
New Community and Sociohealth Challenges Arising from the Early Diagnosis of Mild Cognitive Impairment (MCI)



Abstract
:1. Introduction
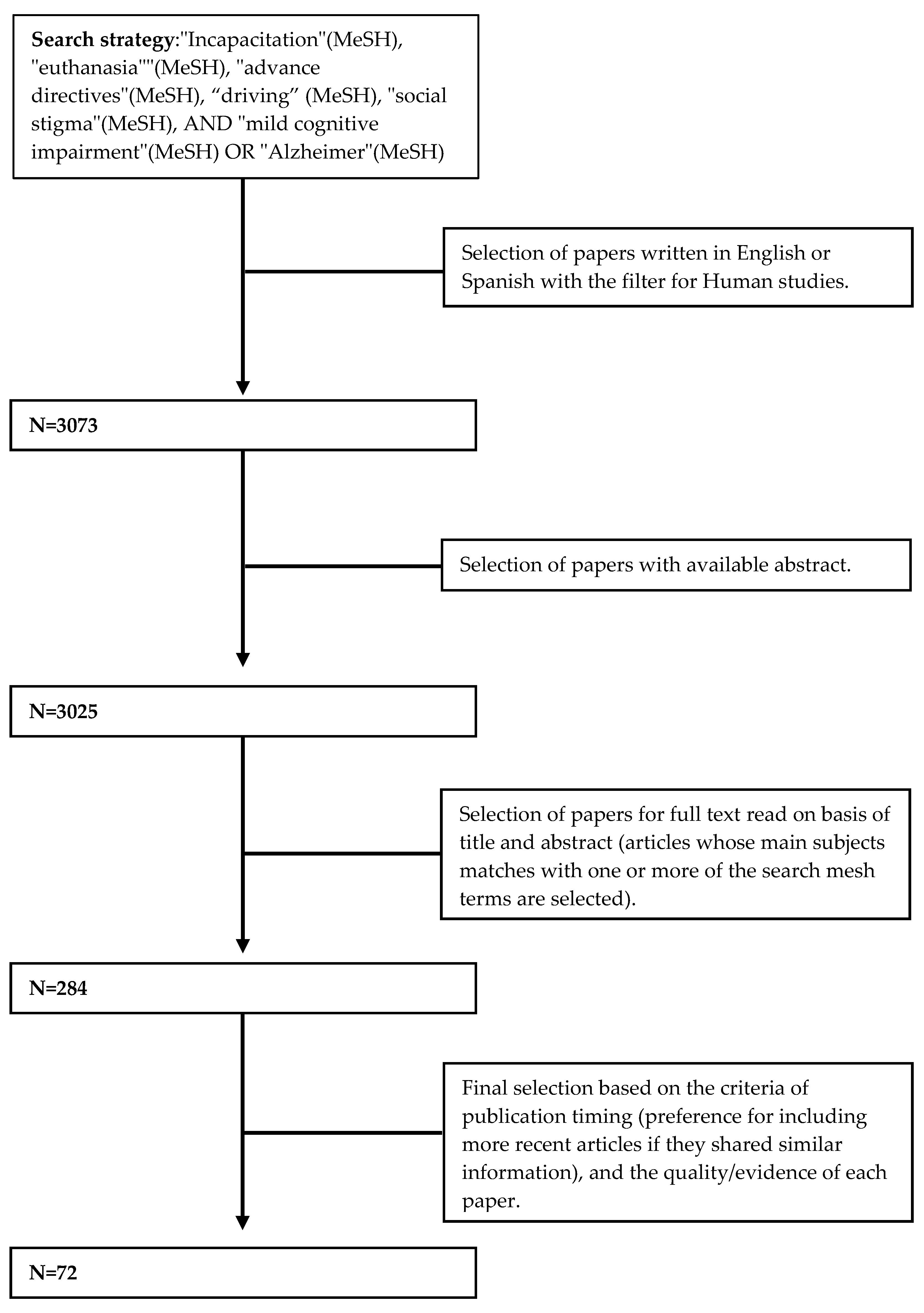
2. Methodology
3. Mild Cognitive Impairment (MCI)
3.1. Prevalence of MCI
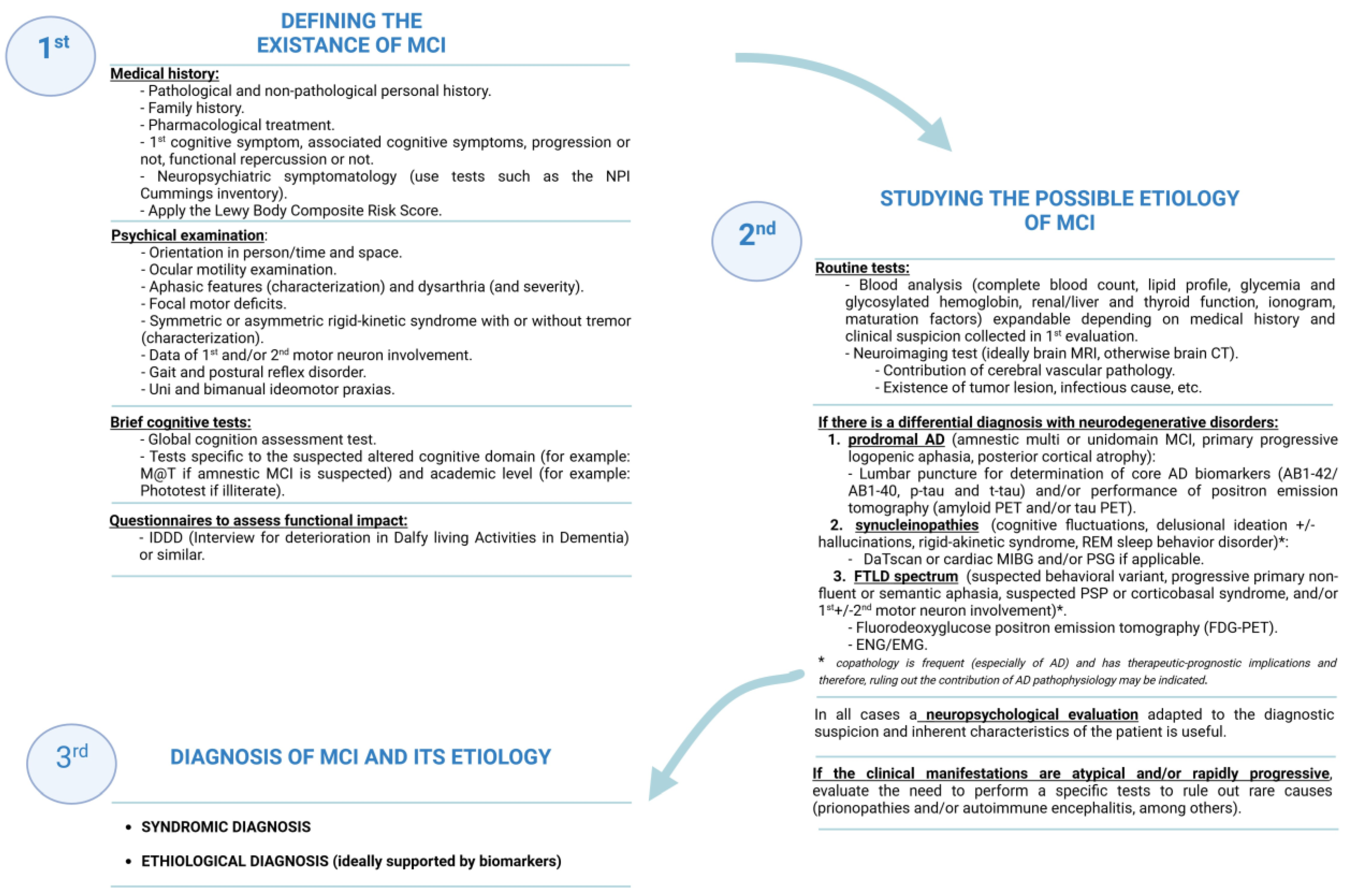
3.2. Diagnosis of MCI
3.3. Etiology of MCI
4. Benefits of an Early Syndromic and Etiological Diagnosis of MCI
4.1. Pharmacological and Nonpharmacological Treatment of MCI
4.2. Advance Directives
4.3. Protection of the Dignity and Integrity of the Person: Legal Perspective
- -
- A power of attorney is useful when a person is unable to perform complex specific tasks without assistance (financial decisions, for instance) and they are not legally incapacitated [38];
- -
- Instead, a healthcare surrogate is a person authorized via the Designation of Health Care Surrogate form to make medical decisions when the patient is not able to do so;
- -
- A guardianship substitutes decision-makers, depending on the type of guardianship imposed by the court, and has the power to perform financial, personal, legal, and healthcare choices for their ward. Guardians of property are responsible for the financial assets of the ward, whereas plenary guardians are responsible for every aspect of the ward.
5. Sociohealth Challenges due to the Early Diagnosis of MCI
5.1. Stigma and Risk of Sociolabor Exclusion
5.2. Impact on Socioemotional Health
5.3. Repercussion on Complex Regulated Activities: Driving
6. Strategies to Reduce Social Stigma and Behavioral–Affective Impact and Favor the Inclusion of People with MCI
6.1. Training for Healthcare and Social–Health Care Professionals and Caregivers and Social Awareness
6.2. Patient Empowerment Strategies
6.3. Promoting Inclusive Policies
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frederiksen, K.S.; Nielsen, T.R.; Winblad, B.; Schmidt, R.; Kramberger, M.G.; Jones, R.W.; Hort, J.; Grimmer, T.; Georges, J.; Frölich, L.; et al. European Academy of Neurology/European Alzheimer’s Disease Consortium Position Statement on Diagnostic Disclosure, Biomarker Counseling, and Management of Patients with Mild Cognitive Impairment. Eur. J. Neurol. 2021, 28, 2147–2155. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Chen, P.; Cai, H.; Zhang, Q.; Su, Z.; Cheung, T.; Jackson, T.; Sha, S.; Xiang, Y.-T. Worldwide Prevalence of Mild Cognitive Impairment among Community Dwellers Aged 50 Years and Older: A Meta-Analysis and Systematic Review of Epidemiology Studies. Age Ageing 2022, 51, afac173. [Google Scholar] [CrossRef] [PubMed]
- Manly, J.J.; Jones, R.N.; Langa, K.M.; Ryan, L.H.; Levine, D.A.; McCammon, R.; Heeringa, S.G.; Weir, D. Estimating the Prevalence of Dementia and Mild Cognitive Impairment in the US: The 2016 Health and Retirement Study Harmonized Cognitive Assessment Protocol Project. JAMA Neurol. 2022, 79, 1242–1249. [Google Scholar] [CrossRef]
- Tampi, R.R.; Forester, B.P.; Agronin, M. Aducanumab: Evidence from Clinical Trial Data and Controversies. Drugs Context 2021, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- van Dyck, C.H.; Swanson, C.J.; Aisen, P.; Bateman, R.J.; Chen, C.; Gee, M.; Kanekiyo, M.; Li, D.; Reyderman, L.; Cohen, S.; et al. Lecanemab in Early Alzheimer’s Disease. N. Engl. J. Med. 2022, 388, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Sims, J.R.; Zimmer, J.A.; Evans, C.D.; Lu, M.; Ardayfio, P.; Sparks, J.; Wessels, A.M.; Shcherbinin, S.; Wang, H.; Monkul Nery, E.S.; et al. Donanemab in Early Symptomatic Alzheimer Disease: The TRAILBLAZER-ALZ 2 Randomized Clinical Trial. JAMA 2023, 330, 512–527. [Google Scholar] [CrossRef]
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef]
- Jack, C.R.J.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a Biological Definition of Alzheimer’s Disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Dunne, R.A.; Aarsland, D.; O’Brien, J.T.; Ballard, C.; Banerjee, S.; Fox, N.C.; Isaacs, J.D.; Underwood, B.R.; Perry, R.J.; Chan, D.; et al. Mild Cognitive Impairment: The Manchester Consensus. Age Ageing 2021, 50, 72–80. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild Cognitive Impairment. Lancet 2006, 367, 1979. [Google Scholar] [CrossRef]
- Parfenov, V.A.; Zakharov, V.V.; Kabaeva, A.R.; Vakhnina, N.V. Subjective Cognitive Decline as a Predictor of Future Cognitive Decline: A Systematic Review. Dement. Neuropsychol. 2020, 14, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Tainta, M.; Iriondo, A.; Ecay-Torres, M.; Estanga, A.; de Arriba, M.; Barandiaran, M.; Clerigue, M.; Garcia-Sebastian, M.; Villanua, J.; Izagirre, A.; et al. Brief Cognitive Tests as a Decision-Making Tool in Primary Care. A Population and Validation Study. Neurologia, 2022; in press. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia Prevention, Intervention, and Care: 2020 Report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Petersen, R.C.; Wiste, H.J.; Weigand, S.D.; Fields, J.A.; Geda, Y.E.; Graff-Radford, J.; Knopman, D.S.; Kremers, W.K.; Lowe, V.; Machulda, M.M.; et al. NIA-AA Alzheimer’s Disease Framework: Clinical Characterization of Stages. Ann. Neurol. 2021, 89, 1145–1156. [Google Scholar] [CrossRef]
- McKeith, I.G.; Ferman, T.J.; Thomas, A.J.; Blanc, F.; Boeve, B.F.; Fujishiro, H.; Kantarci, K.; Muscio, C.; O’Brien, J.T.; Postuma, R.B.; et al. Research Criteria for the Diagnosis of Prodromal Dementia with Lewy Bodies. Neurology 2020, 94, 743–755. [Google Scholar] [CrossRef] [PubMed]
- Gondim, D.D.; Oblak, A.; Murrell, J.R.; Richardson, R.; Epperson, F.; Ross, O.A.; Ghetti, B. Diffuse Lewy Body Disease and Alzheimer Disease: Neuropathologic Phenotype Associated with the PSEN1 p.A396T Mutation. J. Neuropathol. Exp. Neurol. 2019, 78, 585–594. [Google Scholar] [CrossRef]
- Altuna, M.; Olmedo-Saura, G.; Carmona-Iragui, M.; Fortea, J. Mechanisms Involved in Epileptogenesis in Alzheimer’s Disease and Their Therapeutic Implications. Int. J. Mol. Sci. 2022, 23, 4307. [Google Scholar] [CrossRef] [PubMed]
- Vanderschaeghe, G.; Schaeverbeke, J.; Bruffaerts, R.; Vandenberghe, R.; Dierickx, K. From Information to Follow-up: Ethical Recommendations to Facilitate the Disclosure of Amyloid PET Scan Results in a Research Setting. Alzheimer’s Dement. 2018, 4, 243–251. [Google Scholar] [CrossRef]
- Bosisio, F.; Sterie, A.-C.; Rubli Truchard, E.; Jox, R.J. Implementing Advance Care Planning in Early Dementia Care: Results and Insights from a Pilot Interventional Trial. BMC Geriatr. 2021, 21, 573. [Google Scholar] [CrossRef]
- Galvin, J.E.; Aisen, P.; Langbaum, J.B.; Rodriguez, E.; Sabbagh, M.; Stefanacci, R.; Stern, R.A.; Vassey, E.A.; de Wilde, A.; West, N.; et al. Early Stages of Alzheimer’s Disease: Evolving the Care Team for Optimal Patient Management. Front. Neurol. 2020, 11, 592302. [Google Scholar] [CrossRef]
- Smedinga, M.; Tromp, K.; Schermer, M.H.N.; Richard, E. Ethical Arguments Concerning the Use of Alzheimer’s Disease Biomarkers in Individuals with No or Mild Cognitive Impairment: A Systematic Review and Framework for Discussion. J. Alzheimer’s Dis. 2018, 66, 1309–1322. [Google Scholar] [CrossRef] [PubMed]
- Viloria Jiménez, M.A.; Chung Jaén, M.; Vigara García, M.; Barahona-Alvarez, H. Decision-Making in Older People with Dementia. Rev. Clin. Gerontol. 2013, 23, 307–316. [Google Scholar] [CrossRef]
- Demurtas, J.; Schoene, D.; Torbahn, G.; Marengoni, A.; Grande, G.; Zou, L.; Petrovic, M.; Maggi, S.; Cesari, M.; Lamb, S.; et al. Physical Activity and Exercise in Mild Cognitive Impairment and Dementia: An Umbrella Review of Intervention and Observational Studies. J. Am. Med. Dir. Assoc. 2020, 21, 1415–1422.e6. [Google Scholar] [CrossRef] [PubMed]
- Jaroudi, W.; Garami, J.; Garrido, S.; Hornberger, M.; Keri, S.; Moustafa, A.A. Factors Underlying Cognitive Decline in Old Age and Alzheimer’s Disease: The Role of the Hippocampus. Rev. Neurosci. 2017, 28, 705–714. [Google Scholar] [CrossRef]
- Fu, J.; Tan, L.-J.; Lee, J.E.; Shin, S. Association between the Mediterranean Diet and Cognitive Health among Healthy Adults: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 946361. [Google Scholar] [CrossRef]
- Scarmeas, N.; Stern, Y.; Mayeux, R.; Manly, J.J.; Schupf, N.; Luchsinger, J.A. Mediterranean Diet and Mild Cognitive Impairment. Arch. Neurol. 2009, 66, 216–225. [Google Scholar] [CrossRef]
- Ishikawa, K.M.; Davis, J.; Chen, J.J.; Lim, E. The Prevalence of Mild Cognitive Impairment by Aspects of Social Isolation. PLoS ONE 2022, 17, e0269795. [Google Scholar] [CrossRef]
- Kivipelto, M.; Solomon, A.; Ahtiluoto, S.; Ngandu, T.; Lehtisalo, J.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER): Study Design and Progress. Alzheimer’s Dement. 2013, 9, 657–665. [Google Scholar] [CrossRef]
- Stage, E.; Svaldi, D.; Sokolow, S.; Risacher, S.L.; Marosi, K.; Rotter, J.I.; Saykin, A.J.; Apostolova, L.G.; Initiative, for the Alzheimer’s Disease Neuroimaging Initiative. Prescribing Cholinesterase Inhibitors in Mild Cognitive Impairment—Observations from the Alzheimer’s Disease Neuroimaging Initiative. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2021, 7, e12168. [Google Scholar] [CrossRef]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice Guideline Update Summary: Mild Cognitive Impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Fink, H.A.; Jutkowitz, E.; McCarten, J.R.; Hemmy, L.S.; Butler, M.; Davila, H.; Ratner, E.; Calvert, C.; Barclay, T.R.; Brasure, M.; et al. Pharmacologic Interventions to Prevent Cognitive Decline, Mild Cognitive Impairment, and Clinical Alzheimer-Type Dementia: A Systematic Review. Ann. Intern. Med. 2018, 168, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, S. Aducanumab: First Approval. Drugs 2021, 81, 1437–1443. [Google Scholar] [CrossRef] [PubMed]
- Burlá, C.; Rego, G.; Nunes, R. Alzheimer, Dementia and the Living Will: A Proposal. Med. Health Care Philos. 2014, 17, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Vollmann, J. Advance Directives in Patients with Alzheimer’s Disease. Ethical and Clinical Considerations. Med. Health Care. Philos. 2001, 4, 161–167. [Google Scholar] [CrossRef]
- Porteri, C. Advance Directives as a Tool to Respect Patients’ Values and Preferences: Discussion on the Case of Alzheimer’s Disease. BMC Med. Ethics 2018, 19, 9. [Google Scholar] [CrossRef]
- Fazel, S.; Hope, T.; Jacoby, R. Assessment of Competence to Complete Advance Directives: Validation of a Patient Centred Approach. BMJ 1999, 318, 493–497. [Google Scholar] [CrossRef]
- Battin, M.P.; Kious, B.M. Ending One’s Life in Advance. Hastings Cent. Rep. 2021, 51, 37–47. [Google Scholar] [CrossRef]
- Sævareid, T.J.L.; Pedersen, R.; Magelssen, M. Positive Attitudes to Advance Care Planning—A Norwegian General Population Survey. BMC Health Serv. Res. 2021, 21, 762. [Google Scholar] [CrossRef]
- Ma, H.; Kiekhofer, R.E.; Hooper, S.M.; Dulaney, S.; Possin, K.L.; Chiong, W. Goals of Care Conversations and Subsequent Advance Care Planning Outcomes for People with Dementia. J. Alzheimer’s Dis. 2021, 83, 1767–1773. [Google Scholar] [CrossRef]
- Alcolea, D.; Delaby, C.; Muñoz, L.; Torres, S.; Estellés, T.; Zhu, N.; Barroeta, I.; Carmona-Iragui, M.; Illán-Gala, I.; Santos-Santos, M.Á.; et al. Use of Plasma Biomarkers for AT(N) Classification of Neurodegenerative Dementias. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1206–1214. [Google Scholar] [CrossRef]
- Lee, J. Mild Cognitive Impairment in Relation to Alzheimer’s Disease: An Investigation of Principles, Classifications, Ethics, and Problems. Neuroethics 2023, 16, 16. [Google Scholar] [CrossRef]
- Karlawish, J. Addressing the Ethical, Policy, and Social Challenges of Preclinical Alzheimer Disease. Neurology 2011, 77, 1487–1493. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, P.W.; Kerr, A.; Knudsen, L. The Stigma of Mental Illness: Explanatory Models and Methods for Change. Appl. Prev. Psychol. 2005, 11, 179–190. [Google Scholar] [CrossRef]
- Yang, L.H.; Kleinman, A.; Link, B.G.; Phelan, J.C.; Lee, S.; Good, B. Culture and Stigma: Adding Moral Experience to Stigma Theory. Soc. Sci. Med. 2007, 64, 1524–1535. [Google Scholar] [CrossRef]
- Link, B.G.; Phelan, J. Stigma Power. Soc. Sci. Med. 2014, 103, 24–32. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Larson, J.E.; Rüsch, N. Self-Stigma and the “Why Try” Effect: Impact on Life Goals and Evidence-Based Practices. World Psychiatry 2009, 8, 75–81. [Google Scholar] [CrossRef]
- Stites, S.D.; Harkins, K.; Rubright, J.D.; Karlawish, J. Relationships between Cognitive Complaints and Quality of Life in Older Adults with Mild Cognitive Impairment, Mild Alzheimer Disease Dementia, and Normal Cognition. Alzheimer Dis. Assoc. Disord. 2018, 32, 276–283. [Google Scholar] [CrossRef]
- Larson, J.E.; Corrigan, P. The Stigma of Families with Mental Illness. Acad. Psychiatry J. Am. Assoc. Dir. Psychiatr. Resid. Train. Assoc. Acad. Psychiatry 2008, 32, 87–91. [Google Scholar] [CrossRef]
- Benbow, S.M.; Jolley, D. Dementia: Stigma and Its Effects. Neurodegener. Dis. Manag. 2012, 2, 165–172. [Google Scholar] [CrossRef]
- Lynch, C. World Alzheimer Report 2019: Attitudes to Dementia, a Global Survey. Alzheimer’s Dement. 2020, 16, e038255. [Google Scholar] [CrossRef]
- Low, L.-F.; Purwaningrum, F. Negative Stereotypes, Fear and Social Distance: A Systematic Review of Depictions of Dementia in Popular Culture in the Context of Stigma. BMC Geriatr. 2020, 20, 477. [Google Scholar] [CrossRef] [PubMed]
- Lara, B.; Carnes, A.; Dakterzada, F.; Benitez, I.; Piñol-Ripoll, G. Neuropsychiatric Symptoms and Quality of Life in Spanish Patients with Alzheimer’s Disease during the COVID-19 Lockdown. Eur. J. Neurol. 2020, 27, 1744–1747. [Google Scholar] [CrossRef] [PubMed]
- Villarejo-Galende, A.; García-Arcelay, E.; Piñol-Ripoll, G.; Del Olmo-Rodríguez, A.; Viñuela, F.; Boada, M.; Franco-Macías, E.; de la Peña, A.I.; Riverol, M.; Puig-Pijoan, A.; et al. Awareness of Diagnosis in Persons with Early-Stage Alzheimer’s Disease: An Observational Study in Spain. Neurol. Ther. 2022, 11, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Beard, R.L.; Neary, T.M. Making Sense of Nonsense: Experiences of Mild Cognitive Impairment. Sociol. Health Illn. 2013, 35, 130–146. [Google Scholar] [CrossRef]
- Gauthier, S.; Rosa-Neto, P.; Morais, J.A.; Webster, C. World Alzheimer Report 2021: Journey through the Diagnosis of Dementia. Alzheimer’s Dis. Int. 2021, 2022, 30. [Google Scholar]
- Veerhuis, N.; Traynor, V. Evaluation of an Education Intervention for Australian Health Practitioners to Support People with Dementia with Driving Decisions: A Pretest-Posttest Survey. Traffic Inj. Prev. 2022, 23, 327–332. [Google Scholar] [CrossRef]
- Feng, S.; Yan, X.; Sun, H.; Feng, Y.; Liu, H.X. Intelligent Driving Intelligence Test for Autonomous Vehicles with Naturalistic and Adversarial Environment. Nat. Commun. 2021, 12, 748. [Google Scholar] [CrossRef]
- Connors, M.H.; Ames, D.; Woodward, M.; Brodaty, H. Mild Cognitive Impairment and Driving Cessation: A 3-Year Longitudinal Study. Dement. Geriatr. Cogn. Disord. 2017, 44, 63–70. [Google Scholar] [CrossRef]
- Pavlou, D.; Beratis, I.; Papantoniou, P.; Papadimitriou, E.; Golias, J.; Papageorgiou, S. Driving Performance Profiles of Drivers with Brain Pathologies in Rural Roads. Int. J. Transp. 2017, 5, 17–28. [Google Scholar] [CrossRef]
- Bhojak, T.; Jia, Y.; Jacobsen, E.; Snitz, B.E.; Chang, C.-C.H.; Ganguli, M. Driving Habits of Older Adults: A Population-Based Study. Alzheimer Dis. Assoc. Disord. 2021, 35, 250–257. [Google Scholar] [CrossRef]
- Hird, M.A.; Egeto, P.; Fischer, C.E.; Naglie, G.; Schweizer, T.A. A Systematic Review and Meta-Analysis of On-Road Simulator and Cognitive Driving Assessment in Alzheimer’s Disease and Mild Cognitive Impairment. J. Alzheimer’s Dis. 2016, 53, 713–729. [Google Scholar] [CrossRef]
- Stamatelos, P.; Economou, A.; Stefanis, L.; Yannis, G.; Papageorgiou, S.G. Driving and Alzheimer’s Dementia or Mild Cognitive Impairment: A Systematic Review of the Existing Guidelines Emphasizing on the Neurologist’s Role. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2021, 42, 4953–4963. [Google Scholar] [CrossRef] [PubMed]
- Drazkowski, J.F.; Sirven, J.I. Driving and Neurologic Disorders. Neurology 2011, 76, S44–S49. [Google Scholar] [CrossRef] [PubMed]
- Economou, A.; Pavlou, D.; Beratis, I.; Andronas, N.; Papadimitriou, E.; Papageorgiou, S.G.; Yannis, G. Predictors of Accidents in People with Mild Cognitive Impairment, Mild Dementia Due to Alzheimer’s Disease and Healthy Controls in Simulated Driving. Int. J. Geriatr. Psychiatry 2020, 35, 859–869. [Google Scholar] [CrossRef]
- Molinuevo, J.L.; Gramunt, N.; Gispert, J.D.; Fauria, K.; Esteller, M.; Minguillon, C.; Sánchez-Benavides, G.; Huesa, G.; Morán, S.; Dal-Ré, R.; et al. The ALFA Project: A Research Platform to Identify Early Pathophysiological Features of Alzheimer’s Disease. Alzheimer’s Dement. 2016, 2, 82–92. [Google Scholar] [CrossRef]
- Ma, W.; Zhu, L.; Tang, J.; Diao, W.; Qian, L.; Feng, X.; Zhang, X. Testing the Knowledge of Alzheimer’s Disease via an Intervention Study among Community Health Service Center Staff in Jiaxing, China. Front. Public Health 2022, 10, 969653. [Google Scholar] [CrossRef]
- Yang, T.; Huang, Y.; Li, X.; Li, M.; Ma, S.; Xuan, G.; Jiang, Y.; Sun, S.; Yang, Y.; Wu, Z.; et al. Knowledge, Attitudes, and Stigma Related to Dementia Among Illiterate and Literate Older Adults in Shanghai. Risk Manag. Healthc. Policy 2021, 14, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, S.; Leuzy, A.; Racine, E.; Rosa-Neto, P. Diagnosis and Management of Alzheimer’s Disease: Past, Present and Future Ethical Issues. Prog. Neurobiol. 2013, 110, 102–113. [Google Scholar] [CrossRef]
- Prince, M.; Ali, G.-C.; Guerchet, M.; Prina, A.M.; Albanese, E.; Wu, Y.-T. Recent Global Trends in the Prevalence and Incidence of Dementia, and Survival with Dementia. Alzheimer’s Res. Ther. 2016, 8, 23. [Google Scholar] [CrossRef]
- The American Geriatrics Society Expert Panel on Person-Centered Care. Person-Centered Care: A Definition and Essential Elements. J. Am. Geriatr. Soc. 2016, 64, 15–18. [Google Scholar] [CrossRef]
- Bamford, C.; Wheatley, A.; Brunskill, G.; Booi, L.; Allan, L.; Banerjee, S.; Harrison Dening, K.; Manthorpe, J.; Robinson, L.; on behalf of the PriDem study team. Key Components of Post-Diagnostic Support for People with Dementia and Their Carers: A Qualitative Study. PLoS ONE 2021, 16, e0260506. [Google Scholar] [CrossRef] [PubMed]
- Bacsu, J.-D.R.; O’Connell, M.E.; Wighton, M.B. Improving the Health Equity and the Human Rights of Canadians with Dementia through a Social Determinants Approach: A Call to Action in the COVID-19 Pandemic. Can. J. Public Health 2022, 113, 204–208. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Future Perspective |
|---|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López, C.; Altuna, M. New Community and Sociohealth Challenges Arising from the Early Diagnosis of Mild Cognitive Impairment (MCI). J. Pers. Med. 2023, 13, 1410. https://doi.org/10.3390/jpm13091410
López C, Altuna M. New Community and Sociohealth Challenges Arising from the Early Diagnosis of Mild Cognitive Impairment (MCI). Journal of Personalized Medicine. 2023; 13(9):1410. https://doi.org/10.3390/jpm13091410
Chicago/Turabian StyleLópez, Carolina, and Miren Altuna. 2023. "New Community and Sociohealth Challenges Arising from the Early Diagnosis of Mild Cognitive Impairment (MCI)" Journal of Personalized Medicine 13, no. 9: 1410. https://doi.org/10.3390/jpm13091410
APA StyleLópez, C., & Altuna, M. (2023). New Community and Sociohealth Challenges Arising from the Early Diagnosis of Mild Cognitive Impairment (MCI). Journal of Personalized Medicine, 13(9), 1410. https://doi.org/10.3390/jpm13091410