
Home versus Clinic Blood Pressure Monitoring: Evaluating Applicability in Hypertension Management via Telemedicine


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
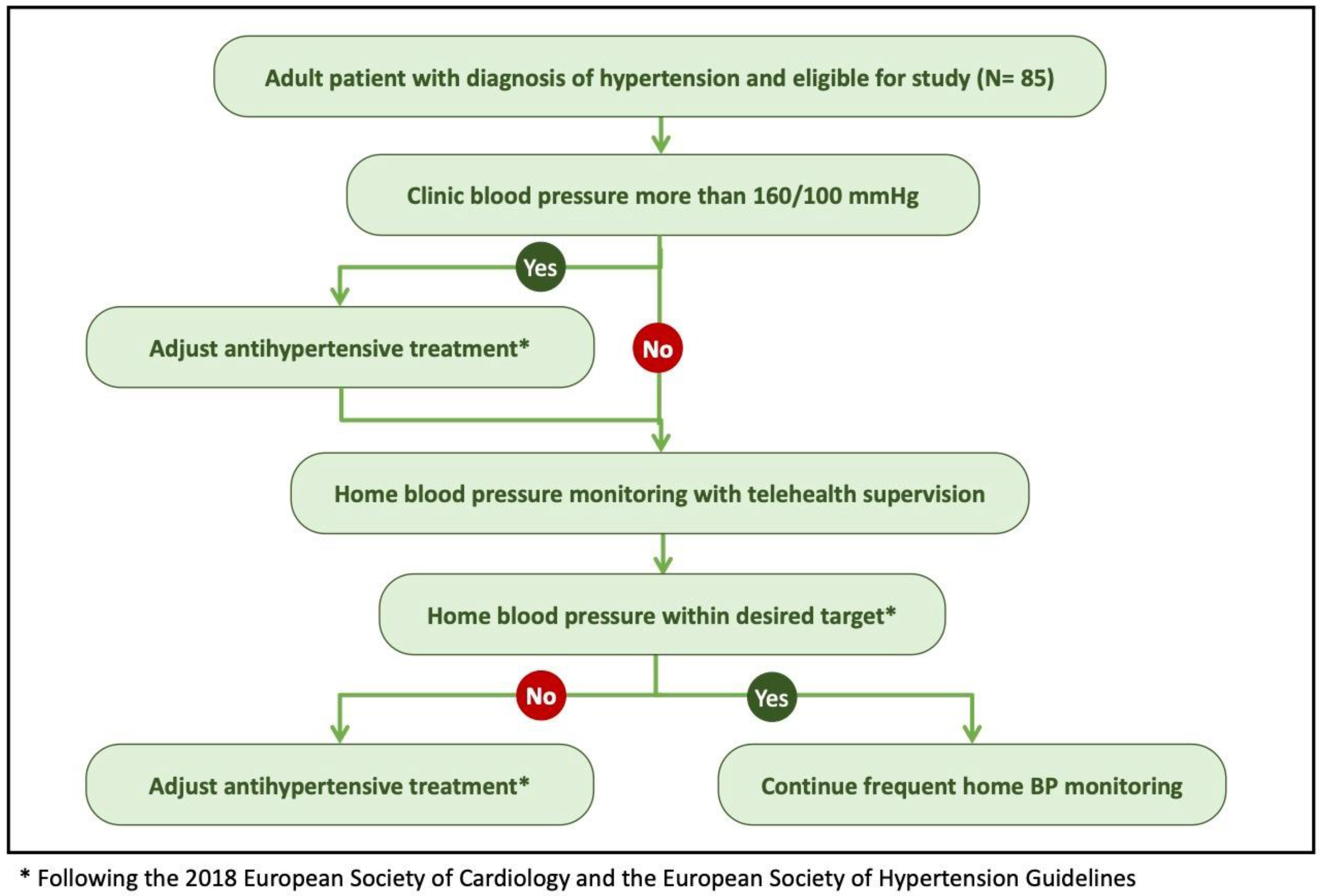
2.2. Study Design
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Home and Clinic Blood Pressure Measurements
2.6. Statistical Analyses
3. Results
4. Discussion
4.1. Difference between CSBP and HSBP
4.2. Telehealth in the Management of Hypertension
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Al-Nozha, M.M.; Abdullah, M.; Arafah, M.R.; Khalil, M.Z.; Khan, N.B.; Al-Mazrou, Y.Y.; A Al-Maatouq, M.; Al-Marzouki, K.; Al-Khadra, A.; Nouh, M.S.; et al. Hypertension in Saudi Arabia. Saudi Med. J. 2007, 28, 77–84. [Google Scholar]
- Son, J.S.; Choi, S.; Kim, K.; Kim, S.M.; Choi, D.; Lee, G.; Jeong, S.-M.; Park, S.Y.; Kim, Y.-Y.; Yun, J.-M.; et al. Association of blood pressure classification in Korean young adults according to the 2017 American College of Cardiology/American Heart Association guidelines with subsequent cardiovascular disease events. JAMA 2018, 320, 1783–1792. [Google Scholar] [CrossRef]
- Hsu, C.Y.; McCulloch, C.E.; Darbinian, J.; Go, A.S.; Iribarren, C. Elevated blood pressure and risk of end-stage renal disease in subjects without baseline kidney disease. Arch. Intern. Med. 2005, 165, 923–928. [Google Scholar] [CrossRef]
- SPRINT Research Group; Wright, J.T.; Williamson, J.D.; Whelton, P.K.; Snyder, J.K.; Sink, K.M.; Rocco, M.V.; Reboussin, D.M.; Rahman, M.; Oparil, S.; et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N. Engl. J. Med. 2015, 373, 2103–2116. [Google Scholar] [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar] [CrossRef]
- Correction to: Heart Disease and Stroke Statistics-2019 Update: A Report from the American Heart Association. Circulation 2020, 141, e33. [CrossRef]
- Bakris, G.L. The implications of blood pressure measurement methods on treatment targets for blood pressure. Circulation 2016, 134, 904–905. [Google Scholar] [CrossRef][Green Version]
- Al-Karkhi, I.; Al-Rubaiy, R.; Rosenqvist, U.; Falk, M.; Nystrom, F.H. Comparisons of automated blood pressures in a primary health care setting with self-measurements at the office and at home using the Omron i-C10 device. Blood Press. Monit. 2015, 20, 98–103. [Google Scholar] [CrossRef]
- Niiranen, T.J.; Hänninen, M.R.; Johansson, J.; Reunanen, A.; Jula, A.M. Home-measured blood pressure is a stronger predictor of cardiovascular risk than office blood pressure: The Finn-Home study. Hypertension 2010, 55, 1346–1351. [Google Scholar] [CrossRef]
- Mahmud, A.; Alahaideb, R.; Alshammary, H.; Abanumay, M.; Alfawwaz, A.; Alhelabi, S.; Alonazy, A.; Al-Zaibag, M. Prevalence and clinical correlates of ambulatory blood pressure phenotypes in a Saudi hypertensive population. J. Clin. Hypertens. 2020, 22, 2372–2376. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Verberk, W.J.; Kroon, A.A.; Kessels, A.G.; de Leeuw, P.W. Home blood pressure measurement: A systematic review. J. Am. Coll. Cardiol. 2005, 46, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Wetterholm, M.; Bonn, S.; Alexandrou, C.; Löf, M.; Trolle Lagerros, Y. Validation of Two Automatic Blood Pressure Monitors with the Ability to Transfer Data via Bluetooth. J. Med. Internet Res. 2019, 21, e12772. [Google Scholar] [CrossRef] [PubMed]
- BM 85 Blood Pressure Monitor. Available online: https://pim.beurer.com/images/attribut/658.03_BM85_2019-10-10_03_IM1_BEU.pdf (accessed on 16 July 2023).
- Geratherm Medical AG. Available online: https://www.manualslib.com/manual/1736003/Geratherm-Smart-Gt-1775.html?page=70&term=iso&selected=8#manual (accessed on 16 July 2023).
- Parati, G.; Stergiou, G.S.; Asmar, R.; Bilo, G.; de Leeuw, P.; Imai, Y.; Kario, K.; Lurbe, E.; Manolis, A.; Mengden, T.; et al. European Society of Hypertension practice guidelines for home blood pressure monitoring. J. Hum. Hypertens. 2010, 24, 779–785. [Google Scholar] [CrossRef]
- Imai, Y.; Kario, K.; Shimada, K.; Kawano, Y.; Hasebe, N.; Matsuura, H.; Tsuchihashi, T.; Ohkubo, T.; Kuwajima, I.; Miyakawa, M. The Japanese Society of Hypertension guidelines for self-monitoring of blood pressure at home (second edition). Hypertens. Res. 2012, 35, 777–795. [Google Scholar] [CrossRef]
- Sharman, J.E.; Howes, F.S.; Head, G.A.; McGrath, B.P.; Stowasser, M.; Schlaich, M.; Glasziou, P.; Nelson, M. How to measure home blood pressure: Recommendations for healthcare professionals and patients. Aust. Fam. Physician 2016, 45, 31–34. [Google Scholar]
- Guo, Q.H.; Cheng, Y.; Zhang, D.Y.; Wang, Y.; Huang, Q.-F.; Sheng, C.-S.; Xu, T.-Y.; Li, Y.; Wang, J.-G. Comparison between home and ambulatory morning blood pressure and morning hypertension in their reproducibility and associations with vascular injury. Hypertension 2019, 74, 137–144. [Google Scholar] [CrossRef]
- Miao, H.; Yang, S.; Zhang, Y. Differences of blood pressure measured at clinic versus at home in the morning and in the evening in Europe and Asia: A systematic review and meta-analysis. J. Clin. Hypertens. 2022, 24, 677–688. [Google Scholar] [CrossRef]
- Masugata, H.; Senda, S.; Inukai, M.; Himoto, T.; Hosomi, N.; Murao, K.; Okada, H.; Goda, F. Clinical significance of differences between home and clinic systolic blood pressure readings in patients with hypertension. J. Int. Med. Res. 2013, 41, 1272–1280. [Google Scholar] [CrossRef]
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.; Hill, M.N.; Jones, D.W.; Kurtz, T.; Sheps, S.G.; Roccella, E.J. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans: A statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension 2005, 45, 142–161. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef] [PubMed]
- Omboni, S.; McManus, R.J.; Bosworth, H.B.; Chappell, L.C.; Green, B.B.; Kario, K.; Logan, A.G.; Magid, D.J.; Mckinstry, B.; Margolis, K.L.; et al. Evidence and recommendations on the use of telemedicine for the management of arterial hypertension: An international expert position paper. Hypertension 2020, 76, 1368–1383. [Google Scholar] [CrossRef] [PubMed]
- Omboni, S.; Gazzola, T.; Carabelli, G.; Parati, G. Clinical usefulness and cost effectiveness of home blood pressure telemonitoring: Meta-analysis of randomized controlled studies. J. Hypertens. 2013, 31, 455–467; discussion 467–468. [Google Scholar] [CrossRef] [PubMed]
- Kario, K.; Park, S.; Buranakitjaroen, P.; Chia, Y.-C.; Chen, C.-H.; Divinagracia, R.; Hoshide, S.; Shin, J.; Siddique, S.; Sison, J.; et al. Guidance on home blood pressure monitoring: A statement of the HOPE Asia Network. J. Clin. Hypertens. 2018, 20, 456–461. [Google Scholar] [CrossRef]
- Parati, G.; Dolan, E.; McManus, R.J.; Omboni, S. Home blood pressure telemonitoring in the 21st century. J. Clin. Hypertens. 2018, 20, 1128–1132. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.E.; Wild, K. Using telehealth in the management of hypertension. Nurs. Stand. 2017, 31, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Tucker, K.L.; Sheppard, J.P.; Stevens, R.; Bosworth, H.B.; Bove, A.; Bray, E.P.; Earle, K.; George, J.; Godwin, M.; Green, B.B.; et al. Self-monitoring of blood pressure in hypertension: A systematic review and individual patient data meta-analysis. PLoS Med. 2017, 14, e1002389. [Google Scholar] [CrossRef]
- Sheppard, J.P.; Tucker, K.L.; Davison, W.J.; Stevens, R.; Aekplakorn, W.; Bosworth, H.B.; Bove, A.; Earle, K.; Godwin, M.; Green, B.B.; et al. Self-monitoring of Blood Pressure in Patients with Hypertension-Related Multi-morbidity: Systematic Review and Individual Patient Data Meta-analysis. Am. J. Hypertens. 2020, 33, 243–251. [Google Scholar] [CrossRef]
- Kappes, M.; Espinoza, P.; Jara, V.; Hall, A. Nurse-led telehealth intervention effectiveness on reducing hypertension: A systematic review. BMC Nurs. 2023, 22, 19. [Google Scholar] [CrossRef]
- McManus, R.J.; Little, P.; Stuart, B.; Morton, K.; on behalf of the HOME BP investigators. Home and Online Management and Evaluation of Blood Pressure (HOME BP) using a digital intervention in poorly controlled hypertension: Randomised controlled trial. BMJ 2021, 372, m4858. [Google Scholar] [CrossRef]
- Stoddart, A.; Hanley, J.; Wild, S.; Pagliari, C.; Paterson, M.; Lewis, S.; Sheikh, A.; Krishan, A.; Padfield, P.; McKinstry, B. Telemonitoring-based service redesign for the management of uncontrolled hypertension (HITS): Cost and cost-effectiveness analysis of a randomised controlled trial. BMJ Open 2013, 3, e002681. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Sub-Category | Overall (n = 85) | Male (n = 44) | Female (n = 41) | χ2 | p-Value |
|---|---|---|---|---|---|---|
| Age (years) | Young age (<40) | 2 (2.4%) | 2 (2.4%) | 0 (0%) | 0.6064 | 0.7384 |
| Middle-aged adult (40–60) | 24 (28.2%) | 11 (13%) | 13 (15.2%) | |||
| Old adult (>60) | 59 (69.4%) | 31 (36.4%) | 28 (33%) | |||
| BMI (kg/m2) | Underweight (<18) | 2 (2.4%) | 1 (1.2%) | 1 (1.2%) | 11.3883 | 0.0098 |
| Normal (18–24) | 15 (18.8%) | 9 (11.7%) | 6 (7.1%) | |||
| Overweight (>24) | 18 (21.2%) | 15 (17.7%) | 3 (3.5%) | |||
| Obese (>29) | 50 (57.6%) | 19 (21.2%) | 31 (36.4%) | |||
| Nationality | Saudi | 84 (98.8%) | 43 (50.6%) | 41 (48.2%) | 0.0011 | 0.9734 |
| Egyptian | 1 (1.2%) | 1 (1.2%) | 0 (0%) | |||
| Smoking History | Yes | 3 (3.5%) | 3 (3.5%) | 0 (0%) | 3.9804 | 0.1366 |
| No | 77 (90.5%) | 36 (42.3%) | 41 (48.2%) | |||
| Ex-smoker | 5 (6%) | 5 (6%) | 0 (0%) | |||
| Newly diagnosed hypertension | 4 (4.7%) | 1 (1.2%) | 3 (3.5%) | 1.2043 | 0.2724 | |
| Medication adjusted in clinic | CBP Reading | 35 (41%) | 16 (21%) | 17 (20%) | 0.2324 | 0.6297 |
| Medication adjusted at home | HBP Reading | 41 (48.2%) | 21 (24.7%) | 20 (23.5%) | 0.0094 | 0.9226 |
| Variable | N | Mean | Median | SD | Range | Minimum | Maximum | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 81 | 64.43 | 64.00 | 11.85 | 58.00 | 33.00 | 91.00 | −0.20 | −0.11 |
| BMI (kg/m2) | 47 | 26.55 | 27.00 | 4.77 | 25.00 | 14.00 | 39.00 | 0.08 | 0.97 |
| Weight (kg) | 47 | 71.30 | 70.00 | 12.65 | 67.00 | 33.00 | 100.00 | −0.05 | 1.27 |
| Height (cm) | 47 | 162.55 | 162.00 | 7.01 | 29.00 | 148.00 | 177.00 | −0.05 | −0.55 |
| Duration HBP Monitoring | 85 | 4.87 | 5.00 | 0.75 | 6.00 | 1.00 | 7.00 | −2.53 | 11.18 |
| Clinic SBP | 85 | 159.45 | 160.00 | 16.09 | 75.00 | 125.00 | 200.00 | 0.06 | −0.12 |
| Clinic DBP | 85 | 79.14 | 80.00 | 11.80 | 53.00 | 57.00 | 110.00 | 0.33 | −0.53 |
| Home SBP (Day) | 84 | 140.69 | 141.13 | 16.83 | 91.00 | 92.00 | 183.00 | −0.11 | 0.88 |
| Home DBP (Day) | 84 | 75.76 | 75.63 | 9.77 | 58.00 | 54.00 | 112.00 | 0.54 | 1.18 |
| Home SBP (Evening) | 85 | 138.95 | 140.00 | 15.92 | 73.70 | 97.00 | 170.70 | −0.37 | −0.36 |
| Home DBP (Evening) | 85 | 75.20 | 74.00 | 9.27 | 46.50 | 57.50 | 104.00 | 0.63 | 0.54 |
| Home Day–Evening SBP (mean) | 85 | 138.99 | 141.50 | 17.75 | 118.00 | 54.50 | 172.50 | −1.35 | 5.34 |
| Home Day–Evening DBP (mean) | 85 | 75.03 | 74.50 | 9.75 | 68.00 | 40.00 | 108.00 | 0.08 | 2.15 |
| Clinic–Home SBP (difference) | 85 | 20.46 | 17.00 | 22.36 | 124.50 | −19.00 | 105.50 | 0.86 | 1.54 |
| Clinic–Home DBP (difference) | 85 | 4.11 | 6.00 | 13.02 | 88.00 | −38.00 | 50.00 | 0.10 | 1.79 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| Clinic SBP | — | |||||||
| Clinic DBP | 0.549 *** | — | ||||||
| Home SBP (Day) | 0.218 * | 0.126 | — | |||||
| Home DBP (Day) | 0.177 | 0.331 ** | 0.349 ** | — | ||||
| Home SBP (Evening) | 0.062 | 0.065 | 0.754 *** | 0.199 | — | |||
| Home DBP (Evening) | 0.059 | 0.338 ** | 0.150 | 0.786 *** | 0.240 * | — | ||
| Home Day–Evening SBP (mean) | 0.129 | 0.045 | 0.941 *** | 0.296 ** | 0.885 *** | 0.154 | — | |
| Home Day–Evening DBP (mean) | 0.115 | 0.282 ** | 0.267 * | 0.948 *** | 0.298 ** | 0.842 *** | 0.419 *** | — |
| Mean Difference between Clinic and Home Blood Pressures | ||||||
|---|---|---|---|---|---|---|
| Variable | n | M | SD | T (84) | p | Cohen’s d |
| CSBP | 85 | 159.4 | 16.09 | 8.43 | <0.001 | 0.92 |
| HSBP | 85 | 139.0 | 17.75 | |||
| CDBP | 85 | 79.1 | 11.80 | 2.91 | 0.005 | 0.32 |
| HDBP | 85 | 75.0 | 9.75 | |||
| Clinic Blood Pressure (CBP) | Home Blood Pressure (HBP) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Systolic BP | Diastolic BP | Systolic BP | Diastolic BP | ||||||||
| mmHg | n | % | mmHg | n | % | mmHg | n | % | mmHg | n | % |
| <120 | 0 | 0.0 | <80 | 55 | 64.7 | <120 | 8 | 9.4 | <80 | 64 | 75.3 |
| 120 | 0 | 0.0 | 80 | 21 | 24.7 | 120 | 1 | 1.2 | 80 | 9 | 10.6 |
| 130 | 4 | 4.7 | 80 | 130 | 13 | 15.3 | 80 | ||||
| 140 | 10 | 11.8 | 90 | 7 | 8.2 | 135 | 6 | 7.1 | 85 | 8 | 9.4 |
| 160 | 40 | 47.1 | 100 | 2 | 2.4 | 145 | 27 | 31.8 | 90 | 4 | 4.7 |
| >160 | 31 | 36.5 | >100 | 0 | 0 | >145 | 30 | 35.3 | >90 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Anazi, A.F.; Gul, R.; Al-Harbi, F.T.; Al-Radhi, S.A.; Al-Harbi, H.; Altaher, A.; Al-Harbi, M.M.; Al-Rashidi, F.O.; Al-Haweeri, O.S.; Al-Mutairi, F.M.; et al. Home versus Clinic Blood Pressure Monitoring: Evaluating Applicability in Hypertension Management via Telemedicine. Diagnostics 2023, 13, 2686. https://doi.org/10.3390/diagnostics13162686
Al-Anazi AF, Gul R, Al-Harbi FT, Al-Radhi SA, Al-Harbi H, Altaher A, Al-Harbi MM, Al-Rashidi FO, Al-Haweeri OS, Al-Mutairi FM, et al. Home versus Clinic Blood Pressure Monitoring: Evaluating Applicability in Hypertension Management via Telemedicine. Diagnostics. 2023; 13(16):2686. https://doi.org/10.3390/diagnostics13162686
Chicago/Turabian StyleAl-Anazi, Ali F., Rahim Gul, Fahad T. Al-Harbi, Sulaiman A. Al-Radhi, Hamood Al-Harbi, Altigani Altaher, Mohammed M. Al-Harbi, Fahad O. Al-Rashidi, Omer S. Al-Haweeri, Fakhri M. Al-Mutairi, and et al. 2023. "Home versus Clinic Blood Pressure Monitoring: Evaluating Applicability in Hypertension Management via Telemedicine" Diagnostics 13, no. 16: 2686. https://doi.org/10.3390/diagnostics13162686
APA StyleAl-Anazi, A. F., Gul, R., Al-Harbi, F. T., Al-Radhi, S. A., Al-Harbi, H., Altaher, A., Al-Harbi, M. M., Al-Rashidi, F. O., Al-Haweeri, O. S., Al-Mutairi, F. M., Al-Riyaee, A. A., Al-Hotan, F. M., Al-Radhi, A. A., Al Shehri, H. M., Alharbi, M. S., & ALGhasab, N. S. (2023). Home versus Clinic Blood Pressure Monitoring: Evaluating Applicability in Hypertension Management via Telemedicine. Diagnostics, 13(16), 2686. https://doi.org/10.3390/diagnostics13162686