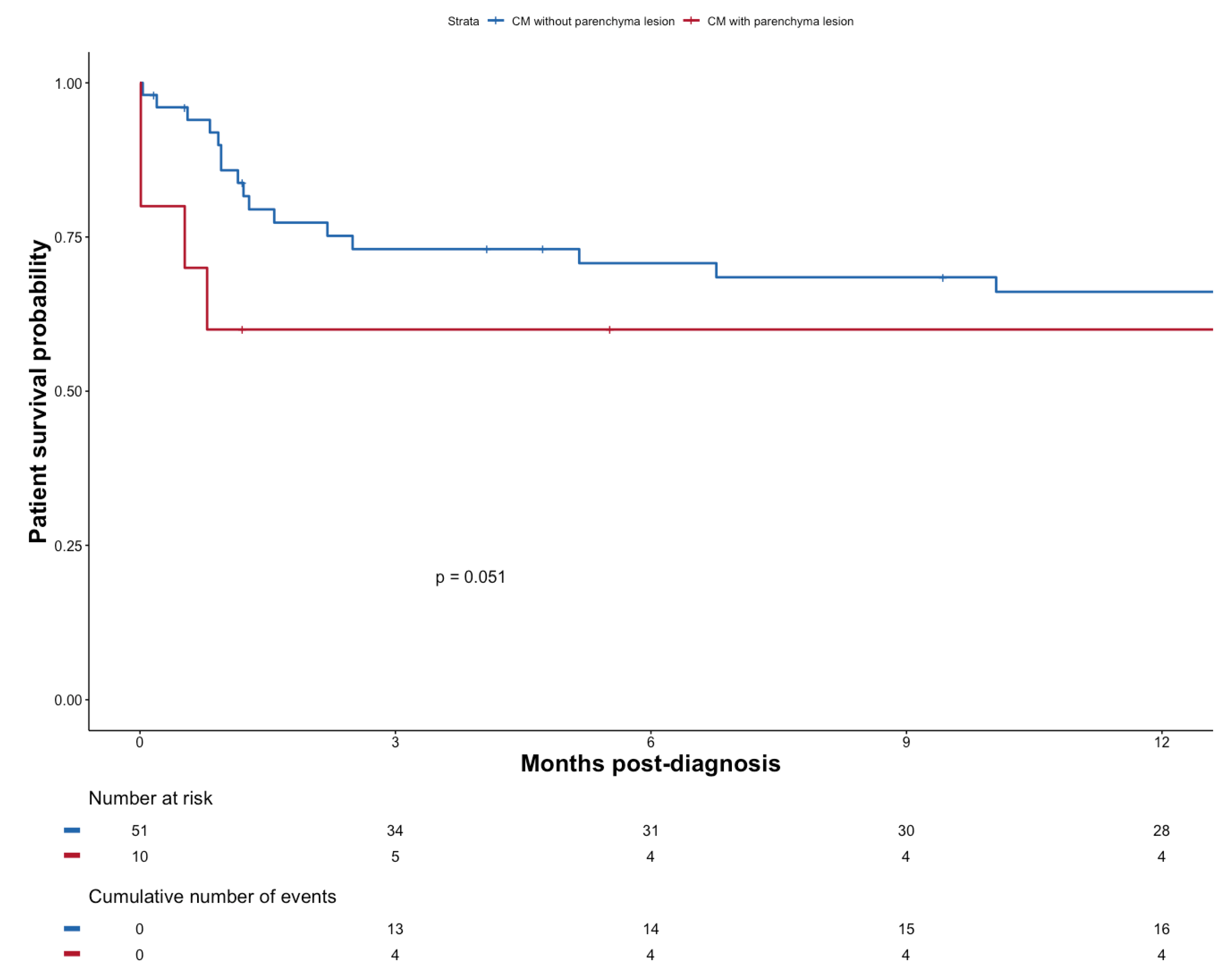
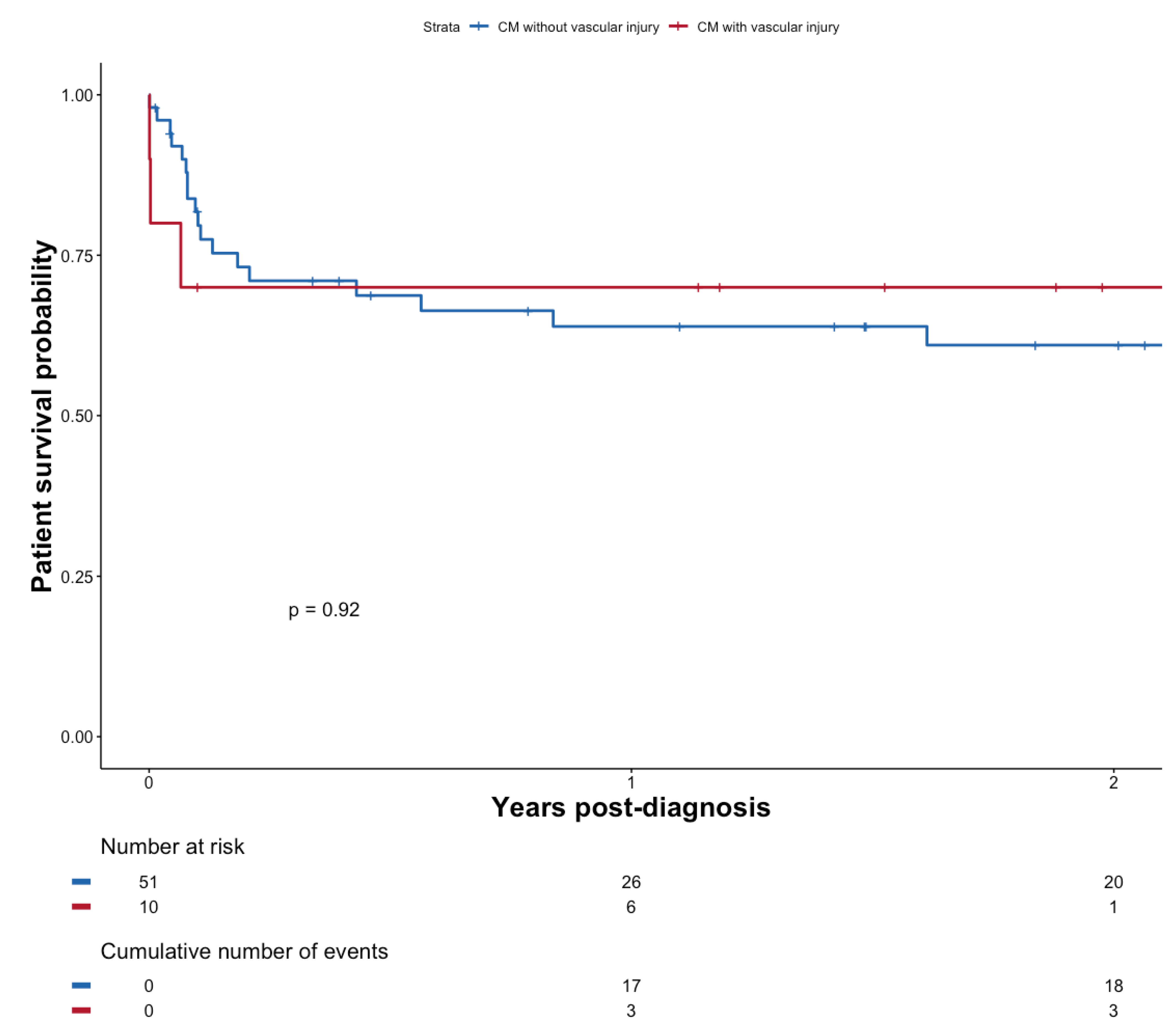
3.3.3. Outcomes According to the Type of Radiological Characteristics
4. Discussion
4.1. Clinical Features and Risk Factors
4.2. Outcome
4.3. Characteristics Based on CNS Imaging
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Ethics Approval
Conflicts of Interest
References
- Pappas, P.G.; Alexander, B.D.; Andes, D.; Hadley, S.; Kauffman, C.A.; Freifeld, A.; Anaissie, E.J.; Brumble, L.M.; Herwaldt, L.; Ito, J.; et al. Invasive Fungal Infections among Organ Transplant Recipients: Results of the Transplant—Associated Infection Surveillance Network (TRANSNET). Clin. Infect. Dis. 2010, 50, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, N.; Reyes, J.; Kusne, S.; Martin, M.; Fung, J. Cryptococcal meningitis after liver transplantation. Transplantation 1996, 61, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Husain, S.; Wagener, M.M.; Singh, N. Cryptococcus neoformansInfection in Organ Transplant Recipients: Variables Influencing Clinical Characteristics and Outcome. Emerg. Infect. Dis. 2001, 7, 375–381. [Google Scholar] [CrossRef] [PubMed]
- John, G.T.; Mathew, M.; Snehalatha, E.; Anandi, V.; Date, A.; Jacob, C.K.; Shastry, J.C.M. Cryptococcosis in renal allograft recipients. Transplantation 1994, 58, 855–856. [Google Scholar] [CrossRef] [PubMed]
- Kullberg, B.J.; Arendrup, M.C. Invasive Candidiasis. Campion EW, éditeur. N. Engl. J. Med. 2015, 373, 1445–1456. [Google Scholar] [CrossRef] [Green Version]
- Lortholary, O.; Renaudat, C.; Sitbon, K.; Desnos-Ollivier, M.; Bretagne, S.; Dromer, F. The French Mycoses Study Group. The risk and clinical outcome of candidemia depending on underlying malignancy. Intensive Care Med. 2017, 43, 652–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osawa, R.; Alexander, B.D.; Lortholary, O.; Dromer, F.; Forrest, G.N.; Lyon, G.M.; Somani, J.; Gupta, K.L.; Del Busto, R.; Pruett, T.L.; et al. Identifying Predictors of Central Nervous System Disease in Solid Organ Transplant RecipientsWith Cryptococcosis. Transplantation 2010, 89, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.; Alexander, B.D.; Lortholary, O.; Dromer, F.; Gupta, K.L.; John, G.T.; del Busto, R.; Klintmalm, G.B.; Somani, J.; Lyon, G.M.; et al. Cryptococcus neoformans in Organ Transplant Recipients: Impact of Calcineurin—Inhibitor Agents on Mortality. J. Infect. Dis. 2007, 195, 756–764. [Google Scholar] [CrossRef] [Green Version]
- Marr, K.A.; Sun, Y.; Spec, A.; Lu, N.; Panackal, A.; Bennett, J.; Pappas, P.; Ostrander, D.; Datta, K.; Zhang, S.X.; et al. A Multicenter, Longitudinal Cohort Study of Cryptococcosis in Human Immunodeficiency Virus–negative People in the United States. Clin. Infect. Dis. 2019, 70, 252–261. [Google Scholar] [CrossRef]
- Singh, N.; Dromer, F.; Perfect, J.R.; Lortholary, O. Immunocompromised Hosts: Cryptococcosis in Solid Organ Transplant Recipients: Current State of the Science. Clin. Infect. Dis. 2008, 47, 1321–1327. [Google Scholar] [CrossRef]
- Nelles, R.; Britton, S.; John, G.T.; Denaro, C. Parkinsonism and prolonged cognitive decline as a manifestation of cryptococcal meningitis in a renal transplant patient. BMJ Case Rep. 2022, 15, e245788. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-T.; Lee, W.-S.; Tsai, C.-A.; Fan, W.-C.; Wu, P.-F.; Wang, F.-D. Incidence of and risk factors for cryptococcosis in kidney transplant recipients in Taiwan—A nationwide population-based study. Int. J. Infect. Dis. 2019, 88, 154–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brizendine, K.D.; Baddley, J.W.; Pappas, P.G. Predictors of Mortality and Differences in Clinical Features among Patients with Cryptococcosis According to Immune Status. PLoS ONE 2013, 8, e60431. [Google Scholar] [CrossRef]
- Beardsley, J.; Sorrell, T.C.; Chen, S.C.-A. Central Nervous System Cryptococcal Infections in Non-HIV Infected Patients. J. Fungi 2019, 5, 71. [Google Scholar] [CrossRef] [Green Version]
- Momi, J.; Tang, C.; Abcar, A.C.; Kujubu, D.A.; Sim, J.J. Hyponatremia in a patient with cryptococcal meningitis: Syndrome of inappropriate antidiuretic hormone (SIADH) or cerebral salt wasting (CSW)? J. Hosp. Med. 2010, 5, 193–195. [Google Scholar] [CrossRef]
- Sahay, M.; Sahay, R. Hyponatremia: A practical approach. Indian J. Endocrinol. Metab. 2014, 18, 760–771. [Google Scholar] [CrossRef]
- Qu, J.; Zhou, T.; Zhong, C.; Deng, R.; Lü, X. Comparison of clinical features and prognostic factors in HIV-negative adults with cryptococcal meningitis and tuberculous meningitis: A retrospective study. BMC Infect. Dis. 2017, 17, 51. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.; Lortholary, O.; Dromer, F.; Alexander, B.D.; Gupta, K.L.; John, G.T.; Del Busto, R.; Klintmalm, G.B.; Somani, J.; Lyon, G.M.; et al. Central Nervous System Cryptococcosis in Solid Organ Transplant Recipients: Clinical Relevance of Abnormal Neuroimaging Findings. Transplantation 2008, 86, 647–651. [Google Scholar] [CrossRef]
- Hamadani, B.H.K.; Franco-Paredes, C.; McCollister, B.; Shapiro, L.; Beckham, J.D.; Henao-Martínez, A.F. Cryptococcosis and cryptococcal meningitis: New predictors and clinical outcomes at a United States academic medical centre. Mycoses 2017, 61, 314–320. [Google Scholar] [CrossRef]
- Huang, S.-H.; Chuang, Y.-C.; Lee, Y.-C.; Hung, C.-C.; Sheng, W.-H.; Su, J.-J.; Sun, H.-Y.; Chen, Y.-C.; Chang, S.-C. Lumbar puncture for non-HIV-infected non-transplant patients with cryptococcosis: Should it be mandatory for all? PLoS ONE 2019, 14, e0221657. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.-L.; Chen, M.; Gu, J.-L.; Zhu, F.-Y.; Xu, X.-G.; Zhang, C.; Chen, J.-H.; Pan, W.-H.; Liao, W.-Q. Cryptococcosis in kidney transplant recipients in a Chinese university hospital and a review of published cases. Int. J. Infect. Dis. 2014, 26, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Zhong, Y.; Zhou, Z.; Fang, X.; Peng, F.; Zhang, W. Magnetic resonance imaging study of cryptococcal neuroradiological lesions in HIV-negative cryptococcal meningitis. Eur. J. Clin. Microbiol. 2017, 36, 1367–1372. [Google Scholar] [CrossRef]
- Lan, S.-H.; Chang, W.; Lu, C.; Lui, C.; Chang, H. Cerebral infarction in chronic meningitis: A comparison of tuberculous meningitis and cryptococcal meningitis. QJM Int. J. Med. 2001, 94, 247–253. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) | |||
|---|---|---|---|
| Characteristics | Non-CM n = 27 | CM n = 61 | p Value |
| Clinical characteristics | |||
| Male, No. (%) | 21 (77.8) | 40 (65.6) | 0.371 |
| Age at diagnosis (years), mean (SD) | 58.07 (12.8) | 57.23 (13.6) | 0.786 |
| BMI (kg/m2), mean (SD) | 22.9 (3.28) | 23.7 (5.94) | 0.472 |
| Pre-transplant diabetes, No. (%) | 3 (11.1) | 12 (19.7) | 0.378 |
| Post-transplant diabetes, No. (%) | 12 (44.4) | 28 (45.9) | 1.000 |
| HIV status, No. (%) | 1 (3.7) | 3 (4.9) | 1.000 |
| Baseline eGFR before cryptococcosis (CKD-EPI in ml/min/1.73 m2), mean (SD) | 46.5 (20.4) | 48.0 (27.8) | 0.779 |
| RRT duration (months), median [IQR] | 48 [19–108] | 32 [12–50] | 0.195 |
| Prior transplant, No. (%) | 5 (20) | 12 (19.7) | 0.972 |
| Deceased donor type (vs. living), No. (%) | 24 (88.9) | 57 (93.4) | 0.671 |
| Length of post-transplant hospitalization (days), mean (SD) | 20.4 (13.2) | 19.0 (10.6) | 0.706 |
| Positive Anti-HLA donor specific antibody at time of transplant, No. (%) | 6 (26.1) | 12 (24.5) | 1.000 |
| Immunosuppressive induction | |||
| None, No. (%) | 2 (9.5) | 1 (2.0) | 0.222 |
| ATG, No. (%) | 14 (66.7) | 36 (70.6) | 0.642 |
| IL2R, No. (%) | 5 (23.8) | 14 (27.5) | 0.782 |
| Other infections prior cryptococcosis | |||
| Infections, No. (%) | |||
| Fungal infections | 3 (11.1) | 2 (3.28) | 0.170 |
| CMV disease | 1 (4) | 9 (15.2) | 0.268 |
| PCR BK positive during follow-up | 2 (12.5) | 3 (8.1) | 0.632 |
| (b) | |||
| Characteristics | Non-CM n = 27 | CM n = 61 | p value |
| Time between transplantation and diagnosis (months), median [IQR] | 42.9 [14.9; 121] | 34.6 [11.6; 72.4] | 0.581 |
| Time between first symptoms and diagnosis (days), median [IQR] | 21 [5–34] | 24 [9–58] | 0.112 |
| Admission delay—diagnosis (days), median [IQR] | 5 [2–11] | 8 [2–18] | 0.466 |
| Number of hospitalizations/consultations with functional complaint before hospitalization, median [IQR] | 1 [0–2] | 1 [0–2] | 0.338 |
| Total length of hospitalization (days), median [IQR] | 16 [8–47] | 30 [21–43] | 0.042 |
| ICU admission, No. (%) | 6 (25) | 25 (42.4) | 0.210 |
| Need for mechanical ventilation, No. (%) | 0 | 17 (27.9) | 0.001 |
| ICU duration (days), median [IQR] | 4.5 [1–8] | 4 [1–13] | 0.816 |
| Clinical presentation at diagnosis, No. (%) | |||
| Asthenia | 9 (34.6) | 27 (45.0) | 0.477 |
| Emesis | 0 | 21 (35.0) | <0.001 |
| Digestive disorder | 4 (15.4) | 8 (13.3) | 0.749 |
| Skin lesion | 5 (19.2) | 4 (6.7) | 0.122 |
| Cough/dyspnea | 9 (34.6) | 9 (15) | 0.049 |
| Fever at diagnostic | 13 (50) | 37 (61.7) | 0.348 |
| Natremia at diagnosis (mmol/L), median [IQR] | 138 [135–139] | 132 [130–134] | <0.001 |
| Hyponatremia at diagnosis (<135 mmol/L), No. (%) | 3 (15.8) | 39 (78.0) | 0.005 |
| Total lymphocytes at diagnosis (mm3), median [IQR] | 960 [340–2000] | 755 [500–1200] | 0.600 |
| CD4 count at diagnosis (mm3), median [IQR] | 79 [51–118] | 89 [46–202] | 0.754 |
| Intracranial pressure at diagnosis(cmH20), median [IQR] | 17.5 [12–23] | 29 [15.5–31] | 0.258 |
| Co-infection associated with diagnosis (viral, bacterial or fungal), No. (%) | 10 (43.5) | 20 (34.5) | 0.457 |
| eGFR (CKD-EPI in ml/min/1.73 m2) at diagnosis (n = 74), mean (SD) | 38.6 (17.1) | 39.9 (21.0) | 0.806 |
| (c) | |||
| Characteristics | Non-CM n = 27 | CM n = 61 | p value |
| Cryptococcus species *, No. (%) | 1.00 | ||
| Cryptoccocus deneoformans (ex C. neoformans) | 22 (88) | 49 (84.5) | |
| Cryptococcus neoformans (ex C. grubii) | 3 (12.0) | 9 (15.5) | |
| Positive serum Ag at diagnosis (n = 73) | 11 (20.0) | 44 (80.0) | <0.001 |
| Serum Ag titer at diagnosis median [IQR] (n = 29) | 1/160 [1/4–1/2018] | 1/114 [1/20–1/512] | 0.935 |
| Positive serum cultures at diagnosis | 6 (24.0) | 29 (47.5) | 0.055 |
| Positive CSF Ag at diagnosis No. (%) | - | 33 (100) | |
| Positive India ink test CSF, No. (%) | - | 21 (40.4) | |
| CSF Ag titer at diagnosis, median [IQR] | - | 1/64 [1/8–1/450] | |
| Positive culture in CSF, No. (%) | - | 16 (29.1) | |
| CSF WBC count (/mm3), median [IQR] | 2.5 [2–3.5] | 55 [5–175] | 0.001 |
| Characteristics | N | OR [95% CI] | p Value |
|---|---|---|---|
| Clinical characteristics | |||
| Age at time of diagnosis (per 1 year increment) | 88 | 0.99 [0.96;1.03] | 0.783 |
| HIV status | 88 | ||
| Negative | Ref. | ||
| Positive | 1.34 [0.13;13.5] | 0.797 | |
| Number of cardiovascular risk factors, (per 1 risk factor increment) | 84 | 1.48 [0.93;2.36] | 0.088 |
| Graft rejection before cryptococcosis | 87 | ||
| No | Ref. | ||
| Yes | 0.44 [0.17;1.17] | 0.102 | |
| Tacrolimus at time of diagnosis | 83 | ||
| No | Ref | ||
| Yes | 1.77 [0.64;4.87] | 0.275 | |
| eGFR (CKD-EPI) at time of diagnosis (per 1 mL/min/1.73 m2 increment) | 85 | 1.01 [0.99;1.03] | 0.504 |
| Time between transplant and diagnosis (per 1 year increment) | 79 | 1.54 [0.33;7.22] | 0.533 |
| Clinical presentation | |||
| ICU hospitalization: | 83 | ||
| No | Ref. | ||
| Yes | 2.21 [0.77;6.36] | 0.131 | |
| Natremia at time of diagnosis (per 1 mmol/l increment) | 69 | 0.71 [0.59;0.85] | <0.001 |
| At least one neurological symptom at time of diagnosis | 86 | ||
| No | Ref. | ||
| Yes | 90.85 [17.56;470.16] | <0.0001 | |
| Fever at time of diagnosis | 84 | ||
| No | Ref | ||
| Yes | 1.69 [0.66;4.35] | 0.272 | |
| Skin lesion | 86 | ||
| No | Ref. | ||
| Yes | 0.31 [0.07;1.23] | 0.094 | |
| Cough/Dyspnea | 86 | ||
| No | Ref. | ||
| Yes | 0.33 [0.11;0.98] | 0.046 | |
| Fungemia | 86 | ||
| No | Ref. | ||
| Yes | 2.87 [1.01;8.17] | 0.041 |
| N | OR [95% CI] | p Value | |
|---|---|---|---|
| Natremia at time of diagnosis (per 1 mmol/L increment) | 69 | 0.76 [0.63;0.93] | 0.008 |
| At least one neurological symptom at time of diagnosis | 69 | ||
| No | Ref. | ||
| Yes | 60.71 [9.12;404.20] | <0.001 |
| Characteristics | Non-CM n = 27 (%) | CM n = 61 (%) | p Value |
|---|---|---|---|
| IRIS, No (%) | 1 (3.70) | 5 (8.20) | 0.662 |
| eGFR M12 after cryptococcosis (CKD-EPI), mean (SD) | 48.8 (32.4) | 35.9 (15.4) | 0.209 |
| eGFR at last follow-up (CKD-EPI), mean (SD) | 40.1 (18.7) | 35.7 (20.7) | 0.430 |
| Graft failure at last follow-up, No (%) | 9 (34.6) | 19 (38) | 0.808 |
| Patient death at M12, No (%) | 7 (25.9) | 20 (32.8) | 0.594 |
| Patient death at last follow-up, No (%) | 10 (37.0) | 26 (42.6) | 0.798 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tardieu, L.; Divard, G.; Lortholary, O.; Scemla, A.; Rondeau, É.; Accoceberry, I.; Agbonon, R.; Alanio, A.; Angoulvant, A.; Albano, L.; et al. Cryptococcal Meningitis in Kidney Transplant Recipients: A Two-Decade Cohort Study in France. Pathogens 2022, 11, 699. https://doi.org/10.3390/pathogens11060699
Tardieu L, Divard G, Lortholary O, Scemla A, Rondeau É, Accoceberry I, Agbonon R, Alanio A, Angoulvant A, Albano L, et al. Cryptococcal Meningitis in Kidney Transplant Recipients: A Two-Decade Cohort Study in France. Pathogens. 2022; 11(6):699. https://doi.org/10.3390/pathogens11060699
Chicago/Turabian StyleTardieu, Laurène, Gillian Divard, Olivier Lortholary, Anne Scemla, Éric Rondeau, Isabelle Accoceberry, Rémi Agbonon, Alexandre Alanio, Adela Angoulvant, Laetitia Albano, and et al. 2022. "Cryptococcal Meningitis in Kidney Transplant Recipients: A Two-Decade Cohort Study in France" Pathogens 11, no. 6: 699. https://doi.org/10.3390/pathogens11060699
APA StyleTardieu, L., Divard, G., Lortholary, O., Scemla, A., Rondeau, É., Accoceberry, I., Agbonon, R., Alanio, A., Angoulvant, A., Albano, L., Attias, P., Bellanger, A. P., Bertrand, D., Bonhomme, J., Botterel, F., Bouvier, N., Buchler, M., Chouaki, T., Crépin, T., ... Rafat, C. (2022). Cryptococcal Meningitis in Kidney Transplant Recipients: A Two-Decade Cohort Study in France. Pathogens, 11(6), 699. https://doi.org/10.3390/pathogens11060699