Abstract
Background/Objectives: Odontogenic keratocysts are benign cysts originating from remnants of the dental lamina, rarely showing peripheral (gingival) localization. In this study, we compiled data on the peripheral variant by reviewing the literature and presenting a new case to establish criteria for accurate differential diagnosis and treatment. Methods: A systematic literature review was conducted following the PRISMA flowchart, leading to the collection of existing data on peripheral odontogenic keratocyst. In addition, we present a new case of a 68-year-old female patient referred to our attention for an asymptomatic swelling of the mandible in the premolar area. Radiographic examination revealed a round radiolucency with well-defined borders located between teeth #4.3 and #4.4, surgically removed and diagnosed as a peripheral (gingival) keratocyst. Results: Including the herein described new case, 37 cases were reviewed from data literature showing occurrence in the mandible (43.2%) and maxilla (46%)—with 10.8% of cases not stated-, with an age range of 14–83 year old, recurrence rate of 12.5–13.6% (total recurrences/total cases) and median follow-up time of 19 months. Conclusions: Data from literature highlights the rarity of odontogenic keratocyst with peripheral (gingival) localization, which can be misleading for differential diagnosis, emphasizing the necessity of histopathological examination as the definitive diagnostic tool for all the cystic lesions of the jaws. The absence of pathognomonic clinical and radiological features, combined with the potential for extraosseous manifestation of odontogenic lesions with high recurrence rates, underscores the importance of complete excision to ensure proper healing and prevent recurrence of odontogenic keratocyst.
1. Introduction
Among odontogenic lesions, the odontogenic keratocyst (OKC) is a common occurrence in the oral cavity, typically characterized by its aggressive and locally invasive nature. It originates from the remnants of the dental lamina and constitutes approximately 10–20% of all jaw cysts [1]. Compared to other odontogenic cysts, OKC has a high recurrence rate (up to 62.5%) and exhibits significant local aggressiveness. Approximately 80% of cases occur in the mandibular region, with a notable preference for the posterior area and the mandibular ramus [2]. Due to its asymptomatic nature, OKC is often diagnosed incidentally through routine radiographic examinations, appearing as either a unilocular or multilocular well-defined radiolucency. Particularly in young patients, it may be associated with an impacted tooth in approximately 30% of cases. Histopathological examination reveals that the cystic lumen contains a creamy, straw-colored fluid, mainly composed of keratin granules. Complete surgical excision remains a challenge due to the exceptionally thin epithelial wall.
Although traditionally considered a subtype of OKC, in 2022, the 5th Edition of the World Health Organization Classification of Head and Neck Tumors reclassified the peripheral variant as a distinct entity due to its unique clinical, histopathological, and biological characteristics.
The extraosseous variant, also referred to as the peripheral odontogenic keratocyst (POKC), is exceedingly rare, with only 36 cases described in the literature [3]. Clinically, it typically presents as a fluctuant soft tissue swelling, ranging from 3 mm to 5 cm in size. It may also be associated with infection, sometimes exhibiting purulent exudate. Radiographic imaging is essential for evaluating lesion localization and potential bony involvement. Orthopantomography is sufficient for assessing bony changes; however, a CT scan is required for a more precise delineation of the lesion’s size, borders, and anatomical relationships [2,3,4,5]. While POKC is generally not apparent on radiographs, it may occasionally present as a unilocular or multilocular radiolucent lesion, resembling other odontogenic cysts and neoplasms [3,4,5].
The presence of extraosseous lesions in the oral cavity presents a significant diagnostic challenge for pathologists and surgeons, often necessitating surgical removal. Differential diagnoses should include inflammatory lesions (e.g., inflammatory cysts, pyogenic granulomas, epulis fissuratum, or dental abscesses) and non-inflammatory lesions (e.g., peripheral giant cell granuloma, lateral periodontal cyst [LPC], gingival cyst of the adult [GCA], peripheral ameloblastoma, peripheral ossifying fibroma, mucocele, fibroma, or vascular lesion). Although benign, POKC exhibits a tendency for recurrence, highlighting the importance of accurate diagnosis and appropriate management. This study aims to review the epidemiology, clinical features, diagnosis, histopathological characteristics, treatment options, recurrence rates, and long-term outcomes of POKC. Additionally, a new case with a gingival manifestation is described, contributing further data to guide the differential diagnosis of peripheral lesions in the oral cavity.
2. Materials and Methods
2.1. Literature Analysis
2.1.1. Protocol and Registration
The study protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO)—Registration number: 1043819.
2.1.2. Search Strategy
A systematic electronic search was performed based on the PICO criteria (Table 1). The research question was formulated as follows: In adults, what are the clinical and histopathological features (I), in relation to other similar peripheral lesions (C), of peripheral keratocysts (P) that enable a better understanding of recurrence rates and long-term outcomes (O)?

Table 1.
Search strategy according to the PICO criteria [6].
A comprehensive systematic review was conducted by four independent reviewers (M.F., A.M., G.D., and S.C.), covering the period from November 2024 to February 2025. The search was performed using a combination of keywords and Medical Subject Headings (MeSH) terms, including: “Peripheral Odontogenic Keratocyst” OR “POKC” AND “Oral Cavity” OR “Odontogenic Keratocyst” AND “Peripheral.”
Articles published between 1974 and 2024 were evaluated for relevance based on their focus on the clinical, histopathological, or treatment-related aspects of POKC. These included studies reporting cases with a histological diagnosis of POKC, case series, case reports, and reviews. Studies that did not specifically address POKC, those lacking a histological diagnosis of POKC, those based on animal models, or case reports with insufficient data were excluded. This study followed the PRISMA Statement guidelines of Preferred Reporting Items of Systematic Review, as also summarized in Figure 1.
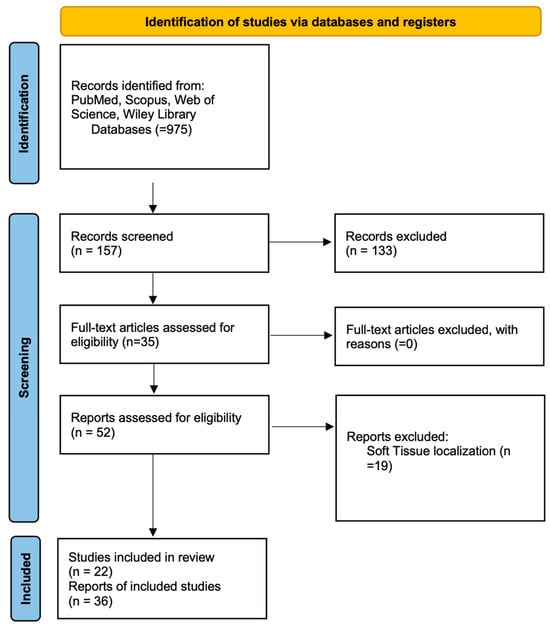
Figure 1.
Search results were conducted and reported in accordance with the PRISMA 2020 statement.
Additionally, cases involving buccal mucosa lesions with immunopathological characteristics consistent with POKC were identified but excluded from the review due to the difficulty in demonstrating their odontogenic nature, according to the opinion of some authors [7,8,9]. In support of this latter theory, we gathered a series of buccal mucosa POKC (Table 2) that were excluded from our review.
Table 2.
Summary of POKC cases reported in the literature.
3. Results
3.1. Case Presentation
A 68-year-old female patient presenting with a small, asymptomatic swelling of the gingiva between the right mandibular canine and first premolar was referred to the University of Bari “Aldo Moro.” The patient denied any history of trauma and reported the lesion’s presence for approximately one year. There was no family history of genetic syndromes or other relevant conditions. Intraoral examination revealed a well-defined, firm, asymptomatic lesion measuring approximately 1.5–2 cm in diameter, confined to the vestibular gingival surface in the region of teeth #4.3 and #4.4 (Figure 2A). Both involved teeth responded positively to vitality testing. Radiographic examination showed a round radiopaque lesion with well-defined radiolucent borders between the roots of #4.3 and #4.4 (Figure 2B,C). Under local anesthesia, a mucoperiosteal marginal flap was elevated, showing the entire lesion. During enucleation, the cystic wall ruptured, releasing a dense, straw-colored fluid; following complete lesion removal, significant alveolar bone resorption was noted, with the lesion in contact with the roots (Figure 3A–C). The cavity was meticulously curetted and the involved roots as well, and the flap was sutured with Vicryl 5/0. The specimen was fixed in 10% formalin and sent for histopathological analysis (Figure 3D). Microscopic examination revealed a stratified squamous epithelium with a parakeratotic epithelial surface and a hyperchromatic, palisaded basal cell layer, leading to the diagnosis of POKC (Figure 4). The postoperative course was uneventful, with no complications observed. Clinical and radiological follow-up at three-month intervals showed no recurrence (Figure 5). Figure 6 summarizes the diagnostic and therapeutic pathway.
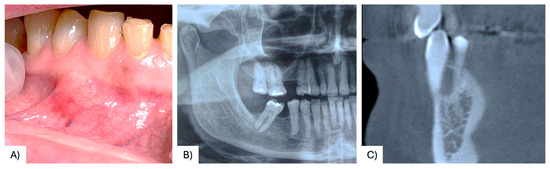
Figure 2.
Small swelling of the vestibular gingiva in the region of #43 and #44 (A); radiograph showing a roundish radiolucency with radiolucent borders between elements #4.3 and #4.4 (B,C).
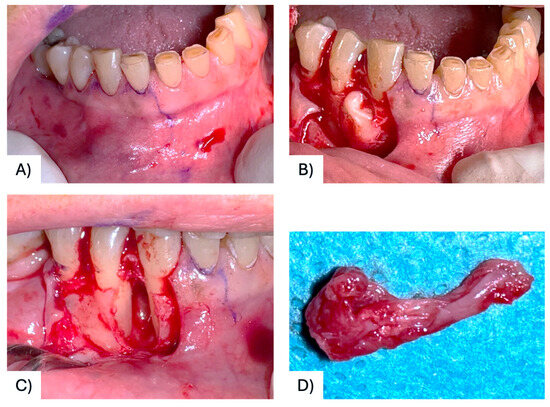
Figure 3.
Surgical design of the flap to access the lesion (A); mucoperiosteal flap elevation showing the cystic lesion located between #43 and #44 (B); intraoperative view after cyst removal and curettage (C); The surgical specimen (D).
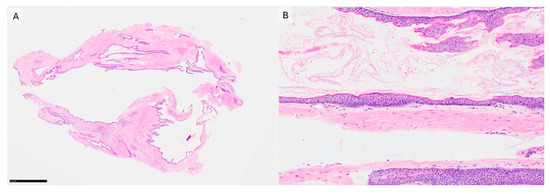
Figure 4.
(A) Low power magnification showing the overall cystic architecture of the lesion (H&E, 20×). (B) High power magnification showing a para-keratinized stratified squamous epithelium with a palisaded basal cell layer surrounding connective tissue (HE, 100×).
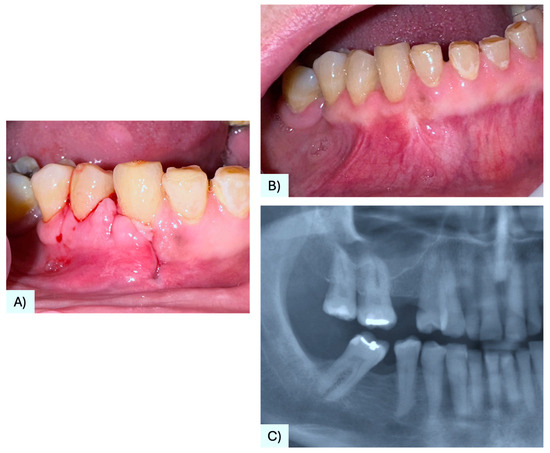
Figure 5.
Partial healing of the treated area at 3 weeks clinical follow-up (A); complete clinical healing of the soft tissue at 2 months follow-up (B); 3 months radiographic follow-up showing no bone alteration, also with healing of the treated site (C).
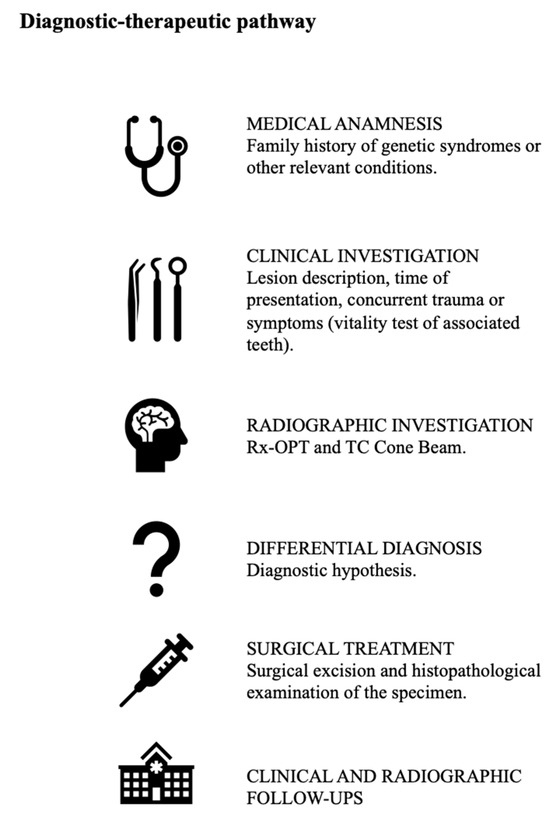
Figure 6.
Summary of the current diagnostic-therapeutic pathway.
3.2. Literature Analysis
From data research, only 22 articles matched the inclusion criteria; 36 cases were described and summarized in Table 2.
Based on the analyzed data, the literature reports only 37 cases with a histological diagnosis of Peripheral Odontogenic Keratocyst (POKC) from 1975 to 2024. These cases include 19 females, 11 males, and 5 individuals with unspecified gender, with ages ranging from 14 to 83 years old. Maxilla was the most prevalent site of manifestation, with 18 cases, mandible 16 cases, although 4 studies did not specify the site of occurrence. In most cases, no radiographic findings were reported, with only 9 cases showing radio-lucent areas with well-defined margins. Nearly all authors opted for surgical management of the lesion, primarily employing conservative enucleation or excision techniques. During the literature review, existing cases involving lesions of the buccal mucosa with immunopathological characteristics consistent with the diagnosis of POKC were also identified. However, according to several authors [7,8,9], these characteristics alone are not sufficient to classify such lesions as part of the same pathological entity described in this study, due to the ongoing difficulty in demonstrating their odontogenic origin. Supporting this position, a compilation of buccal mucosa POKC cases (summarized in Table 3) was excluded from the final review.
Table 3.
OKC cases localized in soft tissues and excluded from our study.
3.3. Quality Assessment and Risk of Bias
Quality assessment and risk of bias evaluation were evaluated by two reviewers (M.F. and G.D.) using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports, which included the reported studies (Table 4). In cases of disagreement, a third reviewer (L.L.) was consulted to resolve discrepancies, and discussions continued until a consensus was achieved. This evaluation was assessed through eight questions (Q1–Q8). Q1: Does the case report clearly describe the patient’s age, sex, race, medical history, diagnosis, prognosis, previous treatments, past and current diagnostic test results, and medications? The setting and context; Q2: A good case report will clearly describe the history of the patient, their medical, family and psychosocial history including relevant genetic information, as well as relevant past interventions and their outcomes (CARE Checklist 2013); Q3: The current clinical condition of the patient should be described in detail including the uniqueness of the condition/disease, symptoms, frequency and severity. The case report should also be able to present whether differential diagnoses was considered may also be described; Q4: A reader of the case report should be provided sufficient information to understand how the patient was assessed. It is important that all appropriate tests are ordered to confirm a diagnosis, and therefore, the case report should provide a clear description of various diagnostic tests used (whether a gold standard or alternative diagnostic tests). Photographs or illustrations of diagnostic procedures, radiographs, or treatment procedures are usually presented when appropriate to convey a clear message to readers; Q5: It is important to clearly describe treatment or intervention procedures, as other clinicians will be reading the paper and therefore may enable a clear understanding of the treatment protocol. The report should describe the treatment/intervention protocol in detail; for e.g., in pharmacological management of dental anxiety—the type of drug, route of administration, drug dosage and frequency, and any side effects; Q6: A good case report should clearly describe the clinical condition post-intervention in terms of the presence or lack thereof symptoms. The outcomes of management/treatment when presented as images or figures would help in conveying the information to the reader/clinician. Q7: With any treatment/intervention/drug, there are bound to be some adverse events and, in some cases, they may be severe. It is important that adverse events are clearly documented and described, particularly when a new or unique condition is being treated or when a new drug or treatment is used. In addition, unanticipated events, if any, that may yield new or useful information should be identified and clearly described; Q8: Case reports should summarize key lessons learned from a case in terms of the background of the condition/disease and clinical practice guidance for clinicians when presented with similar cases. Ref [37] Most of the included studies exhibited a low overall risk of bias, indicating solid methodological rigor and reliability of outcomes. However, certain domains—particularly those related to incomplete demographic data, radiographic evaluation and outcomes—revealed moderate concerns, underscoring the need for enhanced transparency and data management in future studies.
Table 4.
Risk of Bias assessment. [Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports].
4. Discussion
OKC is one of the most frequently diagnosed cystic lesions. In 2005, the WHO classified OKC as a benign neoplasm due to the presence of mutations in the Protein Patched Homolog 1 (PTCH) tumor suppressor gene. These mutations have since been identified in non-neoplastic lesions, leading the WHO to reclassify OKC as an odontogenic cyst in 2017. Despite this latest classification, its locally aggressive behavior and invasiveness often require a more radical treatment approach to ensure complete removal and healing without recurrence [5]. OKC with peripheral manifestations represents an extraosseous variant known as POKC, which remains extremely rare and poorly documented in the literature [3].
4.1. Pathogenesis
The pathogenesis of POKC remains incompletely understood. It is believed to originate from remnants of the dental lamina or the rests of Malassez within the gingival tissue. These remnants may proliferate, forming a cystic lesion with keratinizing epithelial linings. Unlike central OKCs, POKCs do not invade bone but remain confined to the peripheral gingival tissues. Some studies suggest that genetic mutations may contribute to its development, while other hypotheses propose that local inflammatory stimuli or trauma could act as triggering factors [7,8,9,10,11,12,13,14,15,16,17,18,20,21,22,23,24,25,26,27].
4.2. Clinical and Radiographical Features
POKC typically presents as an asymptomatic nodular swelling of soft tissue, with variations in color from white to yellow and consistency ranging from fluctuant to firm. The most commonly reported anatomical site is the vestibular gingiva, with an average size of 0.8 cm (range: 0.15–2.5 cm) [1,2,3,4,5]. Palatal or lingual gingival involvement is rarely documented [23,24]. The lesion may initially appear small but can gradually enlarge over time. Some patients report mild discomfort or tenderness, particularly if secondary infection occurs. In advanced cases, POKC may cause displacement of adjacent teeth, though significant bone destruction is uncommon. POKC is usually not associated with other odontogenic or systemic disorders, although a few cases have been linked to nevoid basal cell carcinoma syndrome (Gorlin-Goltz syndrome). Clinical differential diagnosis should include a variety of odontogenic cysts, neoplasms, and non-odontogenic lesions with similar clinical presentations [8,17]. The main characteristics of POKC differential diagnoses are summarized in Table 4.
4.3. Histopathological Features
Distinct histological characteristics enable pathologists to identify POKC. The cystic wall is composed of stratified parakeratinized squamous epithelium with a palisaded basal cell layer. Multiple invaginations of the epithelium may also be observed. The cystic lumen contains a thick, straw-colored, creamy fluid composed of keratin [5,32]. Although histologically similar to its central intraosseous counterpart, some studies have shown that POKC exhibits a lower percentage of microcysts within the fibrous capsule (12.5%) [1]. To date, no standardized immunohistochemical profile for POKC has been established in the literature. However, Lafuente-Ibanez de Mendoza et al., in their description of three cases, found that all exhibited intense CK14 expression and irregular epithelial CK19 expression [1].
4.4. Differential Diagnosis of Peripheral Odontogenic Lesion
Given the rarity of POKC, only a limited number of cases have been described in the literature. Its diagnosis requires a combination of clinical, radiological, and histopathological evaluations. Clinical diagnosis is based on the lesion’s gingival location and characteristic presentation as a painless, slow-growing mass. In some cases, radiographic imaging may reveal a small radiolucent area at the lesion site, although bone involvement is typically absent or minimal. Panoramic radiographs may show a soft-tissue mass without bony destruction, distinguishing POKC from the central form of OKC [1,2,3,8,9,19,22,23,24,25,26,27,30,38,39]. Histological examination remains the gold standard for differential diagnosis, as it confirms a cystic structure lined by stratified squamous epithelium with orthokeratinization or parakeratinization. The epithelium typically exhibits a characteristic corrugated appearance and may contain areas of keratin production. The cyst wall is generally devoid of significant inflammation or fibrosis, distinguishing it from other odontogenic lesions [5,32]. The diagnosis of POKC requires careful differentiation from several other lesions that may present with similar clinical and radiological features. These include peripheral giant cell granuloma, gingival cyst of the adult (GCA), adenomatoid odontogenic tumor (AOT), inflammatory odontogenic cyst, lateral periodontal cyst (LPA), and peripheral ameloblastoma [32,33,34,35,36,40,41,42]. The key distinguishing characteristics of these lesions are summarized in Table 5 and Table 6.
Table 5.
Summary of the main clinicopathological features of lesions included in the differential diagnosis of POKC [32,33,40].
Table 6.
Differences between intraosseous and peripheral subvariants [1,4].
In the present case, the lesion’s location between mandibular teeth #4.3 and #4.4, along with a positive vitality test, initially suggested a gingival cyst of the adult (GCA) [40,43] or lateral periodontal cyst (LPA) [44]. However, certain clinical features, particularly the fragility of the cystic wall and the release of a straw-colored fluid upon rupture, were indicative of OKC and have been similarly reported in previous studies [1,3,17,20,26]. Overall, differentiating POKC from other gingival lesions requires a comprehensive clinical, radiological, and histopathological assessment. The key distinguishing features include the presence of keratinized epithelium, lack of bone involvement, and specific histopathological patterns seen in peripheral giant cell granuloma, lateral periodontal cyst, and ameloblastoma. Accurate diagnosis is crucial to determining the most appropriate treatment and ensuring a favorable prognosis. Furthermore, distinguishing intraosseous OKCs from their peripheral counterparts is essential and is based on specific clinical, radiological, and histopathological characteristics, as summarized in Table 6.
4.5. Recurrences and Prognosis
According to existing data, POKC has a significantly lower recurrence rate than the intraosseous variant, with recurrence rates reported at 12.5–13.6% (Table 5) [4,28,29,31,45]. The reason for this lower recurrence rate remains unclear, but two hypotheses have been proposed: (1) the greater ease of complete surgical excision at the soft tissue level, and (2) a potentially distinct biological behavior of the peripheral variant compared to its central counterpart, suggesting it may represent a separate pathological entity [4]. Factors contributing to recurrence include incomplete excision, inadequate follow-up, and lesion size at the time of initial treatment. Most recurrences occur within the first five years post-treatment, although long-term follow-up is recommended [19,22,23,25,38,39]. In this study, the patient underwent clinical follow-ups every three months, with no signs of recurrence observed. The prognosis for POKC is generally favorable when complete excision is achieved, with most patients experiencing no further complications. Recurrence, when it occurs, is typically local and does not result in systemic involvement or malignancy [8,9,19,23,24,25,26,27,38,39].
4.6. Treatment Modalities
The management of peripheral odontogenic lesions is challenging due to their lack of radiographic appearance and difficulties in differential diagnosis. Surgical excision remains the primary treatment for POKC. The goal is to achieve complete removal with clear margins to prevent recurrence. The surgical approach is often conservative, involving soft tissue excision with minimal bone involvement. In some cases, curettage may be performed, but this carries a higher recurrence risk. Complete removal of the epithelial lining is essential, as incomplete excision is a common cause of recurrence. For larger lesions, adjunctive treatments such as cryotherapy or peripheral ostectomy may be considered, although their use remains controversial. In this case, excisional biopsy combined with thorough curettage ensured a low recurrence rate and complete healing of the surgical site [3,4,8,9,19,23,24,25,26,27,38].
5. Conclusions
POKC is a rare, benign odontogenic lesion that presents in the gingival tissue. It typically manifests as a painless, slow-growing mass and requires a combination of clinical, radiological, and histopathological assessments for diagnosis. Surgical excision with clear margins remains the treatment of choice. Although prognosis is generally favorable, long-term follow-up is essential to monitor for recurrence. Future research into molecular and genetic markers may provide further insights into the pathogenesis of POKC and contribute to the development of targeted therapeutic strategies. Nonetheless, the present study is inherently limited by the scarcity of reported case series in the literature, which constrains the ability to draw statistically robust conclusions and limits the generalizability of the findings. This underscores the need for larger, multicenter investigations and systematic data collection to improve diagnostic accuracy, refine treatment protocols, and better understand the biological behavior of this uncommon entity.
Author Contributions
Conceptualization, M.F. and G.D.; methodology, L.L.; software, G.I.; validation, S.C., A.M. and E.C.; formal analysis, G.D.; investigation, G.C.; resources, A.d.; data curation, S.C. and G.P.; writing—original draft preparation, M.F. and A.M.; writing—review and editing, E.C. and L.L.; visualization, A.d.; supervision, G.C.; project administration, S.C.; funding acquisition, S.C. and G.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The current study has been approved by the Independent Ethical Committee of the Aldo Moro University of Bari, which approved the study protocol (study number 4576, code 1443/CE, approval date: 23 April 2022).
Informed Consent Statement
Written informed consent for publication was obtained from the patient.
Data Availability Statement
The data collected in the current study were downloaded from the following databases: PubMed (https://pubmed.ncbi.nlm.nih.gov; URL accessed 1 November 2024), Scopus (https://www.scopus.com; URL accessed on 1 November 2024), Web of Science (https://clarivate.com/academia-government/scientific-and-academic-research/research-discovery-and-referencing/web-of-science/; URL accessed on 1 November 2024), and Wiley Library (https://onlinelibrary.wiley.com; URL accessed on 1 November 2024).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- de Mendoza, I.L.; Aguirre-Urizar, J.M.; Villatoro-Ugalde, V.; Magaña-Quiñones, J.; Lana-Ojeda, J.; Mosqueda-Taylor, A. Peripheral odontogenic keratocyst: Clinicopathological and immunohistochemical characterization. Oral Dis. 2022, 28, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Romero, M.; Serrera-Figallo, M.; Alberdi-Navarro, J.; Cabezas-Talavero, J.; Romero-Ruiz, M.; Torres-Lagares, D.; Aguirre-Urizar, J.; Gutierrez-Perez, J. Maxillary peripheral keratocystic odontogenic tumor. A clinical case report. J. Clin. Exp. Dent. 2017, 9, e167–e171. [Google Scholar] [CrossRef]
- Brooks, J.K.; Sultan, A.S.; Rabkin, M.P.; Sands, J.M.; Everett, D.E.; Price, J.B.; Basile, J.R. Recurrent peripheral odontogenic keratocyst: Review of the literature and presentation of a novel case initially masquerading as an atypical infected lateral periodontal cyst. J Stomatol. Oral Maxillofac. Surg. 2024, 125, 101540. [Google Scholar] [CrossRef] [PubMed]
- Villota, M.H.-D.; Pampin-Martínez, M.M.; Moran-Soto, J.; Cebrián-Carretero, J.-L. Peripheral odontogenic keratocyst. A Case report. J. Clin. Exp. Dent. 2023, 15, e169–e172. [Google Scholar] [CrossRef]
- Shathur, A.; Patel, B.; Pitiyage, G.; Cameron, S.; Hyde, N. Odontogenic keratocyst located in the retromolar trigone. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 132, e82–e85. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yih, W.; Zieper, M.; Kratochvil, F.; Stewart, J. Immunohistochemical analysis of the expression of p53, bcl-2, and Ki-67 in peripheral odontogenic keratocyst and gingival cyst of the adult. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2000, 90, 493. [Google Scholar]
- Rodrigues, B.; Israel, M.; de Moura, K.; Pinheiro, G.; Carlos, R.; Pires, F. Peripheral odontogenic keratocyst: Report of two new cases and review of the literature. J. Clin. Exp. Dent. 2020, 12, e1005–e1010. [Google Scholar] [CrossRef]
- Precheur, H.V.; Krolls, S.O. An unusual presentation of an odontogenic keratocyst in the buccal space: Case report. J. Oral Maxillofac. Surg. 2009, 67, 2513–2515. [Google Scholar] [CrossRef] [PubMed]
- Stoelinga, P.J.; Cohen, M.M., Jr.; Morgan, A.F. The origin of keratocysts in the basal cell nevus syndrome. J. Oral. Surg. 1975, 33, 659–663. [Google Scholar] [PubMed]
- Buchner, A.; Hansen, L.S. The histomorphologic spectrum of the gingival cyst in the adult. Oral Surg. Oral Med. Oral Pathol. 1979, 48, 532–539. [Google Scholar] [CrossRef]
- Dayan, D.; Buchner, A.; Gorsky, M.; Harel-Raviv, M. The peripheral odontogenic keratocyst. Int. J. Oral Maxillofac. Surg. 1988, 17, 81–83. [Google Scholar] [CrossRef]
- Chehade, A.; Daley, T.D.; Wysocki, G.P.; Miller, A.S. Peripheral odontogenic keratocyst. Oral Surg. Oral Med. Oral Pathol. 1994, 77, 494–497. [Google Scholar] [CrossRef]
- Fardal, O.; Johannessen, A.C. Rare case of keratin-producing multiple gingival cysts. Oral Surg. Oral Med. Oral Pathol. 1994, 77, 498–500. [Google Scholar] [CrossRef] [PubMed]
- Ide, F.; Shimoyama, T.; Horie, N. Peripheral odontogenic keratocyst: A report of 2 cases. J. Periodontol. 2002, 73, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Chi, A.C.; Owings, J.R.; Muller, S. Peripheral odontogenic keratocyst: Report of two cases and review of the literature. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. Endodontology 2005, 99, 71–78. [Google Scholar] [CrossRef]
- Preston, R.D.; Narayana, N. Peripheral odontogenic keratocyst. J. Periodontol. 2005, 76, 2312–2315. [Google Scholar] [CrossRef]
- Mozaffari, E.; Marmor, D.S.; Alawi, F. Odontogenic keratocyst with a misleading clinical and radiologic appearance. Quintessence Int. 2008, 38, 837–841. [Google Scholar]
- Kinaia, B.M.; Kinaia, M.; Graham, J.; Villaneuva, N.P.; Van Winkle, D.; Dawood, A.; Neely, A.L. Odontogenic keratocyst management using guided tissue regeneration: Literature review—Two case reports. Clin. Adv. Periodontics. 2024, 1–10. [Google Scholar] [CrossRef]
- Faustino, S.E.S.; Pereira, M.C.; Rossetto, A.C.; Oliveira, D.T. Recurrent peripheral odontogenic keratocyst: A case report. Dentomaxillofacial Radiol. 2008, 37, 412–414. [Google Scholar] [CrossRef]
- Ide, F.; Mishima, K.; Saito, I.; Kusama, K. Rare peripheral odontogenic tumors: Report of 5 cases and comprehensive review of the literature. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. Endodontology 2008, 106, e22–e28. [Google Scholar] [CrossRef]
- Jinbu, Y.; Ueno, Y.; Obi, Y.; Ikeda, K.; Kusama, M.; Tsukinoki, K. Peripheral keratocystic odontogenic tumour: A case report. Oral Surg. 2009, 2, 95–98. [Google Scholar] [CrossRef]
- Vij, R.; Vij, H.; Gupta, V.; Sengupta, S. Odontogenic keratocyst: A peripheral variant. Niger. J. Clin. Pr. 2011, 14, 504–507. [Google Scholar] [CrossRef]
- Sakamoto, K.; Morita, K.-I.; Shimada, Y.; Omura, K.; Izumo, T.; Yamaguchi, A. Peripheral odontogenic keratocyst associated with nevoid basal cell carcinoma syndrome: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, e19–e23. [Google Scholar] [CrossRef]
- Zhu, L.; Yang, J.; Zheng, J.W. Radiological and clinical features of peripheral keratocystic odontogenic tumor. Int. J. Clin. Exp. Med. 2014, 7, 300–306. [Google Scholar] [PubMed] [PubMed Central]
- Gröbe, A.; Hanken, H.; Blessmann, M.; Zustin, J.; Heiland, M.; Al-Dam, A. An odontogenic keratocystic tumor in the buccal space: An unusual site of origin and a review of the literature. In Vivo 2012, 26, 847–851. [Google Scholar]
- Yamamoto, K.; Matsusue, Y.; Kurihara, M.; Takahashi, Y.; Kirita, T. A keratocyst in the buccal mucosa with the features of keratocystic odontogenic tumor. Open Dent. J. 2013, 7, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Kaminagakura, E.; Almeida, J.; Carvalho, Y.; Franco, R.; Soares, F.; Rocha, R.; Kowalski, L. Keratocyst of the buccal mucosa: Case report and immunohistochemical comparative study with sporadic Intraosseous keratocystic odontogenic tumor. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, e387–e392. [Google Scholar] [CrossRef] [PubMed]
- Witteveen, M.E.; Flores, I.L.; Karssemakers, L.H.; Bloemena, E. Intramuscular keratocyst as a soft tissue counterpart of keratocystic odontogenic tumor: Differential diagnosis by immunohistochemistry. Hum. Pathol. 2014, 45, 110–118. [Google Scholar] [CrossRef]
- Makarla, S.; Bavle, R.M.; Muniswamappa, S.; Narasimhamurthy, S. A Large Extragnathic Keratocystic Odontogenic Tumour. Case Rep. Pathol. 2015, 2015, 723010. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Witteveen, M.E.; Flores, I.L.; Karssemakers, L.H.; Bloemena, E. Odontogenic keratocysts located in the buccal mucosa: A description of two cases and review of the literature. SAGE Open Med. Case Rep. 2019, 7, 2050313X19849828. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meleveetil, D.; Beena, V.; Cheriyan, L.; Angamuthu, K. Mucosal keratocyst of buccal mucosa: A rare entity. J. Oral Maxillofac. Pathol. 2020, 24, 589. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Watanabe, T. Recurrence of odontogenic keratocyst in the buccal space. BMJ Case Rep. 2022, 15, e246735. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mustakim, K.R.D.; Sodnom-Ish, B.D.; Yoon, H.-J.D.; Kim, S.M.D. Odontogenic Keratocyst in the Masseter Muscle. J. Craniofac. Surg. 2022, 33, e275–e276. [Google Scholar] [CrossRef] [PubMed]
- Kochaji, N.; Alshami, G.; Haddad, B. Primary odontogenic keratocyst in the cheek muscles: Report of the 4th case in the world and review of peripheral OKC literature. Int. J. Surg. Case Rep. 2023, 106, 108161. [Google Scholar] [CrossRef]
- Gonçalves, T.O.d.F.; Daquer, A.K.; Teixeira, L.D.D.; Abrantes, T.C.; Belloti, O.; Maurity, A.; dos Santos, V.L.C.; Ferme, N.S.S.; Agostini, M.; Roza, A.L.O.C.; et al. Soft-tissue keratocyst: Report of 3 new cases from Brazil. Oral Maxillofac. Surg. 2024, 29, 1. [Google Scholar] [CrossRef] [PubMed]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; CARE Group. The CARE Guidelines: Consensus—Based Clinical Case Reporting Guideline Development. Headache J. Head Face Pain 2013, 53, 1541–1547. [Google Scholar] [CrossRef]
- Loro, L.L.; Johannessen, A.C.; Skarstein, K.; Hellem, S. Peripheral odontogenic keratocyst causing bone resorption: Report of two cases. Oral Maxillofac. Surg. Cases 2023, 9, 100301. [Google Scholar] [CrossRef]
- Usui, H.; Sato, T.; Yamamoto, H.; Asada, K.; Nakayama, A.; Ishibashi, K. A case of peripheral keratocystic odontogenic tumor arising in the incisal gingiva of the mandible. Jpn. J. Oral Maxillofac. Surg. 2007, 53, 285–288. [Google Scholar] [CrossRef][Green Version]
- Forte, M.; d’Amati, A.; Manfuso, A.; Vittoli, M.; Girone, G.; Cascardi, E.; Capodiferro, S. Gingival Cyst of the Adult: A Case Description with a Relevant Literature Analysis. Reports 2024, 7, 51. [Google Scholar] [CrossRef]
- Handschel, J.G.; A Depprich, R.; Zimmermann, A.C.; Braunstein, S.; Kübler, N.R. Adenomatoid odontogenic tumor of mandible review of the literature and report of rare case. Head Face Med. 2005, 1, 3. [Google Scholar] [CrossRef] [PubMed]
- Decani, S.; Quatrale, M.; Caria, V.; Moneghini, L.; Varoni, E.M. Peripheral Ameloblastoma: A Case Report and Review of Literature. J. Clin. Med. 2024, 13, 6714. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Malali, V.V.; Satisha, T.; Jha, A.; Rath, S. Gingival cyst of adult: A rare case. J. Ind. Soc. Periodontol. 2012, 16, 465–468. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kerezoudis, N.P.; Donta-Bakoyianni, C.; Siskos, G. The lateral periodontal cyst: Aetiology, clinical significance and diagnosis. Endod. Dent. Traumatol. 2000, 16, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Neville, B.W.; Damm, D.D.; Allen, C.M. Follicular Cysts of The Skin: Oral and Maxillofacial Pathology, 3rd ed.; Saunders: Philadelphia, PA, USA, 2008; pp. 32–34. [Google Scholar]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).