
Performing the ABC Method Twice for Gastric Cancer Risk Stratification: A Retrospective Study Based on Data from a Large-Scale Screening Facility

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statements
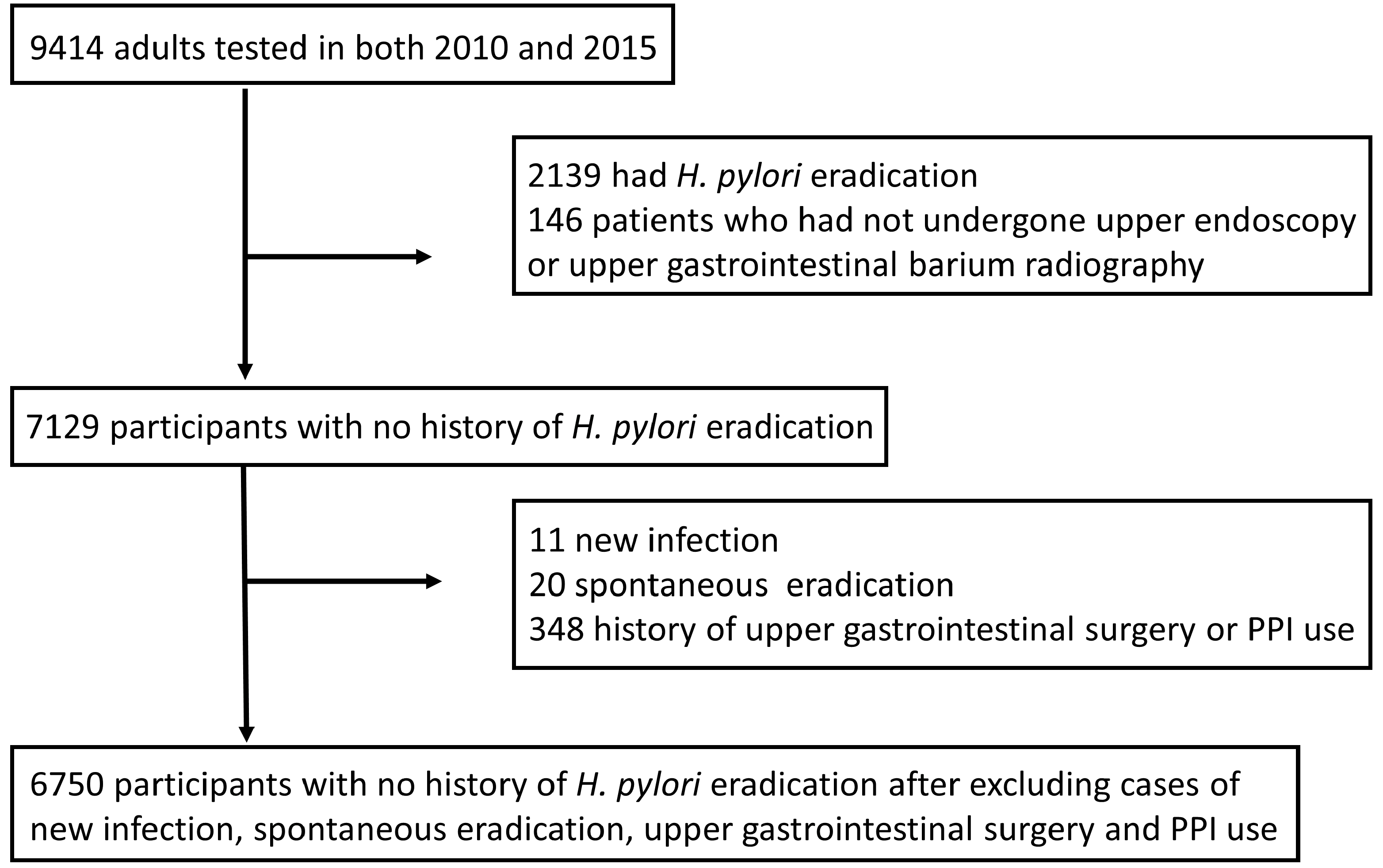
2.2. Study Design and Participants
2.3. Measurement of Anti-H. pylori Antibody Titer
2.4. The ABC Method
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malaty, H.M.; El-Kasabany, A.; Graham, D.Y.; Miller, C.C.; Reddy, S.G.; Srinivasan, S.R.; Yamaoka, Y.; Berenson, G.S. Age at acquisition of Helicobacter pylori infection: A follow-up study from infancy to adulthood. Lancet 2002, 359, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Triantafillidis, J.K.; Gikas, A.; Hyphantis, T.; Cheracakis, P.; Androulakis, G. Helicobacter pylori infection in hospital workers over a 5-year period: Correlation with demographic and clinical parameters. J. Gastroenterol. 2002, 37, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Rolle-Kampczyk, U.E.; Fritz, G.J.; Diez, U.; Lehmann, I.; Richter, M.; Herbarth, O. Well water--one source of Helicobacter pylori colonization. Int. J. Hyg. Environ. Health 2004, 207, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, E.J.; Uyterlinde, A.M.; Peña, A.S.; Roosendaal, R.; Pals, G.; Nelis, G.F.; Festen, H.P.; Meuwissen, S.G. Long-term sequelae of Helicobacter pylori gastritis. Lancet 1995, 345, 1525–1528. [Google Scholar] [CrossRef]
- Wotherspoon, A.C.; Ortiz-Hidalgo, C.; Falzon, M.R.; Isaacson, P.G. Helicobacter pylori-associated gastritis, and primary B-cell gastric lymphoma. Lancet 1991, 338, 1175–1176. [Google Scholar] [CrossRef]
- Yang, J.C.; Lu, C.W.; Lin, C.J. Treatment of Helicobacter pylori infection: Current status and future concepts. World J. Gastroenterol. 2014, 20, 5283–5293. [Google Scholar] [CrossRef]
- Miftahussurur, M.; Waskito, L.A.; Fauzia, K.A.; Mahmudah, I.; Doohan, D.; Adnyana, I.K.; Khomsan, A.; Ratnasari, N.; Rezkitha, Y.A.A. Overview of Helicobacter pylori infection in Indonesia: What distinguishes it from countries with high gastric cancer incidence? Gut Liver 2021, 15, 653–665. [Google Scholar] [CrossRef]
- Inaba, S.; Hirayama, H.; Nagata, C.; Kurisu, Y.; Takatsuka, N.; Kawakami, N.; Shimizu, H. Evaluation of a screening program on reduction of gastric cancer mortality in Japan: Preliminary results from a cohort study. Prev. Med. 1999, 29, 102–106. [Google Scholar] [CrossRef]
- Miki, K.; Morita, M.; Sasajima, M.; Hoshina, R.; Kanda, E.; Urita, Y. Usefulness of gastric cancer screening using the serum pepsinogen test method. Am. J. Gastroenterol. 2003, 98, 735–739. [Google Scholar] [CrossRef]
- Zagari, R.M.; Rabitti, S.; Greenwood, D.C.; Eusebi, L.H.; Vestito, A.; Bazzoli, F. Systematic review with meta-analysis: Diagnostic performance of the combination of pepsinogen, gastrin-17, and anti-Helicobacter pylori antibody serum assays for the diagnosis of atrophic gastritis. Aliment. Pharmacol Ther. 2017, 46, 657–667. [Google Scholar] [CrossRef]
- Miki, K. Gastric cancer screening by combined assay for serum anti-Helicobacter pylori IgG antibody and serum pepsinogen levels—“ABC method”. Proc. Jpn. Acad. Ser. B Phys. Biol. Sci. 2011, 87, 405–414. [Google Scholar] [CrossRef]
- Ikeda, F.; Shikata, K.; Hata, J.; Yonemoto, K.; Hirakawa, Y.; Ohara, T.; Mukai, N.; Nagata, M.; Yoshida, D.; Yonemoto, K.; et al. Combination of Helicobacter pylori antibody and serum pepsinogen as a good predictive tool of gastric cancer incidence: 20-year prospective data from the Hisayama study. J. Epidemiol. 2016, 26, 629–636. [Google Scholar] [CrossRef]
- Watabe, H.; Mitsushima, T.; Yamaji, Y.; Okamoto, M.; Wada, R.; Kokubo, T.; Doi, H.; Yoshida, H.; Kawabe, T.; Omata, M. Predicting the development of gastric cancer from combining Helicobacter pylori antibodies and serum pepsinogen status: A prospective endoscopic cohort study. Gut 2005, 54, 764–768. [Google Scholar] [CrossRef]
- Zhang, X.; Xue, L.; Xing, L.; Wang, J.; Cui, J.; Mi, J.; Xing, X.; Wang, J.; Du, Z.; Misumi, J.; et al. Low serum pepsinogen I and pepsinogen I/II ratios and Helicobacter pylori infection are associated with an increased risk of gastric cancer: A 14-year follow-up result in a rural Chinese community. Int. J. Cancer 2012, 130, 1614–1619. [Google Scholar] [CrossRef]
- Takahashi, Y.; Yamamichi, N.; Kubota, D.; Shimamoto, T.; Nagao, S.; Sakuma, N.; Sakaguchi, Y.; Yakabi, S.; Tsuji, Y.; Wada, R.; et al. Risk factors for gastric cancer in Japan in the 2010s: A large, long-term observational study. Gastric Cancer 2022, 25, 481–489. [Google Scholar] [CrossRef]
- Hu, Y.; Wan, J.H.; Li, X.Y.; Zhu, Y.; Graham, D.Y.; Lu, N.H. Systematic review with meta-analysis: The global recurrence rate of Helicobacter pylori. Aliment. Pharmacol. Ther. 2017, 46, 773–779. [Google Scholar] [CrossRef]
- Fukuda, K.; Kodama, M.; Mizukami, K.; Okamoto, K.; Ogawa, R.; Hirashita, Y.; Fukuda, M.; Togo, K.; Matsunari, O.; Okimoto, T.; et al. Analysis of long-term serological and histological changes after H. pylori eradication. J. Clin. Biochem. Nutr. 2022, 71, 151–157. [Google Scholar] [CrossRef]
- Toyoshima, O.; Nishizawa, T.; Arita, M.; Kataoka, Y.; Sakitani, K.; Yoshida, S.; Yamashita, H.; Hata, K.; Watanabe, H.; Suzuki, H. Helicobacter pylori Infection in subjects negative for high-titer serum antibody. World J. Gastroenterol. 2018, 24, 1419–1428. [Google Scholar] [CrossRef]
- Kishikawa, H.; Kimura, K.; Takarabe, S.; Kaida, S.; Nishida, J. Helicobacter pylori antibody titer and gastric cancer screening. Dis. Markers 2015, 2015, 156719. [Google Scholar] [CrossRef]
- Otani, K.; Watanabe, T.; Kosaka, S.; Matsumoto, Y.; Nakata, A.; Nadatani, Y.; Fukunaga, S.; Hosomi, S.; Tanaka, F.; Kamata, N.; et al. Utility of Kyoto Classification of Gastritis in subjects with a high-negative titer of anti-Helicobacter pylori antibody during a medical check-up. J. Clin. Biochem. Nutr. 2020, 67, 317–322. [Google Scholar] [CrossRef]
- Fawcett, J.P.; Barbezat, G.O.; Poulton, R.; Milne, B.J.; Xia, H.H.; Talley, N.J. Helicobacter pylori serology in a birth cohort of New Zealanders from age 11 to 26. World J. Gastroenterol. 2005, 11, 3273–3276. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, S.; Ohgihara, A.; Hasegawa, A.; Miki, K.; Kaneko, E.; Mizukoshi, H. Seroconversion and seroreversion of Helicobacter pylori antibodies over a 9-year period and related factors in Japanese adults. Helicobacter 2004, 9, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Choi, K.D.; Han, S.; Jung, H.Y.; Do, M.Y.; Chang, H.S.; Choe, J.W.; Lee, G.H.; Song, H.J.; Kim, D.H.; et al. Seroconversion rates of Helicobacter pylori infection in Korean adults. Helicobacter 2013, 18, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Yamamichi, N.; Yamaji, Y.; Shimamoto, T.; Takahashi, Y.; Majima, K.; Wada, R.; Mitsushima, T.; Koike, K. Inverse time trends of peptic ulcer and reflux esophagitis show significant association with reduced prevalence of Helicobacter pylori infection. Ann. Med. 2020, 52, 506–514. [Google Scholar] [CrossRef]
- Okuda, M.; Osaki, T.; Lin, Y.; Yonezawa, H.; Maekawa, K.; Kamiya, S.; Fukuda, Y.; Kikuchi, S. Low prevalence and incidence of Helicobacter pylori infection in children: A population-based study in Japan. Helicobacter 2015, 20, 133–138. [Google Scholar] [CrossRef]
- Tang, Y.; Tang, G.; Pan, L.; Zhu, H.; Zhou, S.; Wei, Z. Clinical factors associated with initial Helicobacter pylori eradication therapy: A retrospective study in China. Sci Rep. 2020, 10, 15403. [Google Scholar] [CrossRef]
- Yu, H.; Liu, Y.; Jiang, S.; Zhou, Y.; Guan, Z.; Dong, S.; Chu, F.F.; Kang, C.; Gao, Q. Serum pepsinogen II levels are doubled with Helicobacter pylori infection in an asymptomatic population of 40,383 Chinese subjects. Medicine 2021, 100, e26562. [Google Scholar] [CrossRef]
- Daugule, I.; Ruskule, A.; Moisejevs, G.; Rudzite, D.; Jonaitis, L.; Janciauskas, D.; Kiudelis, G.; Kupcinskas, L.; Leja, M. Long-term dynamics of gastric biomarkers after eradication of Helicobacter pylori infection. Eur. J. Gastroenterol. Hepatol. 2015, 27, 501–505. [Google Scholar] [CrossRef]
- Sasaki, Y.; Abe, Y.; Shoji, M.; Mizumoto, N.; Takeda, H.; Oizumi, H.; Yaoita, T.; Sawada, N.; Yamagishi, K.; Saito, E.; et al. Reliability of self-reported questionnaire for epidemiological investigation of Helicobacter pylori eradication in a population-based cohort study. Sci. Rep. 2021, 11, 15605. [Google Scholar] [CrossRef]


{kind=link}
| p-Value | ||||
|---|---|---|---|---|
| Year | 2010 | 2015 | ||
| Number | 7129 | 7129 | ||
| Age | 48.4 (±8.3) | 53.4 (±8.3) | ||
| Male | 4145 (58.1%) | 4145 (58.1%) | ||
| BMI | 23.1 (±3.4) | 23.1 (±3.5) | 0.23 | |
| Anti-H. pylori antibody titer, n (%) | <3 U/mL | 5641 (79.1%) | 5705 (80.0%) | |
| 3–9.9 U/mL | 338 (4.7%) | 331 (4.6%) | ||
| >10 U/mL | 1150 (16.1%) | 1093 (15.3%) | 0.38 | |
| PG I | 50.9 (±26.7) | 60 (±36.8) | <0.01 | |
| PG II | 9.9 (±7.1) | 11.8 (±8.3) | <0.01 | |
| PG I/PG II | 5.9 (±1.9) | 5.7 (±1.8) | <0.01 | |
| ABC screening | Group A | 5613 | 5659 | |
| Group B | 1059 | 1022 | ||
| Group C | 429 | 402 | ||
| Group D | 28 | 46 | 0.11 | |
| Use of PPIs | Yes | 97 | 217 | |
| No | 7032 | 6912 | <0.01 | |
| Upper gastrointestinal | Yes | 59 | 54 | |
| tract surgery | No | 7070 | 7075 | 0.71 |
| Smoking | Current | 1470 | 1252 | |
| Former | 1888 | 2132 | ||
| Never | 3771 | 3745 | <0.01 | |
| Use of anticoagulants | Yes | 153 | 242 | |
| No | 6976 | 6887 | <0.01 | |
| Use of steroids | Yes | 57 | 46 | |
| No | 7072 | 7083 | 0.28 | |
| Use of NSAIDs | Yes | 449 | 579 | |
| No | 6680 | 6550 | <0.01 | |
| Anti-H. pylori Antibody Titers Recorded in 2010 | |||||
|---|---|---|---|---|---|
| <3 U/mL | 3–9.9 U/mL | ≥10 U/mL | |||
| Anti-H. pylori antibody titers recorded in 2015 | <3 U/mL | 5577 | 108 | 20 | 5705 |
| 78.20% | 1.50% | 0.30% | 80.00% | ||
| 3–9.9 U/mL | 53 | 205 | 73 | 331 | |
| 0.70% | 2.90% | 1.00% | 4.60% | ||
| ≥10 U/mL | 11 | 25 | 1057 | 1093 | |
| 0.20% | 0.40% | 14.80% | 15.30% | ||
| 5641 | 338 | 1150 | 7129 | ||
| 79.10% | 4.70% | 16.10% | 100.00% | ||
| New H. pylori Infection | Non-Adjusted Odds Ratio (95% CI) | p-Value | Multivariate Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Male vs. Female | 3.0 (0.63–14.4) | 0.17 | 2.1 (0.36–13.1) | 0.37 |
| Age * | 1.03 (0.96–1.1)) | 0.41 | 1.01 (0.94–1.09) | 0.66 |
| BMI * | 1.08 (0.94–1.25) | 0.28 | 1.1 (0.83–1.20) | 0.97 |
| Upper intestinal tract surgery (yes vs. no) | NA | 0.99 | NA | |
| History of smoking (yes vs. no) | 2.9 (0.89–9.7) | 0.78 | 2.1 (0.46–10.0) | 0.3 |
| Use of PPIs (yes vs. no) | 5.5 (0.60–51) | 0.13 | 4.8 (1.02–6.2) | 0.23 |
| Use of anticoagulants (yes vs. no) | NA | NA | ||
| Use of steroids (yes vs. no) | NA | NA | ||
| Use of NSAIDs (yes vs. no) | 1.5 (0.19–12) | 0.70 | 2.4 (0.28–20.3) | 0.46 |
| Spontaneous eradication of H. pylori | Non-adjusted odds ratio (95% CI) | p-Value | Multivariate odds ratio (95% CI) | p-Value |
| Male vs. Female | 2.4 (0.9–6.5) | 0.09 | 1.7 (0.52–5.6) | 0.36 |
| Age * | 1.13 (1.08–1.18) | <0.01 | 1.1 (1.05–1.16) | <0.01 |
| BMI * | 1.06 (0.95–1.19) | 0.3 | 1.04 (0.90–1.19) | 0.55 |
| Upper intestinal tract surgery (yes vs. no) | 2.2 (0.26–19) | 0.47 | 1.8 (0.19–16.5) | 0.62 |
| History of smoking (yes vs. no) | 1.2 (0.36–4.3) | 0.73 | 1.1 (0.40–3.2) | 0.78 |
| Use of PPIs (yes vs. no) | NA | NA | ||
| Use of anticoagulants (yes vs. no) | 9.7 (3.2–30) | <0.01 | 3.2 (0.95–11.2) | 0.08 |
| Use of steroids (yes vs. no) | 5.6 (0.7–45) | 0.1 | 6.0 (0.72–50.9) | 0.17 |
| Use of NSAIDs (yes vs. no) | 1.8 (0.4–8.3) | 0.44 | 2.0 (0.44–9.4) | 0.39 |
| Cancer Incidence Rate | p-Value | |||||
|---|---|---|---|---|---|---|
| 2010 | 2015 | Fisher’s Exact Test | Bootstrapping Test | Difference between 2010 and 2015 (95% CI) | ||
| Group A | 9/5613 | 11/5659 | 0.82 | 0.33 | −0.03% | (−0.13% to 0.13%) |
| 0.16% | 0.19% | |||||
| Group B | 5/1059 | 4/1022 | 1.00 | 0.36 | 0.08% | (−0.50% to 6.5%) |
| 0.47% | 0.39% | |||||
| Group C + D | 9/457 | 8/448 | 1.00 | 0.41 | 0.18% | (−1.4% to 2.0%) |
| 1.97% | 1.79% | |||||
| 2010 | ABC twice | Fisher’s exact test | Bootstrapping test | Difference between 2010 and ABC twice (95% CI) | ||
| Group A | 9/5613 | 9/5543 | 1.00 | 0.50 | 0.00% | (−0.16% to 0.16%) |
| 0.16% | 0.16% | |||||
| Group B | 5/1059 | 4/1036 | 1.00 | 0.36 | 0.09% | (−0.48% to 0.66%) |
| 0.47% | 0.39% | |||||
| Group C + D | 9/457 | 10/550 | 1.00 | 0.45 | 0.15% | (−1.6% to 1.9%) |
| 1.97% | 1.82% | |||||
| Cancer Rate | p-Value | |||||
|---|---|---|---|---|---|---|
| 2010 | 2015 | Fisher’s Exact Test | Bootstrapping Test | Difference between 2010 and 2015 (95% CI) | ||
| Group A | 7/5356 | 8/5391 | 0.80 | 0.35 | −0.02% | (−0.18% to 0.11%) |
| 0.13% | 0.15% | |||||
| Group B | 4/990 | 2/956 | 0.69 | 0.19 | 0.19% | (−0.31% to 0.71%) |
| 0.40% | 0.21% | |||||
| Group C + D | 7/404 | 8/403 | 0.80 | 0.40 | −0.25% | (−2.3% to 1.7%) |
| 1.73% | 1.99% | |||||
| 2010 | ABC twice | Fisher’s exact test | Bootstrapping test | Difference between 2010 and ABC twice (95% CI) | ||
| Group A | 7/5356 | 7/5302 | 1.00 | 0.43 | −0.01% | (−0.14% to 0.11%) |
| 0.13% | 0.13% | |||||
| Group B | 4/990 | 3/957 | 1.00 | 0.38 | 0.09% | (−0.42% to 0.60%) |
| 0.40% | 0.31% | |||||
| Group C + D | 7/404 | 8/491 | 1.00 | 0.47 | 0.10% | (−1.5% to 1.8%) |
| 1.73% | 1.63% | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mizutani, S.; Takahashi, Y.; Shimamoto, T.; Nakagawa, H.; Hisada, H.; Oshio, K.; Kubota, D.; Mizutani, H.; Ohki, D.; Sakaguchi, Y.; et al. Performing the ABC Method Twice for Gastric Cancer Risk Stratification: A Retrospective Study Based on Data from a Large-Scale Screening Facility. Diagnostics 2023, 13, 1284. https://doi.org/10.3390/diagnostics13071284
Mizutani S, Takahashi Y, Shimamoto T, Nakagawa H, Hisada H, Oshio K, Kubota D, Mizutani H, Ohki D, Sakaguchi Y, et al. Performing the ABC Method Twice for Gastric Cancer Risk Stratification: A Retrospective Study Based on Data from a Large-Scale Screening Facility. Diagnostics. 2023; 13(7):1284. https://doi.org/10.3390/diagnostics13071284
Chicago/Turabian StyleMizutani, Satoru, Yu Takahashi, Takeshi Shimamoto, Hideki Nakagawa, Hiroyuki Hisada, Kaori Oshio, Dai Kubota, Hiroya Mizutani, Daisuke Ohki, Yoshiki Sakaguchi, and et al. 2023. "Performing the ABC Method Twice for Gastric Cancer Risk Stratification: A Retrospective Study Based on Data from a Large-Scale Screening Facility" Diagnostics 13, no. 7: 1284. https://doi.org/10.3390/diagnostics13071284
APA StyleMizutani, S., Takahashi, Y., Shimamoto, T., Nakagawa, H., Hisada, H., Oshio, K., Kubota, D., Mizutani, H., Ohki, D., Sakaguchi, Y., Yakabi, S., Niimi, K., Kakushima, N., Tsuji, Y., Wada, R., Yamamichi, N., & Fujishiro, M. (2023). Performing the ABC Method Twice for Gastric Cancer Risk Stratification: A Retrospective Study Based on Data from a Large-Scale Screening Facility. Diagnostics, 13(7), 1284. https://doi.org/10.3390/diagnostics13071284