

Diagnostic Utility of Podoplanin Immunohistochemistry Combined with the NanoSuit-Correlative Light and Electron Microscopy Method for Thoracic Malignant Tumors
 , , , ,
, , , ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Collection
2.2. Immunohistochemical Analysis
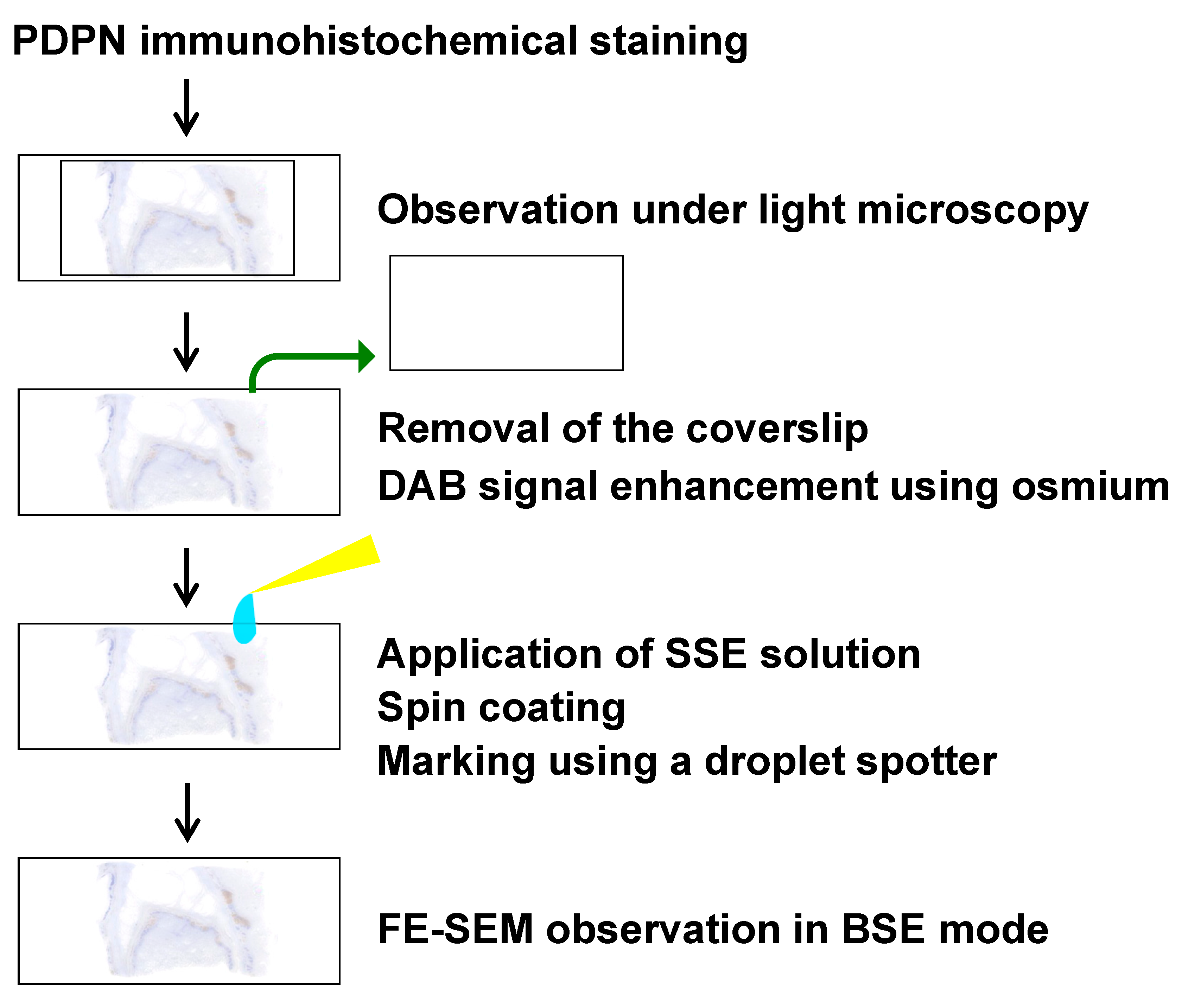
2.3. FE-SEM Analysis of PDPN-Positive Site Using the NanoSuit-CLEM Method
2.4. Statistical Analysis
3. Results
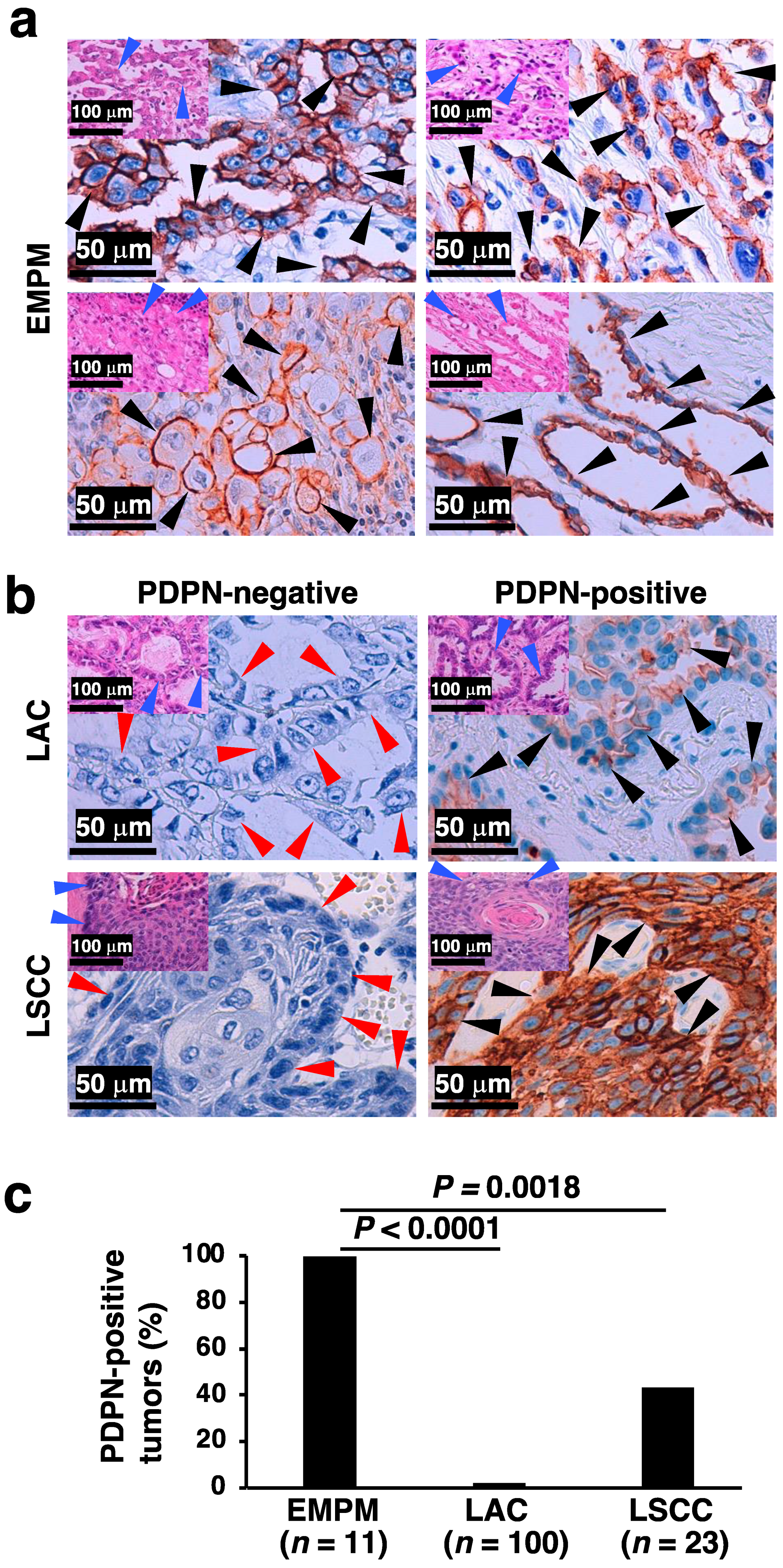
3.1. Differences in PDPN Immunostaining Positivity Among Thoracic Malignant Tumors
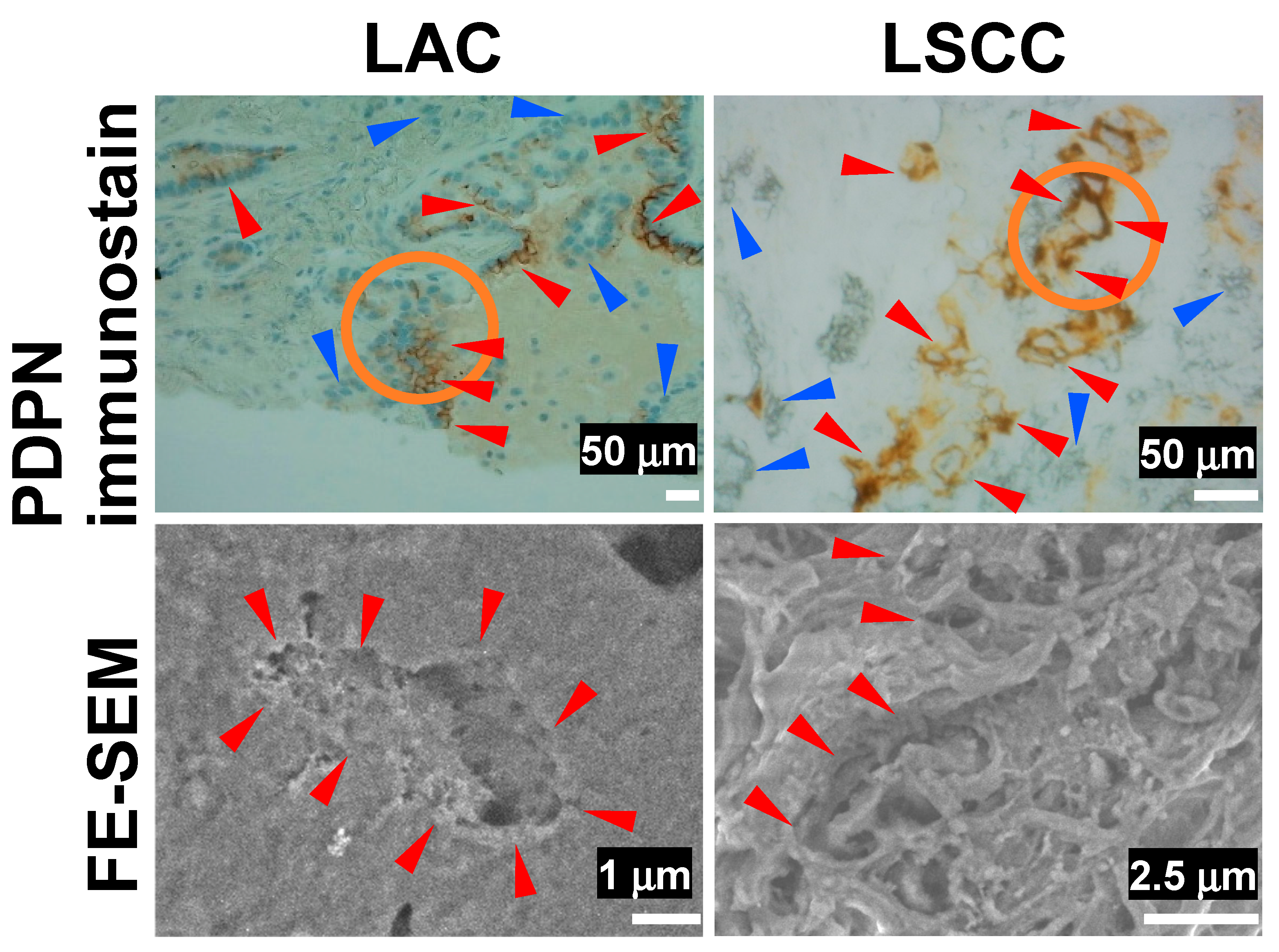
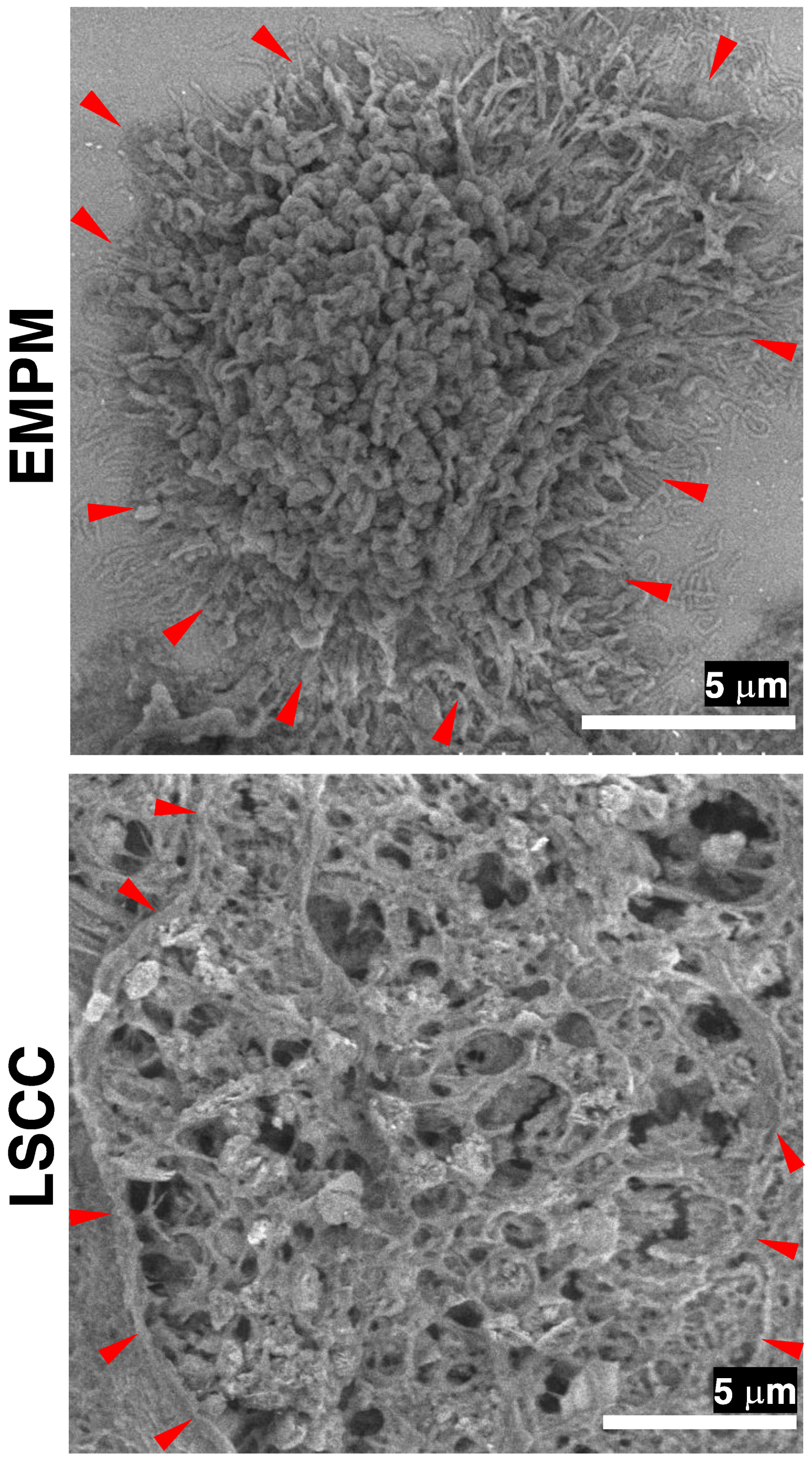
3.2. FE-SEM Observation of PDPN-Positive Sites in Thoracic Malignant Tumors Using the NanoSuit-CLEM Method
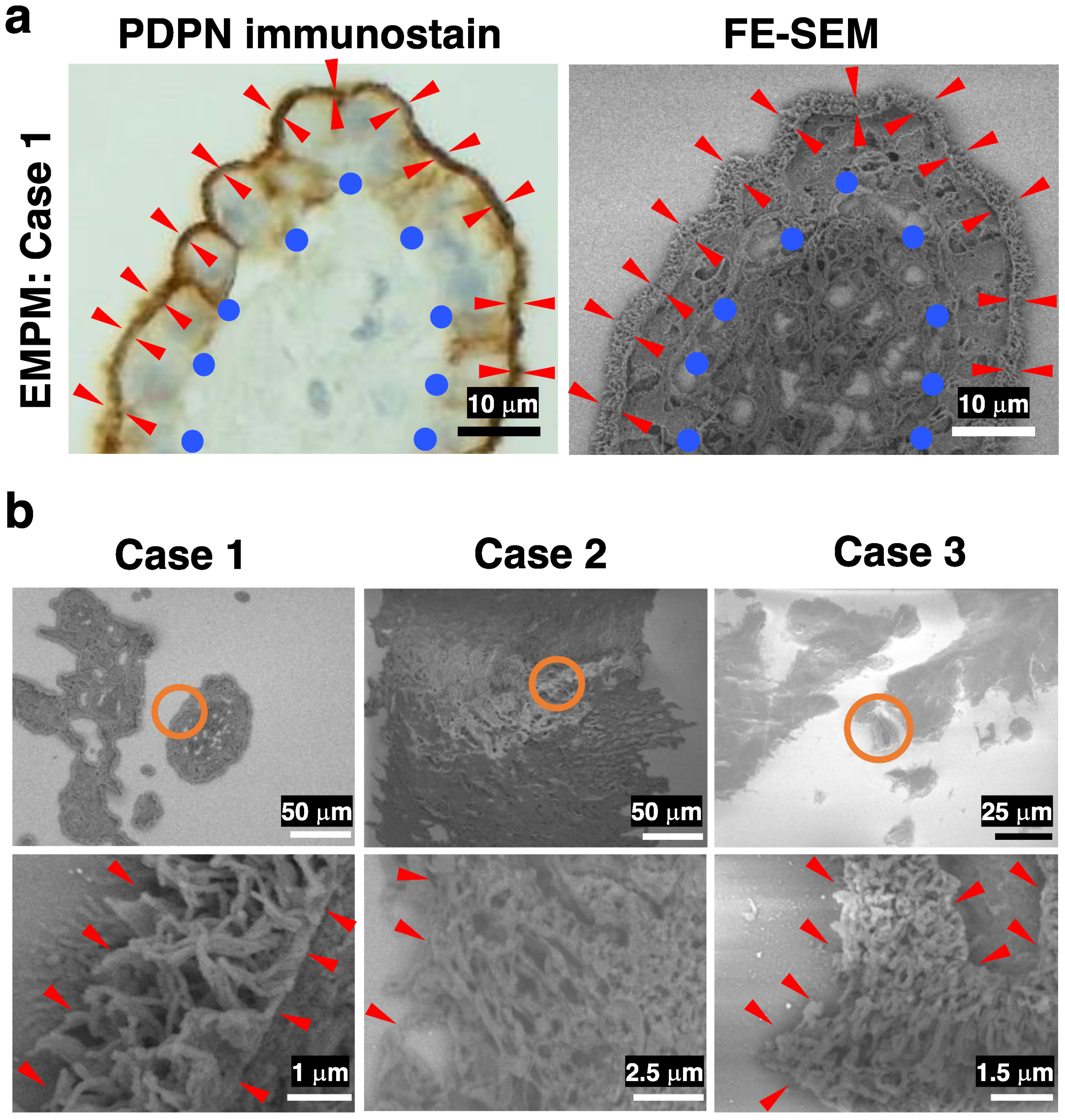
3.3. FE-SEM Using the NanoSuit-CLEM Method for the Detailed Characterization of Surface Structures in Thick-Cut Sections of EMPM
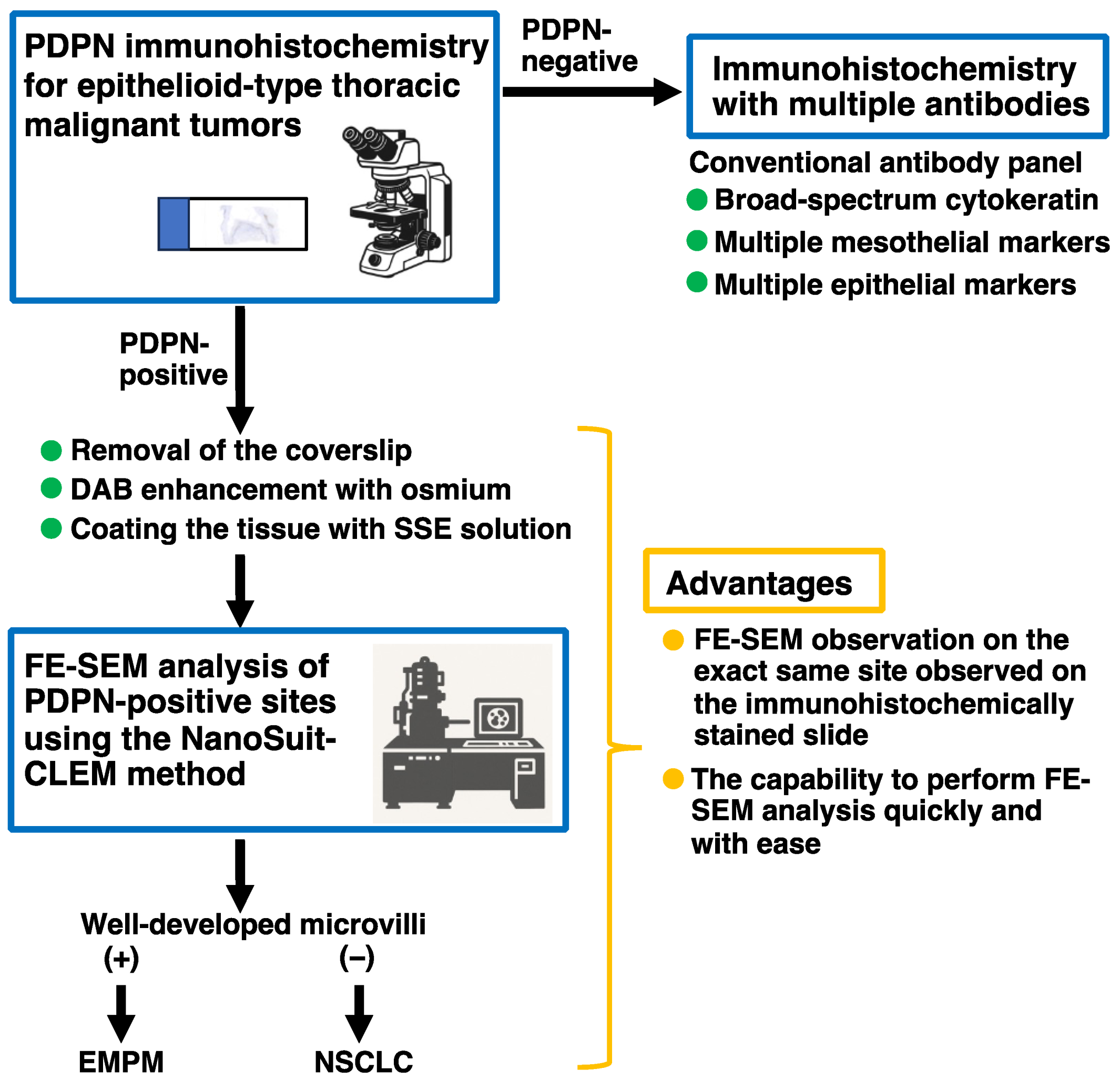
3.4. Proposed Workflow for Differential Diagnosis of Thoracic Malignant Tumors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
Abbreviations
| BSE | Backscattered electron |
| CLEM | Correlative light and electron microscopy |
| DAB | 3,3′-diaminobenzidine tetrahydrochloride |
| EDS | Energy-dispersive X-ray spectroscopy |
| EMPM | Epithelioid malignant pleural mesothelioma |
| FE-SEM | Field emission–scanning electron microscopy |
| FFPE | Formalin-fixed paraffin-embedded |
| H&E | Hematoxylin and eosin |
| H. pylori | Helicobacter pylori |
| LAC | Lung adenocarcinoma |
| LSCC | Lung squamous cell carcinoma |
| PDPN | Podoplanin |
| SSE | Surface shield enhancer |
| YAG | Yttrium aluminum garnet |
References
- Beasley, M.B.; Galateau-Salle, F.; Dacic, S. Pleural Mesothelioma Classification Update. Virchows Arch. 2021, 478, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Dacic, S. Pleural Mesothelioma Classification-Update and Challenges. Mod. Pathol. 2022, 35, 51–56. [Google Scholar] [CrossRef]
- Chapel, D.B.; Schulte, J.J.; Husain, A.N.; Krausz, T. Application of Immunohistochemistry in Diagnosis and Management of Malignant Mesothelioma. Transl. Lung Cancer Res. 2020, 9, S3–S27. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Thai, A.A.; Solomon, B.J.; Sequist, L.V.; Gainor, J.F.; Heist, R.S. Lung Cancer. Lancet 2021, 398, 535–554. [Google Scholar] [CrossRef]
- Alkarn, A.; Stapleton, L.J.; Eleftheriou, D.; Stewart, L.; Chalmers, G.W.; Hamed, A.; Hussein, K.; Blyth, K.G.; van der Horst, J.C.; Maclay, J.D. Real-Life Pre-Operative Nodal Staging Accuracy in Non-Small Cell Lung Cancer and Its Relationship with Survival. Diagnostics 2025, 15, 430. [Google Scholar] [CrossRef]
- Steinestel, K.; Arndt, A. Current Biomarkers in Non-Small Cell Lung Cancer—The Molecular Pathologist’s Perspective. Diagnostics 2025, 15, 631. [Google Scholar] [CrossRef]
- Attanoos, R.L.; Churg, A.; Galateau-Salle, F.; Gibbs, A.R.; Roggli, V.L. Malignant Mesothelioma and Its Non-Asbestos Causes. Arch. Pathol. Lab. Med. 2018, 142, 753–760. [Google Scholar] [CrossRef]
- Husain, A.N.; Chapel, D.B.; Attanoos, R.; Beasley, M.B.; Brcic, L.; Butnor, K.; Chirieac, L.R.; Churg, A.; Dacic, S.; Galateau-Salle, F.; et al. Guidelines for Pathologic Diagnosis of Mesothelioma: 2023 Update of the Consensus Statement from the International Mesothelioma Interest Group. Arch. Pathol. Lab. Med. 2024, 148, 1251–1271. [Google Scholar] [CrossRef]
- Suzuki, H.; Kaneko, M.K.; Kato, Y. Roles of Podoplanin in Malignant Progression of Tumor. Cells 2022, 11, 575. [Google Scholar] [CrossRef]
- Amatya, V.J.; Kushitani, K.; Kai, Y.; Suzuki, R.; Miyata, Y.; Okada, M.; Takeshima, Y. Glypican-1 immunohistochemistry is a novel marker to differentiate epithelioid mesothelioma from lung adenocarcinoma. Mod. Pathol. 2018, 31, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Ordóñez, N.G. The diagnostic utility of immunohistochemistry in distinguishing between epithelioid mesotheliomas and squamous carcinomas of the lung: A comparative study. Mod. Pathol. 2006, 19, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Shimada, Y.; Ishii, G.; Nagai, K.; Atsumi, N.; Fujii, S.; Yamada, A.; Yamane, Y.; Hishida, T.; Nishimura, M.; Yoshida, J.; et al. Expression of podoplanin, CD44, and p63 in squamous cell carcinoma of the lung. Cancer Sci. 2009, 100, 2054–2059. [Google Scholar] [CrossRef] [PubMed]
- Comin, C.E.; Novelli, L.; Cavazza, A.; Rotellini, M.; Cianchi, F.; Messerini, L. Expression of thrombomodulin, calretinin, cytokeratin 5/6, D2-40 and WT-1 in a series of primary carcinomas of the lung: An immunohistochemical study in comparison with epithelioid pleural mesothelioma. Tumori J. 2014, 100, 559–567. [Google Scholar]
- Shah, F.A.; Ruscsák, K.; Palmquist, A. 50 Years of Scanning Electron Microscopy of Bone—A Comprehensive Overview of the Important Discoveries Made and Insights Gained into Bone Material Properties in Health, Disease, and Taphonomy. Bone Res. 2019, 7, 7–15. [Google Scholar]
- Takaku, Y.; Suzuki, H.; Ohta, I.; Ishii, D.; Muranaka, Y.; Shimomura, M.; Hariyama, T. A thin polymer membrane, nano-suit, enhancing survival across the continuum between air and high vacuum. Proc. Natl. Acad. Sci. USA 2013, 110, 7631–7635. [Google Scholar] [CrossRef]
- Hariyama, T.; Takaku, Y.; Kawasaki, H.; Shimomura, M.; Senoh, C.; Yamahama, Y.; Hozumi, A.; Ito, S.; Matsuda, N.; Yamada, S.; et al. Microscopy and Biomimetics: The Nano-Suit® Method and Image Retrieval Platform. Microscopy 2022, 71, 1–12. [Google Scholar] [CrossRef]
- Kawasaki, H.; Itoh, T.; Takaku, Y.; Suzuki, H.; Kosugi, I.; Meguro, S.; Iwashita, T.; Hariyama, T. The NanoSuit method: A novel histological approach for examining paraffin sections in a nondestructive manner by correlative light and electron microscopy. Lab. Investig. 2020, 100, 161–173. [Google Scholar] [CrossRef]
- Shinmura, K.; Kawasaki, H.; Baba, S.; Ohta, I.; Kato, H.; Yasuda, H.; Yamada, S.; Misawa, K.; Sugimoto, K.; Osawa, S.; et al. Utility of Scanning Electron Microscopy Elemental Analysis Using the ‘NanoSuit’ Correlative Light and Electron Microscopy Method in the Diagnosis of Lanthanum Phosphate Deposition in the Esophagogastroduodenal Mucosa. Diagnostics 2019, 10, 1. [Google Scholar] [CrossRef]
- Shinmura, K.; Kusafuka, K.; Kawasaki, H.; Kato, H.; Hariyama, T.; Tsuchiya, K.; Kawanishi, Y.; Funai, K.; Misawa, K.; Mineta, H.; et al. Identification and characterization of primary cilia-positive salivary gland tumours exhibiting basaloid/myoepithelial differentiation. J. Pathol. 2021, 254, 519–530. [Google Scholar] [CrossRef]
- Yamada, S.; Itoh, T.; Ikegami, T.; Imai, A.; Mochizuki, D.; Nakanishi, H.; Ishikawa, R.; Kita, J.; Nakamura, Y.; Takizawa, Y.; et al. Association between human papillomavirus particle production and the severity of recurrent respiratory papillomatosis. Sci. Rep. 2023, 13, 5514. [Google Scholar] [CrossRef]
- Shinmura, K.; Kato, H.; Kawasaki, H.; Hariyama, T.; Yoshimura, K.; Tsuchiya, K.; Watanabe, H.; Ohta, I.; Asahina, E.; Sumiyoshi, F.; et al. Primary Cilia Are Frequently Present in Small Cell Lung Carcinomas but Not in Non-Small Cell Lung Carcinomas or Lung Carcinoids. Lab. Investig. 2023, 103, 100007. [Google Scholar] [CrossRef] [PubMed]
- Suresh, P.K.; Sahu, K.K.; Pai, R.R.; Sridevi, H.B.; Ballal, K.; Khandelia, B.; Minal, J.; Annappa, R. The prognostic significance of neuroendocrine differentiation in colorectal carcinomas: Our experience. J. Clin. Diagn. Res. 2015, 9, EC01–EC04. [Google Scholar] [CrossRef]
- Haraldsson, S.; Klarskov, L.; Nilbert, M.; Bernstein, I.; Bonde, J.; Holck, S. Differential expression of CK20, β-catenin, and MUC2/5AC/6 in Lynch syndrome and familial colorectal cancer type X. BMC Clin. Pathol. 2017, 17, 11. [Google Scholar] [CrossRef]
- Jun, S.Y.; Kim, J.; Yoon, N.; Maeng, L.S.; Byun, J.H. Prognostic potential of Cyclin D1 expression in colorectal cancer. J. Clin. Med. 2023, 12, 572. [Google Scholar] [CrossRef]
- Kalof, A.N.; Cooper, K. D2-40 immunohistochemistry—So far! Adv. Anat. Pathol. 2009, 16, 62–64. [Google Scholar] [CrossRef]
- Sauter, J.L.; Dacic, S.; Galateau-Salle, F.; Attanoos, R.L.; Butnor, K.J.; Churg, A.; Husain, A.N.; Kadota, K.; Khoor, A.; Nicholson, A.G.; et al. The 2021 WHO Classification of Tumors of the Pleura: Advances Since the 2015 Classification. J. Thorac. Oncol. 2022, 17, 608–622. [Google Scholar] [CrossRef]
- Sahin, N.; Akatli, A.N.; Celik, M.R.; Ulutas, H.; Samdanci, E.T.; Colak, C. The Role of CD90 in the Differential Diagnosis of Pleural Malignant Mesothelioma, Pulmonary Carcinoma and Comparison with Calretının. Pathol. Oncol. Res. 2017, 23, 487–491. [Google Scholar] [CrossRef]
- Mawas, A.S.; Amatya, V.J.; Kushitani, K.; Kai, Y.; Miyata, Y.; Okada, M.; Takeshima, Y. MUC4 immunohistochemistry is useful in distinguishing epithelioid mesothelioma from adenocarcinoma and squamous cell carcinoma of the lung. Sci. Rep. 2018, 8, 134. [Google Scholar] [CrossRef]
- Dewar, A.; Valente, M.; Ring, N.P.; Corrin, B. Pleural mesothelioma of epithelial type and pulmonary adenocarcinoma: An ultrastructural and cytochemical comparison. J. Pathol. 1987, 152, 309–316. [Google Scholar] [CrossRef]
- Wick, M.R.; Loy, T.; Mills, S.E.; Legier, J.F.; Manivel, J.C. Malignant epithelioid pleural mesothelioma versus peripheral pulmonary adenocarcinoma: A histochemical, ultrastructural, and immunohistologic study of 103 cases. Hum. Pathol. 1990, 21, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Hammar, S.P. Macroscopic, histologic, histochemical, immunohistochemical, and ultrastructural features of mesothelioma. Ultrastruct. Pathol. 2006, 30, 3–17. [Google Scholar] [CrossRef]
- Carrasco-Ramírez, P.; Greening, D.W.; Andrés, G.; Gopal, S.K.; Martín-Villar, E.; Renart, J.; Simpson, R.J.; Quintanilla, M. Podoplanin is a component of extracellular vesicles that reprograms cell-derived exosomal proteins and modulates lymphatic vessel formation. Oncotarget 2016, 7, 16070–16089. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, K.; Kawasaki, H.; Egami, T.; Kaneko, M.; Ishida, N.; Tamura, S.; Tani, S.; Yamade, M.; Hamaya, Y.; Osawa, S.; et al. Iron Deposition in Gastric Black Spots: Clinicopathological Insights and NanoSuit-Correlative Light and Electron Microscopy Analysis. DEN Open 2024, 5, e398. [Google Scholar] [CrossRef]
- Crawford, J.A.; Sanyal, S.; Burnett, B.R.; Wiesenfeld, S.L.; Abraham, J.L. Accelerated silicosis in sandblasters: Pathology, mineralogy, and clinical correlates. Am. J. Ind. Med. 2024, 67, 179–199. [Google Scholar] [CrossRef]
- Visonà, S.D.; Untalan, M.; Bertoglio, B.; Capella, S.; Belluso, E.; Billò, M.; Ivic-Pavlicic, T.; Taioli, E. Asbestos burden in lungs of subjects deceased from mesothelioma who lived in proximity to an asbestos factory: A topographic post-mortem SEM-EDS study. Am. J. Ind. Med. 2025, 68, 112–121. [Google Scholar] [CrossRef]
- Newbury, D.E.; Ritchie, N.W. Performing Elemental Microanalysis with High Accuracy and High Precision by Scanning Electron Microscopy/Silicon Drift Detector Energy-Dispersive X-ray Spectrometry (SEM/SDD-EDS). J. Mater. Sci. 2015, 50, 493–518. [Google Scholar] [CrossRef]
- Ruaro, B.; Salton, F.; Braga, L.; Wade, B.; Confalonieri, P.; Volpe, M.C.; Baratella, E.; Maiocchi, S.; Confalonieri, M. The History and Mystery of Alveolar Epithelial Type II Cells: Focus on Their Physiologic and Pathologic Role in Lung. Int. J. Mol. Sci. 2021, 22, 2566. [Google Scholar] [CrossRef]
- Pretorius, E. The use of a desktop scanning electron microscope as a diagnostic tool in studying fibrin networks of thrombo-embolic ischemic stroke. Ultrastruct. Pathol. 2011, 35, 245–250. [Google Scholar] [CrossRef]
- Marchand, E.; Bertrand, B.; Hedouin, V.; Demondion, X.; Becart, A. Study of Root Transparency in Different Postmortem Intervals Using Scanning Electron Microscopy. Diagnostics 2023, 13, 2808. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsuragi, S.-y.; Sakano, Y.; Ohta, I.; Kato, H.; Ishikawa, R.; Watanabe, H.; Miyazaki, R.; Yoshimura, K.; Yamada, H.; Sakai, Y.; et al. Diagnostic Utility of Podoplanin Immunohistochemistry Combined with the NanoSuit-Correlative Light and Electron Microscopy Method for Thoracic Malignant Tumors. Diagnostics 2025, 15, 1298. https://doi.org/10.3390/diagnostics15101298
Katsuragi S-y, Sakano Y, Ohta I, Kato H, Ishikawa R, Watanabe H, Miyazaki R, Yoshimura K, Yamada H, Sakai Y, et al. Diagnostic Utility of Podoplanin Immunohistochemistry Combined with the NanoSuit-Correlative Light and Electron Microscopy Method for Thoracic Malignant Tumors. Diagnostics. 2025; 15(10):1298. https://doi.org/10.3390/diagnostics15101298
Chicago/Turabian StyleKatsuragi, Shin-ya, Yuri Sakano, Isao Ohta, Hisami Kato, Rei Ishikawa, Hirofumi Watanabe, Ryosuke Miyazaki, Katsuhiro Yoshimura, Hidetaka Yamada, Yasuhiro Sakai, and et al. 2025. "Diagnostic Utility of Podoplanin Immunohistochemistry Combined with the NanoSuit-Correlative Light and Electron Microscopy Method for Thoracic Malignant Tumors" Diagnostics 15, no. 10: 1298. https://doi.org/10.3390/diagnostics15101298
APA StyleKatsuragi, S.-y., Sakano, Y., Ohta, I., Kato, H., Ishikawa, R., Watanabe, H., Miyazaki, R., Yoshimura, K., Yamada, H., Sakai, Y., Inoue, Y., Takanashi, Y., Sekihara, K., Funai, K., Otsuki, Y., Kawasaki, H., & Shinmura, K. (2025). Diagnostic Utility of Podoplanin Immunohistochemistry Combined with the NanoSuit-Correlative Light and Electron Microscopy Method for Thoracic Malignant Tumors. Diagnostics, 15(10), 1298. https://doi.org/10.3390/diagnostics15101298