
The Presence of Ascending Aortic Dilatation in Patients Undergoing Transcatheter Aortic Valve Replacement Is Negatively Correlated with the Presence of Diabetes Mellitus and Does Not Impair Post-Procedural Outcomes

 , , ,
, , , 
Abstract
1. Introduction
- Can dilatation of the AA in TAVR patients be determined chemically in the laboratory by cardiovascular biomarkers, and can a pathophysiological link be established?
- Do patients with AS and AA dilatation who undergo TAVR have a survival disadvantage compared with patients with a normal AA?
- What clinical, echocardiographic or laboratory criteria/factors influence the diameter of the AA and potentially contribute to or even counteract ectasia?
2. Materials and Methods
2.1. Study Population
2.2. Transthoracic Echocardiography
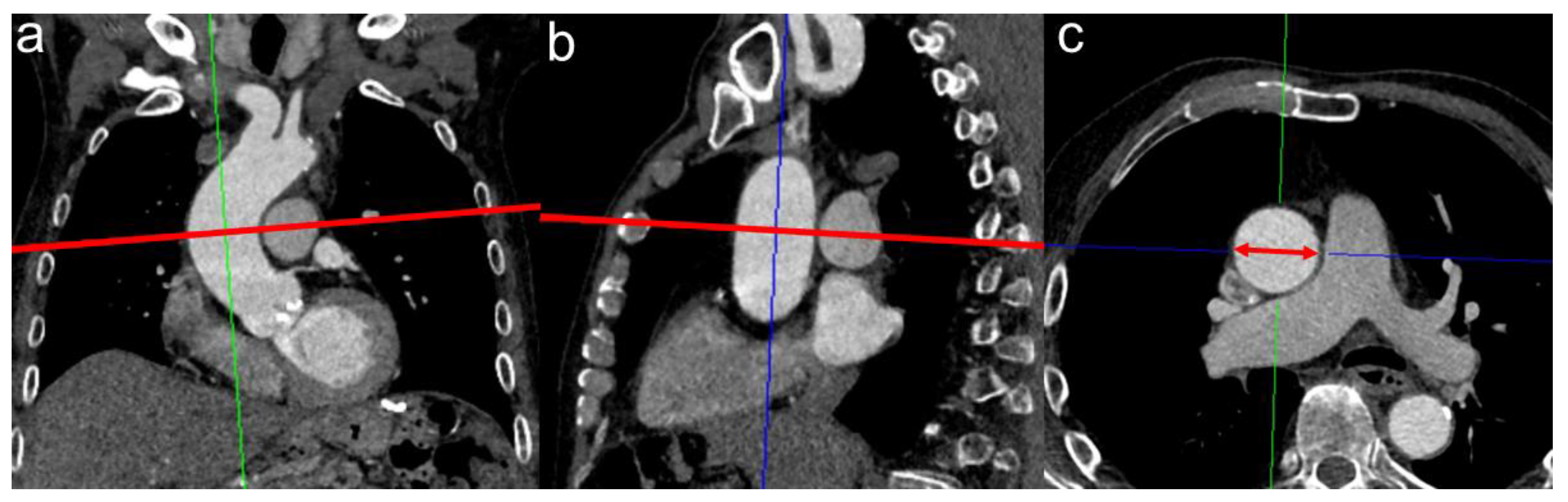
2.3. CTA Protocol and Measurement of MPA Diameter for PH Assessment
2.4. Biomarker Analysis
2.5. TAVR Procedure
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
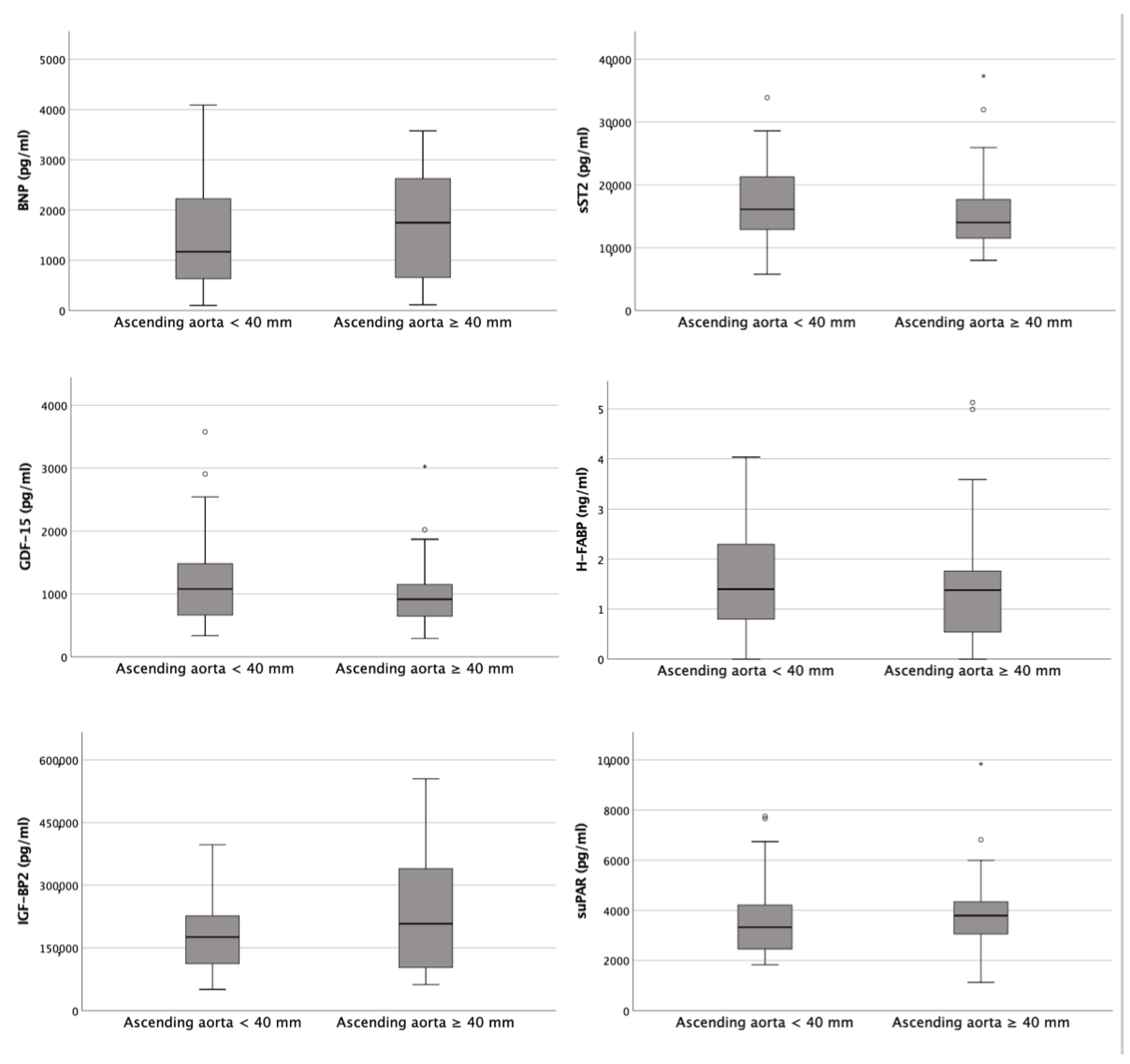
3.2. Biomarker Concentrations
3.3. Kaplan–Meier Curves
3.4. Correlation Analysis
4. Discussion
4.1. Biomarkers Examined Not Indicative of Vascular Remodeling
4.2. Mortality after TAVR Is Not Affected by the Presence of AA Dilatation
4.3. Aortic Dilatation and Diabetes Mellitus Are Negatively Correlated
5. Conclusions
6. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Evangelista, A. Diseases of the aorta: Aneurysm of the ascending aorta. Heart Br. Card. Soc. 2010, 96, 979–985. [Google Scholar] [CrossRef]
- Rogers, I.S.; Massaro, J.M.; Truong, Q.A.; Mahabadi, A.A.; Kriegel, M.F.; Fox, C.S.; Thanassoulis, G.; Isselbacher, E.M.; Hoffmann, U.; O’Donnell, C.J. Distribution, determinants, and normal reference values of thoracic and abdominal aortic diameters by computed tomography (from the Framingham Heart Study). Am. J. Cardiol. 2013, 111, 1510–1516. [Google Scholar] [CrossRef] [PubMed]
- Kerneis, C.; Pasi, N.; Arangalage, D.; Nguyen, V.; Mathieu, T.; Verdonk, C.; Codogno, I.; Ou, P.; Duval, X.; Tubiana, S.; et al. Ascending aorta dilatation rates in patients with tricuspid and bicuspid aortic stenosis: The COFRASA/GENERAC study. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Wilton, E.; Jahangiri, M. Post-stenotic aortic dilatation. J. Cardiothorac. Surg. 2006, 1, 7. [Google Scholar] [CrossRef] [PubMed]
- Balint, B.; Federspiel, J.M.; Schwab, T.; Ehrlich, T.; Ramsthaler, F.; Schäfers, H.J. Aortic Regurgitation Is Associated With Ascending Aortic Remodeling in the Nondilated Aorta. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 1179–1190. [Google Scholar] [CrossRef] [PubMed]
- Avvedimento, M.; Tang, G. Transcatheter aortic valve replacement (TAVR): Recent updates. Prog. Cardiovasc. Dis. 2021, 69, 73–83. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, J.H.; Lee, S.H.; Lee, S.; Youn, Y.N.; Yoo, K.J.; Joo, H.C. Long-term Fate of Dilated Ascending Aorta after Aortic Valve Replacement for Bicuspid Versus Tricuspid Aortic Valve Disease. Am. J. Cardiol. 2020, 129, 53–59. [Google Scholar] [CrossRef]
- Ruparelia, N.; Prendergast, B.D. TAVI in 2015: Who, where and how? Heart Br. Card. Soc. 2015, 101, 1422–1431. [Google Scholar] [CrossRef] [PubMed]
- Wischhusen, J.; Melero, I.; Fridman, W.H. Growth/Differentiation Factor-15 (GDF-15): From Biomarker to Novel Targetable Immune Checkpoint. Front. Immunol. 2020, 11, 951. [Google Scholar] [CrossRef]
- Wesseling, M.; de Poel, J.; de Jager, S. Growth differentiation factor 15 in adverse cardiac remodelling: From biomarker to causal player. ESC Heart Fail. 2020, 7, 1488–1501. [Google Scholar] [CrossRef]
- Sökmen, E.; Uçar, C.; Sivri, S.; Çelik, M.; Güçlü, K. Relationship of growth differentiation factor-15 with aortic stiffness in essential hypertension. Future Sci. OA 2019, 5, FSO406. [Google Scholar] [CrossRef]
- Kim, H.L.; Lee, J.P.; Lim, W.H.; Seo, J.B.; Zo, J.H.; Kim, M.A.; Kim, S.H. Association between the level of serum soluble ST2 and invasively measured aortic pulse pressure in patients undergoing coronary angiography. Medicine 2019, 98, e14215. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Xu, C.; Zhao, R.; Cao, Z. Diagnostic Value of sST2 in Cardiovascular Diseases: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2021, 8, 697837. [Google Scholar] [CrossRef]
- Chen, K.; Chen, Q.J.; Wang, L.J.; Liu, Z.H.; Zhang, Q.; Yang, K.; Wang, H.B.; Yan, X.X.; Zhu, Z.B.; Du, R.; et al. Increment of HFABP Level in Coronary Artery In-Stent Restenosis Segments in Diabetic and Nondiabetic Minipigs: HFABP Overexpression Promotes Multiple Pathway-Related Inflammation, Growth and Migration in Human Vascular Smooth Muscle Cells. J. Vasc. Res. 2016, 53, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Iida, M.; Yamazaki, M.; Honjo, H.; Kodama, I.; Kamiya, K. Predictive value of heart-type fatty acid-binding protein for left ventricular remodelling and clinical outcome of hypertensive patients with mild-to-moderate aortic valve diseases. J. Hum. Hypertens. 2007, 21, 551–557. [Google Scholar] [CrossRef]
- Gustafsson, T.; Andersson, P.; Chen, Y.; Magnusson, J.O.; Arnqvist, H.J. Interaction of angiotensin II and the insulin-like growth factor system in vascular smooth muscle cells. Am. J. Physiol. 1999, 277, H499–H507. [Google Scholar] [CrossRef] [PubMed]
- Muessig, J.M.; Lichtenauer, M.; Wernly, B.; Kelm, M.; Franz, M.; Bäz, L.; Schulze, P.C.; Racher, V.; Zimmermann, G.; Figulla, H.R.; et al. Insulin like growth factor binding protein 2 (IGFBP-2) for risk prediction in patients with severe aortic stenosis undergoing Transcatheter Aortic Valve Implantation (TAVI). Int. J. Cardiol. 2019, 277, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Thunø, M.; Macho, B.; Eugen-Olsen, J. suPAR: The molecular crystal ball. Dis. Mark. 2009, 27, 157–172. [Google Scholar] [CrossRef]
- Deng, G.G.; Martin-McNulty, B.; Sukovich, D.A.; Freay, A.; Halks-Miller, M.; Thinnes, T.; Loskutoff, D.J.; Carmeliet, P.; Dole, W.P.; Wang, Y.X. Urokinase-type plasminogen activator plays a critical role in angiotensin II-induced abdominal aortic aneurysm. Circ. Res. 2003, 92, 510–517. [Google Scholar] [CrossRef]
- Böcskei, R.M.; Benczúr, B.; Losonczy, G.; Illyés, M.; Cziráki, A.; Müller, V.; Bohács, A.; Bikov, A. Soluble Urokinase-Type Plasminogen Activator Receptor and Arterial Stiffness in Patients with COPD. Lung 2019, 197, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Crawford, M.H.; Roldan, C.A. Prevalence of aortic root dilatation and small aortic roots in valvular aortic stenosis. Am. J. Cardiol. 2001, 87, 1311–1313. [Google Scholar] [CrossRef] [PubMed]
- Benedik, J.; Pilarzcyk, K.; Wendt, D.; Price, V.; Tsagakis, K.; Perrey, M.; Baba, H.A.; Jakob, H. Is there any difference in aortic wall quality between patients with aortic stenosis and those with regurgitation? Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2013, 44, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Son, J.Y.; Ko, S.M.; Choi, J.W.; Song, M.G.; Hwang, H.K.; Lee, S.J.; Kang, J.W. Measurement of the ascending aorta diameter in patients with severe bicuspid and tricuspid aortic valve stenosis using dual-source computed tomography coronary angiography. Int. J. Cardiovasc. Imaging 2011, 27 (Suppl. S1), 61–71. [Google Scholar] [CrossRef] [PubMed]
- Ancona, M.B.; Moroni, F.; Chieffo, A.; Spangaro, A.; Federico, F.; Ferri, L.A.; Bellini, B.; Carlino, M.; Romano, V.; Palmisano, A.; et al. Impact of Ascending Aorta Dilation on Mid-Term Outcome After Transcatheter Aortic Valve Implantation. J. Invasive Cardiol. 2019, 31, 278–281. [Google Scholar]
- Girdauskas, E.; Disha, K.; Borger, M.A.; Kuntze, T. Long-term prognosis of ascending aortic aneurysm after aortic valve replacement for bicuspid versus tricuspid aortic valve stenosis. J. Thorac. Cardiovasc. Surg. 2014, 147, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Rylski, B.; Szeto, W.Y.; Bavaria, J.E.; Walsh, E.; Anwaruddin, S.; Desai, N.D.; Moser, W.; Herrmann, H.C.; Milewski, R.K. Transcatheter aortic valve implantation in patients with ascending aortic dilatation: Safety of the procedure and mid-term follow-up. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2014, 46, 228–233. [Google Scholar] [CrossRef]
- Lv, W.Y.; Zhao, Z.G.; Li, S.J.; Li, Y.J.; Liao, Y.B.; Ou, Y.W.; Feng, Y.; Chen, M. Progression of the Ascending Aortic Diameter After Transcatheter Aortic Valve Implantation: Based on Computed Tomography Images. J. Invasive Cardiol. 2019, 31, E234–E241. [Google Scholar]
- He, Y.X.; Fan, J.Q.; Zhu, Q.F.; Zhou, Q.J.; Jiang, J.B.; Wang, L.H.; Ng, S.; Liu, X.B.; Wang, J.A. Ascending aortic dilatation rate after transcatheter aortic valve replacement in patients with bicuspid and tricuspid aortic stenosis: A multidetector computed tomography follow-up study. World J. Emerg. Med. 2019, 10, 197–204. [Google Scholar] [CrossRef]
- Avdic, T.; Franzén, S.; Zarrouk, M.; Acosta, S.; Nilsson, P.; Gottsäter, A.; Svensson, A.M.; Gudbjörnsdottir, S.; Eliasson, B. Reduced Long-Term Risk of Aortic Aneurysm and Aortic Dissection Among Individuals with Type 2 Diabetes Mellitus: A Nationwide Observational Study. J. Am. Heart Assoc. 2018, 7, e007618. [Google Scholar] [CrossRef]
- Golledge, J.; Karan, M.; Moran, C.S.; Muller, J.; Clancy, P.; Dear, A.E.; Norman, P.E. Reduced expansion rate of abdominal aortic aneurysms in patients with diabetes may be related to aberrant monocyte-matrix interactions. Eur. Heart J. 2008, 29, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Dua, M.M.; Miyama, N.; Azuma, J.; Schultz, G.M.; Sho, M.; Morser, J.; Dalman, R.L. Hyperglycemia modulates plasminogen activator inhibitor-1 expression and aortic diameter in experimental aortic aneurysm disease. Surgery 2010, 148, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.F.; Wang, J.A.; Lin, X.F.; Tang, L.J.; Yu, W.F.; Chen, H.; Xie, X.J.; Jiang, J.J.; Peng, X.H. Diabetes mellitus: Is it protective against aortic root dilatation? Cardiology 2009, 112, 138–143. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ascending Aorta < 40 mm n = 32 | Ascending Aorta ≥ 40 mm n = 32 | p | |
|---|---|---|---|
| Clinical Data | |||
| Age (years)—mean ± SD | 81.97 ± 5.41 | 82.06 ± 5.01 | 0.943 |
| Gender (male)—% | 75.0 | 75.0 | 1.000 |
| Weight (kg)—mean ± SD | 79.13 ± 12.78 | 80.34 ± 13.61 | 0.713 |
| Height (cm)—mean ± SD | 169.94 ± 7.46 | 172.00 ± 8.31 | 0.300 |
| BMI (kg/m2)—mean ± SD | 27.34 ± 3.84 | 27.12 ± 4.00 | 0.823 |
| BSA (m2)—mean ± SD | 1.90 ± 0.17 | 1.93 ± 0.18 | 0.527 |
| NYHA—median ± IQR | 3.00 ± 0.75 | 3.00 ± 1.00 | 0.859 |
| STSScore—mean ± SD | 2.23 ± 1.61 | 2.26 ± 1.09 | 0.996 |
| Concomitant Disease | |||
| Diabetes mellitus—% | 31.3 | 6.3 | 0.010 |
| Arterial hypertension—% | 78.1 | 65.6 | 0.266 |
| CVD—% | 81.3 | 71.9 | 0.376 |
| CVD—1 vessel—% | 25.0 | 21.9 | 0.881 |
| CVD—2 vessels—% | 9.4 | 3.1 | 0.334 |
| CVD—3 vessels—% | 9.4 | 6.3 | 0.697 |
| Myocardial infarction—% | 6.3 | 0.0 | 0.151 |
| Atrial fibrillation—% | 40.6 | 56.3 | 0.211 |
| Previous cardiac surgery—% | 9.4 | 9.4 | 1.000 |
| Pacemaker—% | 3.1 | 6.3 | 0.554 |
| Stroke—% | 6.3 | 3.1 | 0.329 |
| PAOD—% | 0.0 | 3.1 | 0.313 |
| COPD—% | 9.4 | 12.5 | 0.689 |
| Smoking—% | 11.2 | 14.6 | 0.588 |
| CTA | |||
| AA (mm)—mean ± SD | 34.99 ± 2.48 | 42.24 ± 2.19 | <0.001 |
| AA/BSA (mm/m2)—mean ± SD | 18.53 ± 1.86 | 22.13 ± 2.99 | <0.001 |
| Echocardiography | |||
| LVEF (%)—mean ± SD | 56.63 ± 12.15 | 52.41 ± 11.53 | 0.159 |
| LVEDD (mm)—mean ± SD | 44.25 ± 5.04 | 47.55 ± 5.77 | 0.221 |
| IVSD (mm)—mean ± SD | 16.00 ± 2.82 | 15.19 ± 2.79 | 0.271 |
| AV Vmax (m/s)—mean ± SD | 4.29 ± 0.60 | 4.34 ± 0.46 | 0.760 |
| AV dPmean (mmHg)—mean ± SD | 49.39 ± 13.93 | 46.44 ± 10.01 | 0.337 |
| AV dPmax (mmHg)—mean ± SD | 78.23 ± 20.07 | 75.66 ± 15.25 | 0.569 |
| sPAP (mmHg)—mean ± SD | 43.81 ± 14.16 | 43.39 ± 27.85 | 0.921 |
| TAPSE (mm)—mean ± SD | 19.54 ± 3.45 | 20.98 ± 3.71 | 0.317 |
| AVI ≥ II—% | 6.3 | 21.9 | 0.060 |
| MVI ≥ II—% | 9.4 | 15.6 | 0.421 |
| TVI ≥ II—% | 9.4 | 12.5 | 0.623 |
| Laboratory Data | |||
| Crea (mg/dL)—median ± IQR | 1.10 ± 0.30 | 1.00 ± 0.28 | 0.326 |
| BNP (pg/mL)—median ± IQR | 1171.00 ± 1740.35 | 1749.50 ± 2010.08 | 0.492 |
| cTnI (pg/mL)—median ± IQR | 34.00 ± 73.75 | 27.00 ± 19.75 | 0.437 |
| Hkt (%)—median ± IQR | 38.20 ± 5.58 | 39.90 ± 2.08 | 0.103 |
| Hb (g/dL)—median ± IQR | 12.70 ± 2.35 | 13.50 ± 2.08 | 0.046 |
| CK (U/L)—median ± IQR | 73.00 ± 97.00 | 105.50 ± 73.75 | 0.479 |
| sST2 (pg/mL)—median ± IQR | 16,114.20 ± 8429.98 | 14,022.15 ± 6256.30 | 0.223 |
| GDF-15 (pg/mL)—median ± IQR | 1080.69 ± 871.92 | 916.977 ± 585.08 | 0.263 |
| H-FABP (ng/mL)—median ± IQR | 1.40 ± 1.62 | 1.38 ± 1.28 | 0.693 |
| IGF-BP2 (pg/mL)—median ± IQR | 176,048.92 ± 124,161.99 | 207,738.60 ± 276,393.81 | 0.750 |
| suPAR (pg/mL)—median ± IQR | 3322.47 ± 1935.84 | 3788.97 ± 1452.53 | 0.143 |
| Correlation | AA ≥ 40 mm | AA | AA/BSA | |||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| NYHA | −0.043 | 0.818 | −0.046 | 0.804 | −0.064 | 0.732 |
| Diabetes mellitus | −0.320 | 0.010 | −0.404 | 0.001 | −0.350 | 0.005 |
| Arterial hypertension | −0.139 | 0.273 | −0.098 | 0.441 | −0.143 | 0.260 |
| CVD | −0.111 | 0.384 | −0.193 | 0.126 | −0.293 | 0.019 |
| CVD—1 | −0.019 | 0.884 | 0.006 | 0.966 | −0.143 | 0.275 |
| CVD—2 | −0.125 | 0.342 | −0.145 | 0.269 | −0.019 | 0.884 |
| CVD—3 | −0.050 | 0.703 | −0.157 | 0.231 | −0.148 | 0.259 |
| Myocardial infarction | −0.180 | 0.156 | −0.193 | 0.127 | 0.061 | 0.633 |
| Atrial fibrillation | 0.156 | 0.217 | 0.255 | 0.042 | 0.132 | 0.298 |
| Previous cardiac surgery | 0.000 | 1.000 | 0.045 | 0.723 | −0.036 | 0.776 |
| Pacemaker | 0.074 | 0.562 | 0.102 | 0.421 | 0.104 | 0.413 |
| Stroke | 0.124 | 0.337 | 0.129 | 0.317 | 0.168 | 0.191 |
| PAOD | 0.126 | 0.321 | 0.099 | 0.436 | 0.140 | 0.270 |
| COPD | 0.050 | 0.694 | 0.030 | 0.815 | −0.009 | 0.941 |
| LVEF | −0.179 | 0.157 | −0.197 | 0.119 | −0.208 | 0.100 |
| LVEDD | 0.227 | 0.364 | 0.476 | 0.046 | 0.202 | 0.422 |
| IVSD | −0.144 | 0.277 | −0.130 | 0.325 | −0.244 | 0.063 |
| AV Vmax | −0.005 | 0.973 | 0.114 | 0.413 | −0.057 | 0.680 |
| AV dpmean | −0.122 | 0.339 | −0.102 | 0.426 | −0.210 | 0.099 |
| AV dpmax | −0.090 | 0.483 | −0.032 | 0.806 | −0.137 | 0.285 |
| sPAP | −0.082 | 0.541 | 0.034 | 0.800 | 0.043 | 0.747 |
| TAPSE | 0.228 | 0.263 | 0.159 | 0.438 | 0.049 | 0.812 |
| AVI ≥ II° | 0.254 | 0.061 | 0.278 | 0.040 | 0.238 | 0.080 |
| MVI ≥ II° | 0.101 | 0.429 | 0.112 | 0.383 | 0.130 | 0.311 |
| TVI ≥ II° | 0.063 | 0.629 | 0.187 | 0.145 | 0.215 | 0.093 |
| Crea | −0.124 | 0.329 | −0.110 | 0.387 | −0.148 | 0.242 |
| BNP | 0.092 | 0.497 | 0.055 | 0.685 | −0.076 | 0.574 |
| cTnI | −0.205 | 0.415 | −0.286 | 0.249 | −0.309 | 0.211 |
| Hkt | 0.206 | 0.103 | 0.135 | 0.287 | −0.006 | 0.960 |
| Hb | 0.251 | 0.045 | 0.152 | 0.231 | −0.023 | 0.858 |
| CK | 0.090 | 0.483 | −0.082 | 0.524 | −0.185 | 0.147 |
| sST2 | −0.156 | 0.226 | −0.111 | 0.389 | −0.148 | 0.252 |
| GDF−15 | −0.143 | 0.266 | −0.129 | 0.318 | −0.179 | 0.163 |
| H−FABP | −0.051 | 0.696 | −0.020 | 0.875 | 0.024 | 0.854 |
| IGF−BP2 | 0.081 | 0.727 | 0.275 | 0.227 | 0.462 | 0.035 |
| suPAR | 0.187 | 0.145 | 0.002 | 0.989 | 0.167 | 0.195 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boxhammer, E.; Hecht, S.; Kaufmann, R.; Kammler, J.; Kellermair, J.; Reiter, C.; Akbari, K.; Blessberger, H.; Steinwender, C.; Lichtenauer, M.; et al. The Presence of Ascending Aortic Dilatation in Patients Undergoing Transcatheter Aortic Valve Replacement Is Negatively Correlated with the Presence of Diabetes Mellitus and Does Not Impair Post-Procedural Outcomes. Diagnostics 2023, 13, 358. https://doi.org/10.3390/diagnostics13030358
Boxhammer E, Hecht S, Kaufmann R, Kammler J, Kellermair J, Reiter C, Akbari K, Blessberger H, Steinwender C, Lichtenauer M, et al. The Presence of Ascending Aortic Dilatation in Patients Undergoing Transcatheter Aortic Valve Replacement Is Negatively Correlated with the Presence of Diabetes Mellitus and Does Not Impair Post-Procedural Outcomes. Diagnostics. 2023; 13(3):358. https://doi.org/10.3390/diagnostics13030358
Chicago/Turabian StyleBoxhammer, Elke, Stefan Hecht, Reinhard Kaufmann, Jürgen Kammler, Jörg Kellermair, Christian Reiter, Kaveh Akbari, Hermann Blessberger, Clemens Steinwender, Michael Lichtenauer, and et al. 2023. "The Presence of Ascending Aortic Dilatation in Patients Undergoing Transcatheter Aortic Valve Replacement Is Negatively Correlated with the Presence of Diabetes Mellitus and Does Not Impair Post-Procedural Outcomes" Diagnostics 13, no. 3: 358. https://doi.org/10.3390/diagnostics13030358
APA StyleBoxhammer, E., Hecht, S., Kaufmann, R., Kammler, J., Kellermair, J., Reiter, C., Akbari, K., Blessberger, H., Steinwender, C., Lichtenauer, M., Hoppe, U. C., Hergan, K., & Scharinger, B. (2023). The Presence of Ascending Aortic Dilatation in Patients Undergoing Transcatheter Aortic Valve Replacement Is Negatively Correlated with the Presence of Diabetes Mellitus and Does Not Impair Post-Procedural Outcomes. Diagnostics, 13(3), 358. https://doi.org/10.3390/diagnostics13030358