
Malacoplakia of the Uterine Cervix: A Case Report


 , and
, and 
Abstract
:1. Introduction
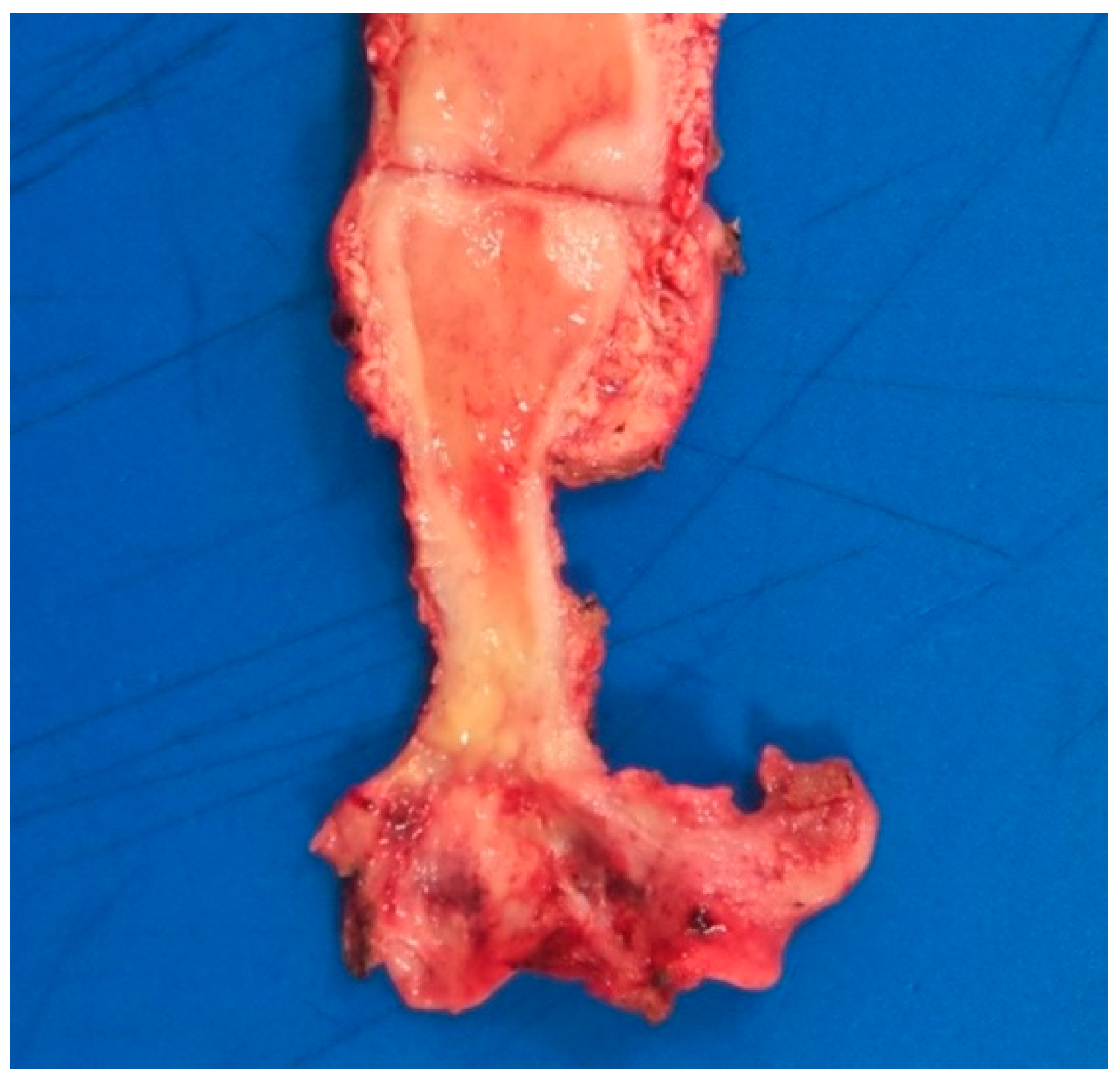
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Michaelis, L.; Gutmann, C. Ueber Einschlüsse in Blasentumoren. Ztschr. Klin. Med. 1902, 47, 208–215. [Google Scholar]
- Darvishian, F.; Teichberg, S.; Meyersfield, S.; Urmacher, C.D. Concurrent malakoplakia and papillary urothelial carcinoma of the urinary bladder. Ann. Clin. Lab. Sci. 2001, 31, 147–150. [Google Scholar] [PubMed]
- Lin, J.I.; Caracta, P.F.; Chang, C.H.; Uchwat, F.; Tseng, C.H. Malacoplakia of the Vagina. South. Med. J. 1979, 72, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Thomas, W.; Sadeghieh, B.; Fresco, R.; Rubenstone, A.I.; Stepto, R.C.; Carasso, B. Malacoplakia of the Endometrium, a Probable Cause of Postmenopausal Bleeding. Am. J. Clin. Pathol. 1978, 69, 637–641. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.J.R.; Thomas, M.A. Malacoplakia of the Uterine Cervix and Endometrium. Cytopathology 1991, 2, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Willén, R.; Stendahl, U.; Willén, H.; Tropé, C. Malacoplakia of the cervix and corpus uteri: A light microscopic, electron microscopic, and X-ray microprobe analysis of a case. Int. J. Gynecol. Pathol. 1983, 2, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Agnarsdóttir, M.; Hahn, L.; Sellgren, U.; Willén, R. Malacoplakia of the cervix uteri and vulva. Acta Obstet. Gynecol. Scand. 2004, 83, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.J.; Survarna, S.K.; Chapple, C.R. Pelvic malakoplakia—An unusual bladder tumour. BJU Int. 1994, 73, 322–323. [Google Scholar] [CrossRef] [PubMed]
- Ramdial, P.K.; Sing, Y.; Chotey, N.A.; Bagratee, J.S. Concomitant Malacoplakia and Granuloma Inguinale of the Cervix in Acquired Immune Deficiency Syndrome. Int. J. Gynecol. Pathol. 2008, 27, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Hall, V. Malakoplakia of the cervix uteri. J. Obstet. Gynaecol. 1996, 16, 62. [Google Scholar] [CrossRef]
- Sonowal, C.; Kalita, P.C.; Das, A.; Rabha, H.; Saikia, A. Malakoplakia of the Uterus: A Rare Cause of Postmenopausal Bleeding Mimicking Malignancy. J. Clin. Diagn. Res. 2019, 13, QD01–QD03. [Google Scholar] [CrossRef]
- Van der Walt, J.J.; Marcus, P.B.; De Wet, J.J.; Burger, A.J. Malacoplakia of the vagina. First case report. S. Afr. Med. J. 1973, 47, 1342–1344. [Google Scholar]
- Rao, N.R. Malacoplakia of broad ligament, inguinal region, and endometrium. Arch. Pathol. 1969, 88, 85–88. [Google Scholar] [PubMed]
- Chalvardjian, A.; Picard, L.; Shaw, R.; Davey, R.; Cairns, J. Malacoplakia of the female genital tract. Am. J. Obstet. Gynecol. 1980, 138, 391–394. [Google Scholar] [CrossRef]
- Wiltenburg, W.; Wouters, M.G.A.J.; Uyterlinde, A.M.; Sporken, J.M.J. Malacoplakie van de tractus genitalis bij een vrouw met postmenopauzaal bloedverlies. Ned. Tijdschr. Geneeskd. 2003, 147, 77–79. [Google Scholar] [PubMed]
- Wahl, R.W. Malacoplakia of the uterine cervix: Report of two cases. Acta Cytol. 1982, 26, 691–694. [Google Scholar] [PubMed]
- Falcon-Escobedo, R.; Mora-Tiscareno, A.; Pueblitz-Peredo, S. Malacoplakia of the uterine cervix: Histologic, cytologic and ultrastructural study of a case. Acta Cytol. 1986, 30, 281–284. [Google Scholar] [PubMed]
- Chen, K.T.; Hendricks, E.J. Malakoplakia of the female genital tract. Obstet. Gynecol. 1985, 65 (Suppl. 3), 84S–87S. [Google Scholar] [PubMed]
- Kapila, K.; Verma, K. Intracellular bacilli in vaginal smears in a case of malacoplakia of the uterine cervix. Acta Cytol. 1989, 33, 410–411. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Age | Clinical Presentation | Other Structure Involved | Immune Suppression | Treatment | E. coli |
|---|---|---|---|---|---|---|
| [14] | 64 | Vaginal bleeding | Vagina | No | Hysterectomy | Urine culture |
| [16] | 72 | Vaginal bleeding. Cervical mass | No | Corticoid therapy | Died before treatment | No |
| [16] | 66 | Vaginal discharge. Friable cervix | No | No | Antibiotic | No |
| [6] | 71 | Vaginal bleeding. Abdominal pain. Cervical mass | Endometrium | No | Hysterectomy | No |
| [18] | 83 | Vaginal bleeding. Cervical mass | Pelvic wall | No | Hysterectomy | Tissue culture |
| [17] | 78 | Vaginal discharge. Friable cervix | No | No | Antibiotics | No |
| [5] | 60 | Vaginal bleeding. Cervical mass | Endometrium | Corticoid therapy | Not reported | No |
| [15] | 74 | Vaginal bleeding. Cervical mass | Endometrium | No | Antibiotics | No |
| [7] | 69 | Ulcerated cervix | No | No | Hysterectomy | No |
| [9] | 27 | Vaginal bleeding. Ulcerated cervix | No | AIDS | Died before treatment | No (GI) |
| [9] | 36 | Vaginal bleeding. Ulcerated cervix | No | AIDS | No follow-up | No (GI) |
| [10] | 81 | Vaginal bleeding. Cervical mass | Vagina | No | Not reported | No |
| Present case | 78 | Vaginal bleeding. Cervical mass. Abdominal pain | Vagina | Corticoid therapy | Hysterectomy | PCR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saco, A.; Rakislova, N.; Marimon, L.; Torne, A.; Diaz-Feijoo, B.; Salvador, R.; Alos, S.; Jordao, D.; Hurtado, J.C.; Ordi, J. Malacoplakia of the Uterine Cervix: A Case Report. Pathogens 2021, 10, 343. https://doi.org/10.3390/pathogens10030343
Saco A, Rakislova N, Marimon L, Torne A, Diaz-Feijoo B, Salvador R, Alos S, Jordao D, Hurtado JC, Ordi J. Malacoplakia of the Uterine Cervix: A Case Report. Pathogens. 2021; 10(3):343. https://doi.org/10.3390/pathogens10030343
Chicago/Turabian StyleSaco, Adela, Natalia Rakislova, Lorena Marimon, Aureli Torne, Berta Diaz-Feijoo, Rafael Salvador, Silvia Alos, Dercio Jordao, Juan Carlos Hurtado, and Jaume Ordi. 2021. "Malacoplakia of the Uterine Cervix: A Case Report" Pathogens 10, no. 3: 343. https://doi.org/10.3390/pathogens10030343
APA StyleSaco, A., Rakislova, N., Marimon, L., Torne, A., Diaz-Feijoo, B., Salvador, R., Alos, S., Jordao, D., Hurtado, J. C., & Ordi, J. (2021). Malacoplakia of the Uterine Cervix: A Case Report. Pathogens, 10(3), 343. https://doi.org/10.3390/pathogens10030343