
Success Factors and Barriers in Combining Personalized Medicine and Patient Centered Care in Breast Cancer. Results from a Systematic Review and Proposal of Conceptual Framework


Abstract
:1. Introduction
2. Materials and Methods
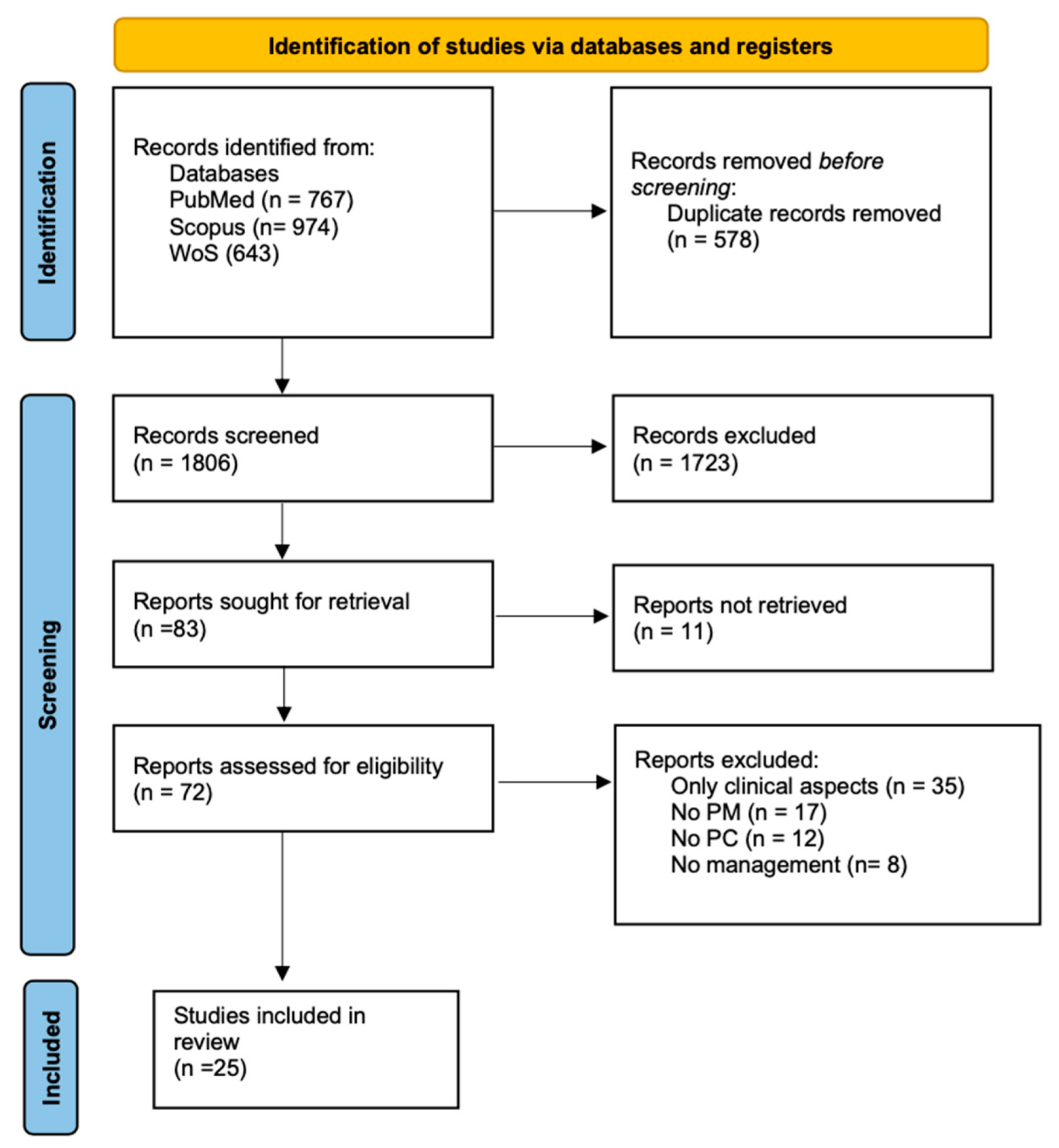
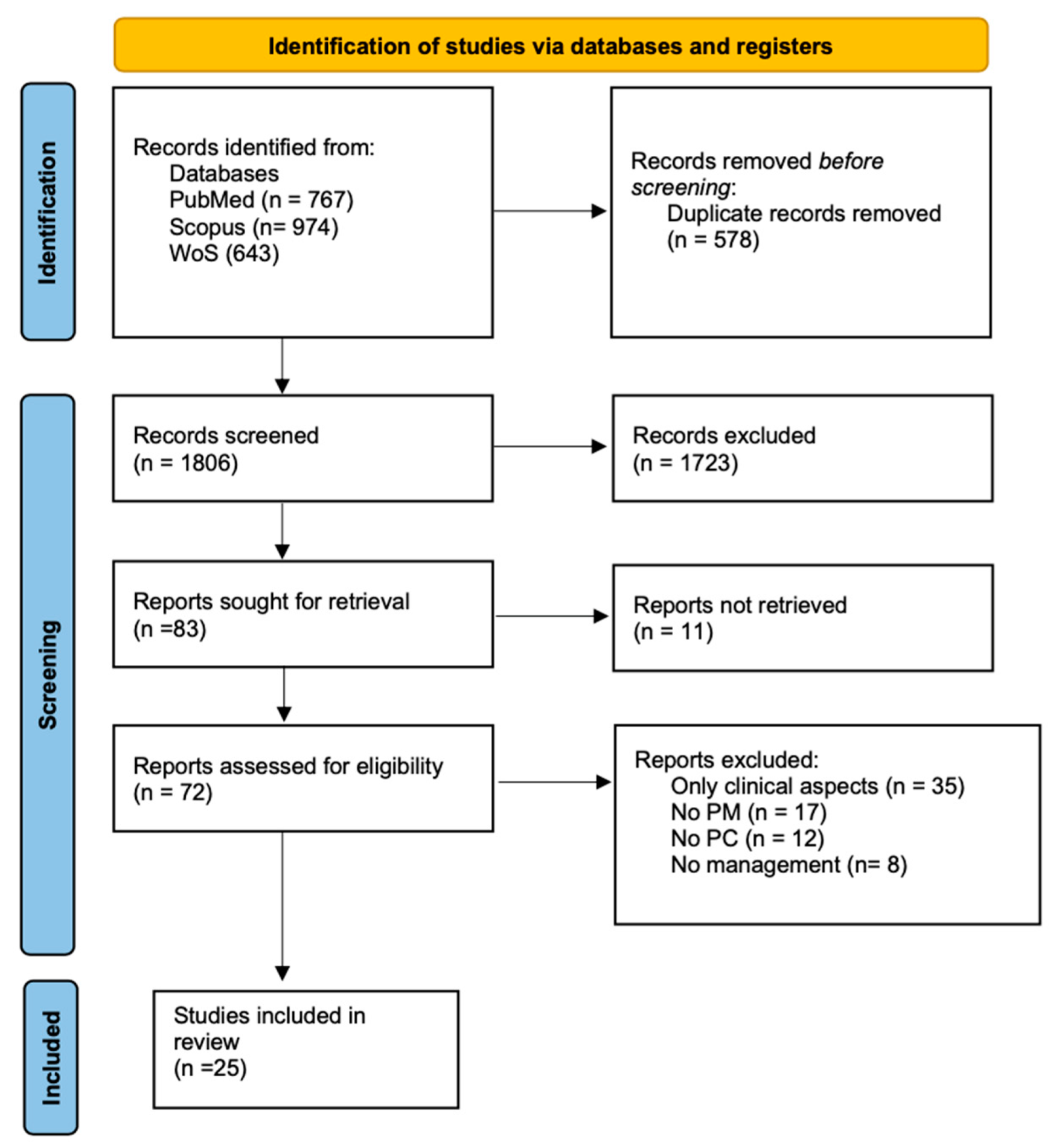
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction and Synthesis
- Study identification (first author, title, journal, publication year);
- Study characteristics (period, country, design);
- Sample characteristics (stage of breast cancer, sample age, sample ethnicity);
- Personalized Medicine and Patient centered aspects;
- Barriers and/or success factors.
2.5. Quality Assessment
3. Results
3.1. Results of Quality Assessment
3.2. Outcome Categories
3.2.1. Patient-Centered Care Key Dimensions
3.2.2. Personalized Medicine Key Dimensions
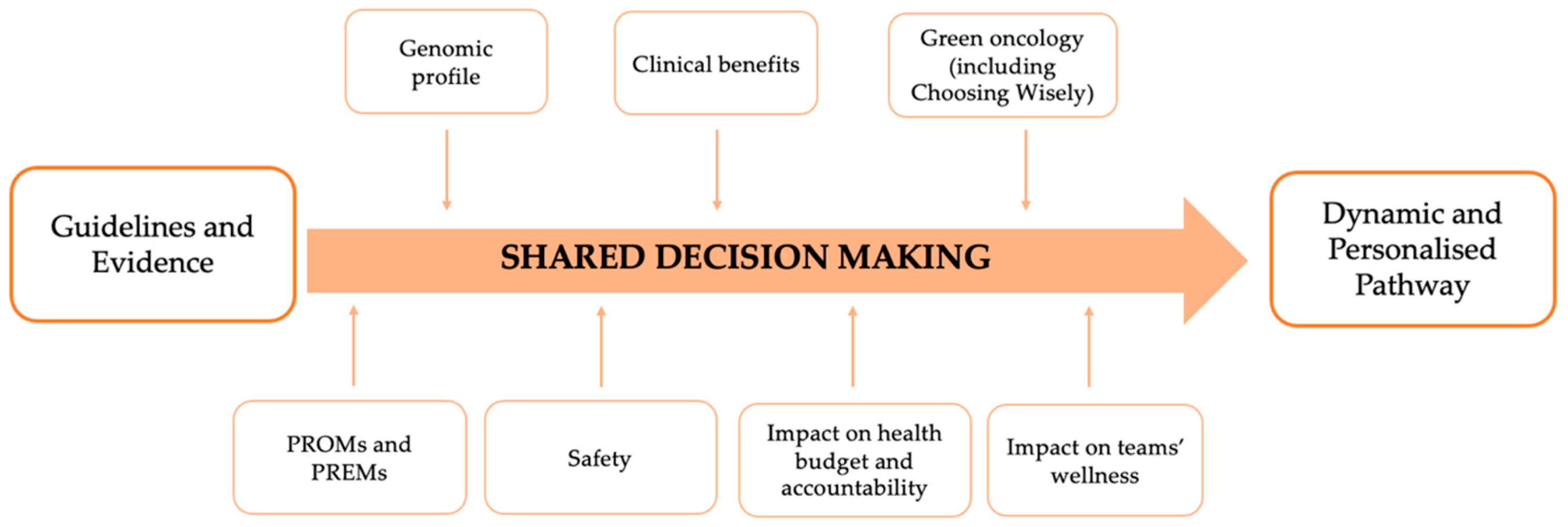
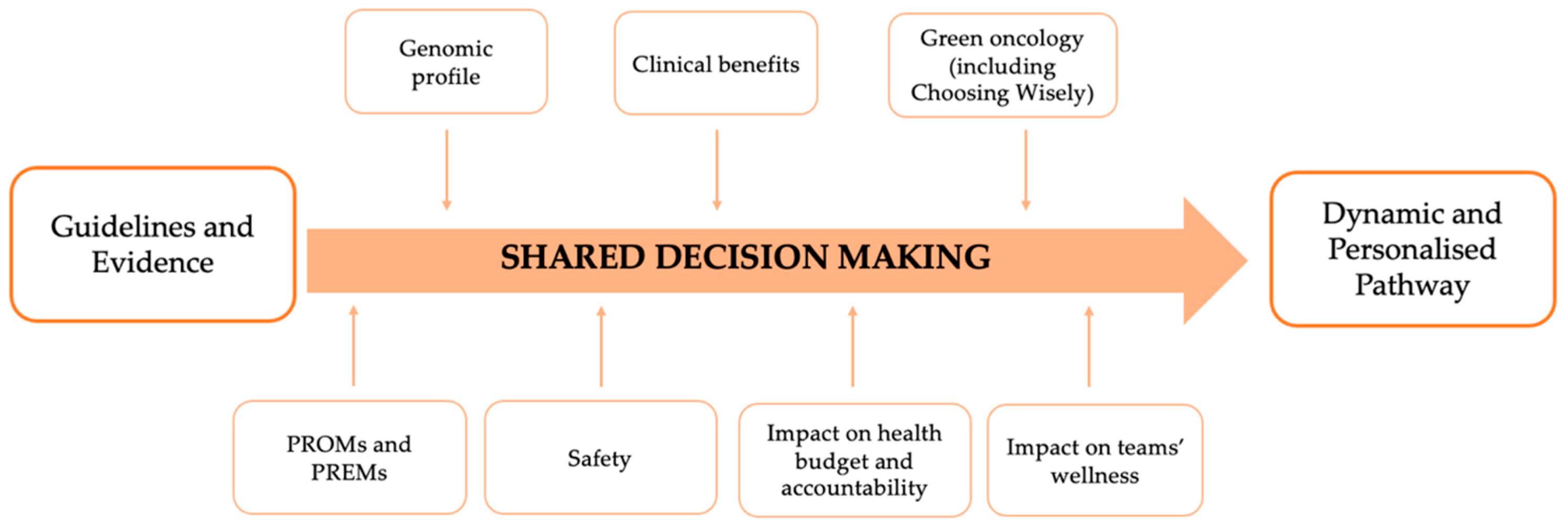
3.2.3. Key Dimensions for Applying Personalized Medicine and Patient-Centered Care
3.3. Success Factors and Barriers in the Management of Breast Cancer Pathway
3.3.1. Success Factors
3.3.2. Barriers
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Shao, J.; Rodrigues, M.; Corter, A.L.; Baxter, N.N. Multidisciplinary Care of Breast Cancer Patients: A Scoping Review of Multidisciplinary Styles, Processes, and Outcomes. Curr. Oncol. 2019, 26, 385–397. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Cataliotti, L.; Costa, A.; Knox, S.; Marotti, L.; Rutgers, E.; Beishon, M. European Breast Cancer Conference manifesto on breast centres/units. Eur. J. Cancer 2017, 72, 244–250. [Google Scholar] [CrossRef] [Green Version]
- Franceschini, G.; Di Leone, A.; Masetti, R. The Breast Unit Update on advantages and the open issues. Ann. Ital. Chir. 2014, 85, 407–412. [Google Scholar]
- Chan, C.W.H.; Law, B.M.H.; So, W.K.W.; Chow, K.M.; Waye, M.M.Y. Novel Strategies on Personalized Medicine for Breast Cancer Treatment: An Update. Int. J. Mol. Sci. 2017, 18, 2423. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Senkus, E.; Costa, A.; Papadopoulos, E.; Aapro, M.; Andre, F.; Harbeck, N.; Lopez, B.A.; Barrios, C.; Bergh, J.; et al. 4th ESO–ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 4). Ann. Oncol. 2018, 29, 1634–1657. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Brennan, S.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. 2020. Available online: https://osf.io/preprints/metaarxiv/v7gm2/ (accessed on 19 May 2021).
- EUR-Lex. C:2015:421:FULL. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=OJ%3AC%3A2015%3A421%3AFULL (accessed on 25 May 2021).
- Medicine I of Crossing the Quality Chasm: A New Health System for the 21st Century. 2001. Available online: https://www.nap.edu/catalog/10027/crossing-the-quality-chasm-a-new-health-system-for-the (accessed on 19 May 2021).
- Naughton, C.A. Patient-Centered Communication. Pharmacy 2018, 6, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotter, T.; Kinsman, L.; James, E.L.; Machotta, A.; Gothe, H.; Willis, J.; Snow, P.; Kugler, J. Clinical pathways: Effects on professional practice, patient outcomes, length of stay and hospital costs. Cochrane Database Syst. Rev. 2010, CD006632. [Google Scholar] [CrossRef]
- Yazdanian, A.; Ayatollahi, H.; Nahvijou, A. Oncology Information System: A Qualitative Study of Users’ Requirements. Asian Pac. J. Cancer Prev. 2019, 20, 3085–3091. [Google Scholar] [CrossRef]
- Melnyk, B.M.; Fineout-Overholt, E. Evidence-Based Practice in Nursing & Healthcare: A Guide to Best Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; 530p. [Google Scholar]
- Horvath, L.E.; Yordan, E.; Malhotra, D.; Leyva, I.; Bortel, K.; Schalk, D.; Mellinger, P.; Huml, M.; Kesslering, C.; Huml, J. Multidisciplinary Care in the Oncology Setting: Historical Perspective and Data from Lung and Gynecology Multidisciplinary Clinics. J. Oncol. Pract. 2010, 6, e21–e26. [Google Scholar] [CrossRef]
- Koopman, B.; Groen, H.J.; Ligtenberg, M.J.; Grünberg, K.; Monkhorst, K.; De Langen, A.J.; Boelens, M.C.; Paats, M.S.; Von Der Thüsen, J.H.; Dinjens, W.N.; et al. Multicenter Comparison of Molecular Tumor Boards in The Netherlands: Definition, Composition, Methods, and Targeted Therapy Recommendations. Oncologist 2020. [Google Scholar] [CrossRef]
- Pagon, R.A.; Hanson, N.B.; Neufeld-Kaiser, W.; Covington, M.L. Genetic testing. West. J. Med. 2001, 174, 344–347. [Google Scholar] [CrossRef]
- Shared Decision Making. Available online: https://www.healthit.gov/sites/default/files/nlc_shared_decision_making_fact_sheet.pdf (accessed on 20 May 2021).
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—A scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Long, H.A.; French, D.P.; Brooks, J.M. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res. Methods Med. Health Sci. 2020, 1, 31–42. [Google Scholar] [CrossRef]
- Martin, J. Joanna Briggs Institute 2017 Critical Appraisal Checklist for Cohort Studies; JBI: Adelaide, Australia, 2017. [Google Scholar]
- Martin, J. Joanna Briggs Institute 2017 Critical Appraisal Checklist for Text and Opinion; JBI: Adelaide, Australia, 2017. [Google Scholar]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, J. Joanna Briggs Institute 2017 Critical Appraisal Checklist for Systematic Reviews and Research Syntheses; JBI: Adelaide, Australia, 2017. [Google Scholar]
- Rosa, M. Advances in the Molecular Analysis of Breast Cancer: Pathway toward Personalized Medicine. Cancer Control 2015, 22, 211–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fountzilas, C.; Kaklamani, V.G. Multi-gene Panel Testing in Breast Cancer Management. Cancer Treat. Res. 2018, 173, 121–140. [Google Scholar] [CrossRef]
- Trivedi, H.; Kling, H.M.; Treece, T.; Audeh, W.; Srkalovic, G. Changing Landscape of Clinical-Genomic Oncology Practice. Acta Medica Acad. 2019, 48, 6–17. [Google Scholar] [CrossRef]
- Biganzoli, L.; Marotti, L.; Hart, C.D.; Cataliotti, L.; Cutuli, B.; Kühn, T.; Mansel, R.E.; Ponti, A.; Poortmans, P.; Regitnig, P.; et al. Quality indicators in breast cancer care: An update from the EUSOMA working group. Eur. J. Cancer 2017, 86, 59–81. [Google Scholar] [CrossRef]
- Lyman, G.H.; Baker, J.; Geradts, J.; Horton, J.; Kimmick, G.; Peppercorn, J.; Pruitt, S.; Scheri, R.P.; Hwang, E.S. Multidisciplinary Care of Patients with Early-Stage Breast Cancer. Surg. Oncol. Clin. N. Am. 2013, 22, 299–317. [Google Scholar] [CrossRef]
- Tischler, J.; Crew, K.D.; Chung, W.K. Cases in Precision Medicine: The Role of Tumor and Germline Genetic Testing in Breast Cancer Management. Ann. Intern. Med. 2019, 171, 925. [Google Scholar] [CrossRef] [PubMed]
- Girotra, S.; Yeghiazaryan, K.; Golubnitschaja, O. Potential biomarker panels in overall breast cancer management: Advancements by multilevel diagnostics. Pers. Med. 2016, 13, 469–484. [Google Scholar] [CrossRef] [PubMed]
- Saini, G.; Mittal, K.; Rida, P.; Janssen, E.A.M.; Gogineni, K.; Aneja, R. Panoptic View of Prognostic Models for Personalized Breast Cancer Management. Cancers 2019, 11, 1325. [Google Scholar] [CrossRef] [Green Version]
- Laronga, C.; Harness, J.K.; Dixon, M.; Borgen, P.I. The role of the breast cancer surgeon in personalized cancer care: Clinical utility of the 21-gene assay. Am. J. Surg. 2012, 203, 751–758. [Google Scholar] [CrossRef] [PubMed]
- McGowan, M.L.; Ponsaran, R.S.; Silverman, P.; Harris, L.N.; Marshall, P.A. “A rising tide lifts all boats”: Establishing a multidisciplinary genomic tumor board for breast cancer patients with advanced disease. BMC Med Genom. 2016, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Weldon, C.B.; Trosman, J.R.; Gradishar, W.J.; Benson, A.B.; Schink, J.C. Barriers to the Use of Personalized Medicine in Breast Cancer. J. Oncol. Pract. 2012, 8, e24–e31. [Google Scholar] [CrossRef] [Green Version]
- Wright, S.; Porteous, M.; Stirling, D.; Young, O.; Gourley, C.; Hallowell, N. Negotiating jurisdictional boundaries in response to new genetic possibilities in breast cancer care: The creation of an ‘oncogenetic taskscape’. Soc. Sci. Med. 2019, 225, 26–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, M.C.; Bryson, A.; Weinberger, M.; Dusetzina, S.; Dinan, M.A.; Reeder-Hayes, K.E.; Wheeler, S.B. Patient-Centered Communication for Discussing Oncotype DX Testing. Cancer Investig. 2016, 34, 205–212. [Google Scholar] [CrossRef]
- Schnapper, G.; Marotti, L.; Casella, D.; Mano, M.P.; Mansel, R.E.; Ponti, A.; The EUSOMA Breast Centers Network Data Managers. Data managers: A survey of the European Society of Breast Cancer Specialists in certified multi-disciplinary breast centers. Breast J. 2018, 24, 811–815. [Google Scholar] [CrossRef]
- Kurian, A.W.; Li, Y.; Hamilton, A.S.; Ward, K.C.; Hawley, S.T.; Morrow, M.; McLeod, M.C.; Jagsi, R.; Katz, S.J. Gaps in Incorporating Germline Genetic Testing into Treatment Decision-Making for Early-Stage Breast Cancer. J. Clin. Oncol. 2017, 35, 2232–2239. [Google Scholar] [CrossRef]
- Komatsu, H.; Yagasaki, K. Are we ready for personalized cancer risk management? The view from breast-care providers. Int. J. Nurs. Pract. 2013, 20, 39–45. [Google Scholar] [CrossRef]
- Jacobs, C.; Pichert, G.; Harris, J.; Tucker, K.; Michie, S. Key messages for communicating information about BRCA1 and BRCA2 to women with breast or ovarian cancer: Consensus across health professionals and service users. Psycho-Oncology 2017, 26, 1818–1824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zardavas, D.; Pugliano, L.; Piccart, M. Personalized therapy for breast cancer: A dream or a reality? Futur. Oncol. 2013, 9, 1105–1119. [Google Scholar] [CrossRef]
- Cowppli-Bony, A.; Trétarre, B.; Marrer, E.; Defossez, G.; Daubisse-Marliac, L.; Coureau, G.; Minicozzi, P.; Woronoff, A.-S.; Delafosse, P.; Molinié, F.; et al. Compliance with clinical guidelines for breast cancer management: A population-based study of quality-of-care indicators in France. PLoS ONE 2019, 14, e0224275. [Google Scholar] [CrossRef] [Green Version]
- Kurian, A.W.; Friese, C.R. Precision Medicine in Breast Cancer Care: An Early Glimpse of Impact. JAMA Oncol. 2015, 1, 1109–1110. [Google Scholar] [CrossRef] [PubMed]
- Powis, M.; Sutradhar, R.; Gonzalez, A.; Enright, K.A.; Taback, N.A.; Booth, C.M.; Trudeau, M.; Krzyzanowska, M.K. Establishing achievable benchmarks for quality improvement in systemic therapy for early-stage breast cancer. Cancer 2017, 123, 3772–3780. [Google Scholar] [CrossRef] [Green Version]
- Wallerstedt, S.M.; Ek, A.N.; Bagge, R.O.; Kovács, A.; Strandell, A.; Linderholm, B. Personalised medicine and the decision to withhold chemotherapy in early breast cancer with intermediate risk of recurrence—A systematic review and meta-analysis. Eur. J. Clin. Pharmacol. 2020, 76, 1199–1211. [Google Scholar] [CrossRef]
- Al-Naqqash, M.A. The 21-gene oncotype DX offers more accurate treatment decisions in early breast cancer. Gastric Breast Cancer 2020, 15, 1–7. [Google Scholar] [CrossRef]
- Perez, E.A. Breast Cancer Management: Opportunities and Barriers to an Individualized Approach. Oncologist 2011, 16, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Van Hoeve, J.; De Munck, L.; Otter, R.; De Vries, J.; Siesling, S. Quality improvement by implementing an integrated oncological care pathway for breast cancer patients. Breast 2014, 23, 364–370. [Google Scholar] [CrossRef]
- El-Alti, L.; Sandman, L.; Munthe, C. Person Centered Care and Personalized Medicine: Irreconcilable Opposites or Potential Companions? Health Care Anal. 2017, 27, 45–59. [Google Scholar] [CrossRef] [Green Version]
- Nardini, C.; Osmani, V.; Cormio, P.G.; Frosini, A.; Turrini, M.; Lionis, C.; Neumuth, T.; Ballensiefen, W.; Borgonovi, E.; D’Errico, G. The evolution of personalized healthcare and the pivotal role of European regions in its implementation. Pers. Med. 2021, 18, 283–294. [Google Scholar] [CrossRef]
- Maes-Carballo, M.; Martín-Díaz, M.; Mignini, L.; Khan, K.; Trigueros, R.; Bueno-Cavanillas, A. Evaluation of the Use of Shared Decision Making in Breast Cancer: International Survey. Int. J. Environ. Res. Public Health 2021, 18, 2128. [Google Scholar] [CrossRef]
- Panella, M.; Marchisio, S.; Di Stanislao, F. Reducing clinical variations with clinical pathways: Do pathways work? Int. J. Qual. Health Care 2003, 15, 509–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smeds, M. Managing Care Pathways for Patients with Complex Care Needs; Linköping University Electronic Press: Linköping, Sweden, 2019; Available online: http://urn.kb.se/resolve?urn=urn:nbn:se:liu:diva-156836 (accessed on 20 May 2021).
- Elwyn, G.; Laitner, S.; Coulter, A.; Walker, E.; Watson, P.; Thomson, R. Implementing shared decision making in the NHS. BMJ 2010, 341, c5146. [Google Scholar] [CrossRef] [Green Version]
- Committee on Improving the Quality of Cancer Care: Addressing the Challenges of an Aging Population, Board on Health Care Services, Institute of Medicine. Delivering High-Quality Cancer Care: Charting a New Course for a System in Crisis; Levit, L., Balogh, E., Nass, S., Ganz, P.A., Eds.; National Academies Press (US): Washington, DC, USA, 2013. Available online: http://www.ncbi.nlm.nih.gov/books/NBK202148/ (accessed on 19 May 2021).
- Elwyn, G.; Frosch, D.; Thomson, R.; Joseph-Williams, N.; Lloyd, A.; Kinnersley, P.; Cording, E.; Tomson, D.; Dodd, C.; Rollnick, S.; et al. Shared Decision Making: A Model for Clinical Practice. J. Gen. Intern. Med. 2012, 27, 1361–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenfeld, E.M.; Mader, S.; Houghton, C.; Wenger, R.; Probst, M.A.; Schoenfeld, D.A.; Lindenauer, P.K.; Mazor, K.M. The Effect of Shared Decisionmaking on Patients’ Likelihood of Filing a Complaint or Lawsuit: A Simulation Study. Ann. Emerg. Med. 2019, 74, 126–136. [Google Scholar] [CrossRef]
- Maes-Carballo, M.; Muñoz-Núñez, I.; Martín-Díaz, M.; Mignini, L.; Bueno-Cavanillas, A.; Khan, K.S. Shared decision making in breast cancer treatment guidelines: Development of a quality assessment tool and a systematic review. Health Expect. 2020, 23, 1045–1064. [Google Scholar] [CrossRef] [PubMed]
- Bodenheimer, T.; Sinsky, C. From Triple to Quadruple Aim: Care of the Patient Requires Care of the Provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Study | Overall % | Quality |
|---|---|---|
| Biganzoli et al. 2017 [27] | 83% | Group 1 |
| Fountzilas et al. 2018 [25] | 83% | Group 1 |
| Rosa 2015 [24] | 83% | Group 1 |
| Jacobs et al. 2017 [40] | 90% | Group 1 |
| Weldon et al. 2012 [34] | 90% | Group 1 |
| Zardavas et al. 2013 [41] | 83% | Group 1 |
| Cowppli-Bony et al. 2019 [42] | 60% | Group 2 |
| Powis et al. 2017 [44] | 60% | Group 2 |
| Wallerstedt et al. 2020 [45] | 55% | Group 2 |
| Saini et al. 2019 [31] | 67% | Group 2 |
| Schnapper et al. 2018 [37] | 70% | Group 2 |
| Komatsu et al. 2014 [39] | 70% | Group 2 |
| McGowan et al. 2016 [33] | 60% | Group 2 |
| Wright et al. 2019 [35] | 60% | Group 2 |
| Kurian et al. 2017 [38] | 60% | Group 2 |
| Kurian et al. 2015 [43] | 67% | Group 2 |
| Trivedi et al. 2019 [26] | 58% | Group 2 |
| Tischler et al. 2019 [29] | 42% | Group 3 |
| Girotra et al. 2016 [30] | 42% | Group 3 |
| Lyman et al. 2013 [28] | 33% | Group 3 |
| Laronga et al. 2012 [32] | 50% | Group 3 |
| Roberts et al. 2016 [36] | 30% | Group 3 |
| van Hoeve et al. 2014 [48] | 27% | Group 3 |
| Al-Naqqash 2020 [46] | 45% | Group 3 |
| Perez 2011 [47] | 33% | Group 3 |
| Study | Country | Study Design | Sample (Ethnicity/Age) | Type of BC | PM or/and PC | Dimensions Involved | Barriers | Success Factors |
|---|---|---|---|---|---|---|---|---|
| Van Hoeve et al. 2014 | The Netherlands | Cohort | NA | Primary BC | Both | Evidence based genetic testing (Shared) clinical decision-making Audit/feedback Evidence based application | Lack of clinicians’ involvement in critical pathways’ construction | Data-derived benchmarking for quality improvements |
| Cowppli-Bony et al. 2019 | France | Cross-sectional | Median age 61 | Primary invasive non-metastatic BC | PC | Audit/feedback Evidence based application | Heterogeneous adherence to guidelines among facilities | Data-derived benchmarking for quality improvements |
| Al-Naqqash 2020 | Iraq | Prospective cohort study | Mean age 54 | Grade I or grade II cancer, and HER2 negative status | PM | Evidence based genetic testing (Shared) clinical decision-making | Lack of public reimbursement scheme for diagnostics in study context Scarce adherence to guidelines | |
| Powis et al. 2017 | Canada | Retrospective analysis | Age ≥ 65 years | Early-stage BC | PC | Evidence based application | Lack of standardization in treatment and clinical practice | Data-derived benchmarking for quality improvements |
| McGowan et al. 2016 | USA | Qualitative study | Median age 54 | Advanced BC | PM | Molecular board | Insufficient integration and engagement of geneticist in MGTB and in counselling Lack of geneticist-patient relationship | Multi-professional and multi-specialist collaboration |
| Weldon et al. 2012 | USA | Qualitative study | NA | Any | PM | Evidence based genetic testing (Shared) clinical decision-making | Lack of public reimbursement scheme for diagnostics in study context Poor timing and seguencing of test relative to decisions Counterincentives to appropriate use of genetic test | Stakeholders’ collaboration with a larger role for patient advocates |
| Wright et al. 2019 | UK | Qualitative study | NA | Any | PM | Molecular board Evidence based genetic testing (Shared) clinical decision-making | Clear allocation of tasks between oncologists and geneticists | |
| Roberts et al. 2016 | North Carolina | Qualitative study | NA | Early stage, hormone receptor positive BC, with lymph node negative or lymph node positive disease | PC | Communication | Patients excluded from choices regarding genetic tests | Communication with patients tailored to their needs and background |
| Schnapper et al. 2018 | Italy | Qualitative study | NA | Any | PC | Informative systems | Non-uniform professional profile of DM at EU level | |
| Kurian et al. 2017 | USA | Qualitative study | Black, Asian, Hispanic and white women age 20 to 79 years | Early-stage BC | Both | Evidence based genetic testing Communication (Shared) clinical decision-making | Insufficient integration and engagement of geneticist in counseling Cost barriers to effective testing despite price reduction | Communication with patients tailored to their needs and background |
| Komatsu et al. 2014 | Japan | Qualitative study | NA | Any | Both | Evidence based genetic testing Communication Informative system Multidisciplinary approach | Delay in adoption of new technologies in clinical practice Fragmented communication of genetic data among multidisciplinary professionals | Education and training on genetic testing also among non-geneticists |
| Jacobs 2017 | UK | Delphi study | Median age 53 | Any | Both | Molecular board Communication Multidisciplinary approach | Protocols for doctor-patient communication on (pre and post) genetic testing | |
| Kurian 2015 | Invited Commentary | NA | Any | PM | Evidence based genetic testing (Shared) clinical decision-making | Shared decision-making between patients and clinicians | ||
| Rosa 2015 | USA | Narrative review | NA | Any | PM | Molecular board Evidence based genetic testing (Shared) clinical decision-making | Patologists’ knowledge on genetic test | |
| Fountzilas et al. 2018 | Narrative review | NA | Any | Both | Evidence based genetic testing Multidisciplinary approach | Education and training on genetic testing | ||
| Trivedi et al. 2019 | Narrative review | NA | Any | Both | Molecular board Evidence based genetic testing Multidisciplinary approach | Multiprofessional and multispecialist collaboration | ||
| Biganzoli et al. 2017 | Narrative review | NA | Any | PC | Audit/feedback | Lack of outcome indicators | ||
| Lyman et al. 2013 | Narrative review | NA | Any | PM | Molecular board | Multiprofessional and multispecialist collaboration | ||
| Tischler et al. 2019 | Narrative review | NA | Any | Both | Evidence based genetic testing (Shared) clinical decision-making Communication Multidisciplinary approach | Scarse diffusion of unique vocabulary to guide therapy strategies | Utilization of personalized medicine prevention techniques | |
| Girotra et al. 2016 | Narrative review | NA | Any | PM | Evidence based genetic testing (Shared) clinical decision-making | Utilization of personalized medicine prevention techniques | ||
| Geetanjali et al. 2019 | Narrative review | NA | Any | Both | Evidence based genetic testing (Shared) clinical decision-making Multidisciplinary approach | Dynamicity of genomic data generation and gathering | Multiprofessional and multispecialist collaboration | |
| Laronga et al. 2012 | Narrative review | NA | Newly diagnosed, estrogen receptor (ER)-positive, node-negative, early-stage BC treated with endocrine therapy | PM | Molecular board Evidence based genetic testing (Shared) clinical decision-making | Multiprofessional and multispecialist collaboration | ||
| Zardavas 2013 | Review | NA | Any | PM | Evidence based genetic testing (Shared) clinical decision-making | Lack of systematic approach to the adoption of new technologies in clinical practice | Creation of unique vocabulary to guide therapy strategies | |
| Perez 2011 | USA | Review | NA | Any | Both | Molecular board Evidence based genetic testing Multidisciplinary approach | Evidence based on evaluation of personalized medicine only for primary breast cancer | Multiprofessional and multispecialist collaboration |
| Wallerstedt et al. 2020 | Sweden | Systematic review | NA | Post-surgical BC | PM | Evidence based genetic testing (Shared) clinical decision-making | Lack of evidence of therapy effects on HRQL | Utilization of personalized medicine prevention techniques |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Belvis, A.G.; Pellegrino, R.; Castagna, C.; Morsella, A.; Pastorino, R.; Boccia, S. Success Factors and Barriers in Combining Personalized Medicine and Patient Centered Care in Breast Cancer. Results from a Systematic Review and Proposal of Conceptual Framework. J. Pers. Med. 2021, 11, 654. https://doi.org/10.3390/jpm11070654
de Belvis AG, Pellegrino R, Castagna C, Morsella A, Pastorino R, Boccia S. Success Factors and Barriers in Combining Personalized Medicine and Patient Centered Care in Breast Cancer. Results from a Systematic Review and Proposal of Conceptual Framework. Journal of Personalized Medicine. 2021; 11(7):654. https://doi.org/10.3390/jpm11070654
Chicago/Turabian Stylede Belvis, Antonio Giulio, Rossella Pellegrino, Carolina Castagna, Alisha Morsella, Roberta Pastorino, and Stefania Boccia. 2021. "Success Factors and Barriers in Combining Personalized Medicine and Patient Centered Care in Breast Cancer. Results from a Systematic Review and Proposal of Conceptual Framework" Journal of Personalized Medicine 11, no. 7: 654. https://doi.org/10.3390/jpm11070654
APA Stylede Belvis, A. G., Pellegrino, R., Castagna, C., Morsella, A., Pastorino, R., & Boccia, S. (2021). Success Factors and Barriers in Combining Personalized Medicine and Patient Centered Care in Breast Cancer. Results from a Systematic Review and Proposal of Conceptual Framework. Journal of Personalized Medicine, 11(7), 654. https://doi.org/10.3390/jpm11070654