
Effectiveness of Disinfection with Chlorine Dioxide on Respiratory Transmitted, Enteric, and Bloodborne Viruses: A Narrative Synthesis


 ,
,  and
and
Abstract
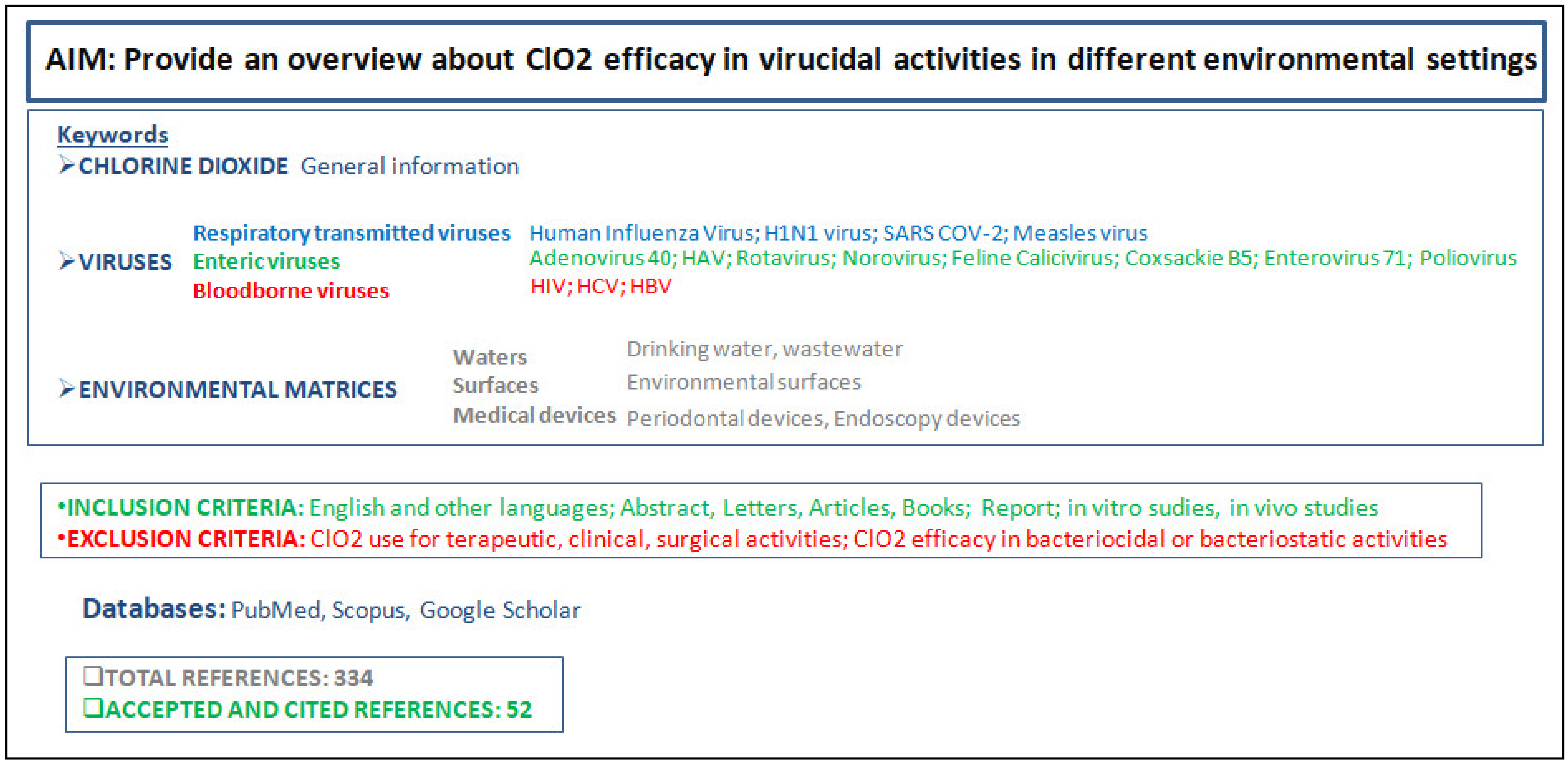
1. Introduction
1.1. Virucidal Activity of ClO2
1.2. ClO2 Activity on Respiratory Transmitted Viruses
1.3. ClO2 Activity on Enteric Viruses
1.4. ClO2 Activity on Bloodborne Viruses
2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ma, J.-W.; Huang, B.-S.; Hsu, C.-W.; Peng, C.-W.; Cheng, M.-L.; Kao, J.-Y.; Way, T.-D.; Yin, H.-C.; Wang, S.-S. Efficacy and Safety Evaluation of a Chlorine Dioxide Solution. Int. J. Environ. Res. Public Heal 2017, 14, 329. [Google Scholar] [CrossRef]
- Symons, J.M.; Stevens, A.; Clark, R.M.; Geldreich, E.E.; Love, O.T., Jr.; DeMarco, J. Treatment tecniques for controlling trihalomethanes in drinking water. Cincinnati EPA 1981, 1, 10–22. [Google Scholar]
- Michael, G.E.; Miday, R.K.; Bercz, J.P.; Miller, R.G.; Greathouse, D.G.; Kraemer, D.F.; Lucas, J.B. Chlorine Dioxide Water Disinfection: A Prospective Epidemiology Study. Arch. Environ. Health Int. J. 1981, 36, 20–27. [Google Scholar] [CrossRef] [PubMed]
- WHO. Quantifying selected major risks to health. In The World Health Report 2002; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Ngwenya, N.; Ncube, E.J.; Parsons, J. Recent Advances in Drinking Water Disinfection: Successes and Challenges No Title. Rev. Environ. Contam. Toxicol. 2013, 22, 111–170. [Google Scholar]
- Thurston-Enriquez, J.A.; Haas, C.N.; Jacangelo, J.; Gerba, C.P. Inactivation of enteric adenovirus and feline calicivirus by ozone. Water Res. 2005, 39, 3650–3656. [Google Scholar] [CrossRef] [PubMed]
- Aieta, E.M.; Berg, J.D. A review of chlorine dioxide in drinking water treatment. J. Am. Water Work. Assoc. 1986, 78, 62–72. [Google Scholar] [CrossRef]
- Noszticzius, Z.; Wittmann, M.; Kály-Kullai, K.; Beregvári, Z.; Kiss, I.; Rosivall, L.; Szegedi, J. Chlorine Dioxide Is a Size-Selective Antimicrobial Agent. PLoS ONE 2013, 8, e79157. [Google Scholar] [CrossRef] [PubMed]
- Kály-Kullai, K.; Wittmann, M.; Noszticzius, Z.; Rosivall, L. Can chlorine dioxide prevent the spreading of coronavirus or other viral infections? Medical hypotheses. Physiol. Int. 2020, 107, 1–11. [Google Scholar] [CrossRef]
- Noss, C.I.; Hauchman, F.S.; Olivieri, V.P. Chlorine dioxide reactivity with proteins. Water Res. 1986, 20, 351–356. [Google Scholar] [CrossRef]
- Arbely, E.; Granot, Z.; Kass, I.; Orly, A.J.; Arkin, I. A Trimerizing GxxxG Motif Is Uniquely Inserted in the Severe Acute Respiratory Syndrome (SARS) Coronavirus Spike Protein Transmembrane Domain†. Biochemistry 2006, 45, 11349–11356. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shigematsu, S.; Dublineau, A.; Sawoo, O.; Batéjat, C.; Matsuyama, T.; Leclercq, I.; Manuguerra, J.-C. Influenza A virus survival in water is influenced by the origin species of the host cell. Influenza Respir. Viruses 2013, 8, 123–130. [Google Scholar] [CrossRef]
- Berman, D.; Hoff, J.C. Inactivation of simian rotavirus SA11 by chlorine, chlorine dioxide, and monochloramine. Appl. Environ. Microbiol. 1984, 48, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Sanekata, T.; Fukuda, T.; Miura, T.; Morino, H.; Lee, C.; Maeda, K.; Araki, K.; Otake, T.; Kawahata, T.; Shibata, T. Evaluation of the antiviral activity of chlorine dioxide and sodium hypochlorite against feline calicivirus, human influenza virus, measles virus, canine distemper virus, human herpesvirus, human adenovirus, canine adenovirus and canine parvovirus. Biocontrol Sci. 2010, 15, 45–49. [Google Scholar] [CrossRef]
- Li, J.W.; Xin, Z.T.; Wang, X.W.; Zheng, J.L.; Chao, F.H. Mechanisms of inactivation of hepatitis A virus in water by chlorine dioxide. Water Res. 2004, 38, 1514–1519. [Google Scholar] [CrossRef] [PubMed]
- Jolley, R.L.; Brungs, W.A.; Cotruvo, J.A.; Cumming, R.B.; Mattice, J.S.; Jacobs, V.A. Nucleic Acids and Proteins. In Proceedings of the Water Chlorination: Environmental Impact and Health Effects; Chemistry and Water Treatment: Pacific Grove, CA, USA, 1983. [Google Scholar]
- Jolley, R.L.; Davis, W.P.; Katz, S.; Roberts, M.H.; Bull, R.J. Water chlorination: Chemistry, environmental impact and health effects. In Proceedings of the Fifth Conference on Water Chlorination: Environmental Impact and Health Effects, Williamsburg, VA, USA, 3–8 June 1984. [Google Scholar]
- Palcsó, B.; Moldován, Z.; Süvegh, K.; Herczegh, A.; Zelkó, R. Chlorine dioxide-loaded poly (acrylic acid) gels for prolonged antimicrobial effect. Mater. Sci. Eng. C 2019, 98, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Lénès, D.; Deboosere, N.; Ménard-Szczebara, F.; Jossent, J.; Alexandre, V.; Machinal, C.; Vialette, M. Assessment of the removal and inactivation of influenza viruses H5N1 and H1N1 by drinking water treatment. Water Res. 2010, 44, 2473–2486. [Google Scholar] [CrossRef]
- Ogata, N.; Shibata, T. Protective effect of low-concentration chlorine dioxide gas against influenza A virus infection. J. Gen. Virol. 2008, 89, 60–67. [Google Scholar] [CrossRef]
- Lentz, M.R.; Webster, R.G.; Air, G. Site-directed mutation of the active site of influenza neuraminidase and implications for the catalytic mechanism. Biochemistry 1987, 26, 5351–5358. [Google Scholar] [CrossRef]
- Ogata, N. Inactivation of influenza virus haemagglutinin by chlorine dioxide: Oxidation of the conserved tryptophan 153 residue in the receptor-binding site. J. Gen. Virol. 2012, 93, 2558–2563. [Google Scholar] [CrossRef]
- Carducci, A.; Federigi, I.; Liu, D.; Thompson, J.R.; Verani, M. Making Waves: Coronavirus detection, presence and persistence in the water environment: State of the art and knowledge needs for public health. Water Res. 2020, 179, 115907. [Google Scholar] [CrossRef]
- Wang, X.-W.; Li, J.-S.; Jin, M.; Zhen, B.; Kong, Q.-X.; Song, N.; Xiao, W.-J.; Yin, J.; Wei, W.; Wang, G.-J.; et al. Study on the resistance of severe acute respiratory syndrome-associated coronavirus. J. Virol. Methods 2005, 126, 171–177. [Google Scholar] [CrossRef]
- Singh, S.; Kumar, V.; Kapoor, D.; Dhanjal, D.S.; Bhatia, D.; Jan, S.; Singh, N.; Romero, R.; Ramamurthy, P.C.; Singh, J. Detection and disinfection of COVID-19 virus in wastewater. Environ. Chem. Lett. 2021, 19, 1917–1933. [Google Scholar] [CrossRef] [PubMed]
- Aguiar-Oliveira, M.d.L.; Campos, A.; Matos, A.R.; Rigotto, C.; Sotero-Martins, A.; Teixeira, P.F.P.; Siqueira, M.M. Wastewater-Based Epidemiology (WBE) and Viral Detection in Polluted Surface Water: A Valuable Tool for COVID-19 Surveillance—A Brief Review. Int. J. Environ. Res. Public Health 2020, 17, 9251. [Google Scholar] [CrossRef]
- Deborde, M.; von Gunten, U. Reactions of chlorine with inorganic and organic compounds during water treatment-Kinetics and mechanisms: A critical review. Water Res. 2008, 42, 13–51. [Google Scholar] [CrossRef]
- Zoni, R.; Zanelli, R.; Riboldi, E.; Bigliardi, L.; Sansebastiano, G. Investigation on virucidal activity of chlorine dioxide. experimental data on feline calicivirus, HAV and Coxsackie B5. J. Prev. Med. Hyg. 2007, 48, 91–95. [Google Scholar] [PubMed]
- Xin, Z.T.; Liu, C.; Dong, B.; Gao, Y.P.; Shao, N.S.; Liu, W.; Zhang, J.; Dong, J.; Ling, S.G.; Xue, Y.N. A subtractive fluorescence-activated cellsorting strategy to identify mimotopes of HBV-preS protein from bacterially displayed peptide library. J. Immunol. Methods 2004, 293, 13–21. [Google Scholar] [CrossRef]
- Simonet, J.; Gantzer, C. Degradation of the Poliovirus 1 genome by chlorine dioxide. J. Appl. Microbiol. 2006, 100, 862–870. [Google Scholar] [CrossRef]
- Brigano, F.A.; Scarpino, P.V.; Cronier, S.; Zink, M.L. Effects of particulates on inactivation of enteroviruses in water by chlorine dioxide. In Progress in Wastewater Disinfection Technology; Venosa, A.D., Ed.; Publication no. EPA-600/9-79-018; Environmental Protection Agency: Cincinnati, OH, USA, 1979; pp. 86–92. [Google Scholar]
- Alvarez, M.E.; O’Brien, R.T. Mechanisms of inactivation of poliovirus by chlorine dioxide and iodine. Appl. Environ. Microbiol. 1982, 44, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Zierler, S. Drinking Water and Reproductive Health. Epidemiology 1992, 3, 77–78. [Google Scholar] [CrossRef]
- Granstrom, M.L. Efficiency of Chlorine Dioxide. Microbiology 1965, 13, 5. [Google Scholar]
- Tenno, K.M.; Fujioka, R.S.; Loh, P.C. The mechanism of poliovirus inactivation by hypochlorous acid. In Proceedings of the 3rd Conference on Water Chlorination: Environmental Impact and Health Effects, Colorado Springs, CO, USA, 28 October–2 November 1979; Jolley, R., Brungs, W.A., Cumming, R.B., Eds.; Ann Arbor Science Publishers: Lansing, MI, USA, 1980; pp. 665–675. [Google Scholar]
- Harakeh, S. The behavior of viruses on disinfection by chlorine dioxide and other disinfectants in effluent. FEMS Microbiol. Lett. 1987, 44, 335–341. [Google Scholar] [CrossRef]
- Jolley, R.L. Water Chlorination: Environmental Impact and Health Effects. In Proceedings of the 3rd Conference on Water Chlorination: Environmental Impact and Health Effects, Colorado Springs, CO, USA, 28 October–2 November 1979; Ann Arbor Science Publishers: Lansing, MI, USA, 1980. [Google Scholar]
- Simonet, J.; Gantzer, C. Inactivation of Poliovirus 1 and F-Specific RNA Phages and Degradation of Their Genomes by UV Irradiation at 254 Nanometers. Appl. Environ. Microbiol. 2006, 72, 7671–7677. [Google Scholar] [CrossRef] [PubMed]
- Tachikawa, M.; Saita, K.; Tezuka, M.; Sawamura, R. Inactivation of poliovirus with chlorine dioxide. Eisei Kagaku 1993, 39, 572–576. [Google Scholar] [CrossRef]
- Farr, R.W.; Walton, C. Inactivation of Human Immunodeficiency Virus by a Medical Waste Disposal Process Using Chlorine Dioxide. Infect. Control. Hosp. Epidemiol. 1993, 14, 527–529. [Google Scholar] [CrossRef]
- Watamoto, T.; Egusa, H.; Sawase, T.; Yatani, H. Clinical evaluation of chlorine dioxide for disinfection of dental instruments. Int. J. Prosthodont. 2013, 26, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Isomoto, H.; Urata, M.; Kawazoe, K.; Matsuda, J.; Nishi, Y.; Wada, A.; Ohnita, K.; Hirakata, Y.; Matsuo, N.; Inoue, K.; et al. Endoscope disinfection using chlorine dioxide in an automated washer-disinfector. J. Hosp. Infect. 2006, 63, 298–305. [Google Scholar] [CrossRef]
- Ebonwu, J.I. Antimicrobial Effect of Slow Release Chlorine Dioxide Disinfectant, in Comparison with Sodium Dichloroisocyanurate. Master’s Thesis, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa, 2010. [Google Scholar]
- Ge, Y.; Zhang, X.; Shu, L.; Yang, X. Kinetics and Mechanisms of Virus Inactivation by Chlorine Dioxide in Water Treatment: A Review. Bull. Environ. Contam. Toxicol. 2021, 106, 560–567. [Google Scholar] [CrossRef]
- US EPA. Contaminant Candidate List (CCL) and Regulatory Determination. 2018. Available online: https//www.epa.gov/ccl/microbialcontaminantsccl-4 (accessed on 30 March 2018).
- Totaro, M.; De Vita, E.; Giorgi, S.; Profeti, S.; Porretta, A.; Gallo, A.; Frendo, L.; Casini, B.; Valentini, P.; Privitera, G.; et al. Comparison of Anolyte and Chlorine Dioxide for a Continuous Hot Water Disinfection in Nursing Home: A Two Years Legionnaires’ Disease Prevention. J. Water Resour. Prot. 2019, 11, 233–243. [Google Scholar] [CrossRef][Green Version]
- Ljujic, B.; Sundac, L. Council Directive 98/83/EC of 3 November 1998 on the quality of water intended for human consumption. Voda Sanitarna Tehnika 1998, 41, 32–54. [Google Scholar] [CrossRef]
- Lu, M.-C.; Chen, P.-L.; Huang, D.-J.; Liang, C.-K.; Hsu, C.-S.; Liu, W.-T. Disinfection efficiency of hospital infectious disease wards with chlorine dioxide and hypochlorous acid. Aerobiologia 2020, 37, 29–38. [Google Scholar] [CrossRef]
- Abreu, A.C.; Tavares, R.R.; Borges, A.; Mergulhão, F.; Simões, M. Current and emergent strategies for disinfection of hospital environments. J. Antimicrob. Chemother. 2013, 68, 2718–2732. [Google Scholar] [CrossRef] [PubMed]
- British Standards Institution. Chemical disinfectants and antiseptics—Quantitative suspension test for the evaluation of bactericidal activity in the medical area—Test method and requirements (phase 2, step 1). Eur. Comm. Stand. 2012, 3. Available online: https://shop.bsigroup.com/ProductDetail/?pid=000000000030318657 (accessed on 1 October 2012).
- Gruppo di lavoro ISS Biocidi COVID-19. Raccomandazioni ad Interim sui Disinfettanti Nell’Attuale Emergenza COVID-19: Presidi Medico Chirurgici e Biocidi; Rapporto ISS COVID-19 n. 19/2020 Rev.; Superior Institute of Health: Rome, Italy, 2020. [Google Scholar]
- Block, S.S. Disinfection, Sterilization, and Preservation, 5th ed.; Limpicott Williams & Wilkins: Gainesville, FL, USA, 2011. [Google Scholar]


{kind=link}
| Chlorine Dioxide Concentration | Exposure Time | Viral Reduction | Author and Year |
|---|---|---|---|
| 1 mg/L | 15 s | Human influenza virus (99.9%) | Sanekata 2010 |
| 0.5 mg/L | 5 min | H1N1 virus (99.9%) | Lénès 2010 |
| 20 mg/L in sewage | 30 min | SARS-CoV-2 (99.99%) | Carducci 2020 |
| 10 mg/L 100 mg/L | 30 s 15 s | Measles virus (99.99%) | Sanekata 2010 |
| Chlorine Dioxide Concentration | Exposure Time | Viral Reduction | Author and Year |
|---|---|---|---|
| 0.67 mg/L (pH 8) 1.28 mg/L (pH 6) | 1 min | Adenovirus type 40 (4 log) | Thurston-Enriquez 2005 |
| 7.5 mg/L | 10 min | Human Hepatitis A Virus (100%, total genomic damage) | Li 2004 |
| 0.8 mg/L | 0.5 min | Human Hepatitis A Virus (99%) | Zoni 2007 |
| 0.4 mg/L | 5 min | Human Hepatitis A Virus (99%) | Zoni 2007 |
| 0.5 mg/L | 15 s | Rotavirus (4log) | Berman 1984 |
| 1 mg/L 10 mg/L | 3 min 15 s | Norovirus (99.99%) Norovirus (99.99%) | Sanekata 2010 |
| 0.2 mg/L | 30 min | Feline Calicivirus (99.99%) | Zoni 2007 |
| 0.4 mg/L | 4 min | Coxsackie B5 virus (99.99%) | Zoni 2007 |
| 0.5 mg/L | 30 min | Enterovirus 71 (99.99%) | Thurston-Enriquez 2005 |
| 0.5 mg/L | 30 min | Poliovirus 1 (RNA damage) | Simonet 2005 |
| 1 mg/L | 2.5 min | Poliovirus (4 log) | Tachikawa 1993 |
| Chlorine Dioxide Concentration | Exposure Time | Viral Reduction | Author and Year |
|---|---|---|---|
| 30 mg/L (in blood sample) | 5 min | Human Immunodeficiency Virus type 1 (4 log) | Farr 1993 |
| 0.02% 30 mg/L | 10 min 5 min | Hepatitis C Virus (periodontal device) (99.99%) Hepatitis C Virus (endoscopy device) (99.99%) | Watamoto 2013 Isomoto 1998 |
| 24 mg/L (Aseptrol®) | 5 min | Hepatitis B Virus (99.99%) | Ebonwu 2010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Totaro, M.; Badalucco, F.; Costa, A.L.; Tuvo, B.; Casini, B.; Privitera, G.; Menchini Fabris, G.B.; Baggiani, A. Effectiveness of Disinfection with Chlorine Dioxide on Respiratory Transmitted, Enteric, and Bloodborne Viruses: A Narrative Synthesis. Pathogens 2021, 10, 1017. https://doi.org/10.3390/pathogens10081017
Totaro M, Badalucco F, Costa AL, Tuvo B, Casini B, Privitera G, Menchini Fabris GB, Baggiani A. Effectiveness of Disinfection with Chlorine Dioxide on Respiratory Transmitted, Enteric, and Bloodborne Viruses: A Narrative Synthesis. Pathogens. 2021; 10(8):1017. https://doi.org/10.3390/pathogens10081017
Chicago/Turabian StyleTotaro, Michele, Federica Badalucco, Anna Laura Costa, Benedetta Tuvo, Beatrice Casini, Gaetano Privitera, Giovanni Battista Menchini Fabris, and Angelo Baggiani. 2021. "Effectiveness of Disinfection with Chlorine Dioxide on Respiratory Transmitted, Enteric, and Bloodborne Viruses: A Narrative Synthesis" Pathogens 10, no. 8: 1017. https://doi.org/10.3390/pathogens10081017
APA StyleTotaro, M., Badalucco, F., Costa, A. L., Tuvo, B., Casini, B., Privitera, G., Menchini Fabris, G. B., & Baggiani, A. (2021). Effectiveness of Disinfection with Chlorine Dioxide on Respiratory Transmitted, Enteric, and Bloodborne Viruses: A Narrative Synthesis. Pathogens, 10(8), 1017. https://doi.org/10.3390/pathogens10081017