

Enhancing the Outcomes of Temporalis Fascia Tympanoplasty Using Autologous Platelet-Rich Plasma and Gel: A Randomized Controlled Trial

 ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
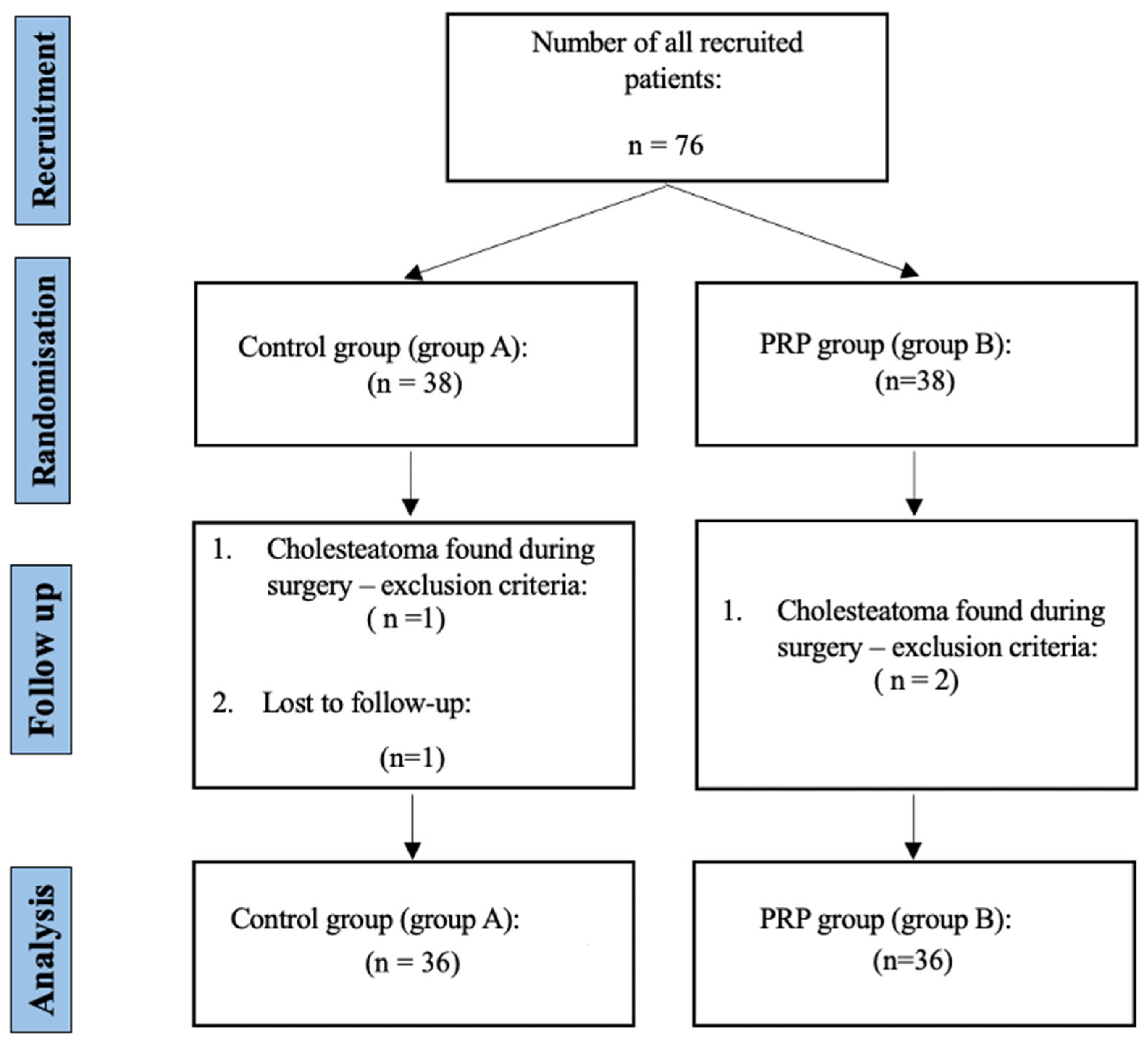
2.1. Recruitment
2.2. Intervention Allocation
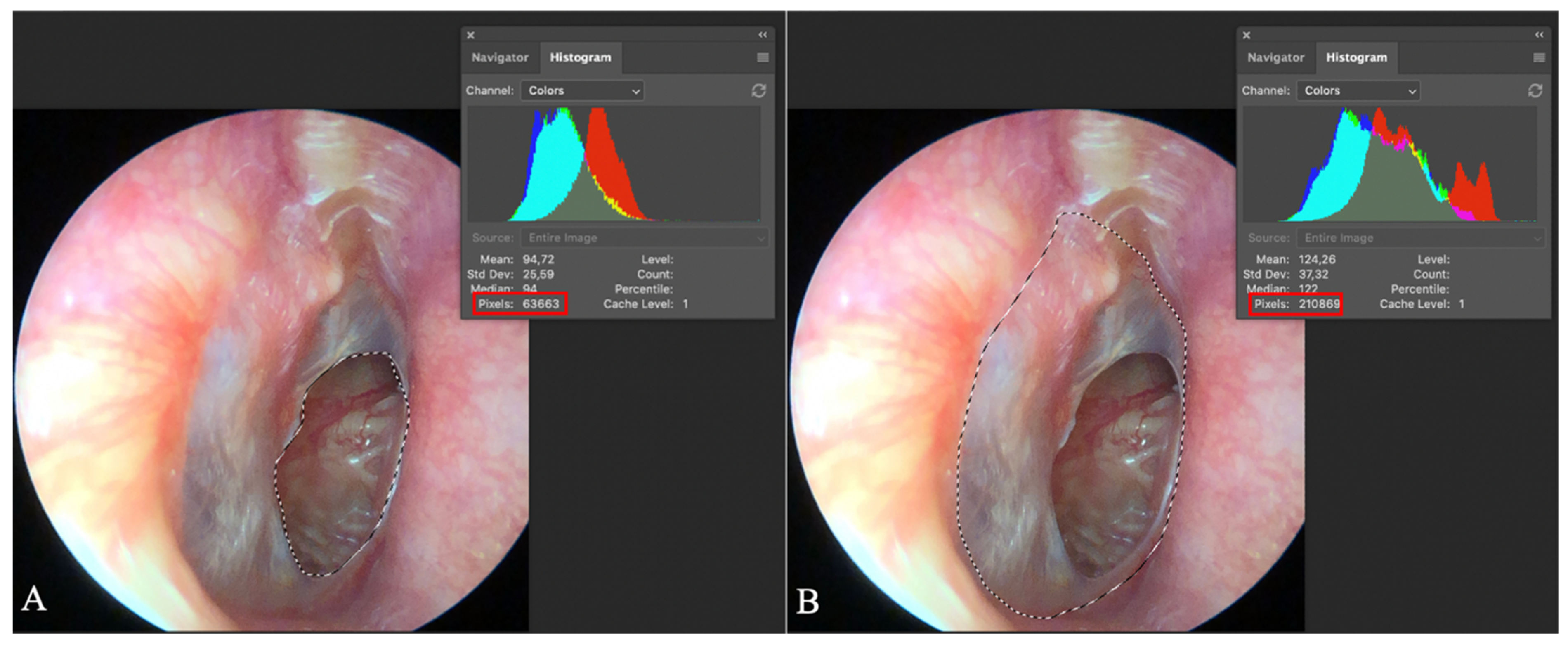
2.3. Preoperative Evaluation
2.4. Surgical Treatment
2.4.1. Surgical Management of the Control Group (Group A)
2.4.2. Surgical Management of the PRP Group (Group B)
- In addition to the 1 mL of ciprofloxacin solution (3 mg/mL), 1 mL of PRP was applied to numerous pieces of atelocollagen sponge. This preparation was then inserted into the middle ear cavity to provide medial support for the graft.
- PRG was applied to the lateral surface of the reconstructed eardrum.
- Finally, the external auditory canal was packed with the remaining pieces of atelocollagen sponge soaked in PRP and ciprofloxacin solution.
2.4.3. Preparation of PRP and PRG
- Blood Collection: Nine milliliters of venous blood was drawn into two four and a half milliliters test tubes containing sodium citrate (9 NC sodium citrate 0.105 M, BD Vacutainer, Becton Dickinson, Franklin Lakes, NJ, USA).
- First Centrifugation: Conducted at 300× g for 5 min at 18 °C, resulting in the blood separating into three distinct layers (plasma, buffy coat and red blood cells).
- ○
- Supernatant (plasma and buffy coat) was carefully removed from the tube and transferred into a new sterile, empty plastic tube.
- Second Centrifugation: Plastic tube with supernatant was centrifuged at 700× g for 17 min at 18 °C, resulting in the sedimentation of platelets and plasma at the bottom of the tube.
- ○
- The upper half of centrifugate was removed and discarded, while the bottom, representing PRP, was collected. A total of 1 mL of PRP was used to prepare PRG, and the remainder was applied to atelocollagen sponge.
- PRG preparation: PRP was exogenously activated by mixing 1 mL of PRP with 10 μL of 1 M CaCl2 (1:100 ratio to PRP) and 0.2 mL of autologous serum (1:5 ratio to PRP).
- ○
- Autologous serum is prepared by centrifuging whole blood in a 4 mL plastic test tube without anticoagulant (Z Serum, Vacutube, LT Burnik, Komenda, Slovenia) at 1260× g for 10 min at 18 °C. The resulting supernatant, representing the autologous serum, is then carefully collected.
2.5. Outcome Measures
2.5.1. Primary Outcome Measure
2.5.2. Secondary Outcome Measures
2.6. Postoperative Period
2.7. Adverse Event Monitoring and Assessment
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PRP | Platelet-Rich Plasma |
| PRG | Platelet-Rich Gel |
| PTA | Pure Tone Audiometry |
| COMQ-12 | Chronic Otitis Media Questionnaire (12-item version) |
| EAC | External Auditory Canal |
| ET | Eustachian Tube |
| ME | Middle Ear |
| dB | Decibels |
| M | Mean |
| Mdn | Median |
| SD | Standard Deviation |
| CI | Confidence Interval |
| RCT | Randomized Controlled Trial |
| CaCl₂ | Calcium Chloride |
| COM | Chronic Otitis Media |
| JAMA | Journal of the American Medical Association |
| CONSORT | Consolidated Standards of Reporting Trials |
| USA | United States of America |
| R | R Statistical Software |
Appendix A
Appendix A.1. Inclusion and Exclusion Criteria

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| dry ear drum perforation dry middle ear cavity absence of exclusion criteria | signs of cholesteatoma anemia thrombocytopenia chronic use of immunomodulating agents and/or antimicrobial drugs the presence or condition after treatment of malignancy in the area of the ear positive current history of systemic infectious disease positive current history of autoimmune disease inability and/or refusal of the patient to participate in the research pregnancy and/or breastfeeding |
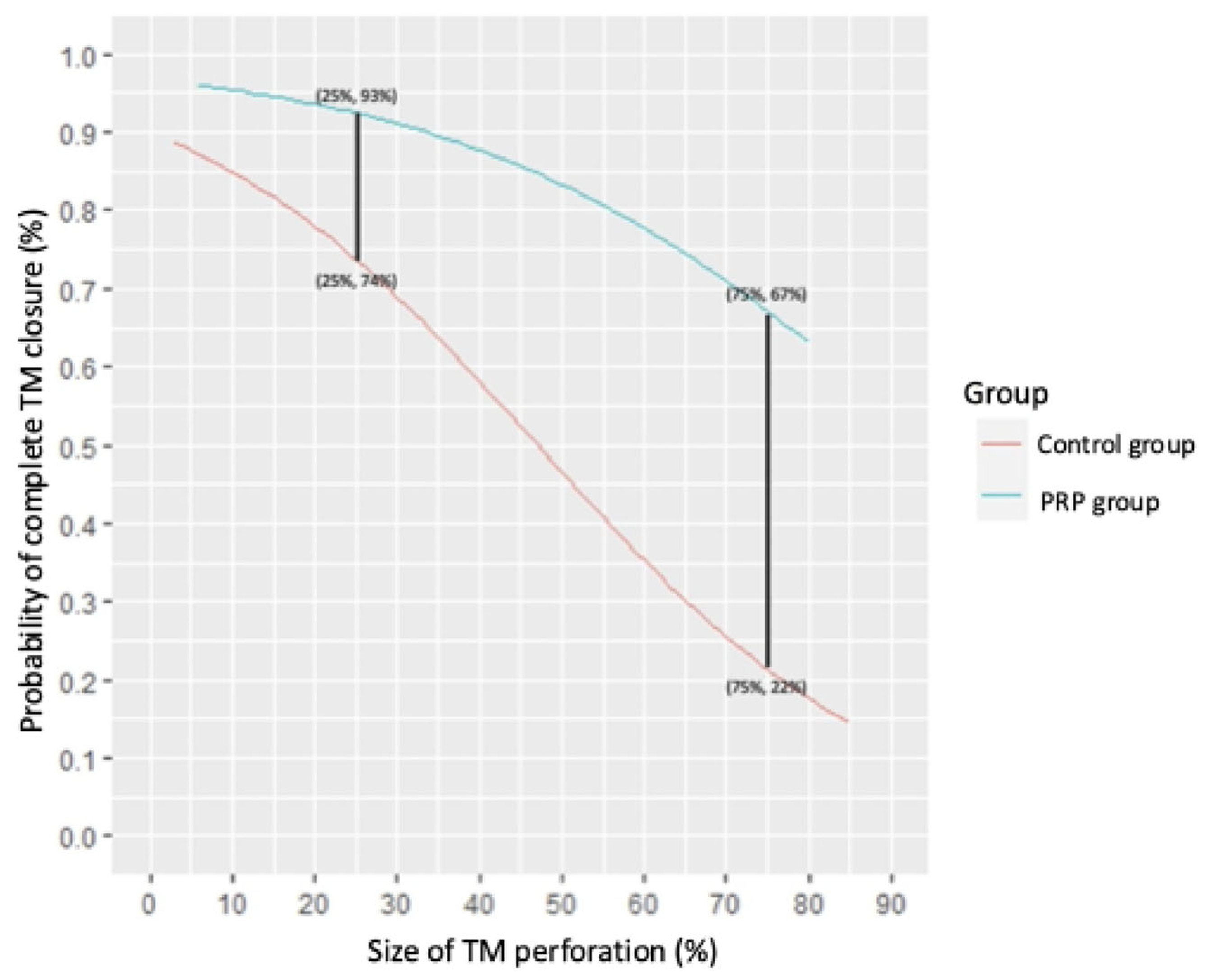
Appendix A.2. Equations for Calculating the Probability of Tympanic Membrane Healing
References
- Mohamad, S.H.; Khan, I.; Hussain, S.S.M. Is Cartilage Tympanoplasty More Effective than Fascia Tympanoplasty? A Systematic Review. Otol. Neurotol. 2012, 33, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Sheehy, J.L.; Anderson, R.G. Myringoplasty: A Review of 472 Cases. Ann. Otol. Rhinol. Laryngol. 1980, 89, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Balough, B.J. Evaluation of Prognostic Factors and Middle Ear Risk Index in Tympanoplasty. Yearb. Otolaryngol. Head. Neck Surg. 2009, 2009, 160–162. [Google Scholar] [CrossRef]
- De Seta, E.; De Seta, D.; Covelli, E.; Viccaro, M.; Filipo, R. Type I Tympanoplasty with Island Chondro-Perichondral Tragal Graft: The Preferred Technique? J. Laryngol. Otol. 2013, 127, 354–358. [Google Scholar] [CrossRef]
- De Seta, E.; Covelli, E.; De Seta, D.; Mancini, P.; Filipo, R. Cartilage Tympanoplasty: How to Reduce Surgery Time. J. Laryngol. Otol. 2010, 124, 784–785. [Google Scholar] [CrossRef]
- Dinaki, K.; Grigoriadis, N.; Vizirianakis, I.S.; Constantinidis, J.; Triaridis, S.; Karkos, P. The Impact of Submucosal PRP Injection on Wound Healing after Endoscopic Sinus Surgery: A Randomized Clinical Trial. Eur. Arch. Otorhinolaryngol. 2024, 281, 3587–3599. [Google Scholar] [CrossRef]
- Huang, J.; Shi, Y.; Wu, L.; Lv, C.; Hu, Y.; Shen, Y. Comparative Efficacy of Platelet-Rich Plasma Applied in Myringoplasty: A Systematic Review and Meta-Analysis. PLoS One 2021, 16, e0245968. [Google Scholar] [CrossRef]
- Mandour, M.F.; Elsheikh, M.N.; Amer, M.; Elzayat, S.; Barbara, M.; Covelli, E.; Elfarargy, H.H.; Tomoum, M. The Impact of Adding Platelet-Rich Plasma during Fat Graft Myringoplasty for Managing Medium-Sized Tympanic Membrane Perforations: A Prospective Randomized Case-Control Study. Am. J. Otolaryngol. 2023, 44, 103755. [Google Scholar] [CrossRef]
- Vozel, D.; Božič, D.; Jeran, M.; Jan, Z.; Pajnič, M.; Pađen, L.; Uršič, B.; Iglič, A.; Kralj-Iglič, V.; Battelino, S. Treatment with Platelet- and Extracellular Vesicle-Rich Plasma in Otorhinolaryngology-a Review and Future Perspectives. In Advances in Biomembranes and Lipid Self-Assembly; Academic Press: Cambridge, MA, USA, 2020. [Google Scholar]
- Yadav, S.P.S.; Malik, J.S.; Malik, P.; Sehgal, P.K.; Gulia, J.S.; Ranga, R.K. Studying the Result of Underlay Myringoplasty Using Platelet-Rich Plasma. J. Laryngol. Otol. 2018, 132, 990–994. [Google Scholar] [CrossRef]
- Yan, C.H.; Jang, S.S.; Lin, H.-F.C.; Ma, Y.; Khanwalkar, A.R.; Thai, A.; Patel, Z.M. Use of Platelet-Rich Plasma for COVID-19–Related Olfactory Loss: A Randomized Controlled Trial. Int. Forum Allergy Rhinol. 2023, 13, 989–997. [Google Scholar] [CrossRef]
- Bielecki, T.M.; Gazdzik, T.S.; Arendt, J.; Szczepanski, T.; Król, W.; Wielkoszynski, T. Antibacterial Effect of Autologous Platelet Gel Enriched with Growth Factors and Other Active Substances: An in Vitro Study. J. Bone Jt. Surg. Br. 2007, 89, 417–420. [Google Scholar] [CrossRef]
- Tao, S.-C.; Guo, S.-C.; Zhang, C.-Q. Platelet-Derived Extracellular Vesicles: An Emerging Therapeutic Approach. Int. J. Biol. Sci. 2017, 13, 828–834. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2000, 284, 3043–3045. [CrossRef]
- Abramson, J.H. WINPEPI Updated: Computer Programs for Epidemiologists, and Their Teaching Potential. Epidemiol. Perspect. Innov. 2011, 8, 1. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010, 7, e1000251. [Google Scholar] [CrossRef]
- Lajdam, G.B.; Alahmadi, R.A.; Alhakami, M.; Ghaddaf, A.A.; Abdulhamid, A.S.; Alahmadi, A.; Abdelsamad, Y.; Hagr, A. Comparison of Temporalis Muscle Fascia and Cartilage Grafts for Primary Type 1 Tympanoplasty: A Meta-Analysis of Randomized Controlled Trials. Eur. Arch. Otorhinolaryngol. 2023, 280, 12. [Google Scholar] [CrossRef]
- Nicholas Jungbauer, W.; Jeong, S.; Nguyen, S.A.; Lambert, P.R. Comparing Myringoplasty to Type I Tympanoplasty in Tympanic Membrane Repair: A Systematic Review and Meta-Analysis. Otolaryngol. Head. Neck Surg. 2023, 168, 922–934. [Google Scholar] [CrossRef]
- Zwierz, A.; Haber, K.; Sinkiewicz, A.; Kalińczak-Górna, P.; Tyra, J.; Mierzwiński, J. The Significance of Selected Prognostic Factors in Pediatric Tympanoplasty. Eur. Arch. Otorhinolaryngol. 2019, 276, 323–333. [Google Scholar] [CrossRef]
- Illés, K.; Gergő, D.; Keresztély, Z.; Dembrovszky, F.; Fehérvári, P.; Bánvölgyi, A.; Csupor, D.; Hegyi, P.; Horváth, T. Factors Influencing Successful Reconstruction of Tympanic Membrane Perforations: A Systematic Review and Meta-Analysis. Eur. Arch. Otorhinolaryngol. 2023, 280, 2639–2652. [Google Scholar] [CrossRef]
- Xu, N.; Wang, L.; Guan, J.; Tang, C.; He, N.; Zhang, W.; Fu, S. Wound Healing Effects of a Curcuma Zedoaria Polysaccharide with Platelet-Rich Plasma Exosomes Assembled on Chitosan/Silk Hydrogel Sponge in a Diabetic Rat Model. Int. J. Biol. Macromol. 2018, 117, 102–107. [Google Scholar] [CrossRef]
- Steiner, N.; Vozel, D.; Urbančič, J.; Božič, D.; Kralj-Iglič, V.; Battelino, S. Clinical Implementation of Platelet- and Extracellular Vesicle-Rich Product Preparation Protocols. Tissue Eng. Part. A 2022, 28, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Akash; Datta, R.; Suri, G.S.; Mucha, S.; Sheikh, M.A.; Taneja, N.S. A Randomised Controlled Trial on the Efficacy of Topical Application of Autologous Platelet Rich Plasma (PRP) on Graft Uptake Rate in Adults Undergoing Type 1 Tympanoplasty for Inactive COM Mucosal Disease. Indian. J. Otolaryngol. Head. Neck Surg. 2023, 75, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Alahmadi, R.A.; Lajdam, G.B.; Aghashami, A.; Hamdan, D.; Almalki, A.H.; Altalhi, A.A.; Amoodi, H.A. Platelet Concentrates Impact on Myringoplasty Outcomes in Chronic Otitis Media Patients: Systematic Review and Meta-Analysis. Otolaryngol. Head. Neck Surg. 2025, 172, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Parida, P.K.; Preetam, C.; Mukherjee, S.; Nayak, A.; Pradhan, P. Outcome of Temporalis Fascia Myringoplasty With and Without Use of Platelet Rich Plasma: A Randomized Control Trial. Indian. J. Otolaryngol. Head. Neck Surg. 2022, 74, 3832–3840. [Google Scholar] [CrossRef]
- Huang, J.; Teh, B.M.; Zhou, C.; Shi, Y.; Shen, Y. Tympanic Membrane Regeneration Using Platelet-Rich Fibrin: A Systematic Review and Meta-Analysis. Eur. Arch. Otorhinolaryngol. 2022, 279, 557–565. [Google Scholar] [CrossRef]
- Al-Arman, A.M.; Moneir, W.; Amer, H.E.; Ebada, H.A. Platelet Rich Fibrin Augmented Tympanoplasty versus Cartilage Tympanoplasty: A Randomized Clinical Trial. Eur. Arch. Otorhinolaryngol. 2024, 281, 5739–5746. [Google Scholar] [CrossRef]
- Navarrete Álvaro, M.L.; Ortiz, N.; Rodriguez, L.; Boemo, R.; Fuentes, J.F.; Mateo, A.; Ortiz, P. Pilot Study on the Efficiency of the Biostimulation with Autologous Plasma Rich in Platelet Growth Factors in Otorhinolaryngology: Otologic Surgery (Tympanoplasty Type I). ISRN Surg. 2011, 2011, 451020. [Google Scholar] [CrossRef]
- Choi, J.; Minn, K.W.; Chang, H. The Efficacy and Safety of Platelet-Rich Plasma and Adipose-Derived Stem Cells: An Update. Arch. Plast. Surg. 2012, 39, 585–592. [Google Scholar] [CrossRef]
- Jain, A.; Samdani, S.; Sharma, M.P.; Meena, V. Island Cartilage vs Temporalis Fascia in Type 1 Tympanoplasty: A Prospective Study. Acta Otorrinolaringol. Esp. (Engl. Ed.) 2018, 69, 311–317. [Google Scholar] [CrossRef]

| PRP Group (n = 36) | Control Group (n = 36) | p-Value | |
|---|---|---|---|
| male | 19 | 18 | 1000 * |
| female | 17 | 18 | |
| children | 3 | 5 | 0.71 * |
| Age | |||
| M ± SD [years] | 40.69 ± 18.27 | 32.42 ± 21.77 | 0.045 ** |
| Size of tympanic membrane perforation | |||
| Mdn [%] | 31 | 25.5 | 1000 ** |
| PRP Group (n = 36) | Control Group (n = 36) | p-Value | |
|---|---|---|---|
| Complete tympanic membrane closure | 32/36 (88.9%) | 24/36 (66.7%) | p < 0.05 * |
| Pure tone average | p = 0.30 ** | ||
| Air conduction Mdn—Pre op. | 39.75 | 32.50 | |
| Air conduction Mdn—Post op. | 24.50 | 18.25 | |
| Bone conduction Mdn—Post op. | 13.21 | 10.35 | |
| Bone conduction Mdn—Pre op. | 13.57 | 10.35 | |
| COMQ-12 questionnaire | p = 0.16 *** | ||
| Pre op. | 26.00 ± 10.40 | 26.02 ± 10.46 | |
| Post op. | 15.56 ± 9.03 | 15.60 ± 8.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steiner, N.; Vozel, D.; Bozanic Urbancic, N.; Troha, K.; Lazar, A.; Kralj-Iglic, V.; Battelino, S. Enhancing the Outcomes of Temporalis Fascia Tympanoplasty Using Autologous Platelet-Rich Plasma and Gel: A Randomized Controlled Trial. J. Pers. Med. 2025, 15, 233. https://doi.org/10.3390/jpm15060233
Steiner N, Vozel D, Bozanic Urbancic N, Troha K, Lazar A, Kralj-Iglic V, Battelino S. Enhancing the Outcomes of Temporalis Fascia Tympanoplasty Using Autologous Platelet-Rich Plasma and Gel: A Randomized Controlled Trial. Journal of Personalized Medicine. 2025; 15(6):233. https://doi.org/10.3390/jpm15060233
Chicago/Turabian StyleSteiner, Nejc, Domen Vozel, Nina Bozanic Urbancic, Kaja Troha, Andraz Lazar, Veronika Kralj-Iglic, and Saba Battelino. 2025. "Enhancing the Outcomes of Temporalis Fascia Tympanoplasty Using Autologous Platelet-Rich Plasma and Gel: A Randomized Controlled Trial" Journal of Personalized Medicine 15, no. 6: 233. https://doi.org/10.3390/jpm15060233
APA StyleSteiner, N., Vozel, D., Bozanic Urbancic, N., Troha, K., Lazar, A., Kralj-Iglic, V., & Battelino, S. (2025). Enhancing the Outcomes of Temporalis Fascia Tympanoplasty Using Autologous Platelet-Rich Plasma and Gel: A Randomized Controlled Trial. Journal of Personalized Medicine, 15(6), 233. https://doi.org/10.3390/jpm15060233