
Deterioration in Quality of Life among COVID-19 Survivors: Population-Based Cohort Study
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Source
Treatment Pattern of COVID-19
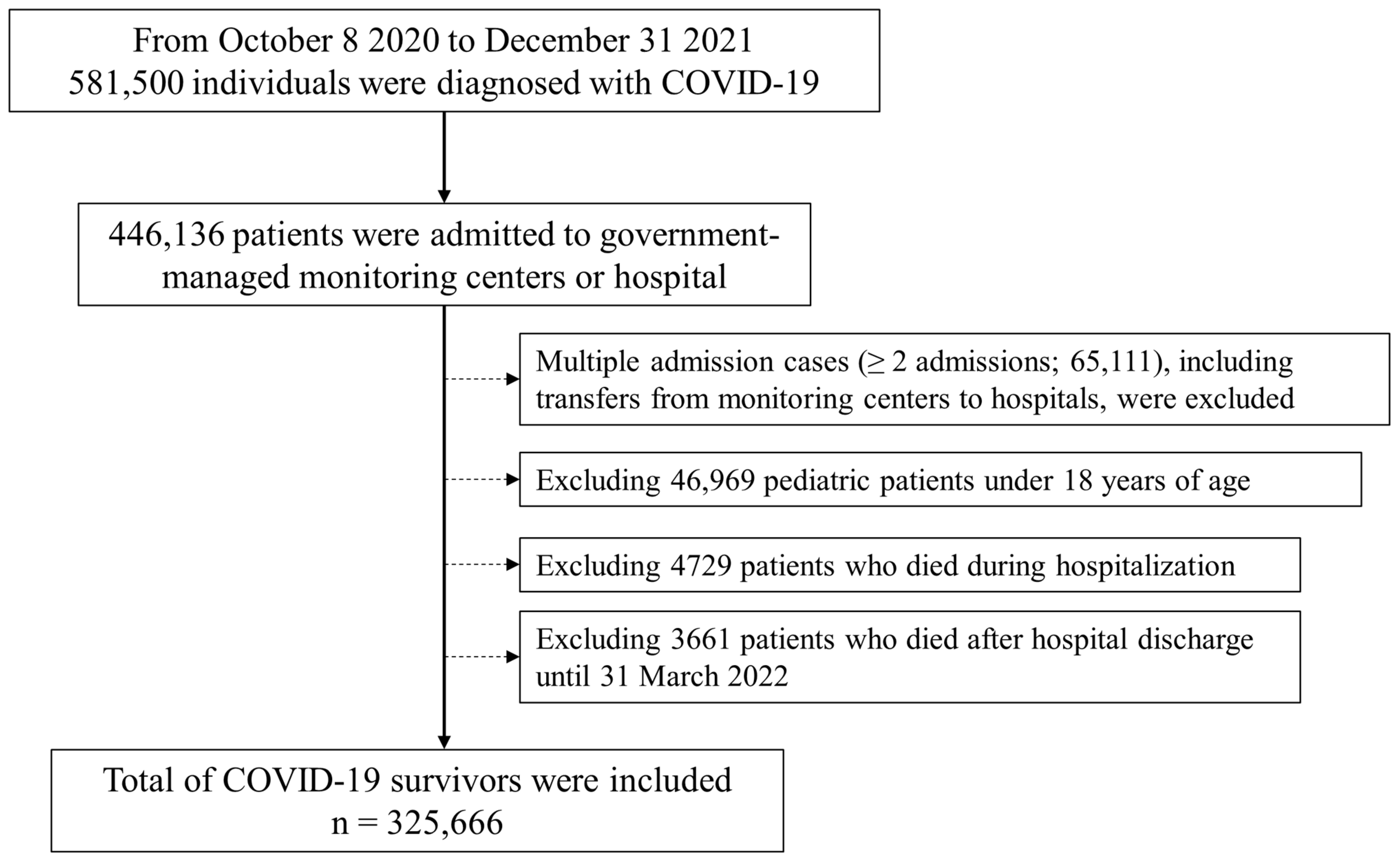
2.3. Study Population: COVID-19 Survivors
2.4. Quality of Life Assessment
2.5. Other Analyzed Variables
2.6. Statistical Analysis
3. Results
QOL Worsening
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.-d.; Sall, A.A.; et al. COVID-19: Towards controlling of a pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef] [PubMed]
- Boon-Itt, S.; Skunkan, Y. Public perception of the COVID-19 pandemic on Twitter: Sentiment analysis and topic modeling study. JMIR Public Health Surveill. 2020, 6, e21978. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernan, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Knoll, M.D.; Wonodi, C. Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef] [PubMed]
- McGowan, V.J.; Bambra, C. COVID-19 mortality and deprivation: Pandemic, syndemic, and endemic health inequalities. Lancet Public Health 2022, 7, e966–e975. [Google Scholar] [CrossRef] [PubMed]
- Bashier, H.; Ikram, A.; Khan, M.A.; Baig, M.; Al Gunaid, M.; Al Nsour, M.; Khader, Y. The anticipated future of public health services post COVID-19. JMIR Public Health Surveill. 2021, 7, e26267. [Google Scholar] [CrossRef] [PubMed]
- Espinosa-Gonzalez, A.B.; Neves, A.L.; Fiorentino, F.; Prociuk, D.; Husain, L.; Ramtale, S.C.; Mi, E.; Mi, E.; Macartney, J.; Anand, S.N. Predicting risk of hospital admission in patients with suspected COVID-19 in a community setting: Protocol for development and validation of a multivariate risk prediction tool. JMIR Res. Protoc. 2021, 10, e29072. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.N.; Pereira, L.N.; da Fé Brás, M.; Ilchuk, K. Quality of life under the COVID-19 quarantine. Qual. Life Res. 2021, 30, 1389–1405. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.; Townsend, L.; Dowds, J.; Bannan, C.; Nadarajan, P.; Kent, B.; Murphy, N.; Sheill, G.; Martin-Loeches, I.; Guinan, E. 1-year quality of life and health-outcomes in patients hospitalised with COVID-19: A longitudinal cohort study. Respir. Res. 2022, 23, 115. [Google Scholar] [CrossRef]
- Sheehy, L.M. Considerations for postacute rehabilitation for survivors of COVID-19. JMIR Public Health Surveill. 2020, 6, e19462. [Google Scholar] [CrossRef]
- Nandasena, H.; Pathirathna, M.L.; Atapattu, A.; Prasanga, P.T.S. Quality of life of COVID 19 patients after discharge: Systematic review. PLoS ONE 2022, 17, e0263941. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Si, T.L.; Chen, P.; Wang, Y.-Y.; Su, Z.; Cheung, T.; Jackson, T.; Xiang, Y.-T.; Feng, Y. Prevalence of COVID-19 fear and its association with quality of life among fire service recruits after ceasing the dynamic zero-COVID policy in China. Front. Public Health 2023, 11, 1257943. [Google Scholar] [CrossRef] [PubMed]
- McFann, K.; Baxter, B.A.; LaVergne, S.M.; Stromberg, S.; Berry, K.; Tipton, M.; Haberman, J.; Ladd, J.; Webb, T.L.; Dunn, J.A. Quality of life (QoL) is reduced in those with severe COVID-19 disease, post-acute sequelae of COVID-19, and hospitalization in United States adults from northern Colorado. Int. J. Environ. Res. Public Health 2021, 18, 11048. [Google Scholar] [CrossRef] [PubMed]
- Lachat, C.; Hawwash, D.; Ocke, M.C.; Berg, C.; Forsum, E.; Hornell, A.; Larsson, C.; Sonestedt, E.; Wirfalt, E.; Akesson, A.; et al. Strengthening the Reporting of Observational Studies in Epidemiology-Nutritional Epidemiology (STROBE-nut): An Extension of the STROBE Statement. PLoS Med. 2016, 13, e1002036. [Google Scholar] [CrossRef] [PubMed]
- Petrosky-Nadeau, N.; Valletta, R.G. An unemployment crisis after the onset of COVID-19. FRBSF Econ. Lett. 2020, 12, 1–5. [Google Scholar]
- VanderWeele, T.J. Challenges estimating total lives lost in COVID-19 decisions: Consideration of mortality related to unemployment, social isolation, and depression. JAMA 2020, 324, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Pompili, M.; Innamorati, M.; Sampogna, G.; Albert, U.; Carmassi, C.; Carra, G.; Cirulli, F.; Erbuto, D.; Luciano, M.; Nanni, M.G.; et al. The impact of Covid-19 on unemployment across Italy: Consequences for those affected by psychiatric conditions. J. Affect. Disord. 2022, 296, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Fan, W. Who loses income during the COVID-19 outbreak? Evidence from China. Res. Soc. Stratif. Mobil. 2020, 68, 100522. [Google Scholar] [CrossRef]
- Hadi, A.A.; Nidzam, N.N.S.; Hamid, M.A.H.; Razali, N.M. COVID-19 Pandemic and Its Effects on Household Income in Malaysia During Lockdown. J. Stat. Model. Anal. (JOSMA) 2022, 4, 43–55. [Google Scholar]
- Sedgwick, P. Questionnaire surveys: Sources of bias. BMJ 2013, 347, f5265. [Google Scholar] [CrossRef]
- de Oliveira Almeida, K.; Nogueira Alves, I.G.; de Queiroz, R.S.; de Castro, M.R.; Gomes, V.A.; Santos Fontoura, F.C.; Brites, C.; Neto, M.G. A systematic review on physical function, activities of daily living and health-related quality of life in COVID-19 survivors. Chronic Illn. 2022, 19, 279–303. [Google Scholar] [CrossRef] [PubMed]
- Gaur, R.; Asthana, S.; Yadav, R.; Ghuleliya, R.; Kumar, D.; Akhtar, M.; Gonnade, N.; Choudhary, A.; Mathew, M.M.; Gaur, N. Assessment of physical disability after three months in patients recovered from COVID-19: A cross-sectional study. Cureus 2022, 14, e21618. [Google Scholar] [CrossRef] [PubMed]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924–944. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043–2054. [Google Scholar] [CrossRef] [PubMed]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D. Clinical severity of, and effectiveness of mRNA vaccines against, COVID-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: Prospective observational study. BMJ 2022, 376, e069761. [Google Scholar] [CrossRef]
- Murillo-Zamora, E.; Guzmán-Esquivel, J.; Bricio-Barrios, J.A.; Mendoza-Cano, O. Comparing the survival of adult inpatients with COVID-19 during the wild-type, Delta, and Omicron emergence. Public Health 2022, 213, 124–126. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Mean (SD) | N (%) | |
|---|---|---|---|
| Age | 49.1 (17.9) | ||
| Male sex | 166,073 (51.0) | ||
| Residence | |||
| Urban area | 161,849 (49.7) | ||
| Rural area | 163,817 (50.3) | ||
| Infection route | |||
| Domestic | 320,386 (98.4) | ||
| Foreign | 5280 (1.6) | ||
| Cause type | |||
| Inflow from foreign countries | 5280 (1.6) | ||
| Contact with person-related inflow from foreign countries | 143 (0.0) | ||
| Outbreak in hospitals or nursing care centers | 16,377 (5.0) | ||
| Outbreak in local communities | 69,442 (21.3) | ||
| Contact with a COVID-19 confirmed patient | 134,191 (41.2) | ||
| Unknown | 100,233 (30.8) | ||
| CCI, point | 2.6 (2.6) | ||
| LOS, day | 10.0 (4.1) | ||
| Receipt of surgery during hospitalization | 1295 (0.4) | ||
| Type of hospital | |||
| Tertiary general hospital | 33,074 (10.2) | ||
| General hospital | 283,556 (87.1) | ||
| Long-term facility care center | 9036 (2.8) | ||
| 1st vaccination | 287,804 (88.4) | ||
| 2nd vaccination | 271,179 (83.3) | ||
| ICU admission | 4930 (1.5) | ||
| Nasal or mask oxygen therapy | 28,584 (8.8) | ||
| Mechanical ventilator support | 528 (0.2) | ||
| ECMO support | 50 (0.0) | ||
| Experience of CPR | |||
| CRRT use | 6 (0.0) | ||
| Total cost for hospitalization in USD | 1483.2 (2435.8) | ||
| Self-payment in USD | 222.3 (383.6) | ||
| Total QOL worsening group | 106,091 (32.6) | ||
| Unemployment group | 21,223 (6.5) | ||
| Decreased household income group | 94,556 (29.0) | ||
| Newly acquired disability group | 559 (0.2) | ||
| Variable | QOL Worsening Group n = 106,091 | No QOL Worsening Group n = 219,575 | p-Value | |
|---|---|---|---|---|
| Age, year | 48.7 (17.8) | 49.2 (17.9) | <0.001 | |
| Male sex | 54,335 (51.2) | 111,738 (50.9) | 0.08 | |
| Residence | 0.009 | |||
| Urban area | 52,374 (49.4) | 109,475 (49.9) | ||
| Rural area | 53,717 (50.6) | 110,100 (50.1) | ||
| Infection route | ||||
| Domestic | 104,384 (98.4) | 216,002 (98.4) | ||
| Foreign | 1707 (1.6) | 3573 (1.6) | 0.70 | |
| Cause type | <0.001 | |||
| Inflow from foreign countries | 1707 (1.6) | 3573 (1.6) | ||
| Contact with person-related inflow from foreign countries | 45 (0.0) | 98 (0.0) | ||
| Outbreak in hospitals or nursing care centers | 4609 (4.3) | 11,768 (5.4) | ||
| Outbreak in local communities | 22,473 (21.2) | 46,969 (21.4) | ||
| Contact with a COVID-19 confirmed patient | 44,061 (41.5) | 90,130 (41.0) | ||
| Unknown | 33,196 (31.3) | 67,037 (30.5) | ||
| CCI, point | 2.5 (2.6) | 2.6 (2.6) | <0.001 | |
| LOS, day | 9.9 (4.1) | 10.0 (4.2) | 0.002 | |
| Receipt of surgery during hospitalization | 448 (0.4) | 847 (0.4) | 0.12 | |
| Type of hospital | <0.001 | |||
| Tertiary general hospital | 10,867 (10.2) | 22,207 (10.1) | ||
| General hospital | 92,504 (87.2) | 191,052 (87.0) | ||
| Long-term facility care center | 2720 (2.6) | 6316 (2.9) | ||
| 1st vaccination | 93,213 (87.9) | 194,591 (88.6) | <0.001 | |
| 2nd vaccination | 88,068 (83.0) | 183,111 (83.4) | 0.006 | |
| ICU admission | 1690 (1.6) | 3240 (1.5) | 0.01 | |
| Nasal or mask oxygen therapy | 9353 (8.8) | 19,231 (8.8) | 0.21 | |
| Mechanical ventilator support | 192 (0.2) | 336 (0.2) | 0.06 | |
| ECMO support | 20 (0.0) | 30 (0.0) | 0.26 | |
| Experience of CPR | 3 (0.0) | 9 (0.0) | 0.12 | |
| CRRT use | 3 (0.0) | 3 (0.0) | 0.75 | |
| Self-payment, 100 USD | 230.2 (413.5) | 218.5 (368.2) | <0.001 | |
| Variable | In the Year When They Were Diagnosed with COVID-19 | 31 March 2022 (Last Follow-Up Date) | |
|---|---|---|---|
| Having a job * | 215,894 (66.3) | 212,324 (65.2) | |
| Household income level group | |||
| Medical aid group | 11,275 (3.5) | 11,830 (3.6) | |
| Q1 (lowest) | 63,196 (19.4) | 67,256 (20.7) | |
| Q2 | 72,596 (22.3) | 66,558 (20.4) | |
| Q3 | 78,106 (24.0) | 78,514 (24.1) | |
| Q4 (highest) | 95,203 (29.2) | 95,169 (29.2) | |
| Unknown | 5290 (1.6) | 6339 (1.9) | |
| Disability ** | |||
| Mild to moderate | 12,117 (3.7) | 12,358 (3.8) | |
| Severe | 7355 (2.3) | 7624 (2.3) | |
| Variable | OR (95% CI) | p-Value | |
|---|---|---|---|
| Age, 10 years | 0.99 (0.98, 0.99) | <0.001 | |
| Male sex | 1.00 (0.99, 1.02) | 0.68 | |
| Residence | |||
| Urban area | 1 | ||
| Rural area | 1.02 (1.01, 1.04) | 0.009 | |
| Infection route | |||
| Domestic | 1 | ||
| Foreign | 0.96 (0.90, 1.02) | 0.17 | |
| Cause type | |||
| Inflow from foreign countries | 1 | ||
| Contact with person-related inflow from foreign countries | 0.00 (0.00-) | ||
| Outbreak in hospitals or nursing care centers | 0.93 (0.65, 1.32) | 0.68 | |
| Outbreak in local communities | 0.82 (0.79, 0.85) | <0.001 | |
| Contact with a COVID-19 confirmed patient | 0.97 (0.95, 0.99) | 0.002 | |
| Unknown | 0.99 (0.97, 1.01) | 0.31 | |
| CCI, point | 1.00 (1.00, 1.00) | 0.52 | |
| LOS, day | 0.99 (0.99, 1.00) | 0.11 | |
| Receipt of surgery during hospitalization | 1.01 (0.99, 1.02) | 0.37 | |
| Type of hospital | |||
| Tertiary general hospital | 1 | ||
| General hospital | 1.00 (0.98, 1.03) | 0.83 | |
| Long-term facility care center | 0.95 (0.90, 1.00) | 0.04 | |
| 1st vaccination | 0.89 (0.86, 0.93) | <0.001 | |
| 2nd vaccination | 0.95 (0.93, 0.96) | <0.001 | |
| ICU admission | 1.08 (1.02, 1.15) | 0.03 | |
| Nasal or mask oxygen therapy | 1.02 (0.99, 1.05) | 0.30 | |
| Mechanical ventilator support | 1.06 (0.86, 1.31) | 0.58 | |
| ECMO support | 1.11 (0.61, 2.03) | 0.74 | |
| Experience of CPR | 0.60 (0.16, 2.25) | 0.45 | |
| CRRT use | 1.65 (0.32, 8.41) | 0.55 | |
| Self-payment, 100 USD | 1.02 (1.02, 1.02) | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, T.K.; Song, I.-A. Deterioration in Quality of Life among COVID-19 Survivors: Population-Based Cohort Study. J. Pers. Med. 2024, 14, 569. https://doi.org/10.3390/jpm14060569
Oh TK, Song I-A. Deterioration in Quality of Life among COVID-19 Survivors: Population-Based Cohort Study. Journal of Personalized Medicine. 2024; 14(6):569. https://doi.org/10.3390/jpm14060569
Chicago/Turabian StyleOh, Tak Kyu, and In-Ae Song. 2024. "Deterioration in Quality of Life among COVID-19 Survivors: Population-Based Cohort Study" Journal of Personalized Medicine 14, no. 6: 569. https://doi.org/10.3390/jpm14060569
APA StyleOh, T. K., & Song, I.-A. (2024). Deterioration in Quality of Life among COVID-19 Survivors: Population-Based Cohort Study. Journal of Personalized Medicine, 14(6), 569. https://doi.org/10.3390/jpm14060569