Abstract
Background: Crowding is the most frequent malocclusion in orthodontics, with a strong hereditary tendency. It already occurs in pediatric age and is mainly hereditary. It is a sign of a lack of space in the arches, and is not self-correcting, but can worsen over time. The main cause of the worsening of this malocclusion is a progressive and physiological decrease in the arch perimeter. Methods: To identify relevant studies investigating the most common possible treatments for mandibular dental crowding, a comprehensive search of PubMed, Scopus and Web of Science was conducted encompassing the last 5 years (2018–2023) using the following MeSH: “mandibular crowding AND treatment” and “mandibular crowding AND therapy “. Results: A total of 12 studies were finally included. An orthodontic treatment cannot ignore the concept of “guide arch”, which concerns the lower arch, because of the objective difficulty in increasing its perimeter; the bone structure of the lower jaw is more compact than that of the upper one. Its expansion, in fact, is limited to a slight vestibularization of the incisors and lateral sectors that may be associated with a limited distalization of the molars. Conclusions: There are various therapeutic solutions available to the orthodontist, and a correct diagnosis through clinical examination, radiographs and model analysis are essential. The decision of how to deal with crowding cannot be separated from an overall assessment of the malocclusion to be treated.
1. Introduction
Crowding is a common orthodontic malocclusion with a strong hereditary tendency. It is caused by a variety of factors, including the impact of environmental and genetic factors on dental arch dimensions [1]. Dental crowding is defined as an inconsistency between tooth size and arch dimension that results in malocclusion; it occurs because of a lack of coordination between tooth size and arch dimensions [2,3,4,5]. The lower incisors are the teeth most frequently involved [6,7,8] (Figure 1).

Figure 1.
Crowding of the permanent mandibular incisors.
Studies show that 46 per cent of children between 6 and 12 years old and 85% of children between 12 and 17 years old have crowding. This is because, if action is not taken, leeway space is lost, and consequently, a mild and easily resolved crowding in mixed dentition becomes stable and significant in permanent dentition [9,10,11,12]. During the third phase of the permutation, when deciduous canines and molars are replaced by permanent canines and premolars, there is a decrease in the length of the dental arch perimeter. The maximum increase in size of both dental arches occurs in the first 2 years of life; after that, the arch length increases up to 13 years in the maxilla and up to 8 years in the mandible; after this age, length decreases in both arches [13]. Crowding is thus considered a malocclusion that never self-corrects and instead worsens over time [14,15,16,17]. If present in deciduous teeth, it will worsen over the next two dental stages [18,19,20]. It generally involves 50% of individuals who were exempt in the first decade of life [21]. An orthodontic treatment cannot ignore the concept of the “guide arch”, which concerns the lower one, because of the objective difficulty in increasing its perimeter; the bone structure of the lower jaw is more compact than that of the upper one. The identification of factors that contribute to mandibular tooth crowding in mixed dentition is critical for treatment planning [22]. Several factors can be assumed to affect the development and severity of crowding, such as the direction of mandibular growth, the early loss of deciduous molars, mesiodistal tooth and arch dimensions, oral and perioral musculature and incisor and molar inclination [23]. The correction of severe mandibular crowding in mixed dentition could be carried out by extraction, distalization and surgical and non-surgical expansion of the mandible [18,24]. It is useful to emphasize that the clinician is confronted not only with crowding but also with clinical situations that are predictive of it or represent a different aspect, such as the lack of diastemas in deciduous dentition, the early loss of deciduous canines, the loss of arch length due to destructive caries, the early loss of the deciduous second molar, the appearance of teeth in ectopic position and protrusion or the accentuated retrusion of the incisors [25]. The early detection of mandibular teeth crowding is critical for interceptive orthodontic treatment planning. The aim of this study is to analyze the diagnostic methods and the treatment possibilities to solve mandibular crowding in mixed dentition.
2. Materials and Methods
2.1. Protocol and Registration
A literature review was conducted using PRISMA Extension for Scoping Reviews (PRISMA-ScR) [26].
2.2. Search Processing
To identify relevant studies investigating the most common possible treatments for mandibular dental crowding, a comprehensive search of PubMed, Scopus and Web of Science (WOS) was conducted encompassing the last 5 years (2018–2023). The following Boolean keywords were incorporated into the search strategy because they perfectly matched the aim of the investigation, which primarily focuses on the possible treatments for mandibular dental crowding: (“mandibular crowding AND treatment”) and (“mandibular crowding AND therapy”).
2.3. Eligibility Criteria
The inclusion criteria were as follows: (1) human in vivo study; (2) English language; (3) open access studies; (4) clinical studies and (5) studies analyzing the variety of therapies for mandibular dental crowding. The review followed the PICO criteria: P (patients with mandibular crowding), I (causes and treatment), C (absence of mandibular crowding) and O (efficacy of treatment options).
The exclusion criteria were as follows: (1) animal and/or in vitro studies; (2) other languages different from English; (3) not open access studies; (4) case report/series, reviews, editorials and book chapters and (5) research about diagnostic aspects of dental crowding.
2.4. Data Processing
Autor disagreements on the choice in articles were discussed and settled.
3. Results
The initial search provided a total of 833 items (PubMed n = 310, Scopus n = 282, WOS n = 241), and 346 articles remained after removing duplicates. A total of 74 articles accessed the screening phase, while 272 items were removed because 27 represented reviews, 3 were book chapters, 31 were not free full text, 3 were not in vivo, 73 were case report/series and 135 were off topic. From these products, 62 articles were additionally removed due to lack of interest in shown data, and eligibility was assigned to 12 records which were finally involved in the inclusion phase (Figure 2). Results of each study are reported in Table 1.
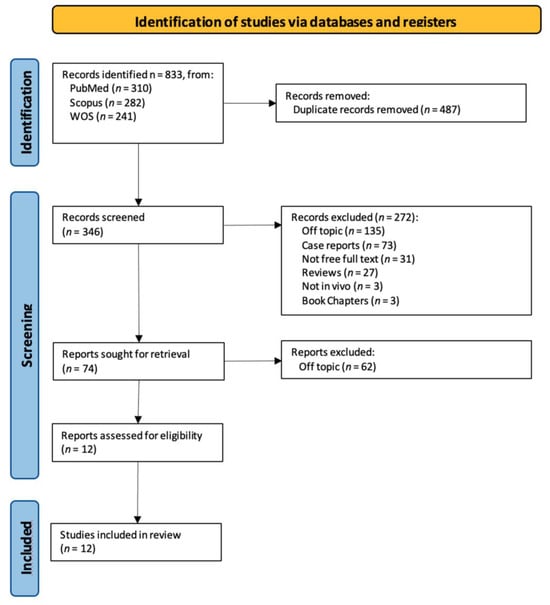
Figure 2.
PRISMA ScR flowchart.

Table 1.
Results table.
4. Discussion
The mandible is considered the guide arch in crowding treatment since it is the less modifiable arch [2]. In the following paragraphs, the diagnostic methods, followed by the strategies and stability of the treatment of mandibular crowding, are described.
4.1. Diagnostic Methods
Regarding the diagnosis, the lack of space in the primary dentition is a predictor to crowding. The inability to accommodate the size difference between the primary and permanent incisors is also due to a “closed” primary dentition, which prevents the mesial shift in the erupting permanent molars into a class I molar relationship during the closing of the private space [27]. Measurements for diagnosing crowding are usually taken on the plaster model with a digital caliper, both before and after treatment. Tooth size is the sum of the mesiodistal diameters of all teeth [27]. Arch length is calculated as the perpendicular distance between a line that connects the medial contact point of the first permanent molars and the most vestibular point between the lower central incisors. Crowding is measured as the difference between tooth size and arch length [27]. As result, crowding is associated with both bigger teeth and a smaller dental arch. The degree of crowding is influenced by the direction of mandibular development, early loss of primary molars, arch size, oral musculature and incisor and molar inclination [22]. Many studies have found a correlation between crowding and the direction of mandibular rotation. Extreme mandibular rotation has been linked to increased crowding, and crowding is also brought on by some growth/skeletal patterns at the start of adolescence [28]. Other factors that should not be underestimated for the diagnosis of crowding are the changes in facial morphology brought on by growth or orthodontic treatment [37]. Dental crowding is also caused by several reasons, including the impact of environmental and genetic variables on dental arch measurements such arch width, arch length and arch perimeter. Further factors influencing mesiodistal tooth width include racial characteristics, sex and inherited traits [18]. Lateral cephalograms can be used for skeletal parameters contributing to dental crowding such as effective maxillary and mandibular length, mandibular plane angle, Y axis, lower anterior face height and dental parameters such as axial inclination of the lower incisor, inclination of the lower incisor to the mandibular plane and interincisal angle [38]. Some authors have found that the use of 2D lateral cephalograms or profile photos for orthodontic measurements may not be adequately accurate. Three-dimensional computed tomography provides better frontal and three-quarter profile data for diagnosis, allowing structures to be precisely measured, aiding in analysis and diagnosis [18]. A template applied for the measurement of crowding is Little’s Irregularity Index. It denotes the total linear displacement of the six mandibular anterior teeth’s anatomical contact locations, represented in millimeters: 0 indicates perfect alignment, 1–3 mm indicates the least amount of irregularity, 4–6 mm indicates moderate abnormality, 7–9 mm indicates severe irregularity and 10 mm or more indicates very severe misalignment [30]. For treatment planning, it is crucial to identify the causes of anterior mandibular tooth crowding in mixed dentition [22]. If malocclusion is characterized by a deep bite, the cause could be skeletal, dental or both [39].
Two clinical disorders can coexist as a result of altered tooth eruption, which is the failure of a tooth to erupt into the proper location in the arch: transmigration and inclusion [40].
4.2. Prophylaxis
Primary dentition is essential for influencing the eruption of permanent teeth. Early primary tooth loss can result in undesired tooth motions and space loss in the permanent dentition [2].
It is recommended to maintain the primary dentition in the arch until exfoliation; nevertheless, if early loss is inevitable, it should be managed to minimize the negative consequences on the developing occlusion [23].
Space maintainers can be utilized for this purpose.
Early primary molar loss might result in a reduction in arch length, increasing the severity of crowding/malocclusion; therefore, in the affected patient, every effort should be made to preserve the natural leeway space [29]. The unilateral loss of a primary canine or first molar can result in a significant centerline disparity and mesial migration of the buccal segments, which is another critical clinical condition to preserve space [38]. Space maintainers are classified into three types: fixed unilateral appliances, fixed bilateral appliances and removable partial dentures. The band and loop space maintainer is one of the most prevalent permanent unilateral appliances [34]. The appliance has a band that cements to the primary second molar. It also has a loop that contacts the distal surface of the primary canine [2].
The distal shoe is another permanent unilateral appliance. A stainless-steel wire extends in front of the unerupted permanent first molar to guide it into position as it grows in. Distal shoes can only be placed on one tooth [2].
Bilateral space maintainers are used once teeth on both sides of the mouth are lost. Common types include Lingual Holding Arch, Nance Arch and Transpalatal Arch.
Removable dentures are often used for cosmetic purposes rather than to avoid space loss, particularly when anterior (front) teeth are lost [2].
4.3. Treatment
The lower jaw is considered the guiding arch in crowding therapy because it is difficult to modify its perimeter due to the more compact bone structure and the continuity with the mandibular branch, which does not allow for distalization [37,41]. In addition, the symphysis cartilage ossifies in the first year of life, so it is not possible to perform an orthopedic bone expansion, as in the upper jaw, working at the level of the median palatine suture [41,42]. The modalities of space recovery in mixed dentition are: arch perimeter increment, reduction in mesiodistal widths of teeth and serial extractions [2,43,44]. In the upper arch, the expansions are quite stable, but inferiorly, it is universally recognized that the expansion of the intercanine diameter always recurs, whereas expansion at the molar level is quite stable, which should be considered [27,45,46,47]. The space that can be recovered in the lower arch depends on the type of sector: in general, in the posterior sector, utilizing a lip bumper-style device, it is possible to recover a maximum of 2 mm of space per molar distalization in the posterior regions. At the molar level in the lateral sectors, the arch length could increase by about 0.4 mm; at the canine level, the arch length increases about 0.7 mm [48]. The vestibularization of one millimeter of the incisal margin in the anterior sector results in the gain of one millimeter of arch space, or roughly a ratio of one to one (changing the arch form) [47]. Schwarz’s appliance (Figure 3) and lip bumper (Figure 4) are two commonly used appliances for increasing lower dental arch dimensions [49]. In their study, Vincenzo Quinzi et al. compared the effects of these appliances on reducing mandibular crowding by increasing lower arch dimensions [27]. The study included twenty subjects (10 males and 10 females). Ten patients were treated with Schwarz’s appliance, and ten with lip bumper. The Schwarz appliance was more effective in increasing intercanine arch dimensions and arch perimeter, although the lip bumper reached a greater increase in arch length [27]. Since the 1970s, there have been reports of spontaneous changes in mandibular dentition caused by maxillary expansion [31,50]. Di Ventura et al. assessed the consequences of rapid maxillary expansion (RME) anchored to primary molars on the mandibular arch. A total of 54 patients were recruited for this study and divided into two groups: a test group (21 patients, 7.4 ± 1.2 years) who underwent RME, and a control group (17 patients, 7.3 ± 1.1 years old) who did not receive any treatment. The results of this study showed a significant increase in interdental width in the lower arch after 9 months of RME therapy [31]. Olivia Griswold et al. evaluated the changes in sagittal mandibular incisors’ position in response to lip bumper therapy using CBCT [32]. In this study, the authors compared a group that was treated only with rapid maxillary expansion (experimental group) and an RME + LB (lip bumper) group (control group) [32]. The CBCTs were placed in 3D on the mandibular structure, and the angular and linear alterations in the mandibular incisors throughout LB therapy were assessed. In the investigation, there was no statistically significant difference in the degree of mandibular incisor protrusion between the two groups; the lip bumper did not generate substantial proclination, protrusion or extrusion of the mandibular incisors. [13]. Air-rotor stripping (ARS) (Figure 5) is a technique for creating space during the mixed dentition period by reducing interproximal enamel thickness. Yahya B. Nakhjavani et al. assessed the efficacy of the mesial stripping of mandibular deciduous canines for the correction of rotated and lingually erupted lateral incisors in 42 patients with <3 mm mandibular crowding [33]. In this study, the mesial stripping of mandibular primary canines resulted in full crowding correction; in just few cases, the amount of crowding did not reach zero, and a small crowding in the range of 0.06 to 0.1 mm remained [33]. The extraction of all the first premolars with subsequent orthodontic treatment is the most used method to relieve dental crowding [51]. The importance and timing of extraction as a component of orthodontic therapy for late incisor crowding have been well investigated [35]. No difference in late incisor crowding is shown by the data, regardless of whether serial extraction or early or late premolar extraction is performed prior to orthodontic treatment. Additionally, selecting a non-extraction orthodontic procedure has been linked to post-retention crowding [35]. Maurits Persson et al. investigated changes in the mandibular incisor area from early adolescence to late adulthood in patients with a class I crowding malocclusion treated in the mixed dentition by the extraction of all first premolars without subsequent orthodontic treatment [35]. The extraction group included 24 subjects who had all their first premolars extracted at a mean age of about 11.5 years to treat a class I space deficiency malocclusion. The control group included 21 subjects who had normal occlusions at the age of 13 years [35]. The extraction group showed no improvements in lower incisor irregularity, and a significant increase in lower tooth space insufficiency into adulthood. Lower incisor irregularity and space shortage developed significantly in the control group throughout late adulthood [35]. Premolar extraction is the sole treatment option for severe crowding in a class I occlusion, allowing for spontaneous adjustments and more stable incisor alignment in late adulthood, according to the authors [35] (Table 2).

Figure 3.
Schwarz’s appliance.

Figure 4.
Lip bumper.

Figure 5.
Air-rotor stripping (ARS).
Table 2.
Summary table.
4.4. Treatment Stability
Long-term stability after orthodontic treatment is a challenge for orthodontists. The retention of lower incisors after alignment is variable, and the severity of the relapse may not be predicted precisely. In the literature, it has been reported that post-treatment relapse occurs in 70% of cases [34]. The dental arches are parts of the organism under constant movement and load during their function. In a situation of balance, the shape of the dental arch remains normal. When tensegrity is lost, a new shape is obtained to gain the new balanced position. Tooth alignment is always accompanied by an increase in intercanine width or protrusion, unless interproximal reduction or extractions are performed [34,35]. Some authors have suggested that the post-treatment position of mandibular incisors may be influenced by several factors, such as initial crowding, treatment procedures, patient cooperation and soft tissue growth [34,35,36]. Outcome and stability between cases treated without extraction and cases treated with extraction of a mandibular incisor or mandibular premolars were assessed by Mahmoudzadeh et al. The study showed that there was no significant correlation between treatment modality and changes in the incisor alignment post-retention. In a retrospective study by Purva Verma et al., 32 subjects treated for mandibular dental crowding were examined at 1 year of follow up. Patients treated with passive self-ligation non-extraction protocol showed worse stability in intercanine width and changes in lower incisor inclination than patients treated with conventional ligation lower incisor extraction protocol [34]. It is likely that arch width and length decrease over time, probably due to the mesial drift of the posterior teeth [34]. In a 50-year case-control study, a comparison between patients undergoing extraction of all first premolars in early adolescence and untreated subjects with a normal alignment was carried out. According to this study, patients treated with extractions showed better stability in lower alignment into late adulthood than untreated subjects, who developed lower incisor crowding with age [35]. Barbert et al. stated that the post-treatment 3 × 3 bonded retainer is useful to prevent the relapse of mandibular crowding. Sixteen patients treated with mandibular incisor extraction were examined at 1 year of follow up: patients without a retainer showed a significant relapse when compared to the retainer group [36].
This review has some limitations. The studies found are few and heterogeneous. Furthermore, it is an analysis conducted over a period of five years. Finally, there was no assessment of the quality of the studies.
5. Conclusions
In dental crowding therapy, it is important to quantify the lack of space in the dental arch in order to choose an appropriate orthodontic therapy. A correct diagnosis is obtained through clinical examination, X-rays, cephalometric analysis and study models. CBCT provides additional support for the diagnosis. The mandible is considered the guiding arch in orthodontic therapy, as it is not very modifiable. The correction of severe mandibular crowding in mixed dentition can be achieved by extraction, distalization and surgical and non-surgical expansion of the mandible. The degree of crowding is influenced by the direction of mandibular development, early loss of primary molars, arch size, buccal musculature and the inclination of the incisors and molars. In mixed dentition, there are various ways to recover space that can be combined: maintaining the leeway space, lengthening the arch perimeter, resorting to extractions, stripping, etc. Decisions on crowding management must be made in the context of an overall assessment of the malocclusion to be treated.
Author Contributions
Conceptualization, A.P., A.M.I., C.L., N.D.L. and A.D.I.; Methodology, D.A., G.G., M.D., S.D. and G.M.T.; Software, D.A., A.D.I., A.M., G.L., D.D.V., G.D., V.C. and G.M.; Validation, C.L., F.I., G.M.T. and D.D.V.; Formal analysis, A.P., N.D.L., A.M.I., A.D.I. and A.M.; Resources, G.L., A.M.I., G.D. and D.D.V.; Data curation, G.D., D.D.V., G.M.T. and F.I.; Writing—original draft preparation, A.M.I., M.D. and G.M.; Writing—review and editing, A.P., G.G., V.C., G.L. and A.M.I.; Visualization, G.L., A.M., G.D., S.D. and G.M.; Supervision, A.P., G.D., F.I. and G.M.; Project administration, G.M., F.I. and G.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| RME | Rapid maxillary expansion |
| LB | Lip bumper |
| ARS | Air-rotor stripping |
| CBCT | Cone beam computed tomography |
References
- Normando, D.; Almeida, M.A.O.; Quintão, C.C.A. Dental Crowding. Angle Orthod. 2013, 83, 10–15. [Google Scholar] [CrossRef]
- Jadhav, V.; Tiwari, M.; Seegavadi, V.; Kamble, R.; Daigavane, P. A Formula for Estimating the Mesiodistal Width of Permanent Mandibular Central Incisors. J. Datta Meghe Inst. Med. Sci. Univ. 2021, 16, 29–32. [Google Scholar] [CrossRef]
- Rizzo, C.; Di Bartolo, I.; Santantonio, M.; Coscia, M.F.; Monno, R.; De Vito, D.; Ruggeri, F.M.; Rizzo, G. Epidemiological and Virological Investigation of a Norovirus Outbreak in a Resort in Puglia, Italy. BMC Infect. Dis. 2007, 7, 135. [Google Scholar] [CrossRef]
- De Vito, D.; Monno, R.; Nuccio, F.; Legretto, M.; Oliva, M.; Coscia, M.F.; Dionisi, A.M.; Calia, C.; Capolongo, C.; Pazzani, C. Diffusion and Persistence of Multidrug Resistant Salmonella Typhimurium Strains Phage Type DT120 in Southern Italy. BioMed Res. Int. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Coscia, M.F.; Monno, R.; Ballini, A.; Mirgaldi, R.; Dipalma, G.; Pettini, F.; Cristallo, V.; Inchingolo, F.; Foti, C.; De Vito, D. Human Papilloma Virus (HPV) Genotypes Prevalence in a Region of South Italy (Apulia). Ann. Dell’istituto Super. Di Sanita 2015, 51, 248–251. [Google Scholar] [CrossRef]
- Paul, S.; Garg, S.; Saraf, B.G.; Sheoran, N.; Chawla, M.; Saji, S.E. Arch Measurements, Bigonial Width, Dental Caries, and Their Effect on Occurrence of Mandibular Incisors Crowding in Early Mixed Dentition Period. Int. J. Clin. Pediatr. Dent. 2021, 14, S57–S62. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef]
- Maspero, C.; Fama, A.; Cavagnetto, D.; Abate, A.; Farronato, M. Treatment of Dental Dilacerations. J. Biol. Regul. Homeost. Agents 2019, 33, 1623–1627. [Google Scholar]
- Grainger, R.M. Orthodontic Treatment Priority Index; Vital Health Stat 2; United States Department of Health, Education, and Welfare: Washington, DC, USA, 1967; pp. 1–49. [Google Scholar]
- Cazzolla, A.P.; Zhurakivska, K.; Ciavarella, D.; Lacaita, M.G.; Favia, G.; Testa, N.F.; Marzo, G.; La Carbonara, V.; Troiano, G.; Lo Muzio, L. Primary Hyperoxaluria: Orthodontic Management in a Pediatric Patient: A Case Report. Spec. Care Dent. 2018, 38, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Lo Russo, L.; Ciavarella, D.; Salamini, A.; Guida, L. Alignment of Intraoral Scans and Registration of Maxillo-Mandibular Relationships for the Edentulous Maxillary Arch. J. Prosthet. Dent. 2019, 121, 737–740. [Google Scholar] [CrossRef]
- Cassano, M.; Russo, G.; Granieri, C.; Ciavarella, D. Modification of Growth, Immunologic and Feeding Parameters in Children with OSAS after Adenotonsillectomy. Acta Otorhinolaryngol. Ital. 2018, 38, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Abate, A.; Inchingolo, F.; Dolci, C.; Cagetti, M.G.; Tartaglia, G.M. Incidental Finding in Pre-Orthodontic Treatment Radiographs of an Aural Foreign Body: A Case Report. Children 2022, 9, 421. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.; Maspero, C.; Abate, A.; Grippaudo, C.; Connelly, S.T.; Tartaglia, G.M. 3D Cephalometry on Reduced FOV CBCT: Skeletal Class Assessment through AF-BF on Frankfurt Plane-Validity and Reliability through Comparison with 2D Measurements. Eur. Radiol. 2020, 30, 6295–6302. [Google Scholar] [CrossRef]
- Ergoren, M.C.; Paolacci, S.; Manara, E.; Dautaj, A.; Dhuli, K.; Anpilogov, K.; Camilleri, G.; Suer, H.K.; Sayan, M.; Tuncel, G.; et al. A Pilot Study on the Preventative Potential of Alpha-Cyclodextrin and Hydroxytyrosol against SARS-CoV-2 Transmission. Acta Bio Med. Atenei Parm. 2020, 91, e2020022. [Google Scholar] [CrossRef]
- Maspero, C. Operculectomy and Spontaneous Eruption of Impacted Second Molars: A Retrospective Study. J. Biol. Regul. Homeost. Agents 2019, 33, 1909–1912. [Google Scholar] [CrossRef]
- Maspero, C.; Cappella, A.; Dolci, C.; Cagetti, M.G.; Inchingolo, F.; Sforza, C. Is Orthodontic Treatment with Microperforations Worth It? A Scoping Review. Children 2022, 9, 208. [Google Scholar] [CrossRef]
- Das, P.J.; Dkhar, W.; Pradhan, A. An Evaluation of Dental Crowding in Relation to the Mesiodistal Crown Widths and Arch Dimensions in Southern Indian Population. J. Clin. Diagn. Res. 2017, 11, TC10–TC13. [Google Scholar] [CrossRef] [PubMed]
- Ciavarella, D.; Monsurrò, A.; Padricelli, G.; Battista, G.; Laino, L.; Perillo, L. Unilateral Posterior Crossbite in Adolescents: Surface Electromyographic Evaluation. Eur. J. Paediatr. Dent. 2012, 13, 25–28. [Google Scholar]
- Inchingolo, A.M.; Fatone, M.C.; Malcangi, G.; Avantario, P.; Piras, F.; Patano, A.; Di Pede, C.; Netti, A.; Ciocia, A.M.; De Ruvo, E.; et al. Modifiable Risk Factors of Non-Syndromic Orofacial Clefts: A Systematic Review. Children 2022, 9, 1846. [Google Scholar] [CrossRef] [PubMed]
- Brunelle, J.A.; Bhat, M.; Lipton, J.A. Prevalence and Distribution of Selected Occlusal Characteristics in the US Population, 1988–1991. J. Dent. Res. 1996, 75, 706–713. [Google Scholar] [CrossRef]
- Jain, R. Prevalence of Mandibular Anterior Teeth Crowding in Mixed Dentition Subjects Reporting to a University Hospital in Chennai City. Int. J. Dent. Oral Sci. 2019, S3, 6–11. [Google Scholar] [CrossRef]
- Grippaudo, M.M.; Quinzi, V.; Manai, A.; Paolantonio, E.G.; Valente, F.; La Torre, G.; Marzo, G. Orthodontic Treatment Need and Timing: Assessment of Evolutive Malocclusion Conditions and Associated Risk Factors. Eur. J. Pediatr. Dent. 2020, 21, 203–208. [Google Scholar] [CrossRef]
- Farronato, M.; Boccalari, E.; Del Rosso, E.; Lanteri, V.; Mulder, R.; Maspero, C. A Scoping Review of Respirator Literature and a Survey among Dental Professionals. Int. J. Environ. Res. Public Health 2020, 17, 5968. [Google Scholar] [CrossRef]
- Leighton, B.C. The Early Signs of Malocclusion. Eur. J. Orthod. 2007, 29, i89–i95. [Google Scholar] [CrossRef]
- Quinzi, V.; Caruso, S.; Mummolo, S.; Nota, A.; Angelone, A.M.; Mattei, A.; Gatto, R.; Marzo, G. Evaluation of Lower Dental Arch Crowding and Dimension after Treatment with Lip Bumper versus Schwarz Appliance. A Prospective Pilot Study. Dent. J. 2020, 8, 34. [Google Scholar] [CrossRef]
- Jain, R. Association Of Mandibular Arch Crowding And Vertical Growth Pattern—A Retrospective Study. Int. J. Dent. Oral Sci. 2021, 8, 4096–4100. [Google Scholar] [CrossRef]
- Satra, P.; Vichare, G.; Bhosale, V. Relationship of Maxillary and Mandibular Effective Base Length, Arch Length and Dental Crowding in Different Vertical Growth Pattern. APOS 2022, 12, 108–114. [Google Scholar] [CrossRef]
- Antoszewska-Smith, J.; Bohater, M.; Kawala, M.; Sarul, M.; Rzepecka-Skupień, M. Treatment of Adults with Anterior Mandibular Teeth Crowding: Reliability of Little’s Irregularity Index. Int. J. Dent. 2017, 2017, 5057941. [Google Scholar] [CrossRef]
- Di Ventura, A.; Lanteri, V.; Farronato, G.; Gaffuri, F.; Beretta, M.; Lanteri, C.; Cossellu, G. Three-Dimensional Evaluation of Rapid Maxillary Expansion Anchored to Primary Molars: Direct Effects on Maxillary Arch and Spontaneous Mandibular Response. Eur. J. Pediatr. Dent. 2019, 20, 38–42. [Google Scholar] [CrossRef]
- Griswold, O.; Li, C.; Orr, J.; Boucher, N.; Shah, S.; Chung, C.-H. Lip Bumper Therapy Does Not Influence the Sagittal Mandibular Incisor Position in a Retrospective CBCT Study. J. Clin. Med. 2022, 11, 6032. [Google Scholar] [CrossRef] [PubMed]
- Nakhjavani, Y.B.; Nakhjavani, F.B.; Jafari, A. Mesial Stripping of Mandibular Deciduous Canines for Correction of Permanent Lateral Incisors. Int. J. Clin. Pediatr. Dent. 2017, 10, 229–233. [Google Scholar] [CrossRef]
- Verma Comparative Evaluation of Stability of Mandibular Anterior Crowding Correction Done with Two Different Treatment Protocols: A Retrospective Study. Available online: https://www.jioh.org/article.asp?issn=0976-7428;year=2022;volume=14;issue=2;spage=189;epage=194;aulast=Verma (accessed on 24 January 2023).
- Persson, M.; Al-Taai, N.; Pihlgren, K.; Westerlund, A. Early Extractions of Premolars Reduce Age-Related Crowding of Lower Incisors: 50 Years of Follow-Up. Clin. Oral Investig. 2022, 26, 4525–4535. [Google Scholar] [CrossRef]
- Berbert, M.; Cotrin, P.; de Oliveira, R.G.; de Oliveira, R.G.; Valarelli, F.P.; de Freitas, M.R.; Freitas, K.M.S. The Influence of 3x3 Bonded Retainer on Anterior Crowding Relapse in Mandibular Incisor Extraction Cases. Dent. Press J. Orthod. 2021, 26, e212081. [Google Scholar] [CrossRef] [PubMed]
- Janson, G.; Goizueta, O.E.F.M.; Garib, D.G.; Janson, M. Relationship between Maxillary and Mandibular Base Lengths and Dental Crowding in Patients with Complete Class II Malocclusions. Angle Orthod. 2011, 81, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Shivaprakash, G. To Evaluate the Correlation Between Skeletal and Dental Parameters to the Amount of Crowding in Class II Div. 1 Malocclusions. J. Clin. Diagn. Res. 2017, 11, ZC22–ZC27. [Google Scholar] [CrossRef]
- Pasciuti, E.; Coloccia, G.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Bordea, I.R.; Cardarelli, F.; Di Venere, D.; Inchingolo, F.; Dipalma, G. Deep Bite Treatment with Aligners: A New Protocol. Appl. Sci. 2022, 12, 6709. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Carpentiere, V.; Piras, F.; Netti, A.; Ferrara, I.; Campanelli, M.; Latini, G.; Viapiano, F.; Costa, S.; Malcangi, G.; et al. Orthodontic Surgical Treatment of Impacted Mandibular Canines: Systematic Review and Case Report. Appl. Sci. 2022, 12, 8008. [Google Scholar] [CrossRef]
- Tepedino, M.; Iancu-Potrubacz, M.; Ciavarella, D.; Masedu, F.; Marchione, L.; Chimenti, C. Expansion of Permanent First Molars with Rapid Maxillary Expansion Appliance Anchored on Primary Second Molars. J. Clin. Exp. Dent. 2018, 10, e241–e247. [Google Scholar] [CrossRef]
- Ciavarella, D.; Tepedino, M.; Chimenti, C.; Troiano, G.; Mazzotta, M.; Foschino Barbaro, M.P.; Lo Muzio, L.; Cassano, M. Correlation between Body Mass Index and Obstructive Sleep Apnea Severity Indexes—A Retrospective Study. Am. J. Otolaryngol. 2018, 39, 388–391. [Google Scholar] [CrossRef]
- Troiano, G.; Dioguardi, M.; Cocco, A.; Zhurakivska, K.; Ciavarella, D.; Muzio, L.L. Increase the Glyde Path Diameter Improves the Centering Ability of F6 Skytaper. Eur. J. Dent. 2018, 12, 089–093. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]
- Ciavarella, D.; Parziale, V.; Mastrovincenzo, M.; Palazzo, A.; Sabatucci, A.; Suriano, M.M.; Bossù, M.; Cazzolla, A.P.; Lo Muzio, L.; Chimenti, C. Condylar Position Indicator and T-Scan System II in Clinical Evaluation of Temporomandibular Intracapsular Disease. J. Cranio-Maxillofac. Surg. 2012, 40, 449–455. [Google Scholar] [CrossRef]
- Cianci, C.; Pappalettera, G.; Renna, G.; Casavola, C.; Laurenziello, M.; Battista, G.; Pappalettere, C.; Ciavarella, D. Mechanical Behavior of PET-G Tooth Aligners Under Cyclic Loading. Front. Mater. 2020, 7, 104. [Google Scholar] [CrossRef]
- Inchingolo, A.M.; Malcangi, G.; Costa, S.; Fatone, M.C.; Avantario, P.; Campanelli, M.; Piras, F.; Patano, A.; Ferrara, I.; Di Pede, C.; et al. Tooth Complications after Orthodontic Miniscrews Insertion. Int. J. Environ. Res. Public Health 2023, 20, 1562. [Google Scholar] [CrossRef] [PubMed]
- Myser, S.A.; Campbell, P.M.; Boley, J.; Buschang, P.H. Long-term stability: Postretention changes of the mandibular anterior teeth. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 420–429. [Google Scholar] [CrossRef]
- Raucci, G.; Pachêco-Pereira, C.; Elyasi, M.; d’Apuzzo, F.; Flores-Mir, C.; Perillo, L. Predictors of Postretention Stability of Mandibular Dental Arch Dimensions in Patients Treated with a Lip Bumper during Mixed Dentition Followed by Fixed Appliances. Angle Orthod. 2017, 87, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina 2021, 57, 288. [Google Scholar] [CrossRef]
- Freitas, K.M.S.; Massaro, C.; Miranda, F.; de Freitas, M.R.; Janson, G.; Garib, D. Occlusal Changes in Orthodontically Treated Subjects 40 Years after Treatment and Comparison with Untreated Control Subjects. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 671–685. [Google Scholar] [CrossRef]
- Mahmoudzadeh, M.; Mirzaei, H.; Farhadian, M.; Mollabashi, V.; Khosravi, M. Comparison of Anterior Crowding Relapse Tendency in Patients Treated with Incisor Extraction, Premolar Extraction, and Nonextraction Treatment. J. World Fed. Orthod. 2018, 7, 61–65. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).