

A Critical Review of the Impact of SMARCA4 Mutations on Survival Outcomes in Non-Small Cell Lung Cancer



Abstract
1. Introduction
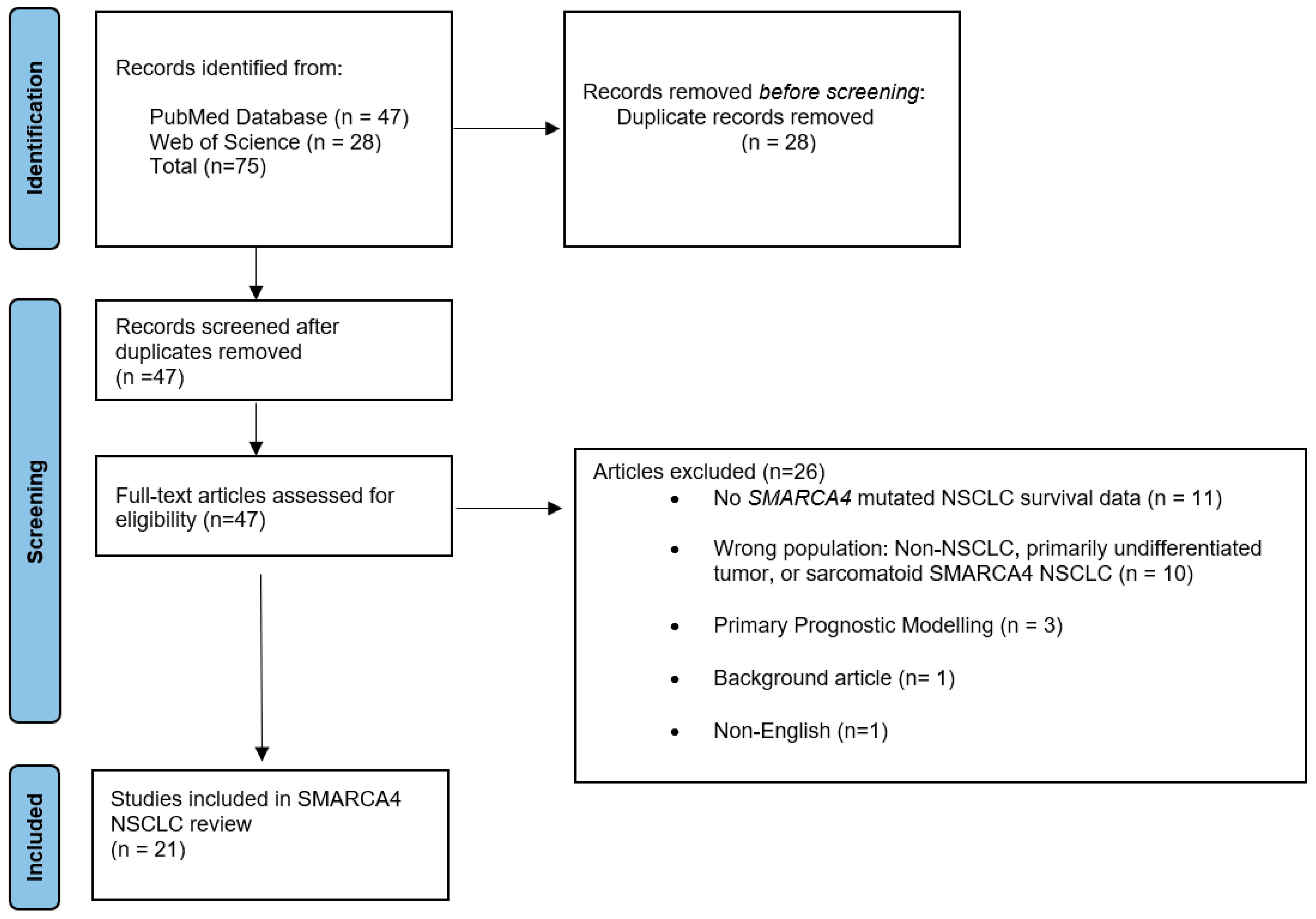
2. Materials and Methods
3. Results
3.1. Results and Description of Studies
3.2. SMARCA4 Mutations
3.3. SMARCA4/KRAS Co-Mutations
4. Discussion
4.1. SMARCA4 Molecular Sub-Types and Genomic Features
4.2. Clinicopathological Features
4.3. SMARCA4/KRAS Co-Mutations
4.4. SMARCA4/KRAS Co-Mutation Treatment Analysis
5. Future Direction
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Compilation of CDER-NME-New Biologic Approvals from 1985–2022. Available online: https://www.fda.gov/media/135308/download (accessed on 1 February 2024).
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. FLAURA Investigators Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Heymach, J.V. Co-occurring genomic alterations in non-small-cell lung cancer biology and therapy. Nat. Rev. Cancer 2019, 19, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Surveillance Epidemiology and End Results (SEER). Cancer Stat Facts: Lung and Bronchus Cancer. Available online: https://seer.cancer.gov/statfacts/html/lungb.html (accessed on 1 March 2024).
- Liang, X.; Gao, X.; Wang, F.; Li, S.; Zhou, Y.; Guo, P.; Meng, Y.; Lu, T. Clinical characteristics and prognostic analysis of SMARCA4-deficient non-small cell lung cancer. Cancer Med. 2023, 12, 14171–14182. [Google Scholar] [CrossRef] [PubMed]
- Dagogo-Jack, I.; Schrock, A.B.; Kem, M.; Jessop, N.; Lee, J.; Ali, S.M.; Ross, J.S.; Lennerz, J.K.; Shaw, A.T.; Mino-Kenudson, M.; et al. Clinicopathologic Characteristics of BRG1-Deficient NSCLC. J. Thorac. Oncol. 2020, 15, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Lamberti, G.; Spurr, L.F.; Li, Y.; Ricciuti, B.; Recondo, G.; Umeton, R.; Nishino, M.; Sholl, L.M.; Meyerson, M.L.; Cherniack, A.D.; et al. Clinicopathological and genomic correlates of programmed cell death ligand 1 (PD-L1) expression in non-squamous non-small-cell lung cancer. Ann. Oncol. 2020, 31, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, A.J.; Bandlamudi, C.; Lavery, J.A.; Montecalvo, J.; Namakydoust, A.; Rizvi, H.; Egger, J.; Concepcion, C.P.; Paul, S.; Arcila, M.E.; et al. The Genomic Landscape of SMARCA4 Alterations and Associations with Outcomes in Patients with Lung Cancer. Clin. Cancer Res. 2020, 26, 5701–5708. [Google Scholar] [CrossRef] [PubMed]
- Imielinski, M.; Berger, A.H.; Hammerman, P.S.; Hernandez, B.; Pugh, T.J.; Hodis, E.; Cho, J.; Suh, J.; Capelletti, M.; Sivachenko, A.; et al. Mapping the hallmarks of lung adenocarcinoma with massively parallel sequencing. Cell 2012, 150, 1107–1120. [Google Scholar] [CrossRef] [PubMed]
- Graziano, S.L.; Lin, D.; Elvin, J.A.; Vergilio, J.A.; Killian, J.K.; Ngo, N.; Ramkissoon, S.; Severson, E.; Hemmerich, A.; Duncan, D.; et al. SMARCA4 deficient non-small cell lung cancer (NSCLC): A comprehensive genomic profiling (CGP) study. Ann. Oncol. 2019, 30, v652–v653. [Google Scholar] [CrossRef]
- Fernando, T.M.; Piskol, R.; Bainer, R.; Sokol, E.S.; Trabucco, S.E.; Zhang, Q.; Trinh, H.; Maund, S.; Kschonsak, M.; Chaudhuri, S.; et al. Functional characterization of SMARCA4 variants identified by targeted exome-sequencing of 131,668 cancer patients. Nat. Commun. 2020, 11, 5551. [Google Scholar] [CrossRef]
- Mardinian, K.; Adashek, J.J.; Botta, G.P.; Kato, S.; Kurzrock, R. SMARCA4: Implications of an Altered Chromatin-Remodeling Gene for Cancer Development and Therapy. Mol. Cancer Ther. 2021, 20, 2341–2351. [Google Scholar] [CrossRef]
- Hodges, H.C.; Stanton, B.Z.; Cermakova, K.; Chang, C.Y.; Miller, E.L.; Kirkland, J.G.; Ku, W.L.; Veverka, V.; Zhao, K.; Crabtree, G.R. Dominant-negative SMARCA4 mutants alter the accessibility landscape of tissue-unrestricted enhancers. Nat. Struct. Mol. Biol. 2018, 25, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Armon, S.; Hofman, P.; Ilié, M. Perspectives and Issues in the Assessment of SMARCA4 Deficiency in the Management of Lung Cancer Patients. Cells 2021, 10, 1920. [Google Scholar] [CrossRef] [PubMed]
- Kadoch, C.; Hargreaves, D.C.; Hodges, C.; Elias, L.; Ho, L.; Ranish, J.; Crabtree, G.R. Proteomic and bioinformatic analysis of mammalian SWI/SNF complexes identifies extensive roles in human malignancy. Nat. Genet. 2013, 45, 592–601. [Google Scholar] [CrossRef] [PubMed]
- Orlando, K.A.; Nguyen, V.; Raab, J.R.; Walhart, T.; Weissman, B.E. Remodeling the cancer epigenome: Mutations in the SWI/SNF complex offer new therapeutic opportunities. Expert Rev. Anticancer Ther. 2019, 19, 375–391. [Google Scholar] [CrossRef] [PubMed]
- St Pierre, R.; Kadoch, C. Mammalian SWI/SNF complexes in cancer: Emerging therapeutic opportunities. Curr. Opin. Genet. Dev. 2017, 42, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Manolakos, P.; Ward, L.D. A Critical Review of the Prognostic and Predictive Implications of KRAS and STK11 Mutations and Co-Mutations in Metastatic Non-Small Lung Cancer. J. Pers. Med. 2023, 13, 1010. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Alessi, J.V.; Ricciuti, B.; Spurr, L.F.; Gupta, H.; Li, Y.Y.; Glass, C.; Nishino, M.; Cherniack, A.D.; Lindsay, J.; Sharma, B.; et al. SMARCA4 and Other SWItch/Sucrose Non Fermentable Family Genomic Alterations in NSCLC: Clinicopathologic Characteristics and Outcomes to Immune Checkpoint Inhibition. J. Thorac. Oncol. 2021, 16, 1176–1187. [Google Scholar] [CrossRef]
- Alessi, J.V.; Elkrief, A.; Ricciuti, B.; Wang, X.; Cortellini, A.; Vaz, V.R.; Lamberti, G.; Frias, R.L.; Venkatraman, D.; Fulgenzi, C.A.; et al. Clinicopathologic and Genomic Factors Impacting Efficacy of First-Line Chemoimmunotherapy in Advanced NSCLC. J. Thorac. Oncol. 2023, 18, 731–743. [Google Scholar] [CrossRef]
- Talvitie, E.M.; Liljeroos, L.; Vilhonen, H.; Orte, K.; Leivo, I.; Kallajoki, M.; Taimen, P. Comprehensive genomic profiling of Finnish lung adenocarcinoma cohort reveals high clinical actionability and SMARCA4 altered tumors with variable histology and poor prognosis. Neoplasia 2022, 32, 100832. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Chen, H.C.; Yang, L.; Yang, G.; Liang, L.; Yang, Y.; Tang, H.; Bao, H.; Wu, X.; Shao, Y.; et al. Mutational landscape of SWI/SNF complex genes reveal correlation to predictive biomarkers for immunotherapy sensitivity in lung adenocarcinoma patients. ESMO Open 2023, 8, 101585. [Google Scholar] [CrossRef] [PubMed]
- Miao, E.; Eichholz, J.E.; Lebow, E.S.; Flynn, J.; Zhang, Z.; Walch, H.; Hubbeling, H.; Beal, K.; Moss, N.S.; Yu, K.K.; et al. Characterization of Central Nervous System Clinico-Genomic Outcomes in ALK-Positive Non-Small Cell Lung Cancer Patients with Brain Metastases Treated with Alectinib. Lung Cancer 2023, 178, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.; Jiang, C.; Zhang, Z.; Achacoso, N.; Solorzano-Pinto, A.V.; Tse, P.; Chung, E.; Suga, J.M.; Thomas, S.; Habel, L.A. Sex- and Co-Mutation-Dependent Prognosis in Patients with SMARCA4-Mutated Malignancies. Cancers 2023, 15, 2665. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Shan, Q.; Guo, J.; Han, X.; Zhao, C.; Li, H.; Wang, Z. PDL1 high expression without TP53, KEAP1 and EPHA5 mutations could better predict survival for patients with NSCLC receiving atezolizumab. Lung Cancer 2021, 151, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, D.; Mazzotta, M.; Scalera, S.; Terrenato, I.; Sperati, F.; D’Ambrosio, L.; Pallocca, M.; Corleone, G.; Krasniqi, E.; Pizzuti, L.; et al. KEAP1-driven co-mutations in lung adenocarcinoma unresponsive to immunotherapy despite high tumor mutational burden. Ann. Oncol. 2020, 31, 1746–1754. [Google Scholar] [CrossRef] [PubMed]
- Velut, Y.; Decroix, E.; Blons, H.; Alifano, M.; Leroy, K.; Petitprez, F.; Boni, A.; Garinet, S.; Biton, J.; Cremer, I.; et al. SMARCA4-deficient lung carcinoma is an aggressive tumor highly infiltrated by FOXP3+ cells and neutrophils. Lung Cancer 2022, 169, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Chang, G.; Li, W.; Bai, H.; Duan, J.; Wang, Z.; Du, X.; Yu, R.; Wang, Y.; Wang, M.; Zhu, Y.; et al. Correlations of switch/sucrose nonfermentable complex mutations with clinical outcomes in advanced non-small cell lung cancer. Thorac. Cancer 2022, 13, 2951–2959. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Tang, M.; Cui, L.; Bai, J.; Yu, J.; Gao, J.; Nie, X.; Li, X.; Xia, X.; Yi, X.; et al. Prognostic and predictive impact of molecular tumor burden index in non-small cell lung cancer patients. Thorac. Cancer 2023, 14, 3097–3107. [Google Scholar] [CrossRef]
- Wang, C.X.; Yan, J.; Lin, S.; Ding, Y.; Qin, Y.R. Mutant-allele dispersion correlates with prognosis risk in patients with advanced non-small cell lung cancer. J. Cancer Res. Clin. Oncol. 2023, 149, 8545–8555. [Google Scholar] [CrossRef]
- La Fleur, L.; Falk-Sörqvist, E.; Smeds, P.; Berglund, A.; Sundström, M.; Mattsson, J.S.; Brandén, E.; Koyi, H.; Isaksson, J.; Brunnström, H.; et al. Mutation patterns in a population-based non-small cell lung cancer cohort and prognostic impact of concomitant mutations in KRAS and TP53 or STK11. Lung Cancer 2019, 130, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.J.; Muzikansky, A.; Lennerz, J.; Narinesingh, F.; Mino-Kenudson, M.; Hung, Y.P.; Piotrowska, Z.; Dagogo-Jack, I.; Sequist, L.V.; Gainor, J.F.; et al. Clinicopathologic Characteristics and Outcomes for Patients with KRAS G12D-Mutant NSCLC. JTO Clin. Res. Rep. 2022, 3, 100390. [Google Scholar] [CrossRef] [PubMed]
- Negrao, M.V.; Araujo, H.A.; Lamberti, G.; Cooper, A.J.; Akhave, N.S.; Zhou, T.; Delasos, L.; Hicks, J.K.; Aldea, M.; Minuti, G.; et al. Comutations and KRASG12C Inhibitor Efficacy in Advanced NSCLC. Cancer Discov. 2023, 13, 1556–1571. [Google Scholar] [CrossRef] [PubMed]
- Boiarsky, D.; Lydon, C.A.; Chambers, E.S.; Sholl, L.M.; Nishino, M.; Skoulidis, F.; Heymach, J.; Luo, J.; Awad, M.; Janne, P.; et al. Molecular markers of metastatic disease in KRAS-mutant lung adenocarcinoma. Ann. Oncol. 2023, 34, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Ahmed, T.; Petty, W.J.; Grant, S.; Ruiz, J.; Lycan, T.W.; Topaloglu, U.; Chou, P.; Miller, L.D.; Hawkins, G.A.; et al. SMARCA4 mutations in KRAS-mutant lung adenocarcinoma: A multi-cohort analysis. Mol. Oncol. 2021, 15, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Ricciuti, B.; Wang, X.; Alessi, J.V.; Rizvi, H.; Mahadevan, N.R.; Li, Y.Y.; Polio, A.; Lindsay, J.; Umeton, R.; Sinha, R.; et al. Association of high tumor mutation burden in non-small cell lung cancers with increased immune infiltration and improved clinical outcomes of PD-L1 blockade across PD-L1 expression levels. JAMA Oncol. 2022, 8, 1160–1168. [Google Scholar] [CrossRef] [PubMed]
- Altorki, N.K.; Markowitz, G.J.; Gao, D.; Port, J.L.; Saxena, A.; Stiles, B.; McGraw, T.; Mittal, V. The lung microenvironment: An important regulator of tumour growth and metastasis. Nat. Rev. Cancer 2019, 19, 9–31. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Wu, K.; Liu, Q.; Han, N.; Zhang, L.; Chu, Q.; Chen, Y. Modification of platinum sensitivity by KEAP1/NRF2 signals in non-small cell lung cancer. J. Hematol. Oncol. 2016, 9, 83. [Google Scholar] [CrossRef]

{kind=link}
| (A) | |||||
| Author | Publication Year | Treatment | NSCLC Mutation Analyzed | Number of NSCLC Patients with Mutation Analyzed | Outcomes/Relevance |
| Schoenfeld | 2020 | Various SOC | SMARCA4 | N = 292 mut [class 1 mut (N = 149) and class 2 (N = 143)] | In a multivariate analysis, both SMARCA4 mut class 1 and 2 had worse OS (p < 0.001) vs. WT. Class 1 mut had worse OS compared to class 2 mut or WT (p < 0.001). |
| ICI cohort | SMARCA4 | N = 87 mut | OS improvement for SMARCA4 mut with ICI treatment vs. without ICI treatment regardless of class 1 or class 2 mut status (p = 0.01). | ||
| The unadjusted ICI analysis showed no difference in PFS (p = 0.74) or OS (p = 0.35) with class 1 mut vs. class 2 mut. | |||||
| Alessi | 2023 | CIT | SMARCA4 | 114 mut | In multivariate analysis: worse OS for SMARCA4 mut vs. WT (8.1 versus 15.0 months, HR: 1.70; p < 0.001) and worse PFS: (2.7 versus 6.1 months, HR: 1.62; p < 0.001). |
| Alessi | 2021 | Various SOC | SMARCA4 | 163 mut | SMARCA4 mut had worse OS (15.6 months) vs. SMARCA4 WT (25 months) (HR: 0.64; p < 0.001). |
| ICI or ICI/CTLA4 cohort | SMARCA4 | 57 mut class 1 non-sense, frameshift, and splice site mut (N = 26) and class 2 missense mut (N = 31) | There were no significant differences in SMARCA4 WT vs. mut: PFS (3.1 vs. 2.1 months; HR = 0.93, p = 0.62) or OS (12.4 vs. 11 months; HR = 0.83, p = 0.25 months). | ||
| There was no OS difference in outcomes after receiving ICI therapy when comparing class 1 nonsense, frameshift, and splice site mut (6.7 months; p = 0.11) vs. WT patients (12.4 months) vs. class 2 missense mut (11.9 months, HR = 1.03, p = 0.87). | |||||
| Fernando | 2020 | Various SOC | SMARCA4 | SMARCA4 mut in four categories: (1) homozygous truncated (N = 102), (2) homozygous nontruncated (N = 101), (3) heterozygous truncated (N = 16), (4) heterozygous nontruncated (N = 49) | There was a significant OS difference when comparing SMARCA4 homozygous truncated mut vs. SMARCA4 WT (7.9 vs. 16.3 months, HR: 1.85; p < 0.0001), but no significant differences when comparing the other SMARCA4 mut categories with WT. |
| ICI cohort | SMARCA4 mut four categories: (1) homozygous truncated (N = 38), (2) homozygous nontruncated (N = 41), (3) heterozygous truncated (N = 5), (4) heterozygous nontruncated (N = 23) | There was a significant OS difference when comparing SMARCA4 mut homozygous truncated vs. SMARCA4 WT (9.9 vs. 19.5 months, HR: 1.62; p = 0.01), but no significant differences when comparing the other SMARCA4 mut categories with WT. | |||
| Dagogo-Jack | 2020 | Chemo or CIT | SMARCA4 | 16 mut | Extremely short PFS for chemo and CIT treatment (38 and 35 days), respectively. |
| Liang | 2023 | Various SOC | SMARCA4 | Stage III mut (N = 21), Stage IV mut (N = 69) | Median OS survival for SMARCA4 mut vs. SMARCA4 WT patients was notably lower in Stage III (23.73 vs. 29.43 months, p = <0.01) and Stage IV (11.93 vs. 28.23 months, p = <0.01). |
| SMARCA4 | 221 mut women (N = 88), men (N = 25) | Multivariate analysis resulted in statistically worse OS for women vs. men (HR = 4.1, p = 0.04). | |||
| Talvitie | 2022 | Various SOC | SMARCA4 | 135 mut | SMARCA4 mut patients had a worse OS than SMARCA4 WT (HR: 3.522; p < 0.002). |
| SMARCA4 | Stage III mut (N = 31) | Stage III multivariate analysis SMARCA4 mut patients had a worse OS vs. WT patients (HR:1.93; p = 0.04). | |||
| Xu | 2023 | Various SOC | SMARCA4 | Four Arms: (1) SMARCA4 WT, TMB Low (N = 761), (2) SMARCA4 WT, TMB High (N = 722), (3) SMARCA4 mut, TMB Low (N = 26), and (4) SMARCA4 mut, TMB High (N = 69). | Statistically better OS for SMARCA4 WT/TMB High (p = 0.00019). |
| Miao | 2023 | Alectinib (ALK) | SMARCA4/ALK | 3 mut | In a multivariate analysis, SMARCA4 mut patients with brain metastasis were the only co-mut with ALK with worse outcomes (HR: 8.76; p = 0.009). |
| Pan | 2023 | Various SOC | SMARCA4 | 44 mut: women (N = 19), men (N = 25) | Multivariate analysis with SMARCA4 mut: men had a significantly worse OS than women (2.75 months vs. un-estimable, HR:14.2; p = 0.02). |
| Wang | 2021 | Atezo (ICI) or docetaxel | SMARCA4 | 100 mut | OAK analysis: there is no statistical difference in OS when comparing atezolizumab vs. docetaxel in SMARCA4 mut, whether PDL-1 high or negative (HR = 0.67; p = 0.256). |
| SMARCA4 | 39 mut | No difference in OS with PDL-1 high vs. low when treated with atezo (HR = 1.185, p = 0.513) | |||
| Marinelli | 2020 | Atezo (ICI) | SMARCA4 | 18 mut | OAK uni-variate analysis: SMARCA4-mutated patients receiving atezo did not fare worse than SMARCA4 WT patients (HR: 1.70; p = 0.064). |
| Velut | 2022 | Nivolumab or pembro | SMARCA4 | 7 mut | SD-NSCLC patients had a shorter OS than patients with non-SD-NSCLC, considering either from the date of diagnosis (p = 0.01, HR: 2.9) or from the date of immunotherapy (p = 0.006, HR: 3.2). OS rates at 1 year were not significantly different between SMARCA4 mut and WT patients but dropped significantly at 2 (58% vs. 74%) and 5 years (37% vs. 53%). |
| Chang | 2022 | ICI (87% of patients) | SMARCA4 | 16 mut | No significant PFS difference in SMARCA4 WT vs. mut (6.3 vs. 3.9 months, HR: 0.64; p = 0.15). |
| Yang | 2023 | Various SOC | SMARCA4 | 5 mut | SMARCA4 mut patients had a worse OS compared to WT patients (4.5 months vs. 13.3 months; HR: 2.86; p = 0.031). Significantly worse PFS for SMARCA4 mut vs. WT (2.3 months vs. 8.1 months, HR: 2.80; p = 0.035). |
| Wang | 2021 | SOC | SMARCA4 | 4 mut | In multivariate analysis, SMARCA4 mut patients fared worse than SMARCA4 WT (HR = 3.098, p = 0.038) and had worse PFS (3 vs. 8 months, p = 0.007). |
| Le Fleur | 2019 | Various SOC | SMARCA4 | 21 mut | In a multivariate all-cause mortality analysis, SMARCA4 mut were independently associated with a worse OS prognosis (HR: 2.06, p = 0.003). |
| (B) | |||||
| Author | Publication Year | Treatment | NSCLC Mutations Analyzed | Number of NSCLC Patients with Mutations Analyzed | Outcomes/Relevance |
| Cooper | 2022 | Various SOC | SMARCA4/KRAS G12D co-mut | 8 co-mut | Significantly worse PFS for co-mut patients; PFS: SMARCA4/KRAS G12D mut vs. SMARCA4 WT/KRAS G12D mut (1.5 vs. 4.0 months; p = 0.0039). |
| SMARCA4 WT/KRAS G12D mut | 49 mut | No significant difference in OS: SMARCA4/KRAS G12D co-mut vs. SMARCA4 WT/KRAS G12D mut (6.1 vs. 17.3 months; p = 0.4202). | |||
| Negrao | 2023 | Sotorasib or adagrasib | SMARCA4/KRAS G12C co-mut | 20 co-mut | SMARCA4/KRAS co-mut patients had significantly worse PFS than SMARCA4 WT/KRAS mut (1.6 months vs. 5.4, HR: 3.04; p < 0.001) and had a significantly worse OS (4.9 months vs. 11.8 months, HR: 3.07; p < 0.001). |
| SMARCA4 WT/KRAS G12C | 214 mut | ||||
| Boiarsky | 2023 | Various SOC | SMARCA4/KRAS co-mut | 33 co-mut | OS was significantly worse for SMARCA4/KRAS co-mut patients with brain metastasis vs. SMARCA4 WT/KRAS-mutated (7.4 months vs. 15.0 months, HR: 2.1; p = 0.0003). |
| SMARCA4 WT/KRAS mut | 231 mut | Liver metastasis: SMARCA4/KRAS co-mut had worse outcomes vs. SMARCA4 WT/KRAS-mutated (5.2 months vs. 13.2 months, HR: 2.1; p = 0.00015). | |||
| Alessi | 2021 | CIT | SMARCA4/KRAS co-mut | 44 co-mut | Significantly worse OS (6.6 vs. 14.6 months; HR: 2.52, p < 0.001) and PFS (2.2 vs. 6.2 months; HR: 2.39, p < 0.001) in SMARCA4/KRAS co-mut vs. SMARCA4 WT/KRAS mut patients. |
| SMARCA4 WT/KRAS mut | 232 mut | ||||
| Alessi | 2023 | Single-agent ICI or ICI combined with CTLA-4 | SMARCA4/KRAS co-mut | 17 co-mut | SMARCA4/KRAS co-mut had significantly shorter PFS (1.4 vs. 4.1 months, HR: 0.25; p < 0.001) and OS (3 vs. 15.1 months, HR: 0.29; p < 0.001) compared with SMARCA4 WT/KRAS mut patients. |
| SMARCA4 WT/KRAS mut | 159 mut | The presence of a SMARCA4/KRAS co-mut may confer a worse outcome to ICIs. | |||
| Schoenfeld | 2020 | Various SOC | SMARCA4/KRAS co-mut | 110 co-mut 58 co-mut (class 1 SMARCA4) 52 co-mut (class 2 SMARCA4) | Multivariate SMARCA4/KRAS co-mut analysis resulted in worse statistical OS regardless of class 1 or 2 alterations. [Class 1: HR: 1.59, and class 2: HR: 2.75] vs. WT (p < 0.001). |
| Liu | 2021 | Various SOC | SMARCA4/KRAS co-mut | Cohort A: SMARCA4/KRAS co-mut (N = 9) vs. SMARCA4 WT/KRAS mut (N = 146) | Cohort A: SMARCA4/KRAS co-mut vs. SMARCA4 WT/KRAS mut had worse OS (15.73 vs. 19.73 months) in non-immunotherapy cohort in The Cancer Genome Atlas (TCGA) (HR: 2.32, p = 0.047). |
| SMARCA4 WT/KRAS mut | Cohort B: SMARCA4/KRAS co-mut (N = 34) vs. SMARCA4 WT/KRAS mut (N = 280) | Cohort B: SMARCA4/KRAS co-mut vs. SMARCA4 WT/KRAS mut had worse OS (5.2 vs. 6.5 months) in non-immunotherapy MSK-CT cohort (HR: 1.95, p = 0.015). | |||
| Cohort C: SMARCA4/KRAS co-mut (N = 9) vs. SMARCA4 WT/KRAS mut (N = 68) | Cohort C: SMARCA4/KRAS co-mut vs. SMARCA4 WT/KRAS mut (1.73 vs. 4.22 months) had worse PFS in immunotherapy MSK-IO cohort (HR: 2.15; p = 0.048). | ||||
| Cohort D: SMARCA4/KRAS co-mut (N = 2) vs. SMARCA4 WT/KRAS mut (N = 16) | Cohort D: SMARCA4/KRAS co-mut vs. SMARCA4 WT/KRAS mut had worse OS in immunotherapy Wake Forest cohort (HR: 11.98, p = 0.0018). | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manolakos, P.; Boccuto, L.; Ivankovic, D.S. A Critical Review of the Impact of SMARCA4 Mutations on Survival Outcomes in Non-Small Cell Lung Cancer. J. Pers. Med. 2024, 14, 684. https://doi.org/10.3390/jpm14070684
Manolakos P, Boccuto L, Ivankovic DS. A Critical Review of the Impact of SMARCA4 Mutations on Survival Outcomes in Non-Small Cell Lung Cancer. Journal of Personalized Medicine. 2024; 14(7):684. https://doi.org/10.3390/jpm14070684
Chicago/Turabian StyleManolakos, Peter, Luigi Boccuto, and Diana S. Ivankovic. 2024. "A Critical Review of the Impact of SMARCA4 Mutations on Survival Outcomes in Non-Small Cell Lung Cancer" Journal of Personalized Medicine 14, no. 7: 684. https://doi.org/10.3390/jpm14070684
APA StyleManolakos, P., Boccuto, L., & Ivankovic, D. S. (2024). A Critical Review of the Impact of SMARCA4 Mutations on Survival Outcomes in Non-Small Cell Lung Cancer. Journal of Personalized Medicine, 14(7), 684. https://doi.org/10.3390/jpm14070684