
Critical Systematic Review of Zoonoses and Transboundary Animal Diseases’ Prioritization in Africa

 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Overview of Zoonosis and Transboundary Animal Disease Prioritization in Africa
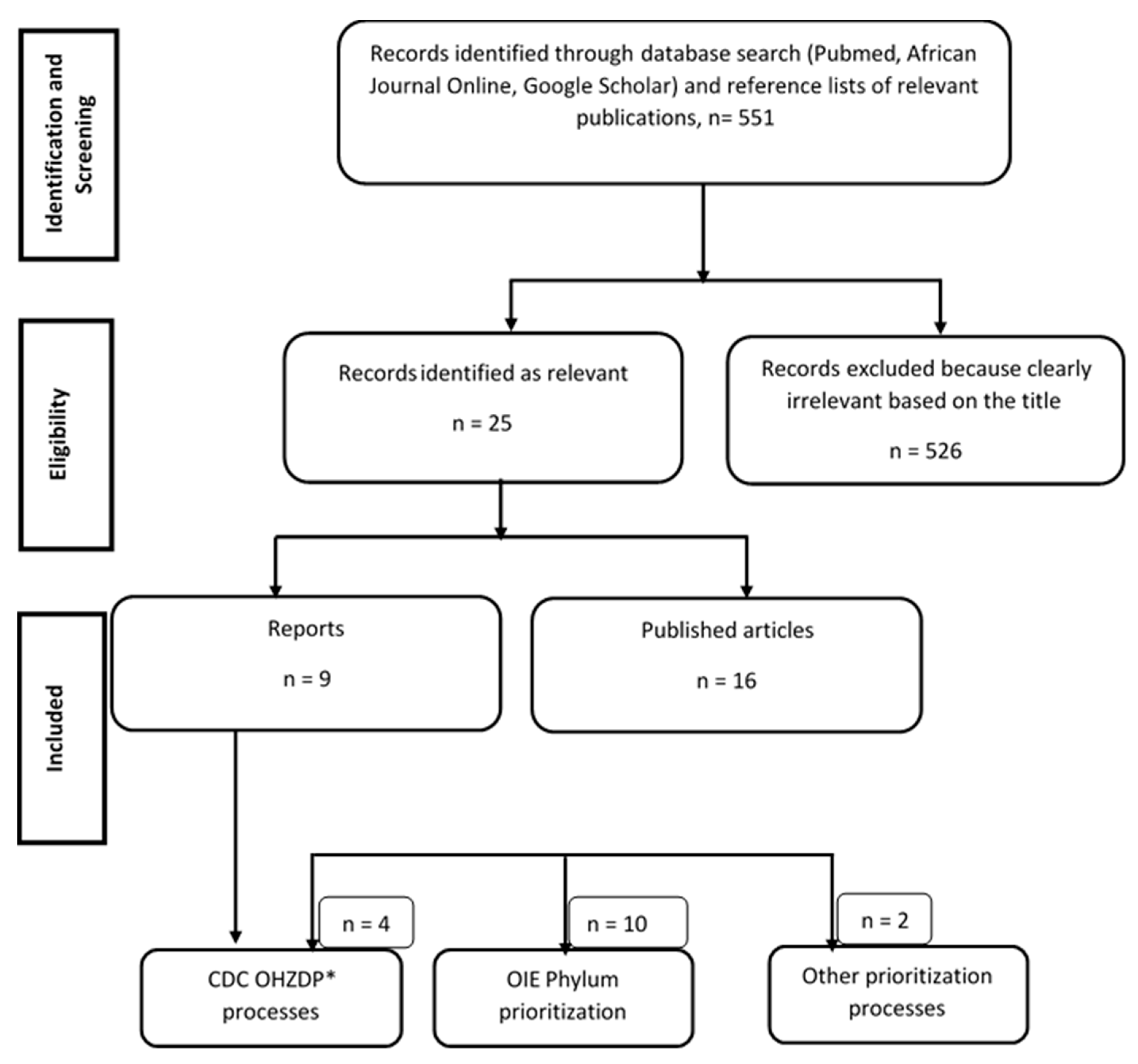
- Four countries (Ethiopia, Kenya, Tanzania, and Uganda) implemented both animal and zoonotic disease prioritization processes at the national level using the Phylum and the OHZDP tool;
- Six countries (Burkina Faso, Cameroon, Cote d’Ivoire, Democratic Republic of Congo, Mali, Mozambique) were concerned only by zoonotic disease prioritization at the national level using the OHZDP tool;
- Six countries (Burundi, Djibouti, Eritrea, Rwanda, South-Sudan, Sudan) used the Phylum tool to prioritize TADs and zoonoses at the national level.
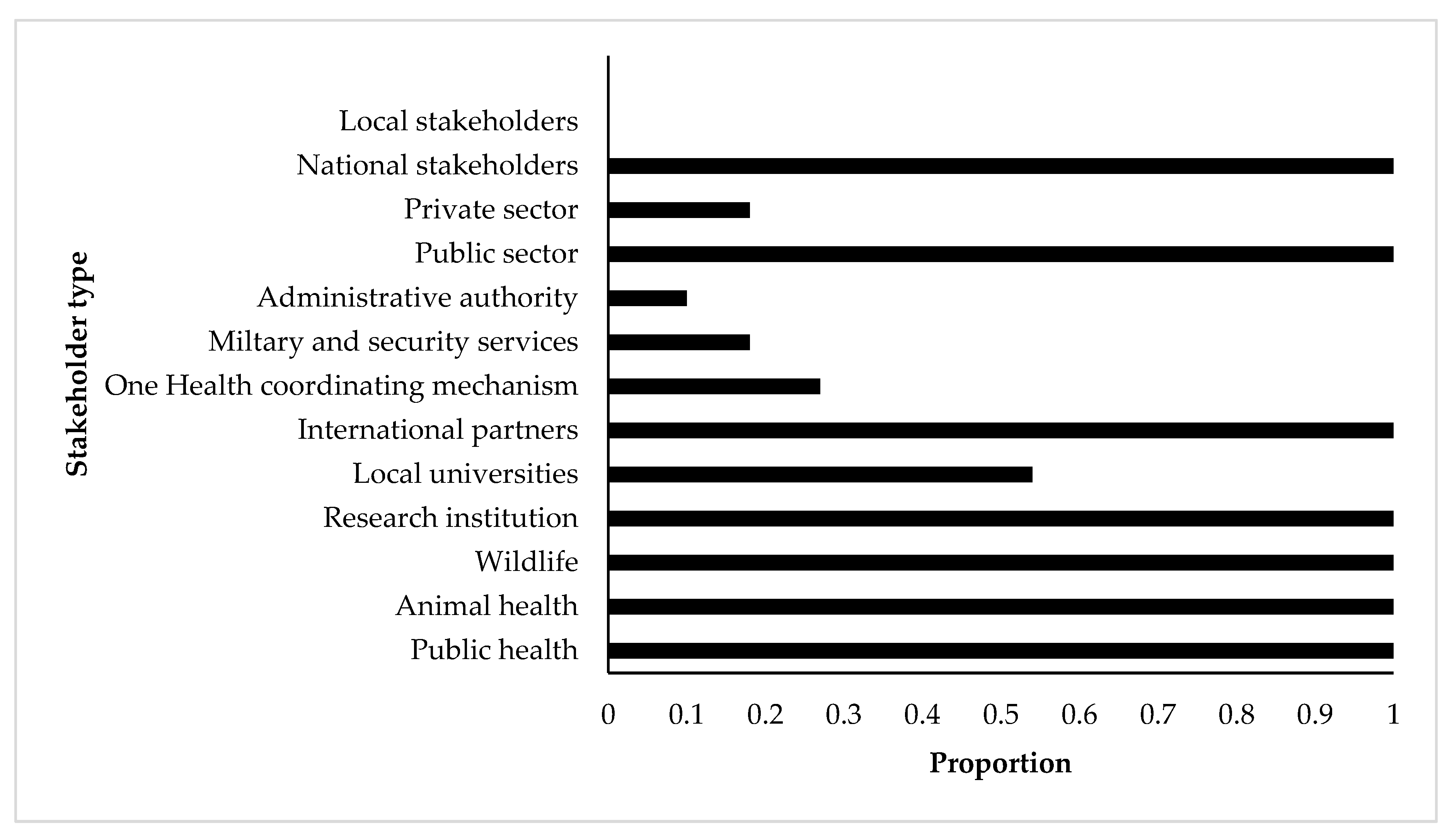
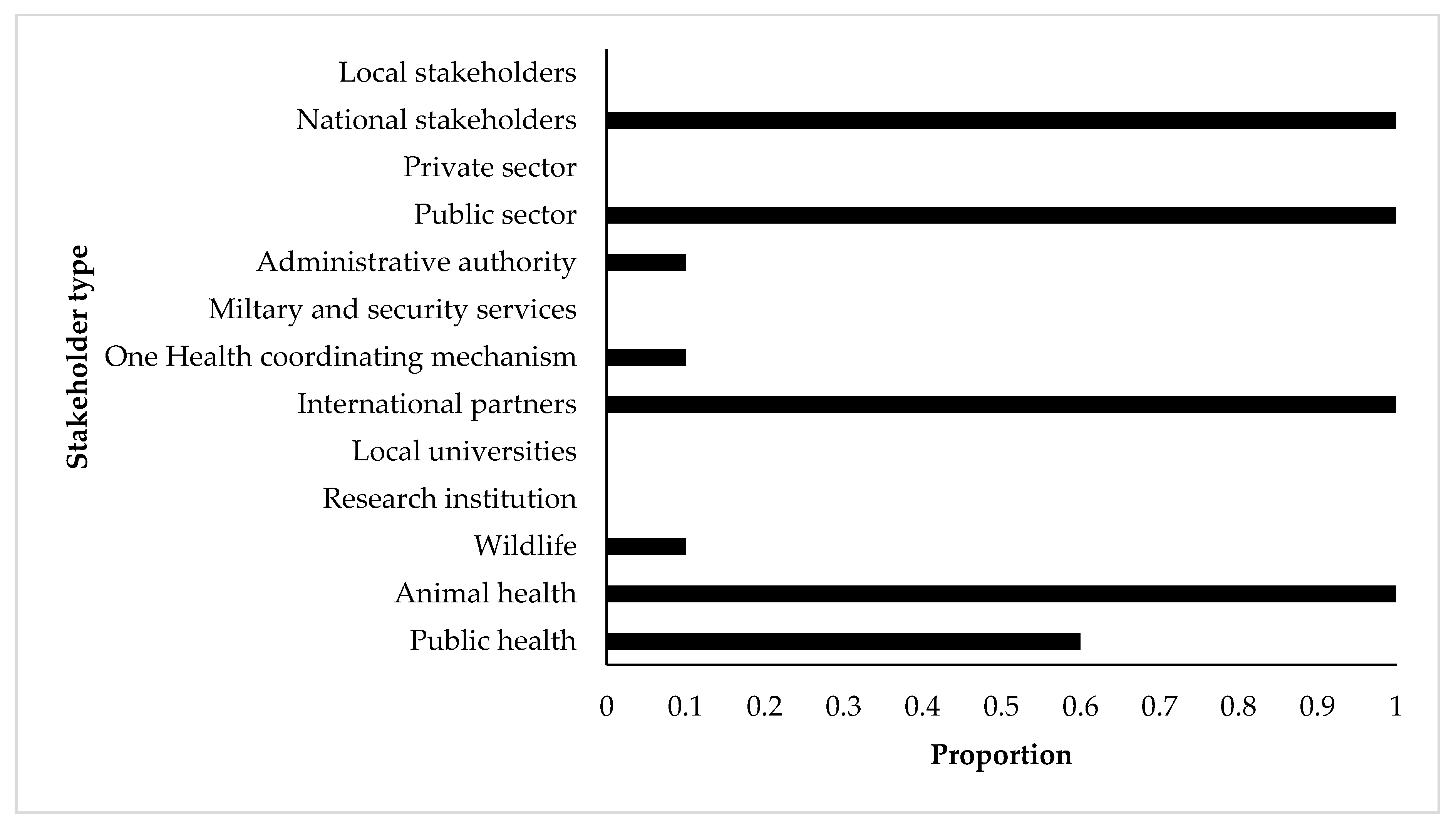
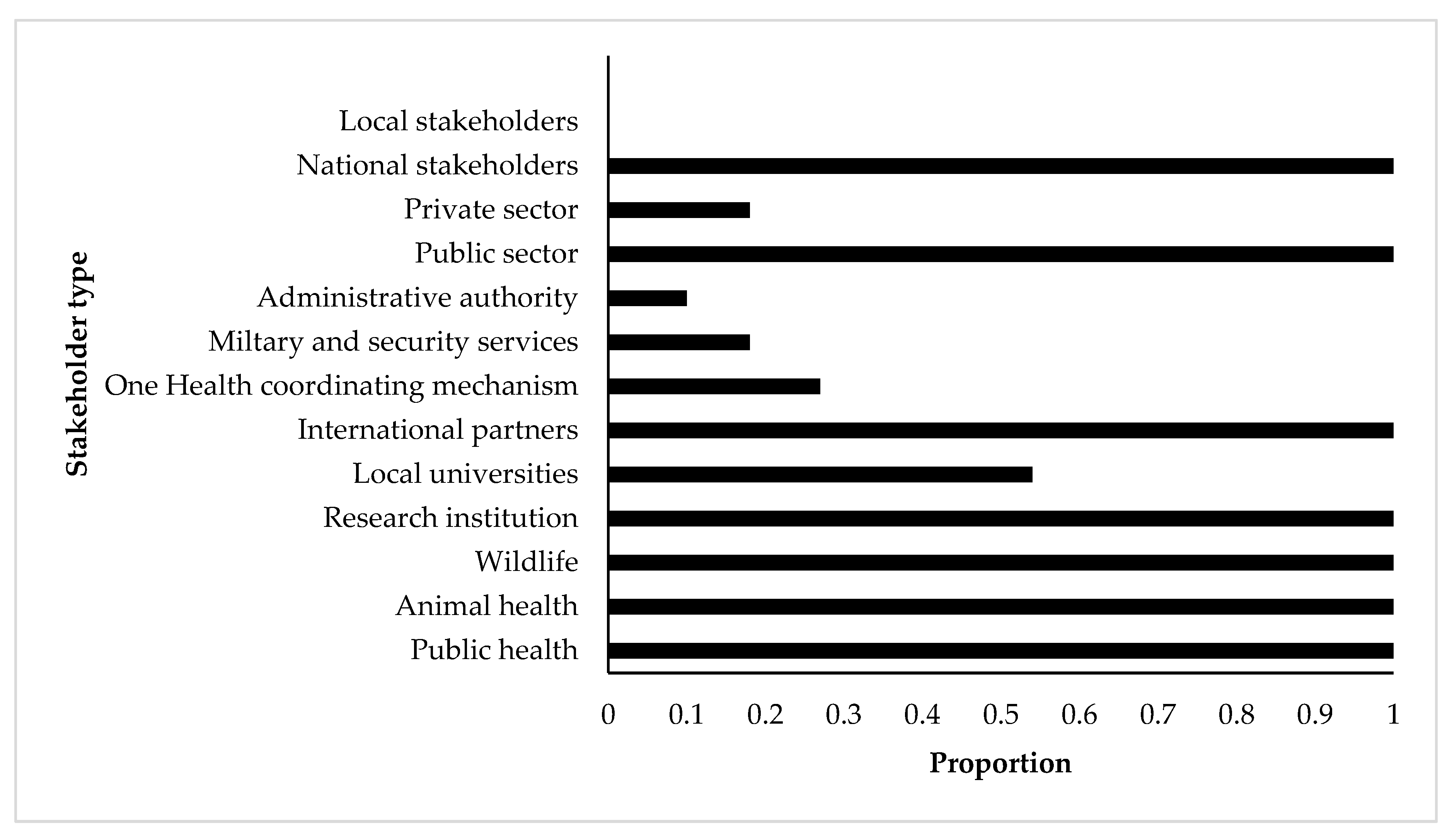
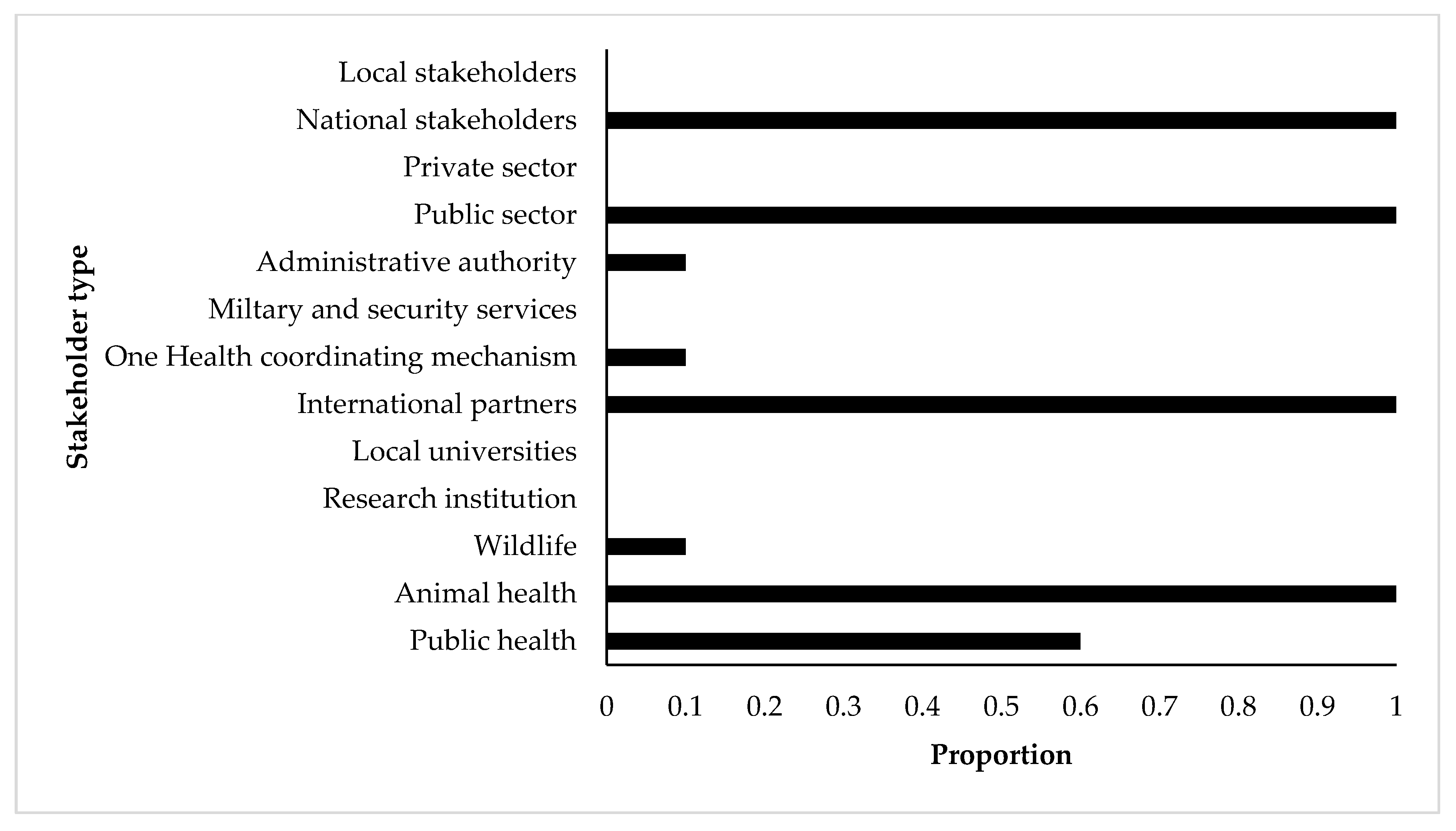
2.2. Prioritization Processes by Stakeholders
2.3. Zoonoses and Transboundary Animal Diseases Prioritization Criteria Chosen by Countries
- Severity of disease in humans (all countries),
- Availability of interventions (i.e., vaccines and/or medical treatment) (all countries),
- Economic, environmental, and/or social impact (9/10 countries),
- Presence of disease in country and/or region (8/10 countries),
- Epidemic/pandemic potential (and/or sustained transmission in humans) (7/10 countries).
2.4. Zoonoses and Transboundary Animal Diseases Ranking
3. Discussion
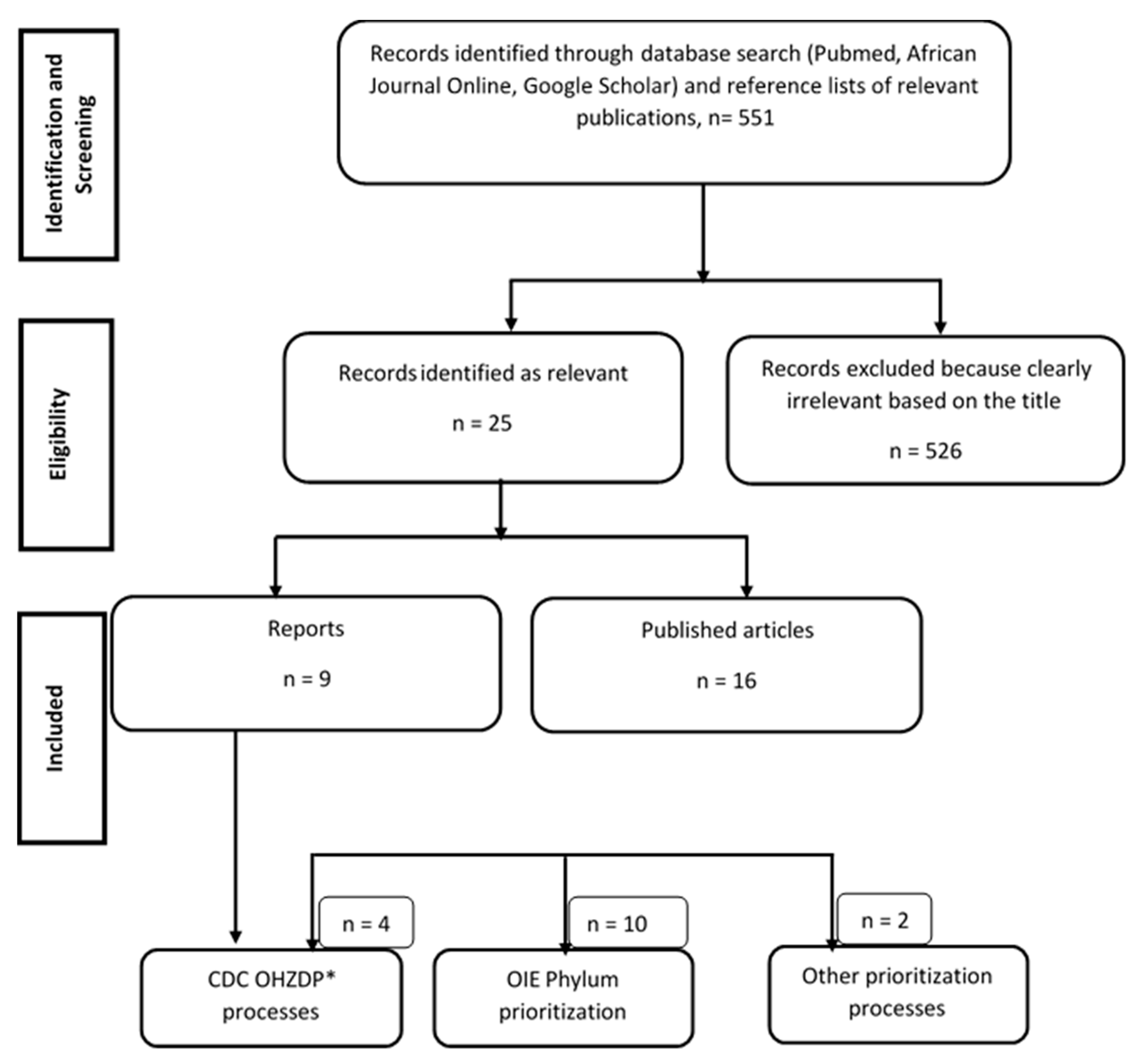
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carter, A.; National Advisory Committee on Epidemiology Subcommittee. Establishing goals, techniques and priorities for national communicable disease surveillance. Can. J. Infect. Dis. 1991, 2, 37–40. [Google Scholar] [CrossRef] [Green Version]
- Brookes, V.J.; Del Rio Vilas, V.J.; Ward, M.P. Disease prioritization: What is the state of the art? Epidemiol. Infect. 2015, 143, 2911–2922. [Google Scholar] [CrossRef] [PubMed]
- Phylum. Listing and Categorization of Priority Animal Diseases, Including Those Transmissible to Humans. Methodological Manual; Phylum: Toulouse, France, 2010. [Google Scholar]
- WHO (World Health Organization). The Dubrovnik Pledge on Surveillance and Prioritization of Infectious Diseases: Report on a WHO Meeting, Bucharest, Romania 21–23 November 2002; WHO Regional Office for Europe: Copenhagen, Denmark, 2003; Available online: http://www.euro.who.int/data/assets/pdffile/0005/128039/E78888.pdf. (accessed on 20 February 2021).
- Wentholt, M.T.A.; Cardoen, S.; Imberechts, H.; Van Huffel, X.; Ooms, B.W.; Frewer, L.J. Defining European preparedness and research needs regarding emerging infectious animal diseases: Results from a Delphi expert consultation. Prev. Vet. Med. 2012, 103, 81–92. [Google Scholar] [CrossRef] [PubMed]
- FAO (Food and Agriculture Organization of the United Nations); OIE (World Organization for Animal Health). The Global Framework for the Progressive Control of Transboundary Animal Diseases (GF-TADs); FAO-OIE: Paris, France, 2004; Available online: http://www.fao.org/3/ak136e/ak136e.pdf (accessed on 20 February 2021).
- Gary, F. Critères et Facteurs d’une Priorisation Rationnelle des Maladies Animales Devant Faire l’objet de Politiques Sanitaires Publiques. In Proceedings of the OIE 82è Session Générale, Assemblée Mondiale, Paris, France, 25–30 May 2014; Available online: http://www.oie.int/fr/publications-et-documentation/recueil-de-themes-techniques/ (accessed on 15 December 2020).
- WHO (World Health Organization). Setting Priorities in Communicable Disease Surveillance; World Health Organization: Lyon, France, 2006. [Google Scholar]
- Mehand, M.S.; Millett, P.; Al-Shorbaji, F.; Roth, C.; Kieny, M.P.; Murgue, B. World Health Organization methodology to prioritize emerging infectious diseases in need of research and development. Emerg. Infect. Dis. 2018, 24, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Rist, C.L.; Arriola, C.S.; Rubin, C. Prioritizing zoonoses: A proposed one health tool for collaborative decision-making. PLoS ONE 2014, 9, e109986. [Google Scholar] [CrossRef] [PubMed]
- Salyer, S.J.; Dilver, S.R.; Simone, K.; Behravesh, B.C. Prioritizing zoonoses for global health capacity building-themes from one health zoonotic disease workshops in 7 countries, 2014–2016. Emerg. Infect. Dis. 2017, 23, 57–63. [Google Scholar] [CrossRef] [Green Version]
- EPHI (Ethiopian Public Health Institute); MoLFR (Ministry of Livestock and Fishery Resources, Ethiopia, Formerly Part of the Ministry of Agriculture); MEF (Ministry of Environment and Forestry, Ethiopia); WHO (World Health Organization); USDA (United States Department of Agriculture); CDC (U.S. Centers for Disease Control and Prevention); DTRA/CBEP (Defense Threat Reduction Agency/Cooperative, Biological Engagement Program); OSU (The Ohio State University); FAO (United Nations Food and Agriculture Organization); AHRI (Armauer Hansen Research Institute); et al. Zoonotic Disease Prioritization for Inter-Sectoral Sectoral Engagement in Ethiopia. Workshop Summary. Adis Abeba, Ethiopia 2015. Available online: https://www.cdc.gov/onehealth/pdfs/hammett-ethiopi-workshop-508.pdf (accessed on 10 September 2020).
- PNPLZER (National Program for the Prevention and Control against Emerging and Re-emerging Zoonozes); MINEPIA (Ministry of Livestock, Fisheries, and Animal Industries); MINFOF (Ministry of Forests and Fauna); MINSANTE (Ministry of Public Health); MINEPDED (Ministry of Environment; Nature Protection and Sustainable Development); MINRESI (Ministry of Scientific Research and Innovation), CREMER (Research Center for Emerging and Re-emerging diseases); LANAVET (National Veterinary Laboratory); CRESAR (Military Health Research Center); USAID Prepare & Respond Project; et al. Zoonotic Disease Prioritization for Inter-Sectoral Sectoral Engagement in Cameroon. Workshop Summary. Yaounde, Cameroon 2016. Available online: https://www.cdc.gov/onehealth/pdfs/Cameroon-english-508.pdf (accessed on 10 September 2020).
- Munyua, P.; Bitek, A.; Osoro, E.; Pieracci, E.G.; Muema, J.; Mwatondo, A.; Kungu, M.; Nanyingi, M.; Gharpure, R.; Njenga, K.; et al. Prioritization of zoonotic diseases in Kenya, 2015. PLoS ONE 2016, 11, e0161576. [Google Scholar] [CrossRef]
- Pieracci, E.G.; Hall, A.J.; Gharpure, R.; Haile, A.; Walelign, E.; Deressa, A.; Bahiru, G.; Kibebe, M.; Walke, H.; Belay, E. Prioritizing zoonotic diseases in Ethiopia using a one health approach. One Health 2016, 2, 131–135. [Google Scholar] [CrossRef] [Green Version]
- MSHP (Ministry of Health and Public Hygiene); MESRS (Ministry of Higher Education and Scientific Research); MINADER (Ministry for Agriculture and Rural Development); MINEF (Ministry of Water and Forests); MIRAH (Ministry of Animal and Fisheries Resources); MINSEDD (Ministry of Wholesomeness, Environment and Sustainable Development). One Health Zoonotic Diseases Prioritization for Multisectoral Engagement in Côte D’Ivoire. Workshop Summary. Abidjan, Côte D’Ivoire 2017. Available online: https://www.cdc.gov/onehealth/pdfs/cote-dlvoire-english-508.pdf (accessed on 12 September 2020).
- MOH (Ministry of Health); MAAIF (Ministry of Agriculture, Animal Industry, and Fisheries); CPHL (Central Public Health Laboratory); MWE (Ministry of Water and Environment); UWA (Uganda Wildlife Authority); NADDEC (National Animal Disease Diagnostics and Epidemiology Centre); PHEOC (Public Health Emergency Operation Centre); OHTWG-ZDCO (Uganda National One Health Platform including One Health Technical Working Group-Zoonotic Diseases Coordination Office); COCTU (Coordinating Office for the Control of Trypanosomiasis in Uganda); IDI (Infectious Disease Institute); et al. One Health Zoonotic Diseases Prioritization for Multisectoral Engagement in Uganda. Workshop Summary. Kampala, Uganda, 2017. Available online: https://www.cdc.gov/onehealth/pdfs/uganda-one-health-zoonotic-disease-prioritization-report-508.pdf (accessed on 12 September 2020).
- OHCU (One Health Coordination Unit-Prime Minister’s Office); MoH (Ministry of Health); Community Development, Gender, Elderly and Children; Ministry of Agriculture, Livestock and Fisheries (now referred to as the Ministry of Livestock and Fisheries and the Ministry of Agriculture); Tanzania Veterinary Laboratory Agency; Ministry of Natural Resources and Tourism; Tanzania Wildlife Research Institute; Tanzania National Parks; NEMC (National Environmental Management Council); Vice President’s Office-Environment; et al. One Health Zoonotic Diseases Prioritization for Multisectoral Engagement in Tanzania. Workshop Summary. Dar es Salaam, Tanzania 2017. Available online: https://www.cdc.gov/onehealth/pdfs/tanzania-report-508.pdf (accessed on 12 September 2020).
- MRAH (Ministère des Ressources Animales et Halieutiques); MEEVCC (Ministère de l’Environnement, de l’Economie Verte et du Changement Climatique); Ministère de la Santé; CDC Atlanta; OIE; USAID/ Burkina Faso; FAO Burkina Faso; CDC Burkina Faso; USAID Washington; IRSS (Institut de Recherche en Sciences de la Santé); et al. One Health Zoonotic Diseases Prioritization for Multisectoral Engagement in Burkina Faso. Workshop Summary. Ouagadougou, Burkina Faso 2017. Available online: https://www.cdc.gov/onehealth/pdfs/burkinafaso-english-508.pdf (accessed on 14 September 2020).
- ASCOMA (Consumer Association of Mali); CDC (U.S. Centers for Disease Control and Prevention); CNAM (National Center for Support of Disease Control, Ministry of Health and Public Hygiene); CNASA (National Center for Support of Animal Health, Ministry of Livestock and Fisheries); CT/MESRS (Technical Adviser in the Ministry of Higher Education Scientific Research); DCSSA (Central Directorate of Army Health Services); DGPC (General Directorate of Civil Protection, Ministry of Security and Civil Protection); DNA (National Directorate of Agriculture, Ministry of Agriculture); DNACPN (National Directorate of Sanitation and the Fight against Pollution and Nuisances); DNEF (National Directorate of Water and Forest, Ministry of Environment, Sanitation and Sustainable Development); et al. One Health Zoonotic Diseases Prioritization for Multisectoral Engagement in Mali. Workshop Summary. Bamako, Mali 2017. Available online: https://www.cdc.gov/onehealth/pdfs/mali-508.pdf (accessed on 14 September 2020).
- MASA (Ministry of Agriculture and Food Security, DINAV); Ministry of Health (MISAU, INS); Ministry of Land, Environment, and Rural Development (MITADER, ANAC); MIMAIP (Ministry of Sea, Inland Waters, Fisheries); INIP (National Fish Inspection Institute); FAVET (Faculty of Veterinary Medicine); UEM (Eduardo Mondlane University); Directorate of Animal Sciences; NMNH (National Museum of Natural History); Order of Physicians of Mozambique; et al. One Health Zoonotic Diseases Prioritization for Multisectoral Engagement in Mozambique. Workshop Summary. Maputo, Mozambique 2018. Available online: https://www.cdc.gov/onehealth/pdfs/Mozambique-508.pdf (accessed on 15 September 2020).
- Muhemedi, S.; Masumu, J.; Lubula, L.; Kabambi, P.; Okitolonda, E. Prioritization of zoonotic diseases in the Democratic Republic of the Congo, 2016. J. Zoonotic Dis. Public Health 2018, 2, 1–6. [Google Scholar]
- Sekamatte, M.; Krishnasamy, V.; Bulage, L.; Kihembo, C.; Nantima, N.; Monje, F.; Ndumu, D.; Sentumbwe, J.; Mbolanyi, B.; Aruho, R.; et al. Multisectoral prioritization of zoonotic diseases in Uganda, 2017: A One Health perspective. PLoS ONE 2018, 13, e0196799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adwok, D.S.; Yuot, M.M.A.; Jakwot, M.J.; Kwai, A.M.; Korok, J.M.; Magona, J.; Olaho-Mukani, W.; Muruiki, S.; Abdulaziz, M.A.R.; Baboucarr, J. Prioritisation of transboundary animal diseases (TADs) and zoonoses for the development of an effective disease control strategy in South Sudan. Bull. Anim. Health Prod. Afr. 2018, 66, 363–373. [Google Scholar]
- Assenga, S.P.; Sero, H.L.; Tinuga, D.K.; Abdu, A.H.; Mtiba, P.P.; Olaho-Mukani, W.; Muruiki, S.; Abdulaziz, M.A.R.; Wesonga, T.W.; Baboucarr, J. Transboundary animal diseases and zoonoses: Prioritization and interventions in Tanzania. Bull. Anim. Health Prod. Afr. 2018, 66, 415–426. [Google Scholar]
- Cheikh, M.; Hoch, M.G.; Guirreh, D.A.; Miguil, S.W.; Barkhad, M.M.; Djama, A.G.; Issa, A.A.; Elmi, M.; Magona, J.; Olaho-Mukani, W.; et al. Priority transboundary animal diseases and zoonoses and their proposed control strategies for Djibouti. Bull. Anim. Health Prod. Afr. 2018, 66, 231–237. [Google Scholar]
- Hanan Yousif, M.A.; Faiza Awad, A.; Abdel Rahman, A.; Beigi Khidir, M.A.; Amel Mahgoub, A.; Wahba, M.; Kamal Tag, E.; Magona, J.; Olaho Mukani, W.; Muruiki, S.; et al. Prioritisation of transboundary animal diseases (TADs) and zoonoses for effective control in Sudan. Bull. Anim. Health Prod. Afr. 2018, 66, 395–405. [Google Scholar]
- Nantima, N.; Bwire, G.; Mwebe, R.; Mugabi, K.; Ademun, A.R.O.; Kaboyo, W.; Acheng, J.R.; Magoona, J.; Kauta, N.; Olaho-Mukani, W.; et al. Prioritisation of transboundary animal diseases and zoonoses to strengthen control in Uganda. Bull. Anim. Health Prod. Afr. 2018, 66, 351–361. [Google Scholar]
- Niyokwishimira, A.; Nshimirimana, Y.; Havyarimana, J.P.; Moza, S.; Nsanganiyumwami, D.; Olaho-Mukani, W.; Muruiki, S.; Abdulaziz, M.A.R.; Wesonga, T.W.; Baboucarr, J. Prioritisation of transboundary animal diseases and zoonoses for effective control in Burundi. Bull. Anim. Health Prod. Afr. 2018, 66, 239–247. [Google Scholar]
- Njagi, L.; Osoro, E.; Mwololo, D.; Murekefu, W.; Thaiya, J.; Ngeiywa, K.; Murithi, M.; Olaho-Mukani, W.; Muruiki, S.; Abdulaziz, M.A.R.; et al. Prioritisation of transboundary animal diseases and zoonoses to strengthen control measures in Kenya. Bull. Anim. Health Prod. Afr. 2018, 66, 287–297. [Google Scholar]
- Mwenedata, J.C.; Kinani, J.F.; Kabeja, A.; Isidore Mapendo, I.G.; Kanyandekwe, C.; Rutagwenda, T.; Olaho-Mukani, W.; Muruiki, S.; Abdulaziz, M.A.R.; Wesonga, T.W.; et al. Prioritisation and categorisation of transboundary animal diseases and zoonoses for effective surveillance and control in Rwanda. Bull. Anim. Health Prod. Afr. 2018, 66, 387–393. [Google Scholar]
- Uqbazghi, K.; Teklemariam, T.; Goitom, H.; Magona, J.; Olaho-Mukani, W.; Muruiki, S.; Abdulaziz, M.A.R.; Baboucarr, J. Prioritisation and control strategies of transboundry and zoonotic animal diseases in Eritrea. Bull. Anim. Health Prod. Afr. 2018, 66, 249–263. [Google Scholar]
- Walelign, E.; Yilma, G.; Haile, A.; Regassa, F.; Magona, J.; Olaho-Mukani, W.; Muruiki, S.; Abdulaziz, M.A.R.; Baboucarr, J. Transboundary animal diseases and zoonoses prioritization and proposed interventions in Ethiopia. Bull. Anim. Health Prod. Afr. 2018, 66, 265–273. [Google Scholar]
- ECOWAS (Economic Community of West African States); RAHC (Regional Animal Health Centre); FAO (Food and Agriculture Organization); EISMV (Inter-State School for Sciences and Veterinary Medicine); LNERV (National Laboratory for Veterinary Studies and Research); NCDC (Nigeria Centre for Disease Control); USAID (United States Agency for International Development); CDC (United States Centers for Disease Control and Prevention); DTRA (United States Defense Threat Reduction Agency); USDA (United States Department of Agriculture); et al. One Health Zoonotic Diseases Prioritization for Multisectoral Engagement in the Economic Community of West African States (ECOWAS). Workshop Summary. Dakar, Senegal 2019. Available online: https://www.cdc.gov/onehealth/pdfs/ECOWAS-508.pdf (accessed on 25 September 2020).
- Bahiru, A.; Assefa, A. Prioritization of economically important cattle diseases using participatory epidemiology tools in Lalibela, Sekota, and Ziquala districts of Amhara region, Northern Ethiopia. Vet. Med. Int. 2020, 1–4. [Google Scholar] [CrossRef]
- Campbell, Z.; Coleman, P.; Guest, A.; Kushwaha, P.; Ramuthivheli, T.; Osebe, T.; Perry, B.; Salt, J. Prioritizing smallholder animal health needs in East Africa, West Africa, and South Asia using three approaches: Literature review, expert workshops, and practitioner surveys. Prev. Vet. Med. 2021, 189, 105279. [Google Scholar] [CrossRef]
- Cediel, N.; Villamil, L.C.; Romero, J.; Renteria, L.; de Meneghi, D. Setting priorities for surveillance, prevention, and control of zoonoses in Bogotá, Colombia. RPSP 2013, 33, 316–324. [Google Scholar] [CrossRef] [Green Version]
- Ng, V.; Sargeant, J.M. A quantitative approach to the prioritization of zoonotic diseases in North America: A health professionals’ perspective. PLoS ONE 2013, 8, e72172. [Google Scholar] [CrossRef] [PubMed]
- Krause, G.; Prioritization Working Group. How can infectious diseases be prioritized in public health? A standardized prioritization scheme for discussion. EMBO Rep. 2008, 9, S22–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ANSES. Méthodologie de Hiérarchisation des Maladies Animals, Application aux Agents Pathogènes Exotiques pour la France Métropolitaine; Rapport D’expertise Collective: Paris, France, 2012.
- Humblet, M.-F.; Vandeputte, S.; Albert, A.; Gosset, C.; Kirschvink, N.; Haubruge, E.; Fecher-Bourgeois, F.; Pastoret, P.P.; Saegerman, C. Multidisciplinary and evidence-based method for prioritizing diseases of food-producing animals and zoonoses. Emerging. Infect. Dis. 2012, 18, e1. [Google Scholar] [CrossRef] [PubMed]
- Bianchini, J.; Humblet, M.-F.; Cargnel, M.; Van der Stede, Y.; Koenen, F.; de Clercq, K.; Saegerman, C. Prioritization of livestock transboundary diseases in Belgium using a multicriteria decision analysis tool based on drivers of emergence. Transbound. Emerg. Dis. 2020, 67, 344–376. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.J.; Ward, M.P.; Garner, M.G. A framework for assessing the intangible impacts of emergency animal disease. Prev. Vet. Med. 2013, 111, 194–199. [Google Scholar] [CrossRef] [PubMed]
- De La Rocque, S.; Rioux, J.A.; Slingenbergh, J. Climate change: Effects on animal disease systems and implications for surveillance and control. Sci. Tech. Rev. 2008, 27, 339–354. [Google Scholar]
- Dodet, B.; Tejiokem, M.C.; Aguemon, A.R.; Bourhy, H. Human rabies deaths in Africa: Breaking the cycle of indifference. Int. Health 2015, 7, 4–6. [Google Scholar] [CrossRef] [Green Version]
- Hampson, K.; Coudeville, L.; Lembo, T.; Sambo, M.; Kieffer, A.; Attlan, M. Estimating the global burden of endemic canine rabies. PLoS Negl. Trop. Dis. 2015, 9, e0003709. [Google Scholar] [CrossRef] [Green Version]
- Knobel, D.L.; Cleaveland, S.; Coleman, P.G.; Fèvre, E.M.; Meltzer, M.I.; Miranda, M.E.G.; Shaw, A.; Zinsstag, J.; Meslin, F.-X. Re-evaluating the burden of rabies in Africa and Asia. Bull. World Health Organ. 2005, 83, 360–368. [Google Scholar] [PubMed]
- Ducrotoy, M.; Bertu, W.J.; Matope, G.; Cadmus, S.; Conde-Álvarez, R.; Gusi, A.M.; Welburn, S.; Ocholi, R.; Blasco, J.M.; Moriyón, I. Brucellosis in Sub-Saharan Africa: Current challenges for management, diagnosis and control. Acta Trop. 2017, 165, 179–193. [Google Scholar] [CrossRef]
- Franc, K.A.; Krecek, R.C.; Häsler, B.N.; Arenas-Gamboa, A.M. Brucellosis remains a neglected disease in the developing world: A call for interdisciplinary action. BMC Public Health 2018, 18, 125. [Google Scholar] [CrossRef]
- Simpson, G.; Thompson, P.N.; Saegerman, C.; Marcotty, T.; Letesson, J.J.; de Bolle, X.; Godfroid, J. Brucellosis in wildlife in Africa: A systematic review and meta-analysis. Sci. Rep. 2021, 16, 5960. [Google Scholar] [CrossRef] [PubMed]
- Lokamar, P.N.; Kutwah, M.A.; Atieli, H.; Gumo, S.; Ouma, C. Socio-economic impacts of brucellosis on livestock production and reproduction performance in Koibatek and Marigat regions, Baringo County, Kenya. BMC Vet. Res. 2020, 16, 61. [Google Scholar] [CrossRef] [Green Version]
- Salaam-Blyther, T. US and the International Responses to the Ebola Outbreak in West Africa; Report 7-7500 (R43697); CRS (Congressional Research Service): Washington, DC, USA, 2014.
- UNDP (United Nations Development Programme)-Regional Bureau for Africa (UNDP-RBA). Ebola Virus Disease Outbreak (EVD) is overstressing the fiscal capacity of Governments in Guinea, Liberia and Sierra Leone. Afr. Policy Note 2014, 1, 24. [Google Scholar]
- UNDG (United Nations Development Group)–Western and Central Africa. Socio-Economic Impact of Ebola Virus Disease in West African Countries: A Call for National and Regional Containment, Recovery and Prevention; UNDG (United Nations Development Group)–Western and Central Africa: Dakar, Senegal, 2015. [Google Scholar]
- Romero-Alvarez, D.; Peterson, A.T.; Salzer, J.S.; Pittiglio, C.; Shadomy, S.; Traxler, R. Potential distributions of Bacillus anthracis and Bacillus cereus biovar anthracis causing anthrax in Africa. PLoS Negl. Trop. Dis. 2020, 14, e0008131. [Google Scholar] [CrossRef] [Green Version]
- WHO (World Health Organization). Anthrax in Humans and Animals, 4th ed.; World Health Organization Press: Geneva, Switzerland, 2008. [Google Scholar]
- Jernigan, J.A.; Stephens, D.S.; Ashford, D.A.; Omenaca, C.; Topiel, M.S.; Galbraith, M.; Tapper, M.; Fisk, T.L.; Zaki, S.; Popovic, T.; et al. Bioterrorism-related inhalational anthrax: The first 10 cases reported in the United States. Emerging. Infect. Dis. 2001, 7, 933–944. [Google Scholar] [CrossRef] [PubMed]
- Lancelot, R.; Béral, M.; Rakotoharinome, V.M.; Andriamandimby, S.F.; Heraud, J.-M.; Coste, C.; Apolloni, A.; Squarzoni-Diaw, C.; de La Rocque, S.; Formenty, P.B.; et al. Drivers of Rift Valley fever epidemics in Madagascar. Proc. Natl. Acad. Sci. USA 2017, 114, 938–943. [Google Scholar] [CrossRef] [Green Version]
- Wright, D.; Kortekaas, J.; Bowden, T.A.; Warimwe, G.M. Rift Valley fever: Biology and epidemiology. J. Gen. Virol. 2019, 100, 1187–1199. [Google Scholar] [CrossRef]
- Cosivi, O.; Grange, J.M.; Daborn, C.J.; Raviglione, M.C.; Fujikura, T.; Robinson, R.A.; Huchzermeyer, H.F.; de Kantor, I.; Meslin, F.X. Zoonotic tuberculosis due to Mycobacterium bovis in developing countries. Emerg. Infect. Dis. 1998, 4, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Ayele, W.Y.; Neill, S.D.; Zinsstag, J.; Weiss, M.G.; Pavlik, I. Bovine tuberculosis: An old disease but a new threat to Africa. Int. J. Tuberc. Lung Dis. 2004, 8, 924–937. [Google Scholar]
- Etter, E.; Donado, P.; Jori, F.; Caron, A.; Goutard, F.; Roger, F. Risk analysis and bovine tuberculosis, a re-emerging zoonosis. Ann. N. Y. Acad. Sci. 2006, 1081, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Thoen, C.O.; Steele, J.H.; Kaneene, J.B. Zoonotic Tuberculosis: Mycobacterium Bovis and Other Pathogenic Mycobacteria; John Wiley & Sons: Oxford, UK, 2014. [Google Scholar]
- Tambi, N.E.; Maina, W.O.; Ndi, C. An estimation of the economic impact of contagious bovine pleuropneumonia in Africa. OIE Rev. Sci. Tech. 2006, 25, 999–1012. [Google Scholar] [CrossRef]
- Harrison, J.L.; Alders, R.G. An assessment of chicken husbandry including Newcastle disease control in rural areas of Chibuto, Mozambique. Trop. Anim. Health Prod. 2010, 42, 729–736. [Google Scholar] [CrossRef]
- Knight-Jones, T.J.D.; Rushton, J. The economic impacts of foot and mouth disease–What are they, how big are they and where do they occur? Prev. Vet. Med. 2013, 112, 161–173. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.A.; Rich, K.M.; Mariner, J.C.; Anderson, J.; Jeggo, M.; Thevasagayam, S.; Cai, Y.; Peters, A.R.; Roeder, P. The economic impact of eradicating peste des petits ruminants: A benefit-cost analysis. PLoS ONE 2016, 11, e0149982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iqbal Yatoo, M.; Raffiq Parray, O.; Tauseef Bashir, S.; Muheet, A.B.R.; Gopalakrishnan, A.; Karthik, K.; Dhama, K.; Singh, S.V. Contagious caprine pleuropneumonia—A comprehensive review. Vet. Q. 2019, 39, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Mort, M.; Convery, I.; Baxter, J.; Bailey, C. Psychosocial effects of the 2001 UK foot and mouth disease epidemic in a rural population: Qualitative diary based study. BMJ 2005, 331, 1234–1237. [Google Scholar] [CrossRef] [Green Version]
- Souley Kouato, B.; Thys, E.; Renault, V.; Abatih, E.; Marichatou, H.; Issa, S.; Saegerman, C. Spatio-temporal patterns of foot-and-mouth disease transmission in cattle between 2007 and 2015 and quantitative assessment of the economic impact of the disease in Niger. Transbound. Emerg. Dis. 2018, 65, 1049–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboe, P.A.T.; Boa-Amponsem, K.; Okantah, S.A.; Butler, E.A.; Dorward, P.T.; Bryant, M.J. Free-range village chickens on the Accra Plains, Ghana: Their husbandry and productivity. Trop. Anim. Health Prod. 2006, 38, 235–248. [Google Scholar] [CrossRef]
- Otim, M.O.; Kabagambe, E.K.; Mukiibi, G.M.; Christensen, H.; Bisgaard, M. A study of risk factors associated with Newcastle disease epidemics in village free-range chickens in Uganda. Trop. Anim. Health Prod. 2007, 39, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Bessell, P.R.; Auty, H.K.; Roberts, H.; McKendrick, I.J.; Bronsvoort, B.M.C.; Boden, L.A. A tool for prioritizing livestock disease threats to Scotland. Front. Vet. Sci. 2020, 7, 223. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.D. Responding to global infectious disease outbreaks: Lessons from SARS on the role of risk perception, communication and management. Soc. Sci. Med. 2006, 63, 3113–3123. [Google Scholar] [CrossRef]
- Heffernan, C. Panzootics and the poor: Devising a global livestock disease prioritisation framework for poverty alleviation. OIE Rev. Sci. Tech. 2009, 28, 897–907. [Google Scholar] [CrossRef] [Green Version]
- Keeney, R.L. Common mistakes in making value tradeoffs. Oper. Res. 2002, 50, 935–945. [Google Scholar] [CrossRef]
- Del Rio Vilas, V.; Montibeller, G.; Franco, L. Prioritisation of infectious diseases in public health: Feedback on the prioritisation methodology, 15 July 2008 to 15 January 2009 [Letter to the editor]. Eurosurveillance 2011, 27, 7–16. [Google Scholar]
- FAO. Challenges of animal health information systems and surveillance for animal diseases and zoonoses. In Proceedings of the International Workshop Organized by FAO, Rome, Italy, 23–26 November 2010; FAO Animal Production and Health Proceedings: Rome, Italy, 2011. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Region–Country–Locality | Year | Scale | Purpose of Prioritization | Methods | Reference |
|---|---|---|---|---|---|
| Burkina Faso, Cameroon, Cote d’Ivoire, Democratic Republic of Congo, Ethiopia *, Kenya *, Mali, Mozambique, Tanzania *, Uganda * | 2015–2018 | National | To identify zoonotic diseases of greatest national concern for the concerned countries using equal input from representatives of human health, animal resources, and the environment | Semi quantitative, CDC OHZDP tool | [12,13,14,15,16,17,18,19,20,21,22,23] |
| Burundi, Djibouti, Eritrea, Ethiopia *, Kenya *, Rwanda, South-Sudan, Sudan, Tanzania *, Uganda * | 2015–2016 | National | To identify, prioritize, and categorize the key transboundary animal diseases and zoonoses for public policy and animal health programs at the national level | Semi quantitative, OIE Phylum tool | [24,25,26,27,28,29,30,31,32,33] |
| ECOWAS (Benin, Burkina Faso Cape Verde, Côte d’Ivoire, Gambia, Ghana, Guinea, Guinea Bissau, Liberia, Mali, Niger, Nigeria, Senegal, Sierra Leone, Togo | 2019 | Regional | To use a multisectoral, One Health approach to identify zoonotic diseases of greatest regional concern for ECOWAS (13 countries) | Semi quantitative, CDC OHZDP tool | [34] |
| Ethiopia * (districts of Lalibela, Sekota, and Ziquala) | 2016–2018 | Local | To identify and prioritize primary cattle disease with the aid of participatory epidemiology tools (i.e., focus group discussions and questionnaires) | Participatory epidemiology tool | [35] |
| West Africa: Senegal, Mali, Ghana, Burkina Faso, Cote D’Ivoire, Chad, Togo, Benin, Nigeria, Sierra Leone. East Africa: Tanzania *, Kenya *, Uganda *, Ethiopia *, South Sudan, Malawi, Mozambique, Zambia | 2019 | Regional | To prioritize animal health needs in East and West Africa and South Asia to identify diseases and syndromes that impact livestock keepers | -Systematic literature Review -Expert workshops -Veterinary practitioner survey | [36] |
| Disease Ranking Criteria | No. Countries | Average Assigned Weight (Range) |
|---|---|---|
| Economic, environmental, and/or social impact | 9 | 0.170 (0.105–0.210) |
| Economic impact only | 0 | |
| Economic and/or social impact | 5 | |
| Economic, environmental, and/or social impact | 4 | |
| Availability of interventions (i.e., vaccines and/or medical treatment) | 10 | 0.174 (0.130–0.206) |
| Epidemic/pandemic potential (and/or sustained transmission in humans) | 7 | 0.201 (0.170–0.220) |
| Human-to-human transmission potential | 7 | |
| History of previous outbreaks | 0 | |
| Severity of disease in humans | 10 | 0.231 (0.180–0.350) |
| Case-fatality rate | 8 | |
| Morbidity and/or mortality rate | 2 | |
| Presence of disease in country and/or region | 8 | 0.232 (0.170–0.330) |
| Human and/or animal cases of illness reported in country and/or region | 6 | |
| Human or animal disease prevalence and distribution in country | 2 | |
| Laboratory capacity/diagnostic testing capacity | 2 | 0.151 (0.143–0.160) |
| Existing multisectoral collaboration | 1 | 0.170 (NA) |
| Bioterrorism potential | 3 | 0.102 (0.040–0.187) |
| Mode of transmission | 1 | 0.200 (NA) |
| Classification Criteria | |||||||
|---|---|---|---|---|---|---|---|
| Economic Impact | Human Health Impact | Societal Impact | Environmental Impact | ||||
| Justification | % | Justification | % | Justification | % | Justification | % |
| Export and trade bans | 100 | Zoonotic disease | 100 | Zoonotic disease | 100 | Contamination of the environment | 100 |
| High mortality | 80 | High cost of control and prevention for public health | 80 | Mortality in animals | 80 | Disposal of animals | 80 |
| High morbidity | 80 | Export and trade bans | 60 | Mortality/case fatality in humans | 80 | Cleaning and disinfecting costs | 60 |
| Hindering industry | 80 | Negative impact on tourism | 40 | Negative impact on pastoralists (poverty) | 80 | Risk for wildlife | 60 |
| High cost of animal disease control and prevention | 60 | Number of reported cases | 40 | Impact on consumption habit | 60 | ||
| High cost of control and prevention for public health | 60 | Mode of transmission | 40 | Morbidity in animals | 60 | ||
| Cost if introduced | 40 | Mortality/case fatality | 40 | Production lost | 60 | ||
| Highly contagious | 40 | Bioterrorism potential | 20 | Social stress | 60 | ||
| Production lost | 40 | Effect on livelihood | 20 | ||||
| Zoonotic disease | 40 | Endemic zoonoses | 20 | High cost of animal disease control and prevention | 40 | ||
| Endemic disease | 20 | Food borne | 20 | High cost of control and prevention for public health | 40 | ||
| Food borne | 20 | Highly contagious | 20 | Number of reported cases | 40 | ||
| Negative impact on pastoralists (poverty) | 20 | Movement restriction | 20 | Bioterorrism potential | 40 | ||
| Negative impact on tourism | 20 | Export and trade bans | 20 | ||||
| Great public importance and implications | 60 | Trade bans | 80 | Control measures’ constraints | 100 | ||
| High mortality | 60 | Endemic | 60 | Wildlife susceptibility | 60 | ||
| Vaccine constraints | 60 | Highly contagious | 60 | Zoonotic disease | 40 | ||
| Culling constraint | 20 | High cost of control and prevention for public health | 60 | Morbidity | 40 | ||
| Food security issues (poultry meat and egg, beef, milk) | 20 | Human economic impacts | 60 | Mortality | 40 | ||
| Testing constraints | 20 | Zoonotic disease | 60 | Consumption habit | 20 | ||
| Local and international trade | 20 | Tourism | 40 | Increased production costs | 20 | ||
| Movement restriction feasibility | 20 | Increased production costs | 20 | Environmental contamination | 20 | ||
| Vector control feasibility | 20 | Control constraints | |||||
| Zoonotic disease | 20 | ||||||
| Country | OHZDP * Tool | Phylum Tool | ||||||
|---|---|---|---|---|---|---|---|---|
| No Listed Diseases | No Prioritized Endemic Diseases [A] | No of Prioritized Exotic Diseases [B] | Total [A] + [B] | No Listed Diseases | No Prioritized Endemic Diseases [C] | No Prioritized Exotic Diseases [D] | Total [C] + [D] | |
| Burkina Faso a | 41 | 4 | 1 | 5 | ||||
| Burundi b | 23 | 10 | 6 | 16 | ||||
| Cameroon a | 41 | 4 | 1 | 5 | ||||
| Cote d’Ivoire a | 40 | 5 | 1 | 6 | ||||
| Democratic Republic of Congo a | 11 | 6 | 0 | 6 | ||||
| Djibouti b | 15 | 6 | 0 | 6 | ||||
| Eritrea b | 16 | 7 | 4 | 11 | ||||
| Ethiopia c | 43 | 5 | 0 | 5 | 16 | 7 | 3 | 10 |
| Kenya c | 36 | 5 | 0 | 5 | 15 | 13 | 2 | 15 |
| Mali a | 38 | 5 | 0 | 5 | ||||
| Mozambique a | 48 | 6 | 1 | 7 | ||||
| Rwanda b | 16 | 10 | 6 | 16 | ||||
| South-Sudan b | 15 | 12 | 3 | 15 | ||||
| Sudan b | 11 | 6 | 6 | 12 | ||||
| Tanzania c | 39 | 5 | 1 | 6 | 16 | 7 | 2 | 9 |
| Uganda c | 48 | 6 | 1 | 7 | 16 | 10 | 3 | 13 |
| Average (S.E. **) | 38.5 (3.30) | 5.1 (0.23) | 0.6 (0.16) | 5.7 (0.26) | 15.9 (0.92) | 8.8 (0.80) | 3.5 (0.64) | 12.3 (1.05) |
| Type | Disease or Health Condition | Causative Agent | No of Countries | |||
|---|---|---|---|---|---|---|
| OHZDP Tool a | Phylum Tool b | |||||
| Endemic | Exotic | Endemic | Exotic | |||
| Zoonosis | Rabies | Virus | 10 | 7 | 1 | |
| Anthrax | Bacteria | 7 | 1 | |||
| Brucellosis | Bacteria | 7 | 8 | |||
| Zoonotic influenza | Virus | 5 | 2 | 1 | 9 | |
| Hemorrhagic fever (Ebola/Marbug) | Virus | 4 | 2 | 2 | ||
| Rift Valley fever | Virus | 4 | 3 | 5 | ||
| Trypanosomiasis | Parasite | 3 | 1 | 1 | ||
| Zoonotic tuberculosis (M. bovis) | Bacteria | 3 | 6 | 1 | ||
| Lassa | Virus | 2 | ||||
| Salmonellosis | Bacteria | 2 | ||||
| Arboviral diseases * | Virus | 1 | ||||
| Crimean-Congo hemorrhagic fever | Virus | 1 | ||||
| Dengue | Virus | 1 | ||||
| Echinococcosis | Parasite | 1 | ||||
| Leptospirosis | Bacteria | 1 | ||||
| Monkey pox | Virus | 1 | ||||
| Plague | Virus | 1 | ||||
| MERS-CoV ** | Virus | 1 | ||||
| Swine erysipelas | 1 | |||||
| TAD | Foot and mouth disease | Virus | 10 | 6 | ||
| Peste des petits ruminants | Virus | 9 | 1 | |||
| Contagious bovine pleuropneumonia | Bacteria | 8 | 2 | |||
| New Castle disease | Virus | 7 | ||||
| Contagious caprine pleuropneumonia | Bacteria | 5 | ||||
| African swine fever | Virus | 4 | 1 | |||
| Lumpy skin disease | Virus | 4 | ||||
| Sheep and goat pox | Virus | 3 | 1 | |||
| East coast fever | Parasite | 2 | ||||
| Porcine cysticercosis | Parasite | 1 | ||||
| Classical swine fever | Virus | 1 | ||||
| PRRS *** | Virus | 1 | ||||
| Camel pox | Virus | 1 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mpouam, S.E.; Mingoas, J.P.K.; Mouiche, M.M.M.; Kameni Feussom, J.M.; Saegerman, C. Critical Systematic Review of Zoonoses and Transboundary Animal Diseases’ Prioritization in Africa. Pathogens 2021, 10, 976. https://doi.org/10.3390/pathogens10080976
Mpouam SE, Mingoas JPK, Mouiche MMM, Kameni Feussom JM, Saegerman C. Critical Systematic Review of Zoonoses and Transboundary Animal Diseases’ Prioritization in Africa. Pathogens. 2021; 10(8):976. https://doi.org/10.3390/pathogens10080976
Chicago/Turabian StyleMpouam, Serge Eugene, Jean Pierre Kilekoung Mingoas, Mohamed Moctar Mouliom Mouiche, Jean Marc Kameni Feussom, and Claude Saegerman. 2021. "Critical Systematic Review of Zoonoses and Transboundary Animal Diseases’ Prioritization in Africa" Pathogens 10, no. 8: 976. https://doi.org/10.3390/pathogens10080976
APA StyleMpouam, S. E., Mingoas, J. P. K., Mouiche, M. M. M., Kameni Feussom, J. M., & Saegerman, C. (2021). Critical Systematic Review of Zoonoses and Transboundary Animal Diseases’ Prioritization in Africa. Pathogens, 10(8), 976. https://doi.org/10.3390/pathogens10080976