
Diagnostic Accuracy of MRI in Detecting the Perineural Spread of Head and Neck Tumors: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Selection
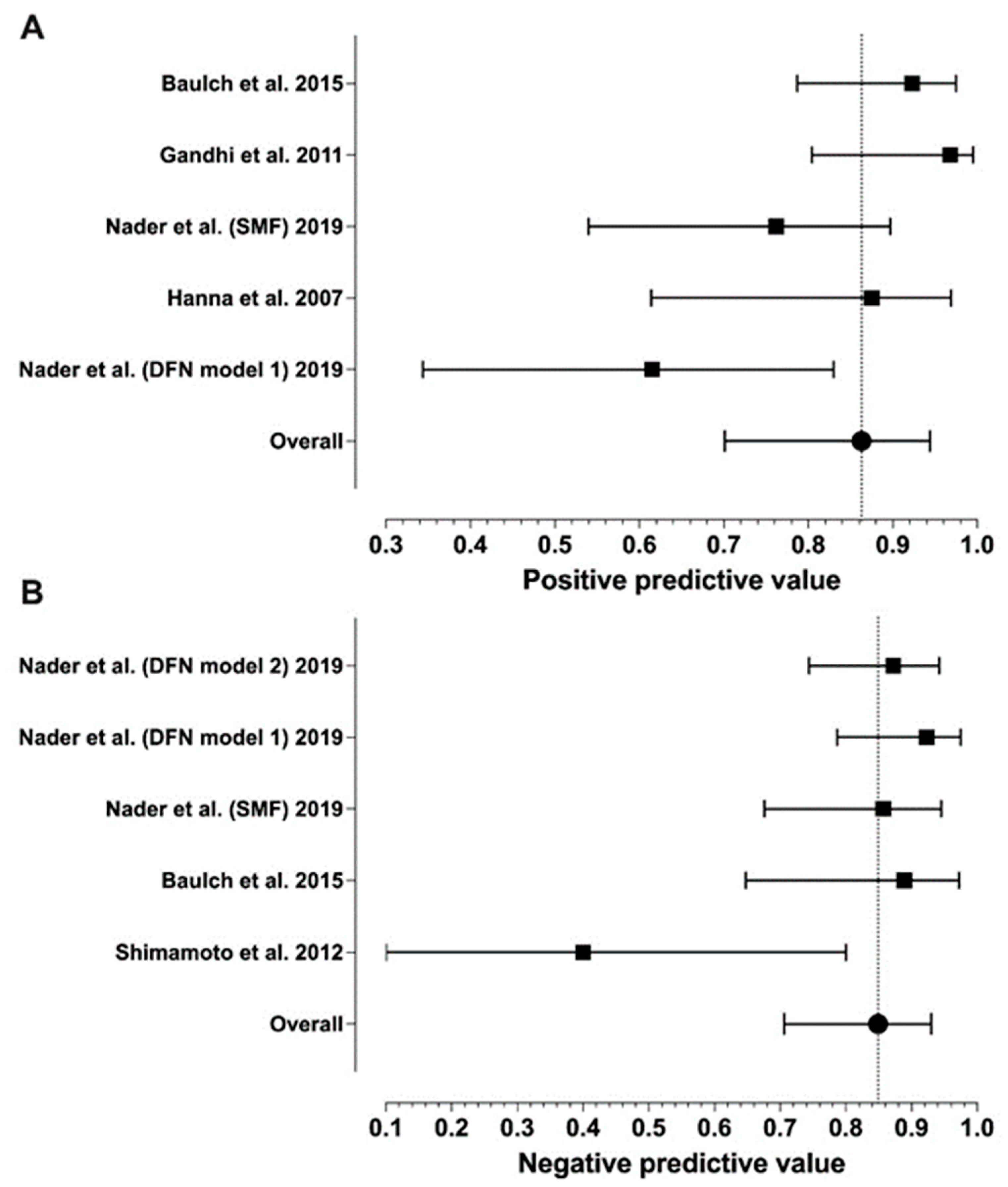
3.2. Diagnostic Performance
3.3. Quality Assessment
3.4. Primary Tumor Histology and Location
3.5. Nerves Affected by PNS
3.6. MRI Technique and Protocols
3.7. MRI Features of PNS
4. Discussion
4.1. Diagnostic Performance
4.2. Quality Assessment
4.3. Primary Tumor Histology and Location
4.4. Nerves Affected by PNS
4.5. MRI Technique and Protocols
4.6. MRI Features of PNS
4.7. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Badger, D.; Aygun, N. Imaging of Perineural Spread in Head and Neck Cancer. Radiol. Clin. N. Am. 2017, 55, 139–149. [Google Scholar] [CrossRef]
- Moonis, G.; Cunnane, M.B.; Emerick, K.; Curtin, H. Patterns of Perineural Tumor Spread in Head and Neck Cancer. Magn. Reson. Imaging Clin. N. Am. 2012, 20, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, T.T.; Abdel Razek, A.A.K. Magnetic Resonance Imaging of Perineural Spread of Head and Neck Cancer. Magn. Reson. Imaging Clin. N. Am. 2022, 30, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Mendenhall, W.M.; Amdur, R.J.; Williams, L.S.; Mancuso, A.A.; Stringer, S.P.; Mendenhall, N.P. Carcinoma of the Skin of the Head and Neck with Perineural Invasion. Head Neck 2002, 24, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.; Parmar, H.; Gandhi, D.; Mukherji, S.K. Imaging Nuances of Perineural Spread of Head and Neck Malignancies. J. Neuro-Ophthalmol. 2007, 27, 129–137. [Google Scholar] [CrossRef]
- Bakst, R.L.; Glastonbury, C.M.; Parvathaneni, U.; Katabi, N.; Hu, K.S.; Yom, S.S. Perineural Invasion and Perineural Tumor Spread in Head and Neck Cancer. Int. J. Radiat. Oncol. 2019, 103, 1109–1124. [Google Scholar] [CrossRef] [PubMed]
- Maroldi, R.; Farina, D.; Borghesi, A.; Marconi, A.; Gatti, E. Perineural Tumor Spread. Neuroimaging Clin. N. Am. 2008, 18, 413–429. [Google Scholar] [CrossRef]
- Chang, P.C.; Fischbein, N.J.; McCalmont, T.H.; Kashani-Sabet, M.; Zettersten, E.M.; Liu, A.Y.; Weissman, J.L. Perineural Spread of Malignant Melanoma of the Head and Neck: Clinical and Imaging Features. AJNR Am. J. Neuroradiol. 2004, 25, 5–11. [Google Scholar] [CrossRef][Green Version]
- Hsieh, K.-C.J.; Addae-Mensah, K.; Alrohaibani, Y.; Goad, A.; Learned, K. Perineural Spread of Tumor in the Skull Base and Head and Neck. Oral Maxillofac. Surg. Clin. N. Am. 2023, 35, 399–412. [Google Scholar] [CrossRef]
- Murthy, N.K.; Amrami, K.K.; Spinner, R.J. Perineural Spread to the Brachial Plexus: A Focused Review of Proposed Mechanisms and Described Pathologies. Acta Neurochir. 2020, 162, 3179–3187. [Google Scholar] [CrossRef]
- Kirsch, C.F.E.; Schmalfuss, I.M. Practical Tips for MR Imaging of Perineural Tumor Spread. Magn. Reson. Imaging Clin. N. Am. 2018, 26, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.D.; Harnsberger, H.R. Clinical-Radiologic Issues in Perineural Tumor Spread of Malignant Diseases of the Extracranial Head and Neck. Radiographics 1991, 11, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Schachtel, M.J.; Panizza, B.J.; Gandhi, M. Evaluation of Facial Nerve Perineural Spread from Cutaneous Squamous Cell Carcinoma Using 3T MR Neurography. J. Med. Imaging Radiat. Oncol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Blandino, A.; Gaeta, M.; Minutoli, F.; Pandolfo, I. CT and MR Findings in Neoplastic Perineural Spread along the Vidian Nerve. Eur. Radiol. 2000, 10, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Chong, V.F.; Fan, Y.F.; Khoo, J.B. Nasopharyngeal Carcinoma with Intracranial Spread: CT and MR Characteristics. J. Comput. Assist. Tomogr. 1996, 20, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Hanna, E.; Vural, E.; Prokopakis, E.; Carrau, R.; Snyderman, C.; Weissman, J. The Sensitivity and Specificity of High-Resolution Imaging in Evaluating Perineural Spread of Adenoid Cystic Carcinoma to the Skull Base. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Nie, X.; Zhou, J.; Zeng, J.; Sun, J.; Chen, W.; Niu, J. Does PET Scan Have Any Role in the Diagnosis of Perineural Spread Associated with the Head and Neck Tumors? Adv. Clin. Exp. Med. 2022, 31, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lazor, J.W.; Assadsangabi, R.; Shah, J. An Imager’s Guide to Perineural Tumor Spread in Head and Neck Cancers: Radiologic Footprints on 18F-FDG PET, with CT and MRI Correlates. J. Nucl. Med. 2019, 60, 304–311. [Google Scholar] [CrossRef]
- Nader, M.-E.; Ginsberg, L.E.; Bell, D.; Roberts, D.B.; Gidley, P.W. Evaluating Perineural Spread to the Intratemporal Facial Nerve on Magnetic Resonance Imaging. Otolaryngol.—Head Neck Surg. 2019, 160, 1087–1094. [Google Scholar] [CrossRef]
- Gandhi, M.R.; Panizza, B.; Kennedy, D. Detecting and Defining the Anatomic Extent of Large Nerve Perineural Spread of Malignancy: Comparing “Targeted” MRI with the Histologic Findings Following Surgery. Head Neck 2011, 33, 469–475. [Google Scholar] [CrossRef]
- Baulch, J.; Gandhi, M.; Sommerville, J.; Panizza, B. 3T MRI Evaluation of Large Nerve Perineural Spread of Head and Neck Cancers. J. Med. Imaging Radiat. Oncol. 2015, 59, 578–585. [Google Scholar] [CrossRef]
- Nemzek, W.R.; Hecht, S.; Gandour-Edwards, R.; Donald, P.; McKennan, K. Perineural Spread of Head and Neck Tumors: How Accurate Is MR Imaging? AJNR Am. J. Neuroradiol. 1998, 19, 701–706. [Google Scholar]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; QUADAS-2 Steering Group. A Systematic Review Classifies Sources of Bias and Variation in Diagnostic Test Accuracy Studies. J. Clin. Epidemiol. 2013, 66, 1093–1104. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Normand, S.L. Meta-Analysis: Formulating, Evaluating, Combining, and Reporting. Stat. Med. 1999, 18, 321–359. [Google Scholar] [CrossRef]
- Warren, T.A.; Panizza, B.; Porceddu, S.V.; Gandhi, M.; Patel, P.; Wood, M.; Nagle, C.M.; Redmond, M. Outcomes after Surgery and Postoperative Radiotherapy for Perineural Spread of Head and Neck Cutaneous Squamous Cell Carcinoma. Head Neck 2016, 38, 824–831. [Google Scholar] [CrossRef]
- Majoie, C.B.; Hulsmans, F.J.; Verbeeten, B.; Castelyns, J.A.; Oldenburger, F.; Schouwenburg, P.F.; Andries Bosch, D. Perineural Tumor Extension along the Trigeminal Nerve: Magnetic Resonance Imaging Findings. Eur. J. Radiol. 1997, 24, 191–205. [Google Scholar] [CrossRef]
- Shimamoto, H.; Chindasombatjaroen, J.; Kakimoto, N.; Kishino, M.; Murakami, S.; Furukawa, S. Perineural Spread of Adenoid Cystic Carcinoma in the Oral and Maxillofacial Regions: Evaluation with Contrast-Enhanced CT and MRI. Dentomaxillofac. Radiol. 2012, 41, 143–151. [Google Scholar] [CrossRef]
- Tomura, N.; Hirano, H.; Kato, K.; Takahashi, S.; Sashi, R.; Tate, E.; Watanabe, O.; Okane, K.; Watarai, J. Comparison of MR Imaging with CT in Depiction of Tumour Extension into the Pterygopalatine Fossa. Clin. Radiol. 1999, 54, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Schmalfuss, I.M.; Tart, R.P.; Mukherji, S.; Mancuso, A.A. Perineural Tumor Spread along the Auriculotemporal Nerve. AJNR Am. J. Neuroradiol. 2002, 23, 303–311. [Google Scholar] [PubMed]
- Lee, K.J.; Abemayor, E.; Sayre, J.; Bhuta, S.; Kirsch, C. Determination of Perineural Invasion Preoperatively on Radiographic Images. Otolaryngol.—Head Neck Surg. 2008, 139, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.S.; Mancuso, A.A.; Mendenhall, W.M. Perineural Spread of Cutaneous Squamous and Basal Cell Carcinoma: CT and MR Detection and Its Impact on Patient Management and Prognosis. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 1061–1069. [Google Scholar] [CrossRef]
- Panizza, B.; Warren, T. Perineural Invasion of Head and Neck Skin Cancer: Diagnostic and Therapeutic Implications. Curr. Oncol. Rep. 2013, 15, 128–133. [Google Scholar] [CrossRef]
- Gandhi, M.; Sommerville, J. The Imaging of Large Nerve Perineural Spread. J. Neurol. Surg. B Skull Base 2016, 77, 113–123. [Google Scholar] [CrossRef]
- Hutcheson, J.A.; Vural, E.; Korourian, S.; Hanna, E. Neural Cell Adhesion Molecule Expression in Adenoid Cystic Carcinoma of the Head and Neck. Laryngoscope 2000, 110, 946–948. [Google Scholar] [CrossRef]
- Panizza, B.J. An Overview of Head and Neck Malignancy with Perineural Spread. J. Neurol. Surg. B Skull Base 2016, 77, 81–85. [Google Scholar] [CrossRef]
- Caldemeyer, K.S.; Mathews, V.P.; Righi, P.D.; Smith, R.R. Imaging Features and Clinical Significance of Perineural Spread or Extension of Head and Neck Tumors. Radiographics 1998, 18, 97–110, quiz 147. [Google Scholar] [CrossRef]
- Barakos, J.A.; Dillon, W.P.; Chew, W.M. Orbit, Skull Base, and Pharynx: Contrast-Enhanced Fat Suppression MR Imaging. Radiology 1991, 179, 191–198. [Google Scholar] [CrossRef]
- Patronas, N.; Bulakbasi, N.; Stratakis, C.A.; Lafferty, A.; Oldfield, E.H.; Doppman, J.; Nieman, L.K. Spoiled Gradient Recalled Acquisition in the Steady State Technique Is Superior to Conventional Postcontrast Spin Echo Technique for Magnetic Resonance Imaging Detection of Adrenocorticotropin-Secreting Pituitary Tumors. J. Clin. Endocrinol. Metab. 2003, 88, 1565–1569. [Google Scholar] [CrossRef] [PubMed]
- Laine, F.J.; Braun, I.F.; Jensen, M.E.; Nadel, L.; Som, P.M. Perineural Tumor Extension through the Foramen Ovale: Evaluation with MR Imaging. Radiology 1990, 174, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Russo, C.P.; Smoker, W.R.; Weissman, J.L. MR Appearance of Trigeminal and Hypoglossal Motor Denervation. AJNR Am. J. Neuroradiol. 1997, 18, 1375–1383. [Google Scholar] [PubMed]
- Jacquesson, T.; Cotton, F.; Attyé, A.; Zaouche, S.; Tringali, S.; Bosc, J.; Robinson, P.; Jouanneau, E.; Frindel, C. Probabilistic Tractography to Predict the Position of Cranial Nerves Displaced by Skull Base Tumors: Value for Surgical Strategy Through a Case Series of 62 Patients. Neurosurgery 2019, 85, E125–E136. [Google Scholar] [CrossRef] [PubMed]
- Medvedev, O.; Hedesiu, M.; Ciurea, A.; Lenghel, M.; Rotar, H.; Dinu, C.; Roman, R.; Termure, D.; Csutak, C. Perineural Spread in Head and Neck Malignancies: Imaging Findings—An Updated Literature Review. Bosn. J. Basic Med. Sci. 2022, 22, 22–38. [Google Scholar] [CrossRef]
- Chong, V.F.; Fan, Y.F. Pterygopalatine Fossa and Maxillary Nerve Infiltration in Nasopharyngeal Carcinoma. Head Neck 1997, 19, 121–125. [Google Scholar] [CrossRef]
- Curtin, H.D. Detection of Perineural Spread: Fat Suppression versus No Fat Suppression. AJNR Am. J. Neuroradiol. 2004, 25, 1–3. [Google Scholar]
- Matzko, J.; Becker, D.G.; Phillips, C.D. Obliteration of Fat Planes by Perineural Spread of Squamous Cell Carcinoma along the Inferior Alveolar Nerve. AJNR Am. J. Neuroradiol. 1994, 15, 1843–1845. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | N of Patients | Mean Age | N of CNs | TP | TN | FP | FN | Se | Sp | PPV | NPV |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hanna et al. [16] | 2007 | 26 | - | 27 | 14 | 11 | 2 | 0 | 1.00 | 0.85 | 0.88 | 1.00 |
| Nader et al. [19] (DFN model 1) | 2019 | 52 | 58 | 52 | 8 | 36 | 5 | 3 | 0.73 | 0.88 | 0.62 | 0.92 |
| Nader et al. [19] (DFN model 2) | 2019 | 52 | 58 | 52 | 5 | 41 | 0 | 6 | 0.46 | 1.00 | 1.00 | 0.87 |
| Nader et al. [19] (SMF) | 2019 | 49 | 58 | 49 | 16 | 24 | 5 | 4 | 0.8 | 0.83 | 0.76 | 0.86 |
| Baulch et al. [21] | 2015 | 33 | 62 | 57 | 36 | 16 | 3 | 2 | 0.95 | 0.84 | 0.92 | 0.75 |
| Gandhi et al. [20] | 2011 | 25 | 59 | 48 | 30 | 17 | 1 | 0 | 1.00 | 0.94 | 0.97 | 1.00 |
| Warren et al. [28] | 2016 | 48 | 60 | 48 | 46 | 0 | 0 | 2 | 0.96 | - | 1.00 | - |
| Chang et al. [8] | 2004 | 8 | 58 | 8 | 8 | 0 | 0 | 0 | 1.00 | - | 1.00 | - |
| Nemzek et al. [22] | 1998 | 19 | 55 | 45 | 18 | 0 | 0 | 1 | 0.95 | - | 1.00 | - |
| Schmalfuss et al. [32] | 2002 | 7 | 62 | 7 | 7 | 0 | 0 | 0 | 1.00 | - | 1.00 | - |
| Majoie et al. [29] | 1997 | 2 | 57 | 2 | 2 | 0 | 0 | 0 | 1.00 | - | 1.00 | - |
| Shimamoto et al. [30] | 2012 | 13 | 58 | 13 | 8 | 2 | 0 | 3 | 0.73 | 1.00 | 1.00 | 0.4 |
| Tomura et al. [31] | 1999 | 12 | - | 12 | 12 | 0 | 0 | 0 | 1.00 | - | 1.00 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdullaeva, U.; Pape, B.; Hirvonen, J. Diagnostic Accuracy of MRI in Detecting the Perineural Spread of Head and Neck Tumors: A Systematic Review and Meta-Analysis. Diagnostics 2024, 14, 113. https://doi.org/10.3390/diagnostics14010113
Abdullaeva U, Pape B, Hirvonen J. Diagnostic Accuracy of MRI in Detecting the Perineural Spread of Head and Neck Tumors: A Systematic Review and Meta-Analysis. Diagnostics. 2024; 14(1):113. https://doi.org/10.3390/diagnostics14010113
Chicago/Turabian StyleAbdullaeva, Umida, Bernd Pape, and Jussi Hirvonen. 2024. "Diagnostic Accuracy of MRI in Detecting the Perineural Spread of Head and Neck Tumors: A Systematic Review and Meta-Analysis" Diagnostics 14, no. 1: 113. https://doi.org/10.3390/diagnostics14010113
APA StyleAbdullaeva, U., Pape, B., & Hirvonen, J. (2024). Diagnostic Accuracy of MRI in Detecting the Perineural Spread of Head and Neck Tumors: A Systematic Review and Meta-Analysis. Diagnostics, 14(1), 113. https://doi.org/10.3390/diagnostics14010113