
Binding Folate Receptor Alpha Autoantibody Is a Biomarker for Leucovorin Treatment Response in Autism Spectrum Disorder

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. FRAA Assay
2.2. Statistical Analysis
3. Results
3.1. Folate Biomarkers
3.2. Patient Characteristics
3.3. Effectiveness of Leucovorin Treatment
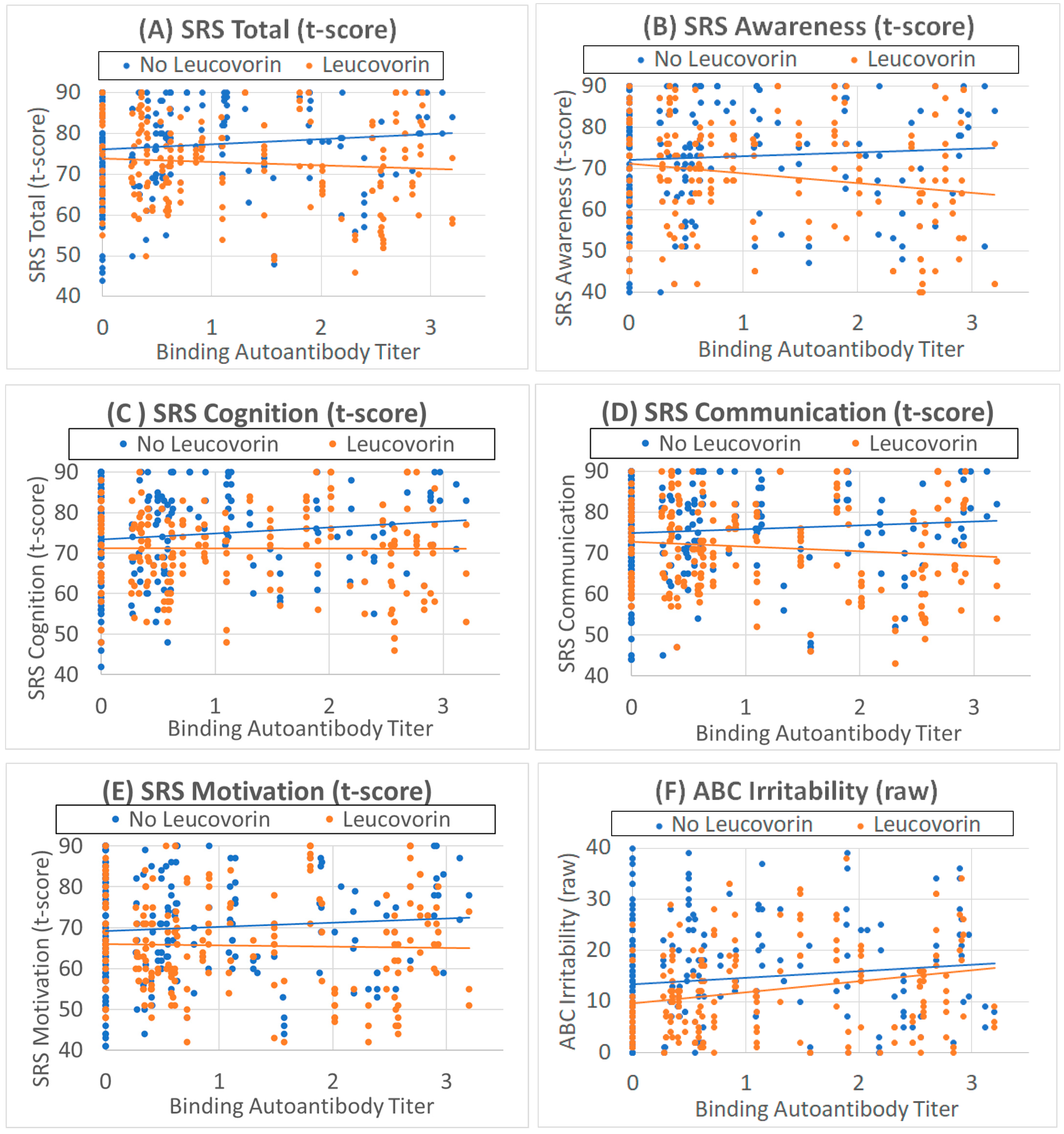
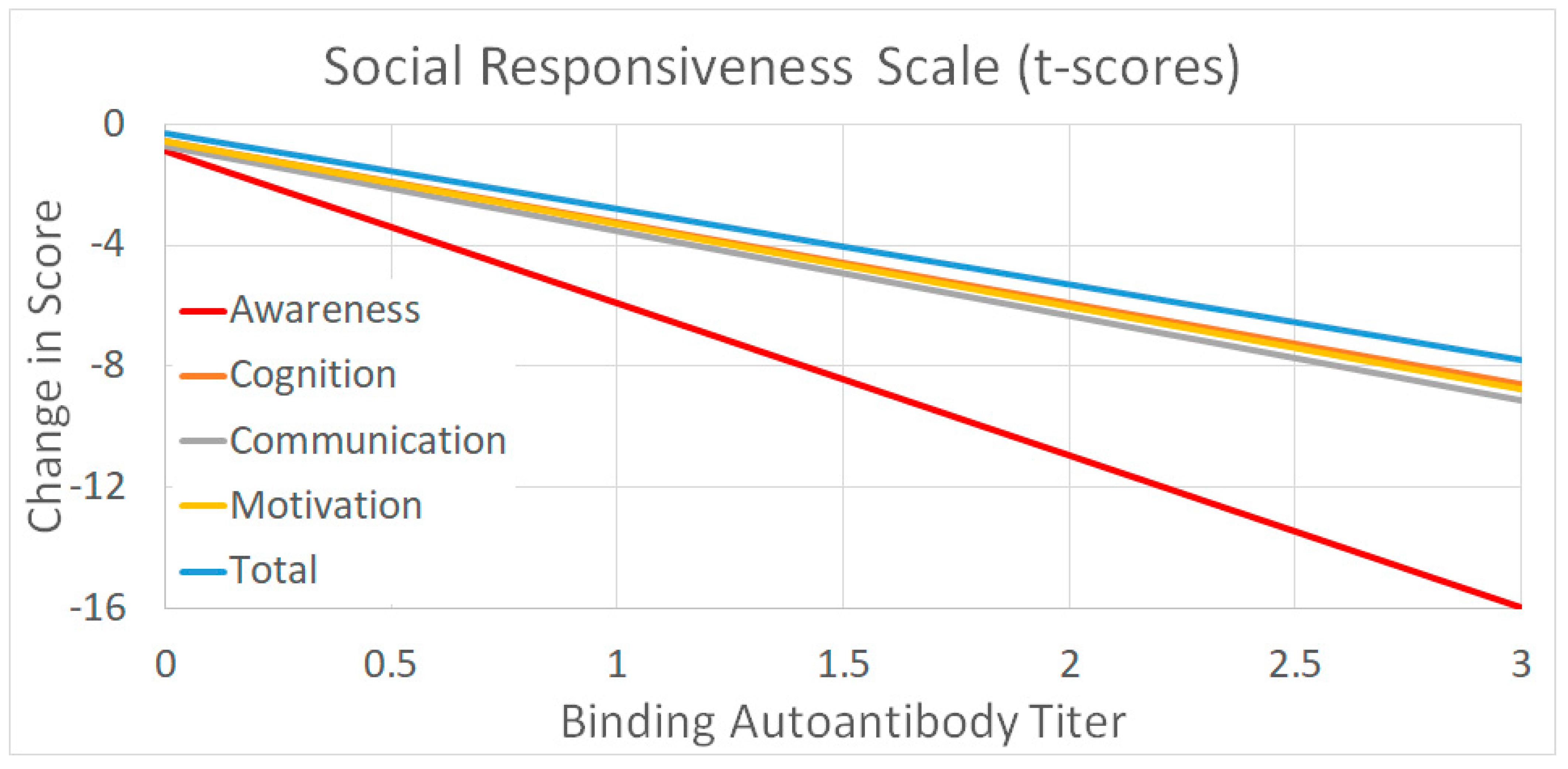
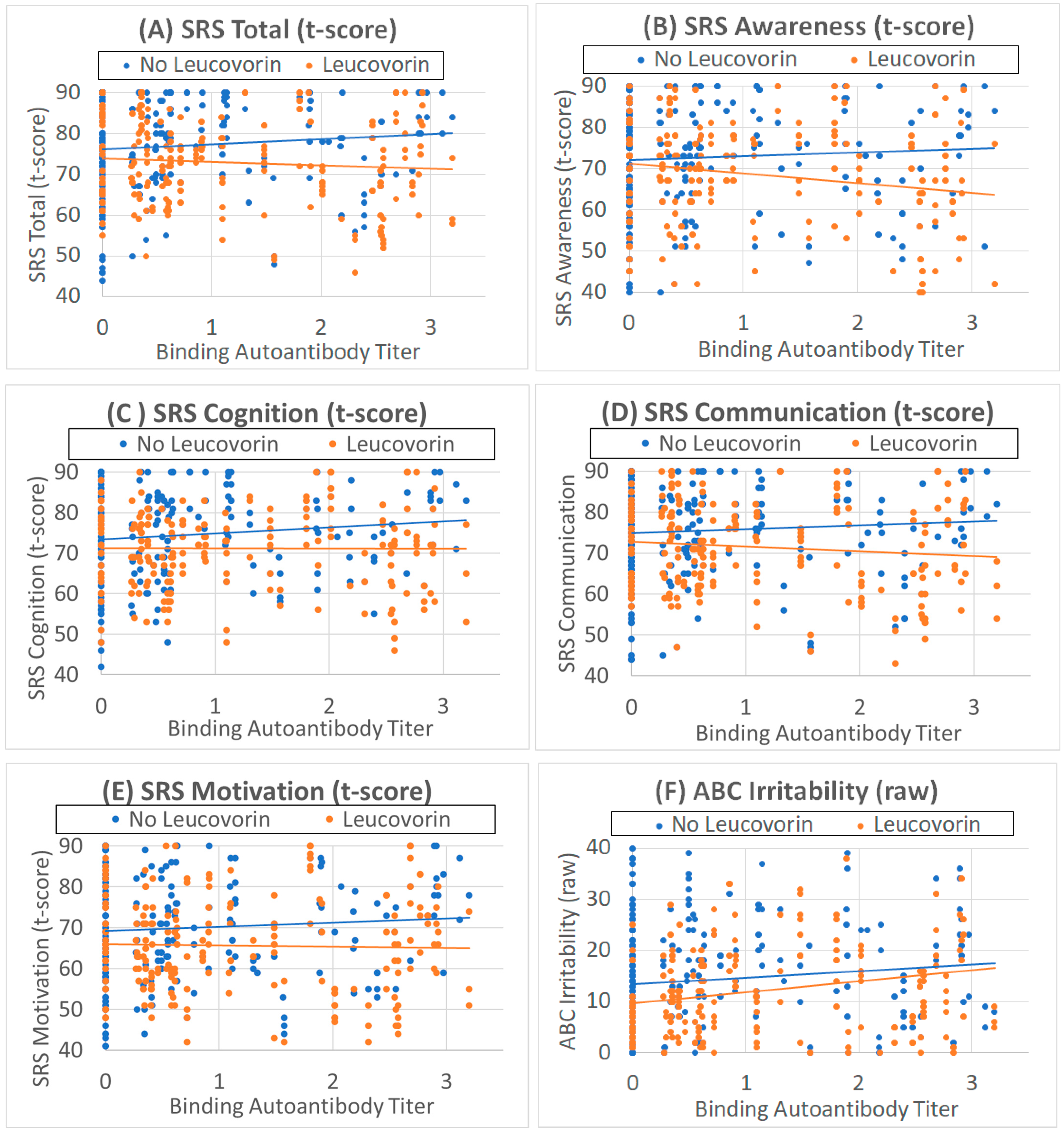
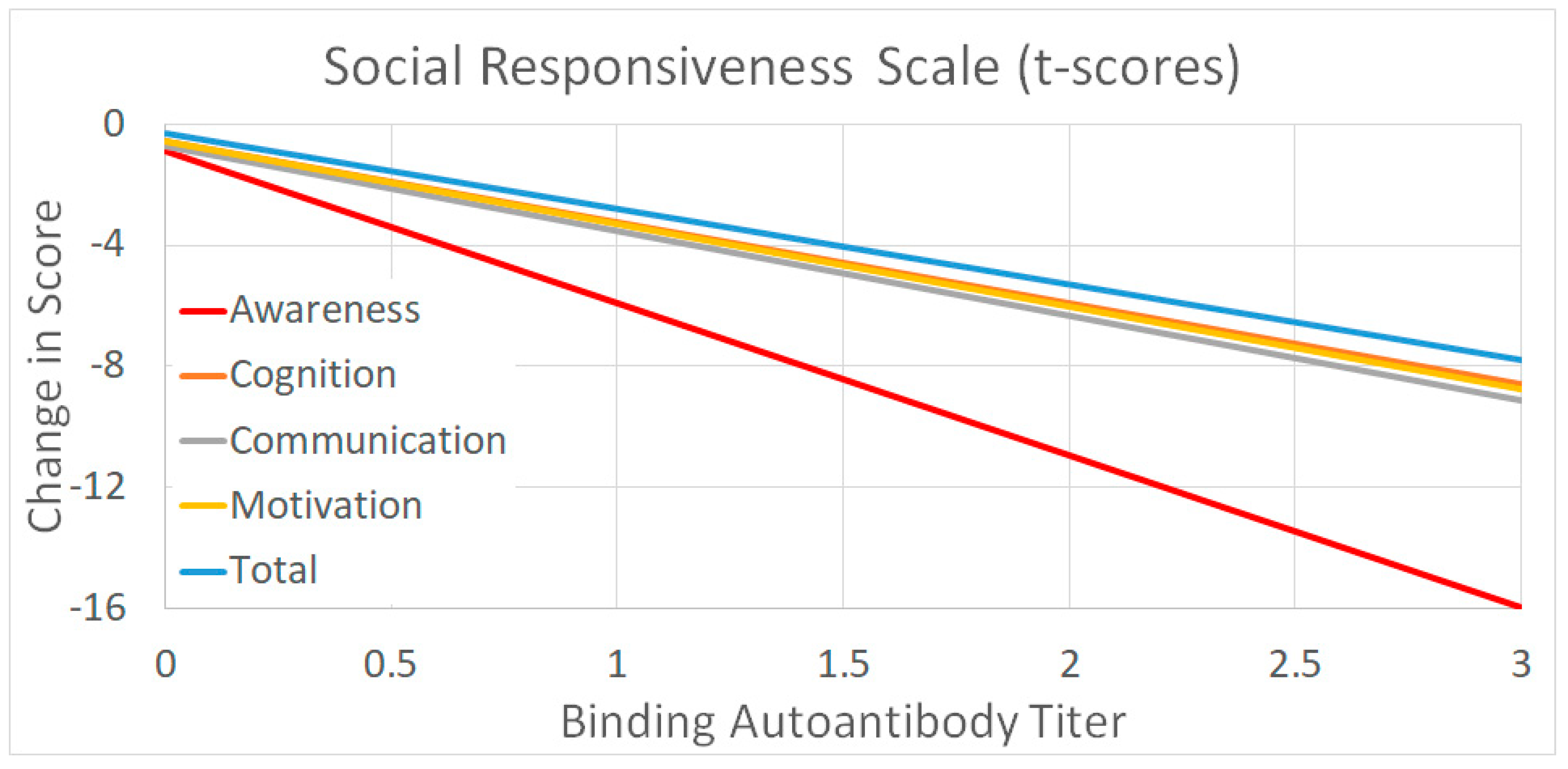
3.3.1. Social Responsiveness Scale
3.3.2. Aberrant Behavior Checklist
3.4. Effect of Leucovorin on Outcomes as a Function of Binding Titers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maenner, M.J.; Warren, Z.; Williams, A.R.; Amoakohene, E.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Fitzgerald, R.T.; Furnier, S.M.; Hughes, M.M.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. MMWR Surveill. Summ. 2023, 72, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Khachadourian, V.; Mahjani, B.; Sandin, S.; Kolevzon, A.; Buxbaum, J.D.; Reichenberg, A.; Janecka, M. Comorbidities in autism spectrum disorder and their etiologies. Transl. Psychiatry 2023, 13, 71. [Google Scholar] [CrossRef] [PubMed]
- Parrella, N.F.; Hill, A.T.; Dipnall, L.M.; Loke, Y.J.; Enticott, P.G.; Ford, T.C. Inhibitory dysfunction and social processing difficulties in autism: A comprehensive narrative review. J. Psychiatr. Res. 2023, 169, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Fan, G.; Ma, J.; Ma, R.; Suo, M.; Chen, Y.; Zhang, S.; Zeng, Y.; Chen, Y. Microglia Modulate Neurodevelopment in Autism Spectrum Disorder and Schizophrenia. Int. J. Mol. Sci. 2023, 24, 7297. [Google Scholar] [CrossRef] [PubMed]
- Kereszturi, É. Diversity and Classification of Genetic Variations in Autism Spectrum Disorder. Int. J. Mol. Sci. 2023, 24, 6768. [Google Scholar] [CrossRef]
- Al-Saei, A.; Nour-Eldine, W.; Rajpoot, K.; Arshad, N.; Al-Shammari, A.R.; Kamal, M.; Akil, A.A.; Fakhro, K.A.; Thornalley, P.J.; Rabbani, N. Validation of plasma protein glycation and oxidation biomarkers for the diagnosis of autism. Mol. Psychiatry 2023. [Google Scholar] [CrossRef]
- Than, U.T.T.; Nguyen, L.T.; Nguyen, P.H.; Nguyen, X.H.; Trinh, D.P.; Hoang, D.H.; Nguyen, P.A.T.; Dang, V.D. Inflammatory mediators drive neuroinflammation in autism spectrum disorder and cerebral palsy. Sci. Rep. 2023, 13, 22587. [Google Scholar] [CrossRef]
- Maier, S.; Nickel, K.; Lange, T.; Oeltzschner, G.; Dacko, M.; Endres, D.; Runge, K.; Schumann, A.; Domschke, K.; Rousos, M.; et al. Increased cerebral lactate levels in adults with autism spectrum disorders compared to non-autistic controls: A magnetic resonance spectroscopy study. Mol. Autism 2023, 14, 44. [Google Scholar] [CrossRef]
- Smith, A.M.; Donley, E.L.R.; Ney, D.M.; Amaral, D.G.; Burrier, R.E.; Natowicz, M.R. Metabolomic biomarkers in autism: Identification of complex dysregulations of cellular bioenergetics. Front. Psychiatry 2023, 14, 1249578. [Google Scholar] [CrossRef]
- Guo, R.; Pang, J.; Zhao, J.; Xiao, X.; Li, J.; Li, J.; Wang, W.; Zhou, S.; Zhao, Y.; Zhang, Z.; et al. Unveiling the neuroprotective potential of dietary polysaccharides: A systematic review. Front. Nutr. 2023, 10, 1299117. [Google Scholar] [CrossRef]
- Ramaekers, V.T.; Blau, N. Cerebral folate deficiency. Dev. Med. Child Neurol. 2004, 46, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Phunsawat, P.; Chiangjong, W.; Chutipongtanate, S.; Dumrongwongsiri, O.; Thommachot, P.; Butdawong, W.; Chuthapisith, J. Folate receptor alpha autoantibodies in children with autism spectrum disorder. Biomarkers 2022, 27, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Frye, R.E.; Lane, A.; Worner, A.; Werner, B.A.; McCarty, P.J.; Scheck, A.C.; Collins, H.L.; Adelman, S.J.; Quadros, E.V.; Rossignol, D.A. The Soluble Folate Receptor in Autism Spectrum Disorder: Relation to Autism Severity and Leucovorin Treatment. J. Pers. Med. 2022, 12, 2033. [Google Scholar] [CrossRef] [PubMed]
- Pineda, M.; Ormazabal, A.; Lopez-Gallardo, E.; Nascimento, A.; Solano, A.; Herrero, M.D.; Vilaseca, M.A.; Briones, P.; Ibanez, L.; Montoya, J.; et al. Cerebral folate deficiency and leukoencephalopathy caused by a mitochondrial DNA deletion. Ann. Neurol. 2006, 59, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Moretti, P.; Sahoo, T.; Hyland, K.; Bottiglieri, T.; Peters, S.; del Gaudio, D.; Roa, B.; Curry, S.; Zhu, H.; Finnell, R.H.; et al. Cerebral folate deficiency with developmental delay, autism, and response to folinic acid. Neurology 2005, 64, 1088–1090. [Google Scholar] [CrossRef] [PubMed]
- Gusso, D.; Prauchner, G.R.K.; Rieder, A.S.; Wyse, A.T.S. Biological Pathways Associated with Vitamins in Autism Spectrum Disorder. Neurotox. Res. 2023, 41, 730–740. [Google Scholar] [CrossRef] [PubMed]
- Zigman, T.; Petkovic Ramadza, D.; Simic, G.; Baric, I. Inborn Errors of Metabolism Associated With Autism Spectrum Disorders: Approaches to Intervention. Front. Neurosci. 2021, 15, 673600. [Google Scholar] [CrossRef]
- Pacheva, I.; Ivanov, I. Targeted Biomedical Treatment for Autism Spectrum Disorders. Curr. Pharm. Des. 2019, 25, 4430–4453. [Google Scholar] [CrossRef]
- Koenig, M.K.; Perez, M.; Rothenberg, S.; Butler, I.J. Juvenile onset central nervous system folate deficiency and rheumatoid arthritis. J. Child Neurol. 2008, 23, 106–107. [Google Scholar] [CrossRef]
- Rossignol, D.A.; Frye, R.E. Cerebral Folate Deficiency, Folate Receptor Alpha Autoantibodies and Leucovorin (Folinic Acid) Treatment in Autism Spectrum Disorders: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 1141. [Google Scholar] [CrossRef]
- Pan, L.A.; Segreti, A.M.; Wrobleski, J.; Shaw, A.; Hyland, K.; Hughes, M.; Finegold, D.N.; Naviaux, R.K.; Brent, D.A.; Vockley, J.; et al. Metabolomic disorders: Confirmed presence of potentially treatable abnormalities in patients with treatment refractory depression and suicidal behavior. Psychol. Med. 2023, 53, 6046–6054. [Google Scholar] [CrossRef] [PubMed]
- Frye, R.E.; Slattery, J.; Delhey, L.; Furgerson, B.; Strickland, T.; Tippett, M.; Sailey, A.; Wynne, R.; Rose, S.; Melnyk, S.; et al. Folinic acid improves verbal communication in children with autism and language impairment: A randomized double-blind placebo-controlled trial. Mol. Psychiatry 2018, 23, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Duvekot, J.; van der Ende, J.; Verhulst, F.C.; Greaves-Lord, K. The Screening Accuracy of the Parent and Teacher-Reported Social Responsiveness Scale (SRS): Comparison with the 3Di and ADOS. J. Autism Dev. Disord. 2015, 45, 1658–1672. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.J.; Mayes, S.D.; Smith, L.A. Brief report: Excellent agreement between two brief autism scales (Checklist for Autism Spectrum Disorder and Social Responsiveness Scale) completed independently by parents and the Autism Diagnostic Interview-Revised. J. Autism Dev. Disord. 2011, 41, 1586–1590. [Google Scholar] [CrossRef] [PubMed]
- Connery, K.; Tippett, M.; Delhey, L.M.; Rose, S.; Slattery, J.C.; Kahler, S.G.; Hahn, J.; Kruger, U.; Cunningham, M.W.; Shimasaki, C.; et al. Intravenous immunoglobulin for the treatment of autoimmune encephalopathy in children with autism. Transl. Psychiatry 2018, 8, 148. [Google Scholar] [CrossRef] [PubMed]
- Frye, R.E.; Sequeira, J.M.; Quadros, E.V.; James, S.J.; Rossignol, D.A. Cerebral folate receptor autoantibodies in autism spectrum disorder. Mol. Psychiatry 2013, 18, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Sequeira, J.M.; Ramaekers, V.T.; Quadros, E.V. The diagnostic utility of folate receptor autoantibodies in blood. Clin. Chem. Lab. Med. 2013, 51, 545–554. [Google Scholar] [CrossRef]
- Holm, J.; Hansen, S.I. Characterization of soluble folate receptors (folate binding proteins) in humans. Biological roles and clinical potentials in infection and malignancy. Biochim. Biophys. Acta (BBA)-Proteins Proteom. 2020, 1868, 140466. [Google Scholar] [CrossRef]
- Cai, C.; Yin, Z.; Liu, A.; Wang, H.; Zeng, S.; Wang, Z.; Qiu, H.; Li, S.; Zhou, J.; Wang, M. Identifying Rare Genetic Variants of Immune Mediators as Risk Factors for Autism Spectrum Disorder. Genes 2022, 13, 1098. [Google Scholar] [CrossRef]
- Hoxha, B.; Hoxha, M.; Domi, E.; Gervasoni, J.; Persichilli, S.; Malaj, V.; Zappacosta, B. Folic Acid and Autism: A Systematic Review of the Current State of Knowledge. Cells 2021, 10, 1976. [Google Scholar] [CrossRef]
- Renard, E.; Leheup, B.; Gueant-Rodriguez, R.M.; Oussalah, A.; Quadros, E.V.; Gueant, J.L. Folinic acid improves the score of Autism in the EFFET placebo-controlled randomized trial. Biochimie 2020, 173, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Liu, A.; He, F.; Jin, Y.; Zhou, S.; Xu, R.; Guo, H.; Zhou, W.; Wei, Q.; Wang, M. High prevalence of serum folate receptor autoantibodies in children with autism spectrum disorders. Biomarkers 2018, 23, 622–624. [Google Scholar] [CrossRef] [PubMed]
- Frye, R.E.; Delhey, L.; Slattery, J.; Tippett, M.; Wynne, R.; Rose, S.; Kahler, S.G.; Bennuri, S.C.; Melnyk, S.; Sequeira, J.M.; et al. Blocking and Binding Folate Receptor Alpha Autoantibodies Identify Novel Autism Spectrum Disorder Subgroups. Front. Neurosci. 2016, 10, 80. [Google Scholar] [CrossRef] [PubMed]
- Fallah, M.S.; Shaikh, M.R.; Neupane, B.; Rusiecki, D.; Bennett, T.A.; Beyene, J. Atypical Antipsychotics for Irritability in Pediatric Autism: A Systematic Review and Network Meta-Analysis. J. Child Adolesc. Psychopharmacol. 2019, 29, 168–180. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.R.; Lane, A.L.; Werner, B.A.; McLees, S.E.; Fletcher, T.S.; Frye, R.E. Modern Biomarkers for Autism Spectrum Disorder: Future Directions. Mol. Diagn. Ther. 2022, 26, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Doaei, S.; Bourbour, F.; Teymoori, Z.; Jafari, F.; Kalantari, N.; Abbas Torki, S.; Ashoori, N.; Nemat Gorgani, S.; Gholamalizadeh, M. The effect of omega-3 fatty acids supplementation on social and behavioral disorders of children with autism: A randomized clinical trial. Pediatr. Endocrinol. Diabetes Metab. 2021, 27, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Ooi, Y.P.; Weng, S.J.; Jang, L.Y.; Low, L.; Seah, J.; Teo, S.; Ang, R.P.; Lim, C.G.; Liew, A.; Fung, D.S.; et al. Omega-3 fatty acids in the management of autism spectrum disorders: Findings from an open-label pilot study in Singapore. Eur. J. Clin. Nutr. 2015, 69, 969–971. [Google Scholar] [CrossRef]
- Cheng, Y.S.; Tseng, P.T.; Chen, Y.W.; Stubbs, B.; Yang, W.C.; Chen, T.Y.; Wu, C.K.; Lin, P.Y. Supplementation of omega 3 fatty acids may improve hyperactivity, lethargy, and stereotypy in children with autism spectrum disorders: A meta-analysis of randomized controlled trials. Neuropsychiatr. Dis. Treat. 2017, 13, 2531–2543. [Google Scholar] [CrossRef]
- Rossignol, D.A.; Frye, R.E. The Effectiveness of Cobalamin (B12) Treatment for Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 784. [Google Scholar] [CrossRef]
- Corejova, A.; Fazekas, T.; Janosikova, D.; Repisky, J.; Pospisilova, V.; Mikova, M.; Rauova, D.; Ostatnikova, D.; Kyselovic, J.; Hrabovska, A. Improvement of the Clinical and Psychological Profile of Patients with Autism after Methylcobalamin Syrup Administration. Nutrients 2022, 14, 2035. [Google Scholar] [CrossRef]
- James, S.J.; Melnyk, S.; Jernigan, S.; Hubanks, A.; Rose, S.; Gaylor, D.W. Abnormal transmethylation/transsulfuration metabolism and DNA hypomethylation among parents of children with autism. J. Autism Dev. Disord. 2008, 38, 1966–1975. [Google Scholar] [CrossRef] [PubMed]
- Hendren, R.L.; James, S.J.; Widjaja, F.; Lawton, B.; Rosenblatt, A.; Bent, S. Randomized, Placebo-Controlled Trial of Methyl B12 for Children with Autism. J. Child Adolesc. Psychopharmacol. 2016, 26, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Geier, D.A.; Kern, J.K.; Davis, G.; King, P.G.; Adams, J.B.; Young, J.L.; Geier, M.R. A prospective double-blind, randomized clinical trial of levocarnitine to treat autism spectrum disorders. Med. Sci. Monit. 2011, 17, PI15–PI23. [Google Scholar] [CrossRef] [PubMed]
- Fahmy, S.F.; El-hamamsy, M.H.; Zaki, O.K.; Badary, O.A. l-Carnitine supplementation improves the behavioral symptoms in autistic children. Res. Autism Spectr. Disord. 2013, 7, 159–166. [Google Scholar] [CrossRef]
- Shakibaei, F.; Jelvani, D. Effect of Adding l-Carnitine to Risperidone on Behavioral, Cognitive, Social, and Physical Symptoms in Children and Adolescents With Autism: A Randomized Double-Blinded Placebo-Controlled Clinical Trial. Clin. Neuropharmacol. 2023, 46, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Nickel, K.; Menke, M.; Endres, D.; Runge, K.; Tucci, S.; Schumann, A.; Domschke, K.; Tebartz van Elst, L.; Maier, S. Altered markers of mitochondrial function in adults with autism spectrum disorder. Autism Res. 2023, 16, 2125–2138. [Google Scholar] [CrossRef] [PubMed]
- Kępka, A.; Ochocińska, A.; Chojnowska, S.; Borzym-Kluczyk, M.; Skorupa, E.; Knaś, M.; Waszkiewicz, N. Potential Role of L-Carnitine in Autism Spectrum Disorder. J. Clin. Med. 2021, 10, 1202. [Google Scholar] [CrossRef]
- Nasiri, M.; Parmoon, Z.; Farahmand, Y.; Moradi, A.; Farahmand, K.; Moradi, K.; Basti, F.A.; Mohammadi, M.R.; Akhondzadeh, S. l-carnitine adjunct to risperidone for treatment of autism spectrum disorder-associated behaviors: A randomized, double-blind clinical trial. Int. Clin. Psychopharmacol. 2023. [Google Scholar] [CrossRef]
- Beversdorf, D.Q. The Role of the Noradrenergic System in Autism Spectrum Disorders, Implications for Treatment. Semin. Pediatr. Neurol. 2020, 35, 100834. [Google Scholar] [CrossRef]
- Zamzow, R.M.; Ferguson, B.J.; Ragsdale, A.S.; Lewis, M.L.; Beversdorf, D.Q. Effects of acute beta-adrenergic antagonism on verbal problem solving in autism spectrum disorder and exploration of treatment response markers. J. Clin. Exp. Neuropsychol. 2017, 39, 596–606. [Google Scholar] [CrossRef]
- Zamzow, R.M.; Ferguson, B.J.; Stichter, J.P.; Porges, E.C.; Ragsdale, A.S.; Lewis, M.L.; Beversdorf, D.Q. Effects of propranolol on conversational reciprocity in autism spectrum disorder: A pilot, double-blind, single-dose psychopharmacological challenge study. Psychopharmacology 2016, 233, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, J.P., 2nd; Zamzow, R.M.; Ferguson, B.J.; Christ, S.E.; Porges, E.C.; Johnson, J.D.; Beversdorf, D.Q. Beta-adrenergic antagonism alters functional connectivity during associative processing in a preliminary study of individuals with and without autism. Autism 2020, 24, 795–801. [Google Scholar] [CrossRef] [PubMed]
- London, E.B.; Yoo, J.H.; Fethke, E.D.; Zimmerman-Bier, B. The Safety and Effectiveness of High-Dose Propranolol as a Treatment for Challenging Behaviors in Individuals With Autism Spectrum Disorders. J. Clin. Psychopharmacol. 2020, 40, 122–129. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Folate Biomarker Groups | ||||
|---|---|---|---|---|
| sFBPs+ (n = 14) | Blocking+ (n = 4) | Binding+ (n = 70) | Overall | |
| sFBP Prevelence | 100% | 10% | 13% | |
| Blocking Prevelence | 100% | 6% | 4% | |
| Blocking Titer (pmol/mL) | 2.45 (0.65) | 0.14 (0.59) | 0.09 (0.47) | |
| Binding Prevelence | 50% | 100% | 100% | 65% |
| Binding Titer (pmol/mL) | 0.34 (0.40) * | 2.03 (1.09) * | 1.37 (0.96) | 0.88 (1.01) |
| sFBPs+ (n = 14) | Blocking+ (n = 4) | Binding+ (n = 70) | Negative (n = 32) | Overall (n = 110) † | |
|---|---|---|---|---|---|
| Age (SD) in years | 11.0 (5.1) | 8.2 (4.2) | 10.5 (5.8) | 10.1 (7.2) | 10.5 (6.2) |
| Sex (% Male) | 93% | 75% | 76% | 63% | 74% |
| Race: White/Black/Asian | 71%/29%/0% | 50%/25%/25% | 80%/3%/10% | 85%/0%/13% * | 81%/5%/10% |
| Ethnicity (% Hispanic) | 7% | 25% | 4% | 16% | 8% |
| Development: Birth/Plateau/Regression | 0%/36%/64% | 0%/0%/100% | 11%/37%/51% | 3%/53%/41% | 8%/42%/49% |
| Treatments | |||||
| Oral Leucovorin/Other Oral Folate | 86% */64% | 75%/75% | 70% ***/48% | 22% ***/44% | 57%/47% |
| mB12 & Leucovorin SQ/Oral B12 | 43%/36% | 75%/50% | 31%/41% | 25%/34% | 30%/38% |
| Other Bs/Non B Vits | 21%/43% | 75%/50% | 32%/56% | 31%/53% | 31%/53% |
| ASD MVI/Other MVI | 14%/29% | 50%/25% | 25%/27% | 28%/32% | 25%/29% |
| Antioxidants/Minerals | 29%/35% | 50%/50% | 30%/37% | 31%/44% | 29%/36% |
| Carnitine/CoQ 10 | 36%/21% | 75%/50% | 41%/39% | 50%/34% | 42%/36% |
| Melatonin/Herbal Meds | 14%/0% | 0%/0% | 18%/4% | 22%/19% * | 18%/8% |
| Fatty Acids/Amino Acids | 29%/21% | 50%/0% | 31%/18% | 25%/13% | 29%/16% |
| Stimulants/Alpha Adenergics | 14%/0% * | 0%/0% | 16%/23% | 9%/28% | 14%/23% |
| Allergy & Asthma/GI Meds | 29%/43% | 25%/75% | 34%/59% | 38%/59% | 34%/57% |
| Inflamatory & Immune/Anti-Microbials | 7%/7% | 0%/25% | 13%/14% | 9%/15% | 12%/14% |
| Antipsychotics/Other Psychotropics | 21%/7% | 0%/50% | 16%/9% | 9%/13% | 13%/10% |
| SSRIs/Beta-Blockers | 21%/7% | 25%/50% | 18%/20% | 13%/16% | 16%/17% |
| Anti-Epileptic Meds/Diuretic | 21%/0% | 0%/25% | 21%/4% | 31%/3% | 25%/4% |
| Thyroid Meds/Other Hormones | 0%/7% | 0%/0% | 1%/4% | 13% **/3% | 5%/5% |
| SRS Subscale | mB12 SQ | β Blocker | Fatty Acids |
|---|---|---|---|
| Total | −2.8 (1.1) ** | 2.8 (1.2) * | |
| Awareness | −3.0 (1.6) * | ||
| Cognition | −4.3 (1.3) *** | 2.8 (1.4) * | −2.4 (1.2) * |
| Communication | −2.3 (1.2) * | −2.4 (1.2) * | |
| Motivation | −3.0 (1.4) * | −3.0 (1.4) * | |
| Mannerisms | −3.6 (1.1) *** | 2.6 (1.3) * |
| ABC Subscale | β Blocker | Fatty Acids | Carnitine |
|---|---|---|---|
| Irritability | 4.8 (1.3) *** | ||
| Social Withdrawal | −2.0 (0.9) * | ||
| Stereotypy | −1.3 (0.5) ** | ||
| Hyperactivity | −2.2 (0.7) ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frye, R.E.; McCarty, P.J.; Werner, B.A.; Scheck, A.C.; Collins, H.L.; Adelman, S.J.; Rossignol, D.A.; Quadros, E.V. Binding Folate Receptor Alpha Autoantibody Is a Biomarker for Leucovorin Treatment Response in Autism Spectrum Disorder. J. Pers. Med. 2024, 14, 62. https://doi.org/10.3390/jpm14010062
Frye RE, McCarty PJ, Werner BA, Scheck AC, Collins HL, Adelman SJ, Rossignol DA, Quadros EV. Binding Folate Receptor Alpha Autoantibody Is a Biomarker for Leucovorin Treatment Response in Autism Spectrum Disorder. Journal of Personalized Medicine. 2024; 14(1):62. https://doi.org/10.3390/jpm14010062
Chicago/Turabian StyleFrye, Richard E., Patrick J. McCarty, Brianna A. Werner, Adrienne C. Scheck, Heidi L. Collins, Steven J. Adelman, Daniel A. Rossignol, and Edward V. Quadros. 2024. "Binding Folate Receptor Alpha Autoantibody Is a Biomarker for Leucovorin Treatment Response in Autism Spectrum Disorder" Journal of Personalized Medicine 14, no. 1: 62. https://doi.org/10.3390/jpm14010062
APA StyleFrye, R. E., McCarty, P. J., Werner, B. A., Scheck, A. C., Collins, H. L., Adelman, S. J., Rossignol, D. A., & Quadros, E. V. (2024). Binding Folate Receptor Alpha Autoantibody Is a Biomarker for Leucovorin Treatment Response in Autism Spectrum Disorder. Journal of Personalized Medicine, 14(1), 62. https://doi.org/10.3390/jpm14010062