
Prognostic Value of Lymph Node Ratio in Patients with Uterine Carcinosarcoma

 ,
,  , , , , , ,
, , , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mbatani, N.; Olawaiye, A.B.; Prat, J. Uterine sarcomas. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. S2), 51–58. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.H.; Broaddus, R.R. Endometrial Cancer. N. Engl. J. Med. 2020, 383, 2053–2064. [Google Scholar] [CrossRef] [PubMed]
- Raffone, A.; Travaglino, A.; Raimondo, D.; Maletta, M.; De Vivo, V.; Visiello, U.; Casadio, P.; Seracchioli, R.; Zullo, F.; Insabato, L.; et al. Uterine carcinosarcoma vs endometrial serous and clear cell carcinoma: A systematic review and meta-analysis of survival. Int. J. Gynaecol. Obstet. 2022, 158, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Takazawa, Y.; Ross, M.S.; Elishaev, E.; Podzielinski, I.; Yunokawa, M.; Sheridan, T.B.; Bush, S.H.; Klobocista, M.M.; Blake, E.A.; et al. Significance of histologic pattern of carcinoma and sarcoma components on survival outcomes of uterine carcinosarcoma. Ann. Oncol. 2016, 27, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Sertier, A.S.; Ferrari, A.; Pommier, R.M.; Treilleux, I.; Boyault, S.; Devouassoux-Shisheboran, M.; Kielbassa, J.; Thomas, E.; Tonon, L.; Le Texier, V.; et al. Dissecting the Origin of Heterogeneity in Uterine and Ovarian Carcinosarcomas. Cancer Res. Commun. 2023, 3, 830–841. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kang, G.H.; Kim, H. Prognostic significance of heterologous component in carcinosarcoma of the gynecologic organs: A systematic review and meta-analysis. J. Gynecol. Oncol. 2023, 34, e73. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Ray-Coquard, I.; Concin, N.; Ngoi, N.Y.L.; Morice, P.; Caruso, G.; Enomoto, T.; Takehara, K.; Denys, H.; Lorusso, D.; et al. Endometrial carcinosarcoma. Int. J. Gynecol. Cancer 2023, 33, 147–174. [Google Scholar] [CrossRef]
- Abu-Rustum, N.; Yashar, C.; Arend, R.; Barber, E.; Bradley, K.; Brooks, R.; Campos, S.M.; Chino, J.; Chon, H.S.; Chu, C.; et al. Uterine Neoplasms, Version 1.2023, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2023, 21, 181–209. [Google Scholar] [CrossRef]
- Amant, F.; Mirza, M.R.; Koskas, M.; Creutzberg, C.L. Cancer of the corpus uteri. Int. J. Gynaecol. Obstet. 2018, 143 (Suppl. S2), 37–50. [Google Scholar] [CrossRef]
- Koskas, M.; Amant, F.; Mirza, M.R.; Creutzberg, C.L. Cancer of the corpus uteri: 2021 update. Int. J. Gynaecol. Obstet. 2021, 155 (Suppl. S1), 45–60. [Google Scholar] [CrossRef] [PubMed]
- van der Horst, R.L.; van der Hel, O.; Lutgens, L.; van der Aa, M.; Slangen, B.; Kruitwagen, R.; Lalisang, R.I. The role of multimodal adjuvant therapy for FIGO I-II carcinosarcoma of the uterus: A systematic review. Crit. Rev. Oncol. Hematol. 2022, 175, 103701. [Google Scholar] [CrossRef] [PubMed]
- Rauh-Hain, J.A.; Starbuck, K.D.; Meyer, L.A.; Clemmer, J.; Schorge, J.O.; Lu, K.H.; Del Carmen, M.G. Patterns of care, predictors and outcomes of chemotherapy for uterine carcinosarcoma: A National Cancer Database analysis. Gynecol. Oncol. 2015, 139, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Harano, K.; Hirakawa, A.; Yunokawa, M.; Nakamura, T.; Satoh, T.; Nishikawa, T.; Aoki, D.; Ito, K.; Ito, K.; Nakanishi, T.; et al. Prognostic factors in patients with uterine carcinosarcoma: A multi-institutional retrospective study from the Japanese Gynecologic Oncology Group. Int. J. Clin. Oncol. 2016, 21, 168–176. [Google Scholar] [CrossRef]
- Polterauer, S.; Schwameis, R.; Grimm, C.; Hillemanns, P.; Jückstock, J.; Hilpert, F.; de Gregorio, N.; Hasenburg, A.; Sehouli, J.; Fürst, S.T.; et al. Lymph node ratio in inguinal lymphadenectomy for squamous cell vulvar cancer: Results from the AGO-CaRE-1 study. Gynecol. Oncol. 2019, 153, 286–291. [Google Scholar] [CrossRef]
- Cui, H.; Huang, Y.; Wen, W.; Li, X.; Xu, D.; Liu, L. Prognostic value of lymph node ratio in cervical cancer: A meta-analysis. Medicine 2022, 101, e30745. [Google Scholar] [CrossRef]
- Hai, J.; Feng, L.; Yang, J.; Niu, X.; Jiang, H. The prognostic value of the lymph node ratio in patients with stage IIIC ovarian cancer treated with preoperative chemotherapy. Ann. Palliat. Med. 2021, 10, 11504–11511. [Google Scholar] [CrossRef]
- Polterauer, S.; Grimm, C.; Hofstetter, G.; Concin, N.; Natter, C.; Sturdza, A.; Pötter, R.; Marth, C.; Reinthaller, A.; Heinze, G. Nomogram prediction for overall survival of patients diagnosed with cervical cancer. Br. J. Cancer 2012, 107, 918–924. [Google Scholar] [CrossRef]
- Chan, J.K.; Kapp, D.S.; Cheung, M.K.; Osann, K.; Shin, J.Y.; Cohn, D.; Seid, P.L. The impact of the absolute number and ratio of positive lymph nodes on survival of endometrioid uterine cancer patients. Br. J. Cancer 2007, 97, 605–611. [Google Scholar] [CrossRef]
- Gao, L.; Lyu, J.; Luo, X.; Zhang, D.; Jiang, G.; Zhang, X.; Gao, X.; Zheng, S.; Wang, X.; Shen, Y. Nomogram to predict overall survival based on the log odds of positive lymph nodes for patients with endometrial carcinosarcoma after surgery. BMC Cancer 2021, 21, 1149. [Google Scholar] [CrossRef]
- Pecorelli, S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int. J. Gynaecol. Obstet. 2009, 105, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Zapardiel, I.; Morrow, C.P. New terminology for cytoreduction in advanced ovarian cancer. Lancet Oncol. 2011, 12, 214. [Google Scholar] [CrossRef] [PubMed]
- Kunos, C.; Simpkins, F.; Gibbons, H.; Tian, C.; Homesley, H. Radiation therapy compared with pelvic node resection for node-positive vulvar cancer: A randomized controlled trial. Obstet. Gynecol. 2009, 114, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Desai, N.B.; Kollmeier, M.A.; Makker, V.; Levine, D.A.; Abu-Rustum, N.R.; Alektiar, K.M. Comparison of outcomes in early stage uterine carcinosarcoma and uterine serous carcinoma. Gynecol. Oncol. 2014, 135, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Polterauer, S.; Khalil, S.; Zivanovic, O.; Abu-Rustum, N.R.; Hofstetter, G.; Concin, N.; Grimm, C.; Reinthaller, A.; Barakat, R.R.; Leitao, M.M., Jr. Prognostic value of lymph node ratio and clinicopathologic parameters in patients diagnosed with stage IIIC endometrial cancer. Obstet. Gynecol. 2012, 119, 1210–1218. [Google Scholar] [CrossRef]
- Gracia, M.; Yildirim, Y.; Macuks, R.; Mancari, R.; Achimas-Cadariu, P.; Polterauer, S.; Iacoponi, S.; Zapardiel, I. Influence of Clinical and Surgical Factors on Uterine Carcinosarcoma Survival. Cancers 2023, 15, 1463. [Google Scholar] [CrossRef]
- Polterauer, S.; Hefler, L.; Seebacher, V.; Rahhal, J.; Tempfer, C.; Horvat, R.; Reinthaller, A.; Grimm, C. The impact of lymph node density on survival of cervical cancer patients. Br. J. Cancer 2010, 103, 613–616. [Google Scholar] [CrossRef]
- Zhou, J.; Chen, Q.H.; Wu, S.G.; He, Z.Y.; Sun, J.Y.; Li, F.Y.; Lin, H.X.; You, K.L. Lymph node ratio may predict the benefit of postoperative radiotherapy in node-positive cervical cancer. Oncotarget 2016, 7, 29420–29428. [Google Scholar] [CrossRef]
- Polterauer, S.; Schwameis, R.; Grimm, C.; Macuks, R.; Iacoponi, S.; Zalewski, K.; Zapardiel, I. Prognostic value of lymph node ratio and number of positive inguinal nodes in patients with vulvar cancer. Gynecol. Oncol. 2017, 147, 92–97. [Google Scholar] [CrossRef]
- Wu, S.G.; Zhang, W.W.; Li, F.Y.; Sun, J.Y.; Zhou, J.; He, Z.Y. Lymph node ratio has prognostic value related to the number of positive lymph nodes in patients with vulvar cancer. Future Oncol. 2018, 14, 2343–2351. [Google Scholar] [CrossRef]
- Gorzelnik, K.; Szubert, S.; Knafel, A.; Wójcikiewicz, A.; Nowakowski, B.; Koper, K.; Wicherek, Ł. An analysis of the significance of the lymph node ratio and extracapsular involvement in the prognosis of endometrial cancer patients. Contemp. Oncol./Współczesna Onkol. 2022, 26, 144–149. [Google Scholar] [CrossRef] [PubMed]
- de Jong, R.A.; Nijman, H.W.; Wijbrandi, T.F.; Reyners, A.K.; Boezen, H.M.; Hollema, H. Molecular markers and clinical behavior of uterine carcinosarcomas: Focus on the epithelial tumor component. Mod. Pathol. 2011, 24, 1368–1379. [Google Scholar] [CrossRef] [PubMed]
- Zammarrelli, W.A., 3rd; Greenman, M.; Rios-Doria, E.; Miller, K.; Broach, V.; Mueller, J.J.; Aviki, E.; Alektiar, K.M.; Soslow, R.A.; Ellenson, L.H.; et al. Sentinel lymph node biopsy alone compared to systematic lymphadenectomy in patients with uterine carcinosarcoma. Gynecol. Oncol. 2022, 165, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Leong, S.P.; Naxerova, K.; Keller, L.; Pantel, K.; Witte, M. Molecular mechanisms of cancer metastasis via the lymphatic versus the blood vessels. Clin. Exp. Metastasis 2022, 39, 159–179. [Google Scholar] [CrossRef] [PubMed]
- Chapman, B.; Paquette, C.; Tooke, C.; Schwartz, M.; Osler, T.; Weaver, D.; Wilcox, R.; Hyman, N. Impact of Schwartz enhanced visualization solution on staging colorectal cancer and clinicopathological features associated with lymph node count. Dis. Colon. Rectum 2013, 56, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Lanowska, M.; Vasiljeva, J.; Chiantera, V.; Marnitz, S.; Schneider, A.; Rudolph, B.; Köhler, C. Implication of the examining pathologist to meet the oncologic standard of lymph node count after laparoscopic lymphadenectomy. Oncology 2010, 79, 161–167. [Google Scholar] [CrossRef]
- Sherbeck, J.P.; Zhao, L.; Lieberman, R.W. High Variability in Lymph Node Counts Among an International Cohort of Pathologists: Questioning the Scientific Validity of Node Counts. J. Natl. Compr. Cancer Netw. 2018, 16, 395–401. [Google Scholar] [CrossRef]
- Parkash, V.; Bifulco, C.; Feinn, R.; Concato, J.; Jain, D. To count and how to count, that is the question: Interobserver and intraobserver variability among pathologists in lymph node counting. Am. J. Clin. Pathol. 2010, 134, 42–49. [Google Scholar] [CrossRef]
- Ahmadi, O.; McCall, J.L.; Stringer, M.D. Does senescence affect lymph node number and morphology? A systematic review. ANZ J. Surg. 2013, 83, 612–618. [Google Scholar] [CrossRef]
- Cakala-Jakimowicz, M.; Kolodziej-Wojnar, P.; Puzianowska-Kuznicka, M. Aging-Related Cellular, Structural and Functional Changes in the Lymph Nodes: A Significant Component of Immunosenescence? An Overview. Cells 2021, 10, 3148. [Google Scholar] [CrossRef]
- Garg, G.; Yee, C.; Schwartz, K.; Mutch, D.G.; Morris, R.T.; Powell, M.A. Patterns of care, predictors, and outcomes of chemotherapy in elderly women with early-stage uterine carcinosarcoma: A population-based analysis. Gynecol. Oncol. 2014, 133, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Gungorduk, K.; Ozdemir, A.; Ertas, I.E.; Gokcu, M.; Telli, E.; Oge, T.; Sahbaz, A.; Sayhan, S.; Sanci, M.; Harma, M.; et al. Adjuvant treatment modalities, prognostic predictors and outcomes of uterine carcinosarcomas. Cancer Res. Treat. 2015, 47, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Rockall, A.G.; Sohaib, S.A.; Harisinghani, M.G.; Babar, S.A.; Singh, N.; Jeyarajah, A.R.; Oram, D.H.; Jacobs, I.J.; Shepherd, J.H.; Reznek, R.H. Diagnostic performance of nanoparticle-enhanced magnetic resonance imaging in the diagnosis of lymph node metastases in patients with endometrial and cervical cancer. J. Clin. Oncol. 2005, 23, 2813–2821. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Distribution |
|---|---|
| Age (years), mean (SD) | 65 (8.9) |
| Menopause | 81 (87.1%) |
| Symptoms | |
| Pain | 4 (4.3%) |
| Pelvic mass | 4 (4.3%) |
| Bleeding | 78 (83.9%) |
| Other | 7 (7.5%) |
| FIGO Stage | |
| I | 58 (62.4%) |
| II | 3 (3.2%) |
| III | 25 (26.9%) |
| IV | 7 (7.5%) |
| Route of Surgery | |
| Laparoscopy | 4 (4.3%) |
| Laparotomy | 89 (95.7%) |
| Lymphadenectomy | |
| Pelvic only | 53 (57%) |
| Para-aortic only | 12 (12.9%) |
| Both | 28 (30.1%) |
| Residual disease | |
| Complete resection | 71 (76.3%) |
| Minimal residual disease (<1 cm) | 4 (4.3%) |
| Gross residual disease (>1 cm) | 2 (2.2%) |
| Not available | 16 (17.2%) |
| Lymph node positivity | |
| Pelvic only | 17 (18.3%) |
| Para-aortic only | 3 (3.2%) |
| Both | 4 (4.3%) |
| Lymph node count | |
| Pelvic, mean (SD) | 15 (13.4) |
| Para-aortic, mean (SD) | 8.2 (6.5) |
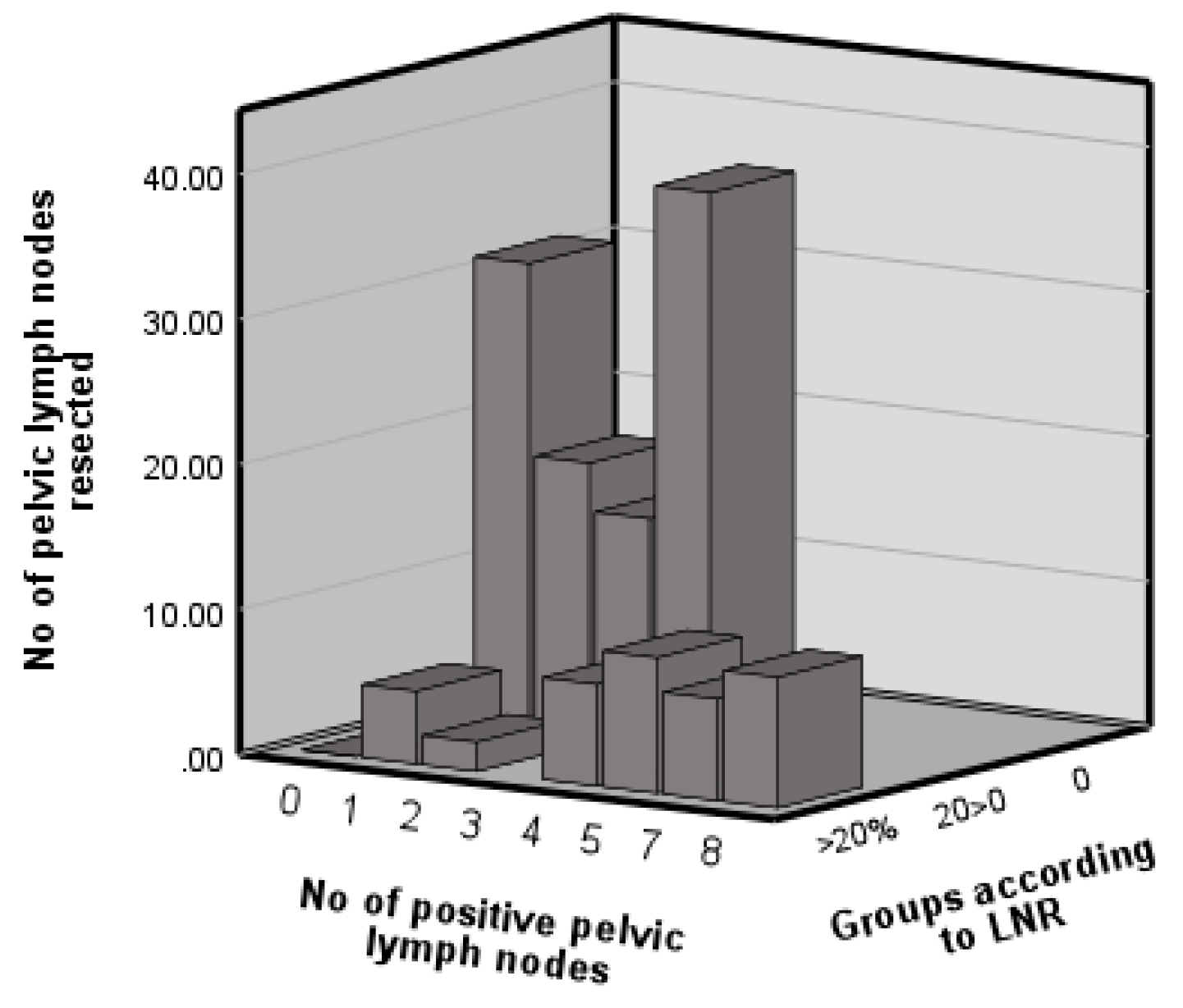
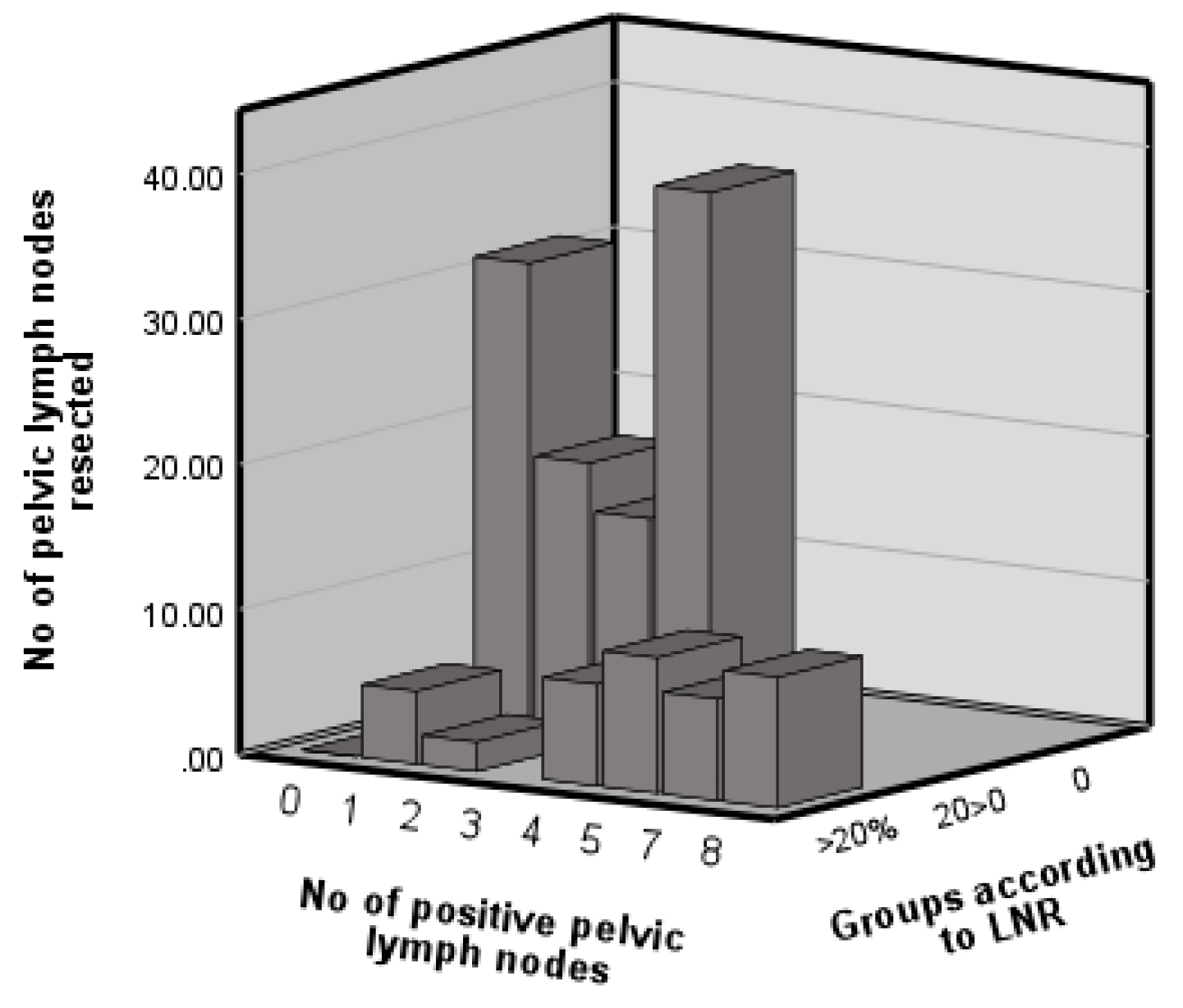
| LNR groups | |
| 0% | 69 (74.2%) |
| 0% < 20% | 8 (8.6%) |
| ≥20% | 16 (17.2%) |
| LVSI | |
| Negative | 40 (43%) |
| Positive | 25 (26.9%) |
| Not available | 28 (30.1%) |
| Necrosis | |
| Yes | 24 (25.8%) |
| No | 32 (34.4%) |
| Not available | 37 (39.8%) |
| Adjuvant therapy | |
| Chemotherapy | 15 (16.1%) |
| Radiotherapy | 33 (35.5%) |
| Both | 19 (20.4%) |
| Recurrence | 38 (40.9%) |
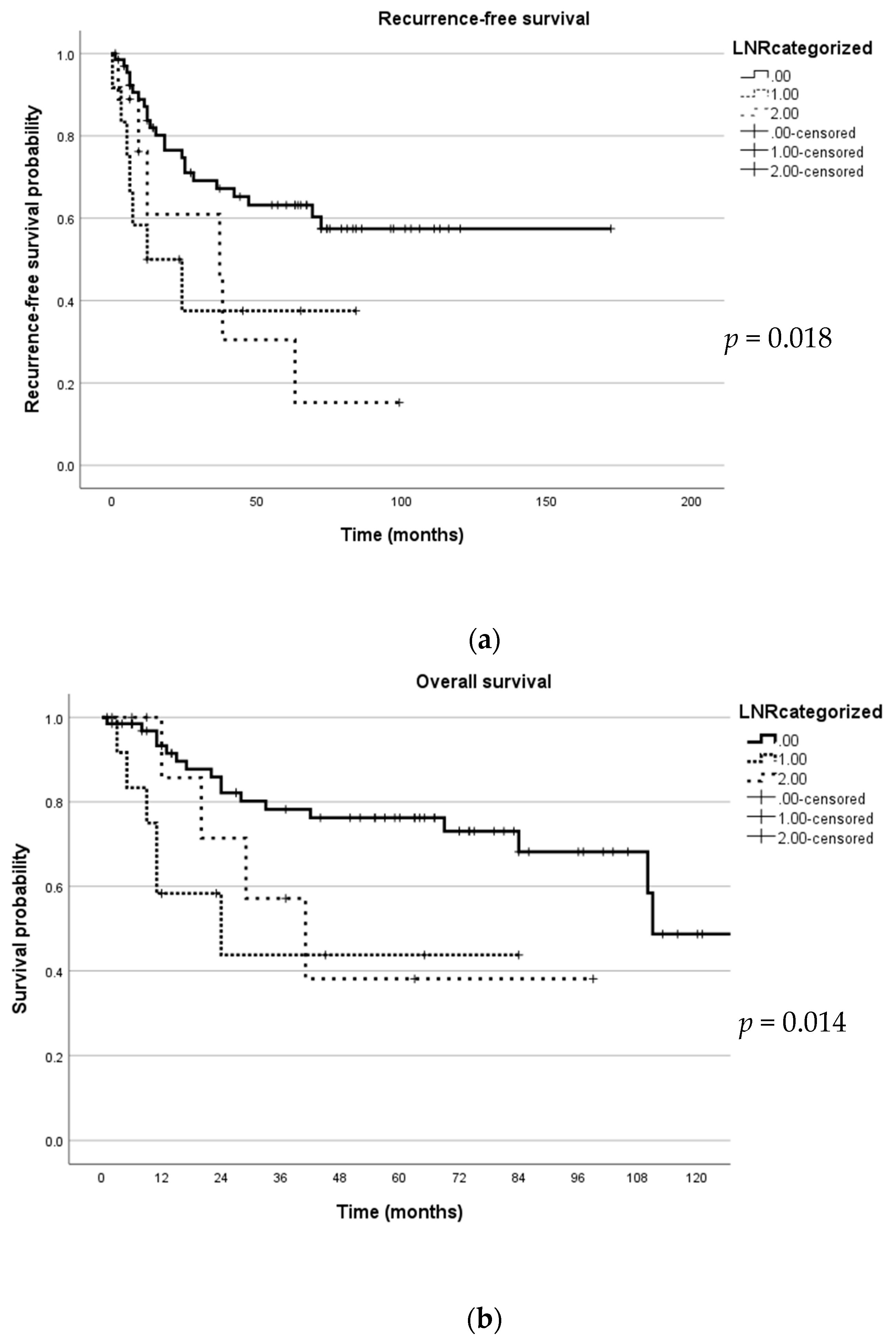
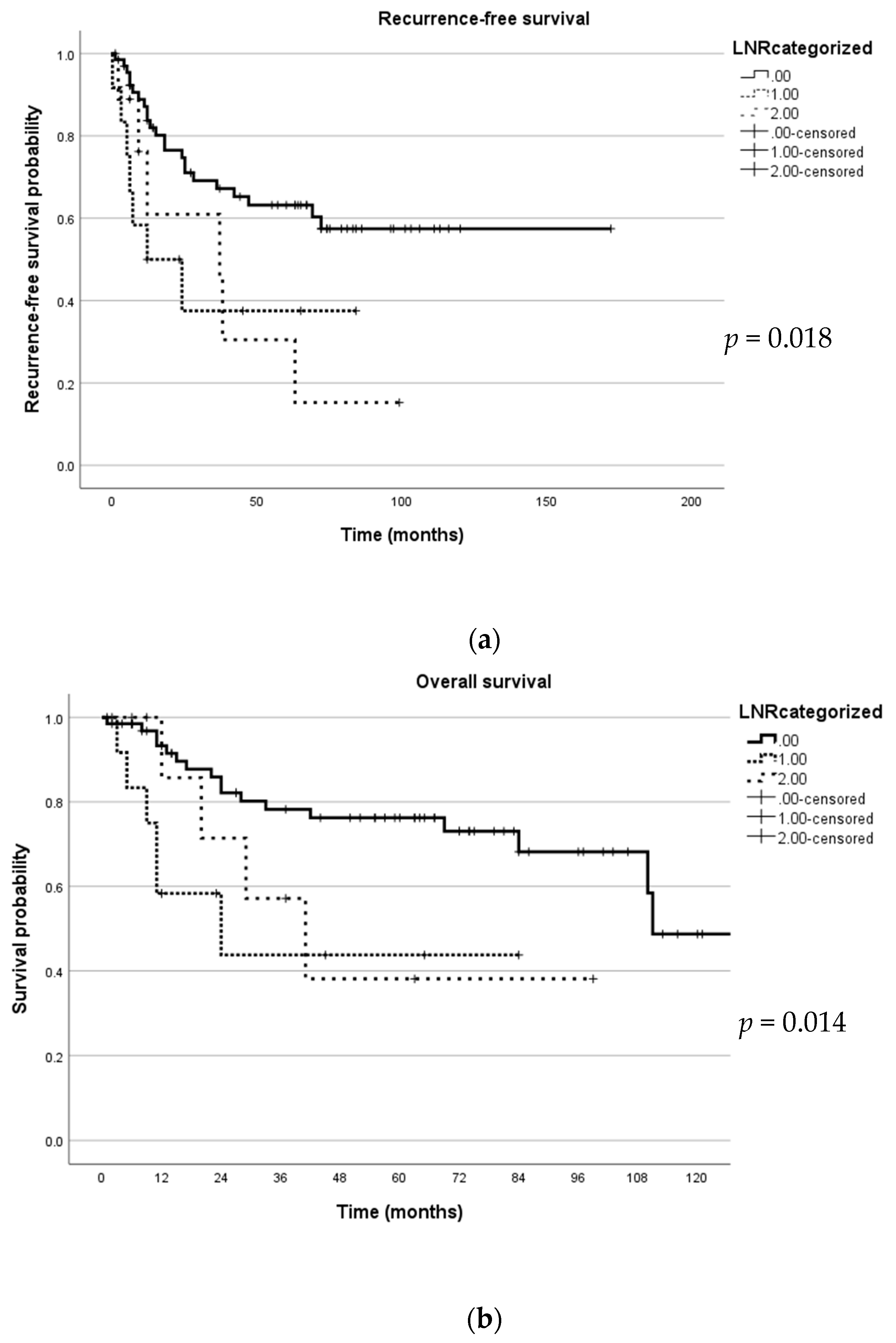
| Disease-free survival, mean (SD) months | 42.7 (38.1) |
| Overall survival, mean (SD) months | 46.9 (38.3) |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age | 1.82 | 0.93–3.55 | 0.08 | |||
| FIGO Stage | 1.41 | 1.05–1.89 | 0.021 | 1.39 | 0.99–1.96 | 0.058 |
| Adjuvant radiotherapy | 0.98 | 0.51–1.9 | 0.95 | |||
| Chemotherapy | 1.84 | 0.94–3.58 | 0.07 | |||
| LNR | 1.69 | 1.12–2.55 | 0.012 | 1.51 | 0.6–3.78 | 0.38 |
| LVSI | 1.66 | 0.79–3.46 | 0.18 | |||
| Positive margin | 3.75 | 1.55–9.08 | 0.003 | 4.63 | 1.35–15.93 | 0.015 |
| Residual disease | 7.34 | 2.5–21.56 | <0.001 | 3.79 | 0.76–18.85 | 0.103 |
| Tumour size > 5 cm | 2.11 | 1.06–4.23 | 0.034 | 2.33 | 1.02–5.32 | 0.045 |
| Positive pelvic LNs | 1.25 | 1.05–1.5 | 0.013 | 0.91 | 0.56–1.46 | 0.69 |
| Surgical approach | 1.68 | 0.23–12.28 | 0.61 | |||
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age | 1.95 | 0.9–4.2 | 0.09 | |||
| FIGO Stage | 1.14 | 0.8–1.64 | 0.47 | |||
| Adjuvant radiotherapy | 1.21 | 0.55–2.64 | 0.64 | |||
| Chemotherapy | 1.29 | 0.58–2.89 | 0.54 | |||
| LNR | 1.71 | 1.07–2.7 | 0.024 | 1.4 | 0.51–3.82 | 0.52 |
| LVSI | 0.88 | 0.37–2.03 | 0.76 | |||
| Positive margin | 2.09 | 0.72–6.09 | 0.18 | |||
| Residual disease | 2.94 | 1.23–6.68 | 0.01 | 1.6 | 0.39–6.6 | 0.52 |
| Tumour size > 5 cm | 2.14 | 1.00–4.54 | 0.049 | 1.13 | 1.05–5.96 | 0.038 |
| Positive pelvic LNs | 1.33 | 1.09–1.62 | 0.005 | 1.13 | 0.69–1.84 | 0.64 |
| Surgical approach | 1.15 | 0.16–8.57 | 0.89 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bharathan, R.; Polterauer, S.; Lopez-Sanclemente, M.C.; Trukhan, H.; Pletnev, A.; Heredia, A.G.; Gil, M.M.; Bakinovskaya, I.; Dalamanava, A.; Romeo, M.; et al. Prognostic Value of Lymph Node Ratio in Patients with Uterine Carcinosarcoma. J. Pers. Med. 2024, 14, 155. https://doi.org/10.3390/jpm14020155
Bharathan R, Polterauer S, Lopez-Sanclemente MC, Trukhan H, Pletnev A, Heredia AG, Gil MM, Bakinovskaya I, Dalamanava A, Romeo M, et al. Prognostic Value of Lymph Node Ratio in Patients with Uterine Carcinosarcoma. Journal of Personalized Medicine. 2024; 14(2):155. https://doi.org/10.3390/jpm14020155
Chicago/Turabian StyleBharathan, Rasiah, Stephan Polterauer, Martha C. Lopez-Sanclemente, Hanna Trukhan, Andrei Pletnev, Angel G. Heredia, Maria M. Gil, Irina Bakinovskaya, Alena Dalamanava, Margarita Romeo, and et al. 2024. "Prognostic Value of Lymph Node Ratio in Patients with Uterine Carcinosarcoma" Journal of Personalized Medicine 14, no. 2: 155. https://doi.org/10.3390/jpm14020155
APA StyleBharathan, R., Polterauer, S., Lopez-Sanclemente, M. C., Trukhan, H., Pletnev, A., Heredia, A. G., Gil, M. M., Bakinovskaya, I., Dalamanava, A., Romeo, M., Rovski, D., Baquedano, L., Chiva, L., Schwameis, R., Zapardiel, I., & on behalf of SARCUT Study Group. (2024). Prognostic Value of Lymph Node Ratio in Patients with Uterine Carcinosarcoma. Journal of Personalized Medicine, 14(2), 155. https://doi.org/10.3390/jpm14020155