
The Train-Line Pattern on Duplex Ultrasound Helps Differentiate Intramural Thrombus from Atheromatous Plaque in Common Carotid Artery Dissection

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
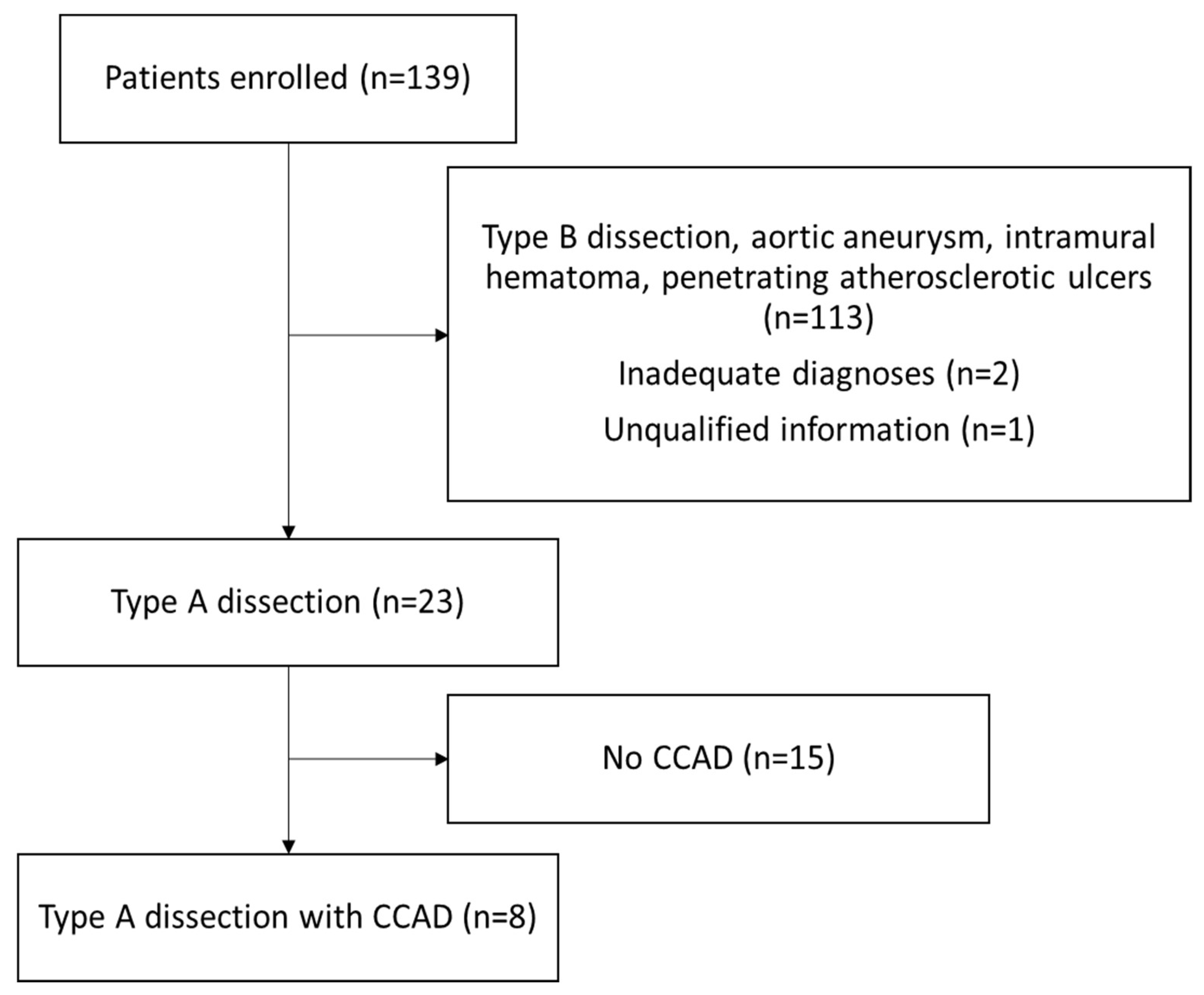
3. Results
3.1. Patient Characteristics
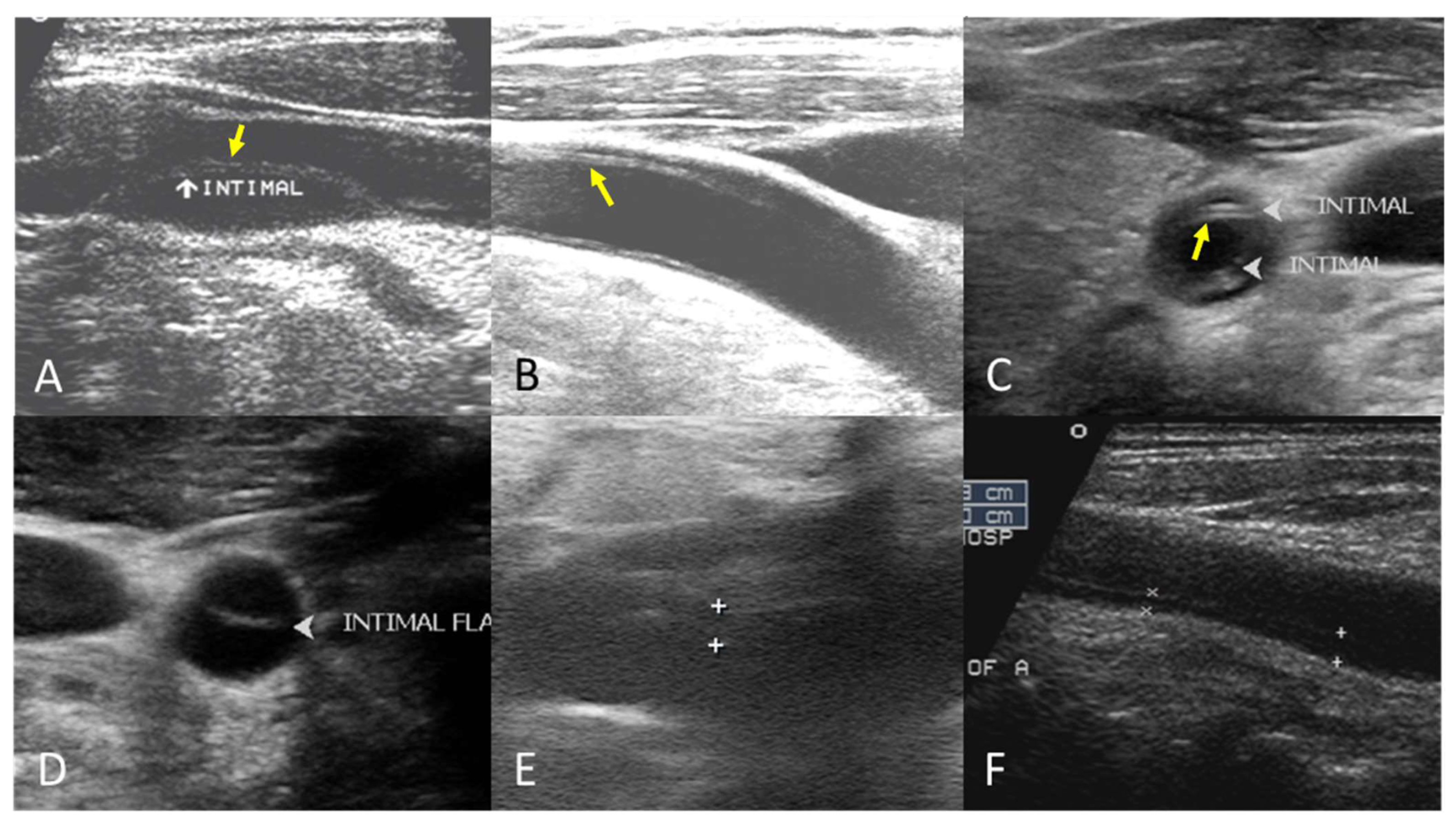
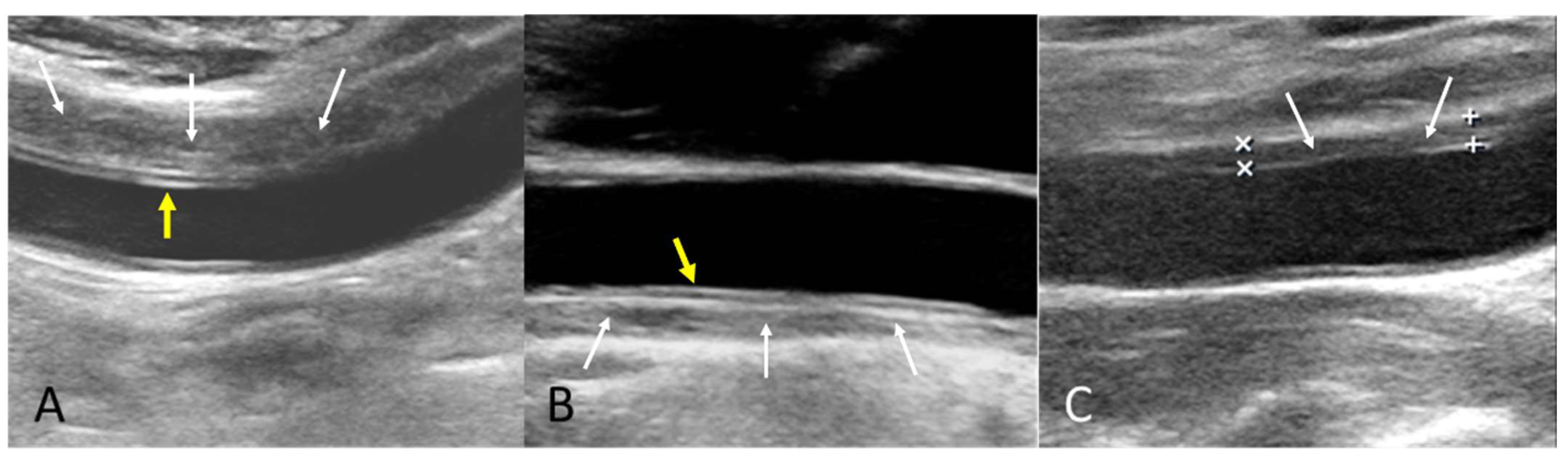
3.2. Ultrasonography Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CCA | common carotid artery |
| CCAD | common carotid artery dissection |
| CT | computed tomography |
| MCA | middle cerebral artery |
| MRI | magnetic resonance imaging |
| mRS | modified Rankin Scale |
| tPA | tissue plasminogen activator |
References
- Gudbjartsson, T.; Ahlsson, A.; Geirsson, A.; Gunn, J.; Hjortdal, V.; Jeppsson, A.; Mennander, A.; Zindovic, I.; Olsson, C. Acute type A aortic dissection—A review. Scand. Cardiovasc. J. 2020, 54, 1–13. [Google Scholar] [CrossRef]
- Sorber, R.; Hicks, C.W. Diagnosis and Management of Acute Aortic Syndromes: Dissection, Penetrating Aortic Ulcer, and Intramural Hematoma. Curr. Cardiol. Rep. 2022, 24, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Chukwu, M.; Ehsan, P.; Aburumman, R.N.; Muthanna, S.I.; Menon, S.R.; Vithani, V.; Sutariya, B.; Montenegro, D.M.; Mohammed, L. Acute Stanford Type A Aortic Dissection: A Review of Risk Factors and Outcomes. Cureus 2023, 15, e36301. [Google Scholar] [CrossRef] [PubMed]
- Flower, L.; EArrowsmith, J.; Bewley, J.; Cook, S.; Cooper, G.; Flower, J.; Greco, R.; Sadeque, S.; Madhivathanan, P.R. Management of acute aortic dissection in critical care. J. Intensiv. Care Soc. 2023, 24, 409–418. [Google Scholar] [CrossRef]
- Hagan, P.G.; Nienaber, C.A.; Isselbacher, E.M.; Bruckman, D.; Karavite, D.J.; Russman, P.L.; Evangelista, A.; Fattori, R.; Suzuki, T.; Oh, J.K.; et al. The International Registry of Acute Aortic Dissection (IRAD): New insights into an old disease. JAMA 2000, 283, 897–903. [Google Scholar] [CrossRef]
- Charlton-Ouw, K.M.; Sandhu, H.K.; Burgess, W.; Vasquez, M.; Estrera, A.L.; Azizzadeh, A.; Coogan, S.M.; Safi, H.J. Duplex Ultrasound Protocol and Findings in Common Carotid Artery Dissection Extending from the Aortic Arch. J. Vasc. Ultrasound 2014, 38, 80–86. [Google Scholar] [CrossRef]
- Zach, V.; Zhovtis, S.; Kirchoff-Torres, K.F.; Weinberger, J.M. Common Carotid Artery Dissection: A Case Report and Review of the Literature. J. Stroke Cerebrovasc. Dis. 2012, 21, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Raksamani, K.; Tangvipattanapong, M.; Charoenpithakwong, N.; Silarat, S.; Pantisawat, N.; Sanphasitvong, V.; Raykateeraroj, N. Postoperative stroke in acute type A aortic dissection: Incidence, outcomes, and perioperative risk factors. BMC Surg. 2024, 24, 1–10. [Google Scholar] [CrossRef]
- Mészáros, I.; Mórocz, J.; Szlávi, J.; Schmidt, J.; Tornóci, L.; Nagy, L.; Szép, L. Epidemiology and Clinicopathology of Aortic Dissection. Chest 2000, 117, 1271–1278. [Google Scholar] [CrossRef]
- Rodallec, M.H.; Marteau, V.; Gerber, S.; Desmottes, L.; Zins, M. Craniocervical Arterial Dissection: Spectrum of Imaging Findings and Differential Diagnosis. RadioGraphics 2008, 28, 1711–1728. [Google Scholar] [CrossRef]
- Gardner, D.J.; Gosink, B.B.; Kallman, C.E. Internal carotid artery dissections: Duplex ultrasound imaging. J. Ultrasound Med. 1991, 10, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Treiman, G.S.; Treiman, R.L.; Foran, R.F.; Levin, P.M.; Cohen, J.; Wagner, W.H.; Cossman, D.V. Spontaneous dissection of the internal carotid artery: A nineteen-year clinical experience. J. Vasc. Surg. 1996, 24, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, A.; Muthukumarassamy, R.; Karthikeyan, V.S.; Rajaraman, G.; Mishra, S. Pseudoaneurysm of internal carotid artery after carotid body tumor excision. Indian. J. Radiol. Imaging 2013, 23, 208–211. [Google Scholar] [CrossRef]
- Jia, S.; Wang, M.; Liu, Y.; Gong, M.; Jiang, W.; Zhang, H. Effect of Asymptomatic Common Carotid Artery Dissection on the Prognosis of Patients With Acute Type A Aortic Dissection. J. Am. Heart Assoc. 2024, 13, e031542. [Google Scholar] [CrossRef]
- Koga, M.; Iguchi, Y.; Ohara, T.; Tahara, Y.; Fukuda, T.; Noguchi, T.; Matsuda, H.; Minatoya, K.; Nagatsuka, K.; Toyoda, K. Acute ischemic stroke as a complication of Stanford type A acute aortic dissection: A review and proposed clinical recommendations for urgent diagnosis. Gen. Thorac. Cardiovasc. Surg. 2018, 66, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Kreibich, M.; Rylski, B.; Czerny, M.; Beyersdorf, F.; Itagaki, R.; Okamura, H.; Kimura, N.; Yamaguchi, A.; Vallabhajosyula, P.; Szeto, W.Y.; et al. Impact of Carotid Artery Involvement in Type A Aortic Dissection. Circulation 2019, 139, 1977–1978. [Google Scholar] [CrossRef]
- Kreibich, M.; Desai, N.D.; Bavaria, J.E.; Szeto, W.Y.; Vallabhajosyula, P.; Beyersdorf, F.; Czerny, M.; Siepe, M.; Rylski, B.; Itagaki, R.; et al. Common carotid artery true lumen flow impairment in patients with type A aortic dissection. Eur. J. Cardio-Thorac. Surg. 2020, 59, 490–496. [Google Scholar] [CrossRef]
- Inoue, T.; Omura, A.; Chomei, S.; Nakai, H.; Yamanaka, K.; Inoue, T.; Okada, K. Early and late outcomes of type A acute aortic dissection with common carotid artery involvement. JTCVS Open. 2022, 10, 1–11. [Google Scholar] [CrossRef]
- Carrillo-Alfonso, N.; Mugeiro, M.; Amado, I.; Ruivo, E.; Lares, A. Ischemic Stroke as a Form of Presentation of Aortic Dissection: A Case Report. Cureus 2024, 16, e52866. [Google Scholar] [CrossRef]
- Zaschke, L.; Habazettl, H.; Thurau, J.; Matschilles, C.; Göhlich, A.; Montagner, M.; Falk, V.; Kurz, S.D. Acute type A aortic dissection: Aortic Dissection Detection Risk Score in emergency care—Surgical delay because of initial misdiagnosis. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, S40–S47. [Google Scholar] [CrossRef]
- Ke, C.; Wu, H.; Xi, M.; Shi, W.; Huang, Q.; Lu, G. Clinical features and risk factors of postoperative in-hospital mortality following surgical repair of Stanford type A acute aortic dissection. BMC Cardiovasc. Disord. 2021, 21, 1–7. [Google Scholar] [CrossRef] [PubMed]
- He, Z.-Y.; Yao, L.-P.; Wang, X.-K.; Chen, N.-Y.; Zhao, J.-J.; Zhou, Q.; Yang, X.-F. Acute ischemic Stroke combined with Stanford type A aortic dissection: A case report and literature review. World J. Clin. Cases 2022, 10, 8009–8017. [Google Scholar] [CrossRef]
- Spittell, P.C.; Spittell, J.A.; Joyce, J.W.; Tajik, A.J.; Edwards, W.D.; Schaff, H.V.; Stanson, A.W. Clinical Features and Differential Diagnosis of Aortic Dissection: Experience With 236 Cases (1980 Through 1990). Mayo Clin. Proc. 1993, 68, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Gaul, C.; Dietrich, W.; Friedrich, I.; Sirch, J.; Erbguth, F.J. Neurological Symptoms in Type A Aortic Dissections. Stroke 2007, 38, 292–297. [Google Scholar] [CrossRef]
- Gaul, C.; Dietrich, W.; Erbguth, F.J. Neurological Symptoms in Aortic Dissection: A Challenge for Neurologists. Cerebrovasc. Dis. 2008, 26, 1–8. [Google Scholar] [CrossRef]
- Derex, L.; Nighoghossian, N.; Turjman, F.; Hermier, M.; Honnorat, J.; Neuschwander, P.; Froment, J.; Trouillas, P. Intravenous tPA in acute ischemic stroke related to internal carotid artery dissection. Neurology 2000, 54, 2159–2161. [Google Scholar] [CrossRef]
- Shu, L.; Akpokiere, F.; Mandel, D.M.; Field, T.S.; Leon Guerrero, C.R.; Henninger, N.; Muppa, J.; Affan, M.; Haq Lodhi, O.U.; Heldner, M.R.; et al. Intravenous Thrombolysis in Patients With Cervical Artery Dissection: A Secondary Analysis of the STOP-CAD Study. Neurology 2024, 103, e209843. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Lee, E.; Field, T.S.; Guo, X.; Henninger, N.; Keser, Z.; Khan, M.; Mistry, E.A.; Nguyen, T.N.; Siegler, J.E.; et al. Intravenous Thrombolysis in Cervical Artery Dissection–Related Stroke: A Nationwide Study. J. Am. Heart Assoc. 2025, 14, e039662. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar]
- Alter, S.M.; Eskin, B.; Allegra, J.R. Diagnosis of Aortic Dissection in Emergency Department Patients is Rare. West J. Emerg. Med. 2015, 16, 629–631. [Google Scholar] [CrossRef]
- Shea, K.; Stahmer, S. Carotid and vertebral arterial dissections in the emergency department. Emerg. Med. Pract. 2012, 14, 1–23, quiz 23–24. [Google Scholar] [PubMed]
- Iguchi, Y.; Kimura, K.; Sakai, K.; Matsumoto, N.; Aoki, J.; Yamashita, S.; Shibazaki, K. Hyper-acute Stroke Patients Associated with Aortic Dissection. Intern. Med. 2010, 49, 543–547. [Google Scholar] [CrossRef]
- Takekawa, H.; Tsukui, D.; Kobayasi, S.; Suzuki, K.; Hamaguchi, H. Point-of-care ultrasound for stroke patients in the emergency room. J. Med. Ultrason. 2022, 49, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Ohara, T.; Koga, M.; Tokuda, N.; Tanaka, E.; Yokoyama, H.; Minatoya, K.; Nagatsuka, K.; Toyoda, K.; Minematsu, K. Rapid Identification of Type A Aortic Dissection as a Cause of Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2016, 25, 1901–1906. [Google Scholar] [CrossRef]
- Uchino, K.; Estrera, A.; Calleja, S.; Alexandrov, A.V.; Garami, Z. Aortic dissection presenting as an acute ischemic stroke for thrombolysis. J. Neuroimaging. 2005, 15, 281–283. [Google Scholar] [CrossRef]
- Tsivgoulis, G.; Vadikolias, K.; Heliopoulos, I.; Patousi, A.; Iordanidis, A.; Souftas, V.; Piperidou, C.; Hibi, K.; Kimura, K.; Nakatogawa, T.; et al. Aortic Arch Dissection Causing Acute Cerebral Ischemia: An Uncommon Contraindication for Intravenous Thrombolysis. Circulation 2011, 124, 657–658. [Google Scholar] [CrossRef]
- Morelli, N.; Rota, E.; Mancuso, M.; Immovilli, P.; Spallazzi, M.; Rocca, G.; Michieletti, E.; Guidetti, D. Carotid Ultrasound Imaging in a Patient with Acute Ischemic Stroke and Aortic Dissection: A Lesson for the Management of Ischemic Stroke? Int. J. Stroke 2013, 8, E53–E54. [Google Scholar] [CrossRef] [PubMed]
- Hama, Y.; Koga, M.; Tokunaga, K.; Takizawa, H.; Miyashita, K.; Iba, Y.; Toyoda, K. Carotid Ultrasonography Can Identify Stroke Patients Ineligible for Intravenous Thrombolysis Therapy due to Acute Aortic Dissection. J. Neuroimaging 2014, 25, 671–673. [Google Scholar] [CrossRef]
- Vassileva, E.; Klissurski, M.G.; Vavrek, E.V.; Daskalov, M.P. Cerebrovascular Ultrasound as a First Method of Detecting Aortic Dissection in Acute Stroke Patients. Int. J. Stroke 2014, 10, E8. [Google Scholar] [CrossRef]
- Sukockienė, E.; Laučkaitė, K.; Jankauskas, A.; Mickevičienė, D.; Jurkevičienė, G.; Vaitkus, A.; Stankevičius, E.; Petrikonis, K.; Rastenytė, D. Crucial role of carotid ultrasound for the rapid diagnosis of hyperacute aortic dissection complicated by cerebral infarction: A case report and literature review. Medicina 2016, 52, 378–388. [Google Scholar] [CrossRef]
- Chua, C.-H.; Lien, L.-M.; Lin, C.-H.; Hung, C.-R. Emergency surgical intervention in a patient with delayed diagnosis of aortic dissection presenting with acute ischemic stroke and undergoing thrombolytic therapy. J. Thorac. Cardiovasc. Surg. 2005, 130, 1222–1224. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, J.; Ruland, S. Cervicocerebral artery dissection. Curr. Opin. Cardiol. 2015, 30, 603–610. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| No. | Gender | Age | B Mode Findings | Train-Line | Doppler Waveform | Ischemic Stroke | Outcome |
|---|---|---|---|---|---|---|---|
| 1 | Female | 59 | Double lumen in right CCA | Present | Biphasic flow in false lumen, wide systolic wave in true lumen | Right subcortical | Survival |
| 2 | Male | 42 | Double lumen in left CCA | Present | Biphasic waves in false and true lumen | Right MCA territory, left basal ganglia, left parietal lobe | Survival |
| 3 | Male | 47 | Double lumen in both right and left CCA | Right: present Left: absent | Right: no data Left: biphasic wave in false lumen, resistive wave in true lumen | Absent | Death |
| 4 | Female | 84 | Double lumen in right CCA | Absent | No data | Bilateral cerebral hemispheres and left cerebellum | Death |
| 5 | Male | 56 | Double lumen in right CCA | Absent | Dampened and nearly occluded wave in false lumen, normal in true lumen | Bilateral watershed | Survival |
| 6 | Female | 75 | Intramural thrombus in right CCA | Present | Normal waveforms in true lumen | Right MCA territory | Death |
| 7 | Male | 52 | Intramural thrombus in right CCA | Present | No data | Right MCA territory | Survival |
| 8 | Male | 40 | Intramural thrombus in right CCA | Absent | Biphasic in true lumen | Absent | Survival |
| Feature | Intramural Thrombus | Atherosclerotic Plaque |
|---|---|---|
| Shape | Crescentic or concentric mural thickening | Focal, eccentric |
| Echotexture | Homogeneous or mildly heterogeneous, hypoechoic | Heterogeneous, with echogenic foci (fibrous tissue or calcification) |
| Surface | Smooth, layered appearance | Irregular, possibly ulcerated |
| Wall location | Located within media or between intima and media | Confined to media |
| Mobility | Generally immobile | May present with instability (especially in soft plaques) |
| Acoustic shadowing | Rare | Common with calcified components |
| Intimal flap/double lumen | May be present, suggesting dissection | Absent |
| Train-line pattern | Present in part of our cases | Absent in our cases |
| Present Study | Charlton-Ouw et al., 2014 [6] | |
|---|---|---|
| Number of patients with type A aortic dissection who received carotid duplex sonography | 23 | 87 |
| Median age | 54 years (range: 40–84) | 59 years (range: 21–99) |
| Gender | 13 male (57%), 10 female (43%) | 62 male (71%), 25 female (29%) |
| CCAD | 8 patients (35%), 9 CCAD | 20 patients (23%), 26 CCAD |
| Side of CCAD | 7 right (78%), 2 left (22%) | 17 right (65%), 9 left (35%) |
| Double lumen | 6 (67%) | 17 (65%) |
| Thrombosed false lumen | 3 (33%) | 9 (35%) |
| Stroke | 6 (75%) | 5 (25%) |
| In-hospital mortality | 5 out of 23 (21%) | 8 out of 87 (9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, M.-H.; Huang, Y.-Y.; Hsieh, F.-I.; Lin, K.-Y.; Yeh, H.-L.; Yeh, K.-J.; Lien, L.-M. The Train-Line Pattern on Duplex Ultrasound Helps Differentiate Intramural Thrombus from Atheromatous Plaque in Common Carotid Artery Dissection. Diagnostics 2025, 15, 1297. https://doi.org/10.3390/diagnostics15101297
Chang M-H, Huang Y-Y, Hsieh F-I, Lin K-Y, Yeh H-L, Yeh K-J, Lien L-M. The Train-Line Pattern on Duplex Ultrasound Helps Differentiate Intramural Thrombus from Atheromatous Plaque in Common Carotid Artery Dissection. Diagnostics. 2025; 15(10):1297. https://doi.org/10.3390/diagnostics15101297
Chicago/Turabian StyleChang, Ming-Hsing, Yen-Yu Huang, Fang-I Hsieh, Kuan-Yu Lin, Hsu-Ling Yeh, Kai-Jing Yeh, and Li-Ming Lien. 2025. "The Train-Line Pattern on Duplex Ultrasound Helps Differentiate Intramural Thrombus from Atheromatous Plaque in Common Carotid Artery Dissection" Diagnostics 15, no. 10: 1297. https://doi.org/10.3390/diagnostics15101297
APA StyleChang, M.-H., Huang, Y.-Y., Hsieh, F.-I., Lin, K.-Y., Yeh, H.-L., Yeh, K.-J., & Lien, L.-M. (2025). The Train-Line Pattern on Duplex Ultrasound Helps Differentiate Intramural Thrombus from Atheromatous Plaque in Common Carotid Artery Dissection. Diagnostics, 15(10), 1297. https://doi.org/10.3390/diagnostics15101297