
Educational Programme for Cancer Nurses in Genetics, Health Behaviors and Cancer Prevention: A Multidisciplinary Consensus Study


Abstract
1. Introduction
2. Materials and Methods
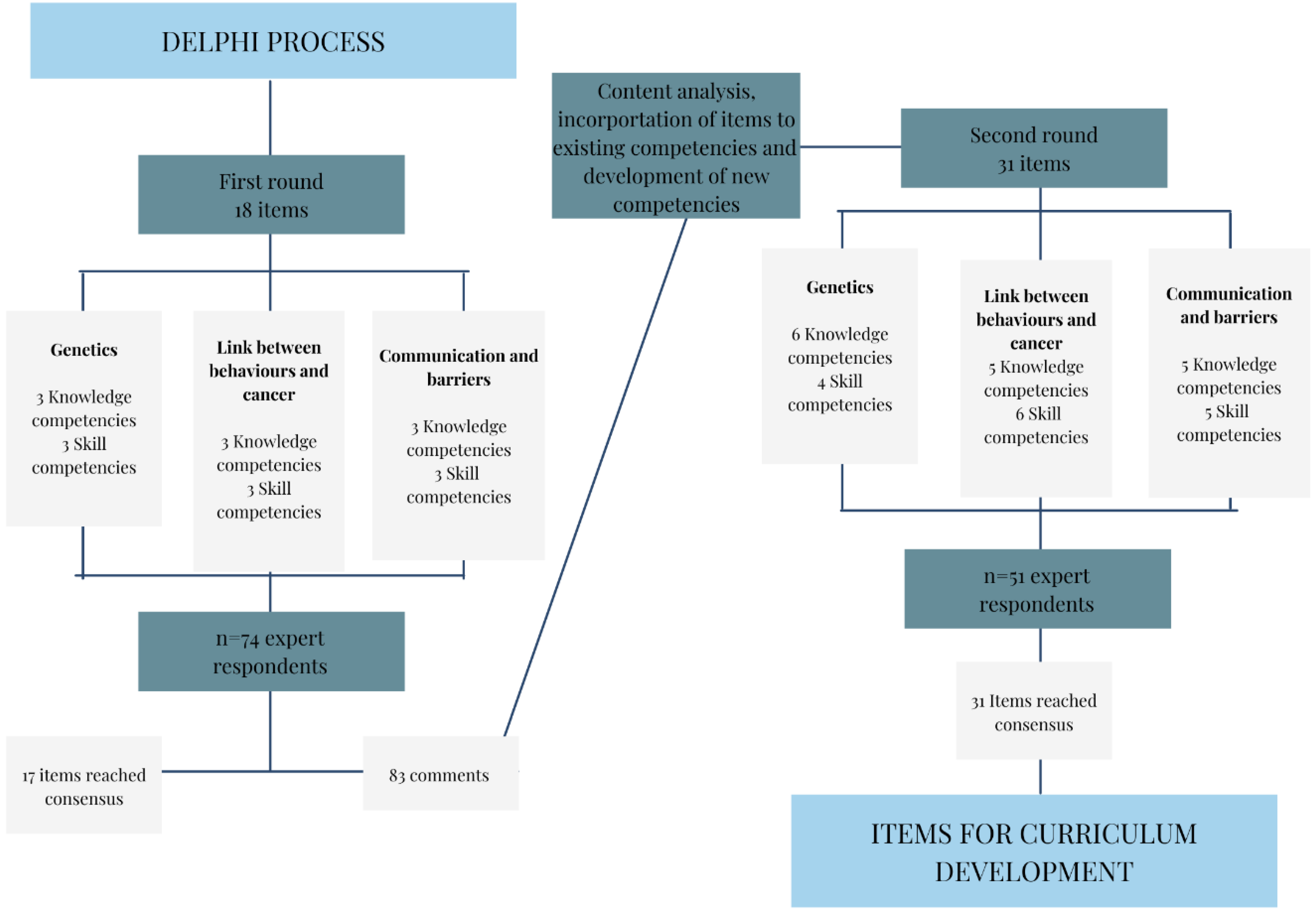
2.1. Delphi Study Process
2.2. Expert Panel
3. Results
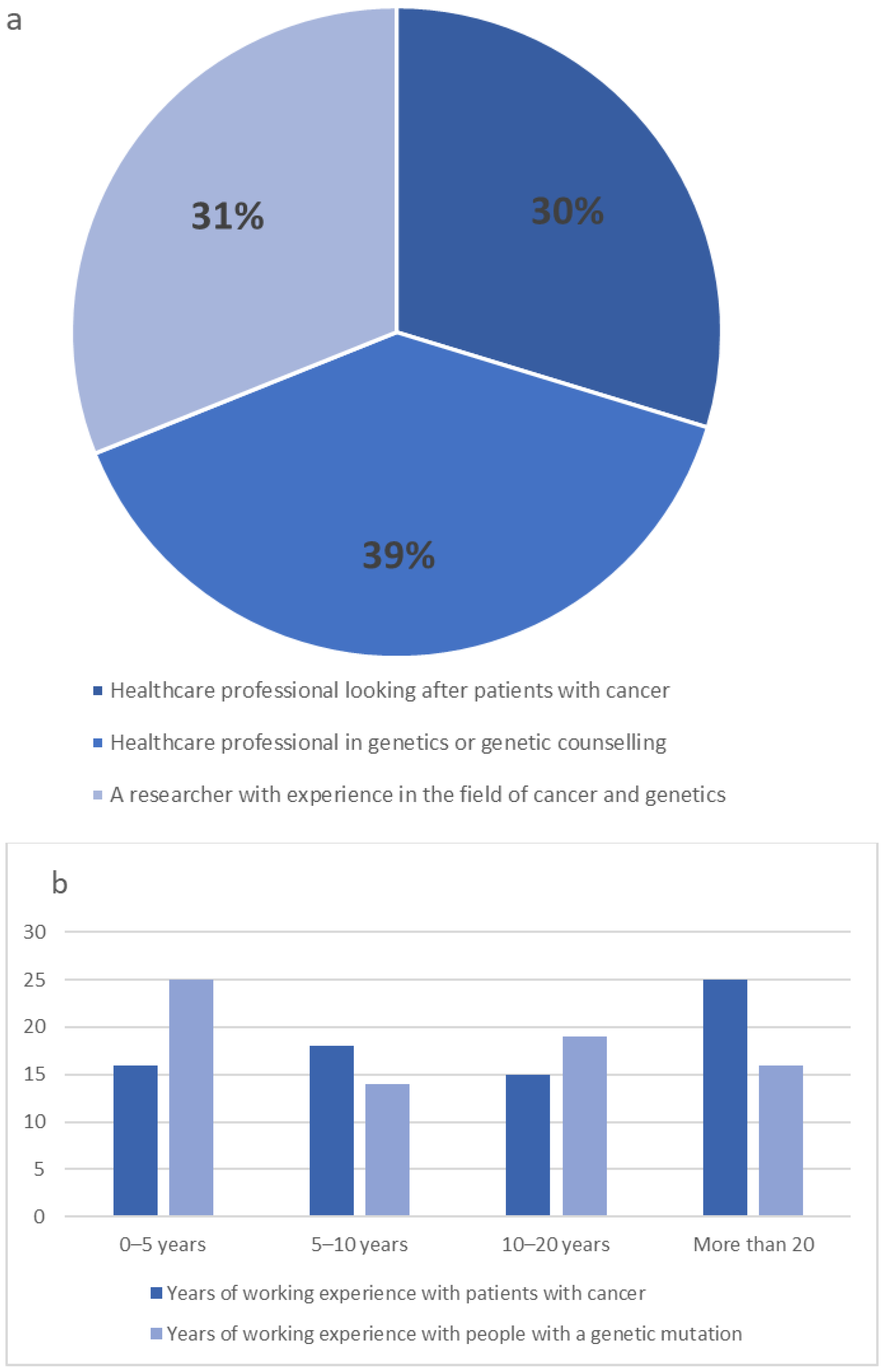
Expert Characteristics
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Merlo, L.M.F.; Pepper, J.W.; Reid, B.J.; Maley, C.C. Cancer as an Evolutionary and Ecological Process. Nat. Rev. Cancer 2006, 6, 924–935. [Google Scholar] [CrossRef] [PubMed]
- Nagy, R.; Sweet, K.; Eng, C. Highly Penetrant Hereditary Cancer Syndromes. Oncogene 2004, 23, 6445–6470. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, A.H.; Lester Kirchner, H.; Schwartz, M.L.B.; Kelly, M.A.; Schmidlen, T.; Jones, L.K.; Hallquist, M.L.G.; Rocha, H.; Betts, M.; Schwiter, R.; et al. Clinical Outcomes of a Genomic Screening Program for Actionable Genetic Conditions. Genet. Med. 2020, 22, 1874–1882. [Google Scholar] [CrossRef] [PubMed]
- Laforest, F.; Mann, B.; Edwards, A.; Kirkegaard, P. Genetic Cancer Risk Assessment in General Practice: Systematic Review of Tools Available, Clinician Attitudes, and Patient Outcomes. Br. J. Gen. Pract. 2019, 69, E97–E105. [Google Scholar] [CrossRef]
- Grzymski, J.J.; Elhanan, G.; Morales Rosado, J.A.; Smith, E.; Schlauch, K.A.; Read, R.; Rowan, C.; Slotnick, N.; Dabe, S.; Metcalf, W.J.; et al. Population Genetic Screening Efficiently Identifies Carriers of Autosomal Dominant Diseases. Nat. Med. 2020, 26, 1235–1239. [Google Scholar] [CrossRef]
- Maxwell, K.N.; Domchek, S.M. Cancer Treatment According to BRCA1 and BRCA2 Mutations. Nat. Rev. Clin. Oncol. 2012, 9, 520–528. [Google Scholar] [CrossRef]
- Cragun, D.; Beckstead, J.; Farmer, M.; Hooker, G.; Dean, M.; Matloff, E.; Reid, S.; Tezak, A.; Weidner, A.; Whisenant, J.G.; et al. IMProving Care After Inherited Cancer Testing (IMPACT) Study: Protocol of a Randomized Trial Evaluating the Efficacy of Two Interventions Designed to Improve Cancer Risk Management and Family Communication of Genetic Test Results. BMC Cancer 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Madlensky, L.; Trepanier, A.M.; Cragun, D.; Lerner, B.; Shannon, K.M.; Zierhut, H. A Rapid Systematic Review of Outcomes Studies in Genetic Counseling. J. Genet. Couns. 2017, 26, 361–378. [Google Scholar] [CrossRef]
- Riley, B.D.; Culver, J.O.; Skrzynia, C.; Senter, L.A.; Peters, J.A.; Costalas, J.W.; Callif-Daley, F.; Grumet, S.C.; Hunt, K.S.; Nagy, R.S.; et al. Essential Elements of Genetic Cancer Risk Assessment, Counseling, and Testing: Updated Recommendations of the National Society of Genetic Counselors. J. Genet. Couns. 2012, 21, 151–161. [Google Scholar] [CrossRef]
- Eggert, J. Genetics and Genomics in Oncology Nursing: What Does Every Nurse Need to Know? Nurs. Clin. 2017, 52, 1–25. [Google Scholar] [CrossRef]
- Schneider, J.L.; Goddard, K.A.B.; Muessig, K.R.; Davis, J.V.; Rope, A.F.; Hunter, J.E.; Peterson, S.K.; Acheson, L.S.; Syngal, S.; Wiesner, G.L.; et al. Patient and Provider Perspectives on Adherence to and Care Coordination of Lynch Syndrome Surveillance Recommendations: Findings from Qualitative Interviews. Hered. Cancer Clin. Pract. 2018, 16, 1–10. [Google Scholar] [CrossRef]
- De Simone, L.M.; Arjunan, A.; Vogel Postula, K.J.; Maga, T.; Bucheit, L.A. Genetic Counselors’ Perspectives on Population-Based Screening for BRCA-Related Hereditary Breast and Ovarian Cancer and Lynch Syndrome. J. Genet. Couns. 2021, 30, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Singer, C.F.; Balmaña, J.; Bürki, N.; Delaloge, S.; Filieri, M.E.; Gerdes, A.M.; Grindedal, E.M.; Han, S.; Johansson, O.; Kaufman, B.; et al. Genetic Counselling and Testing of Susceptibility Genes for Therapeutic Decision-Making in Breast Cancer—an European Consensus Statement and Expert Recommendations. Eur. J. Cancer 2019, 106, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Collins, I.M.; Steel, E.; Mann, G.B.; Emery, J.D.; Bickerstaffe, A.; Trainer, A.; Butow, P.; Pirotta, M.; Antoniou, A.C.; Cuzick, J.; et al. Assessing and Managing Breast Cancer Risk: Clinicians’ Current Practice and Future Needs. Breast 2014, 23, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Keogh, L.A.; Steel, E.; Weideman, P.; Butow, P.; Collins, I.M.; Emery, J.D.; Mann, G.B.; Bickerstaffe, A.; Trainer, A.H.; Hopper, L.J.; et al. Consumer and Clinician Perspectives on Personalising Breast Cancer Prevention Information. Breast 2019, 43, 39–47. [Google Scholar] [CrossRef]
- Williams, J.K.; Katapodi, M.C.; Starkweather, A.; Badzek, L.; Cashion, A.K.; Coleman, B.; Fu, M.R.; Lyon, D.; Weaver, M.T.; Hickey, K.T. Advanced Nursing Practice and Research Contributions to Precision Medicine. Nurs. Outlook 2016, 64, 117–123. [Google Scholar] [CrossRef]
- Seven, M.; Pasalak, S.I.; Guvenc, G.; Kok, G. Knowledge Level and Educational Needs of Turkish Oncology Nurses Regarding the Genetics of Hereditary Breast and Ovarian Cancer. J. Contin. Educ. Nurs. 2017, 48, 570–576. [Google Scholar] [CrossRef]
- Prolla, C.M.D.; Da Silva, P.S.; Oliveira Netto, C.B.; Goldim, J.R.; Ashton-Prolla, P. Knowledge about Breast Cancer and Hereditary Breast Cancer among Nurses in a Public Hospital. Rev. Lat. Am. Enferm. 2015, 23, 90–97. [Google Scholar] [CrossRef]
- Matsumoto, M.; Sasaki, N.; Tsukigawa, Y.; Otsubo, R.; Yano, H.; Nagayasu, T. A Survey of the Awareness and Educational Needs of Nurses in Nagasaki Prefecture Regarding Hereditary Breast and Ovarian Cancer. J. Cancer Educ. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, C.; Rahman, B. One Size Does Not Fit All: The Case for Targeted Education in Genetics and Genomics for Cancer Nurses. Eur. J. Cancer Care 2021, 30, e13480. [Google Scholar] [CrossRef]
- Hickey, K.T.; Taylor, J.Y.; Barr, T.L.; Hauser, N.R.; Jia, H.; Riga, T.C.; Katapodi, M. Nursing Genetics and Genomics: The International Society of Nurses in Genetics (ISONG) Survey. Nurse Educ. Today 2018, 63, 12–17. [Google Scholar] [CrossRef]
- Skirton, H.; Barnoy, S.; Erdem, Y.; Ingvoldstad, C.; Pestoff, R.; Teksen, F.; Williams, J. Suggested Components of the Curriculum for Nurses and Midwives to Enable Them to Develop Essential Knowledge and Skills in Genetics. J. Community Genet. 2012, 3, 323–329. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zureigat, B.; Gould, D.; Seven, M. Educational Interventions to Improve Nurses’ Competency in Genetics and Genomics: A Scoping Review. J. Contin. Educ. Nurs. 2022, 53, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Charalambous, A.; Wells, M.; Campbell, P.; Torrens, C.; Östlund, U.; Oldenmenger, W.; Kelly, D. A scoping review of trials of interventions led or delivered by cancer nurses. Int. J. Nurs. Stud. 2018, 86, 36–43. [Google Scholar] [CrossRef]
- The EONS Cancer Nursing Education Framework. Available online: https://cancernurse.eu/education/cancer-nursing-education-framework/ (accessed on 10 June 2022).
- Rahman, B.; McEwen, A.; Phillips, J.L.; Tucker, K.; Goldstein, D.; Jacobs, C. Genetic and Genomic Learning Needs of Oncologists and Oncology Nurses in the Era of Precision Medicine: A Scoping Review. Per. Med. 2022, 19, 139–153. [Google Scholar] [CrossRef] [PubMed]
- Drumm, S.; Bradley, C.; Moriarty, F. ‘More of an Art than a Science’? The Development, Design and Mechanics of the Delphi Technique. Res. Soc. Adm. Pharm. 2022, 18, 2230–2236. [Google Scholar] [CrossRef] [PubMed]
- Avella, J.R. Delphi Panels: Research Design, Procedures, Advantages, and Challenges. Int. J. Dr. Stud. 2016, 11, 305–321. [Google Scholar] [CrossRef]
- Broomfield, D.; Humphris, G.M. Using the Delphi Technique to Identify the Cancer Education Requirements of General Practitioners. Med. Educ. 2001, 35, 928–937. [Google Scholar] [CrossRef]
- Kirk, M.; Tonkin, E.; Skirton, H. An Iterative Consensus-Building Approach to Revising a Genetics/Genomics Competency Framework for Nurse Education in the UK. J. Adv. Nurs. 2014, 70, 405–420. [Google Scholar] [CrossRef]
- Niederberger, M.; Spranger, J. Delphi Technique in Health Sciences: A Map. Front. Public Health 2020, 8, 457. [Google Scholar] [CrossRef]
- Diez de los Rios de la Serna, C.; Fernandez-Ortega, P.; Lluch-Canut, T. CN13 Review of Healthcare Interventions to Promote Cancer Prevention by Improving Lifestyle Behaviours. Ann. Oncol. 2021, 32, S1260. [Google Scholar] [CrossRef]
- Shariff, N.J. Utilizing the Delphi Survey Approach: A Review. J. Nurs. Care 2015, 4, 246. [Google Scholar] [CrossRef]
- Okoli, C.; Pawlowski, S.D. The Delphi Method as a Research Tool: An Example, Design Considerations and Applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef]
- Hoxhaj, I.; Tognetto, A.; Acampora, A.; Stojanovic, J.; Boccia, S. Core Competencies in Cancer Genomics for Healthcare Professionals: Results From a Systematic Literature Review and a Delphi Process. J. Cancer Educ. 2021, 1–11, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Warner, N.Z.; Gleeson, C.; Fahey, P.; Horgan, R.; Groarke, A.M. Experiences of Living with Lynch Syndrome: A Reflexive Thematic Analysis. Eur. J. Oncol. Nurs. 2022, 58, 102117. [Google Scholar] [CrossRef]
- Mazor, K.M.; Roblin, D.W.; Williams, A.E.; Greene, S.M.; Gaglio, B.; Field, T.S.; Costanza, M.E.; Han, P.K.J.; Saccoccio, L.; Calvi, J.; et al. Health Literacy and Cancer Prevention: Two New Instruments to Assess Comprehension. Patient Educ. Couns. 2012, 88, 54. [Google Scholar] [CrossRef]
- Mahon, S.M. Providing Care for Previvors: Implications for Oncology Nurses. Clin. J. Oncol. Nurs. 2014, 18, 21–24. [Google Scholar] [CrossRef][Green Version]
- Campbell-Salome, G.; Buchanan, A.H.; Hallquist, M.L.G.; Rahm, A.K.; Rocha, H.; Sturm, A.C. Uncertainty Management for Individuals with Lynch Syndrome: Identifying and Responding to Healthcare Barriers. Patient Educ. Couns. 2021, 104, 403–412. [Google Scholar] [CrossRef]
- Benito, L.; Binefa, G.; Vidal, C.; Lluch, M.T.; Puig, M.; Padrol, I.; García, M. Identifying Nursing Activities in Population-Based Colorectal and Breast Cancer Screening Programs in Spain: A Delphi Study. Collegian 2017, 24, 351–359. [Google Scholar] [CrossRef]
- Keeney, S.; Hasson, F.; McKenna, H.P. A Critical Review of the Delphi Technique as a Research Methodology for Nursing. Int. J. Nurs. Stud. 2001, 38, 195–200. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Genetics | Round 1 Agreement | Round 2 Agreement |
|---|---|---|
| Knowledge on determinants of cancer | 100% | 100% |
| Knowledge and understanding of the most common genetic mutations/syndromes in cancer setting | 95% | 95% |
| Knowledge of the role of genetics in cancer treatment | 93% | 95% |
| Knowledge of instruments to estimate risk | NEW in 2 | 80% |
| Knowledge on genetic processes | NEW in 2 | 88% |
| Knowledge of the role of genetic counsellors | NEW in 2 | 80% |
| Ability to undertake a comprehensive history to identify the individual, familial, genetic, sociocultural, economic and environmental factors | 93% | 96% |
| Ability to identify individuals that may be potentially at risk of having a genetic predisposition to cancer | 97% | 96% |
| Ability to create communication links between oncology and genetic healthcare providers | 96% | 92% |
| Ability to explain patients genetic testing | NEW in 2 | 84% |
| Behaviors | Round 1 | Round 2 |
| Knowledge on modifiable determinants of cancer and their importance on people with high risk of cancer | 92% | 90% |
| Health promotion and health education | 91% | 84% |
| Knowledge on the European Code Against Cancer recommendations changed in the second round to: Knowledge of recommendations to reduce risk of cancer | 64% | 76% |
| Knowledge of the social and behavioural determinants of health on genetic susceptibility | NEW in 2 | 86% |
| Surveillance | NEW in 2 | 88% |
| Ability to use health promotion/disease prevention practices that incorporate genetic and genomic information as well as personal and environmental risk factors | 91% | 88% |
| Ability to address peoples’ beliefs and values | 92% | 94% |
| Ability to identify problems with surveillance | 86% | 92% |
| Ability to recognise risk factors | NEW in 2 | 80% |
| Communication | Round 1 | Round 2 |
| Barriers to effective information provision | 92% | 93% |
| Awareness of consequences of cancer such as the emotional experiences associated with the diagnosis of cancer, the impact on the life of the patient and family as well as effects of treatment | 97% | 100% |
| Knowledge on health belief theories and health behaviour change theories. | 78% | 76% |
| Family planning and fertility implications | NEW in 2 | 90% |
| Psycho-social support | NEW in 2 | 88% |
| Ability to identify ethical, ethnic/ancestral, cultural, religious, legal, fiscal, and societal issues related to understanding health and genetic information | 77% | 86% |
| Demonstrate use of a range of effective communication skills/strategies to provide information, psychological and emotional support to individuals and communities about cancer | 96% | 96% |
| Select and adopt an appropriate communication approach, from a range of core communication and consultation skills, to effectively support the people with high risk of cancer | 95% | 96% |
| Ability to communicate and support family members at risk | NEW in 2 | 92% |
| Nurses’ role in the follow up/support | NEW in 2 | 92% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diez de los Rios de la Serna, C.; Fernández-Ortega, P.; Lluch-Canut, T. Educational Programme for Cancer Nurses in Genetics, Health Behaviors and Cancer Prevention: A Multidisciplinary Consensus Study. J. Pers. Med. 2022, 12, 1104. https://doi.org/10.3390/jpm12071104
Diez de los Rios de la Serna C, Fernández-Ortega P, Lluch-Canut T. Educational Programme for Cancer Nurses in Genetics, Health Behaviors and Cancer Prevention: A Multidisciplinary Consensus Study. Journal of Personalized Medicine. 2022; 12(7):1104. https://doi.org/10.3390/jpm12071104
Chicago/Turabian StyleDiez de los Rios de la Serna, Celia, Paz Fernández-Ortega, and Teresa Lluch-Canut. 2022. "Educational Programme for Cancer Nurses in Genetics, Health Behaviors and Cancer Prevention: A Multidisciplinary Consensus Study" Journal of Personalized Medicine 12, no. 7: 1104. https://doi.org/10.3390/jpm12071104
APA StyleDiez de los Rios de la Serna, C., Fernández-Ortega, P., & Lluch-Canut, T. (2022). Educational Programme for Cancer Nurses in Genetics, Health Behaviors and Cancer Prevention: A Multidisciplinary Consensus Study. Journal of Personalized Medicine, 12(7), 1104. https://doi.org/10.3390/jpm12071104