
Quantitative Measurement of Pneumothorax Using Artificial Intelligence Management Model and Clinical Application

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patient Selection
2.2. Hypothesis and Operational Definition
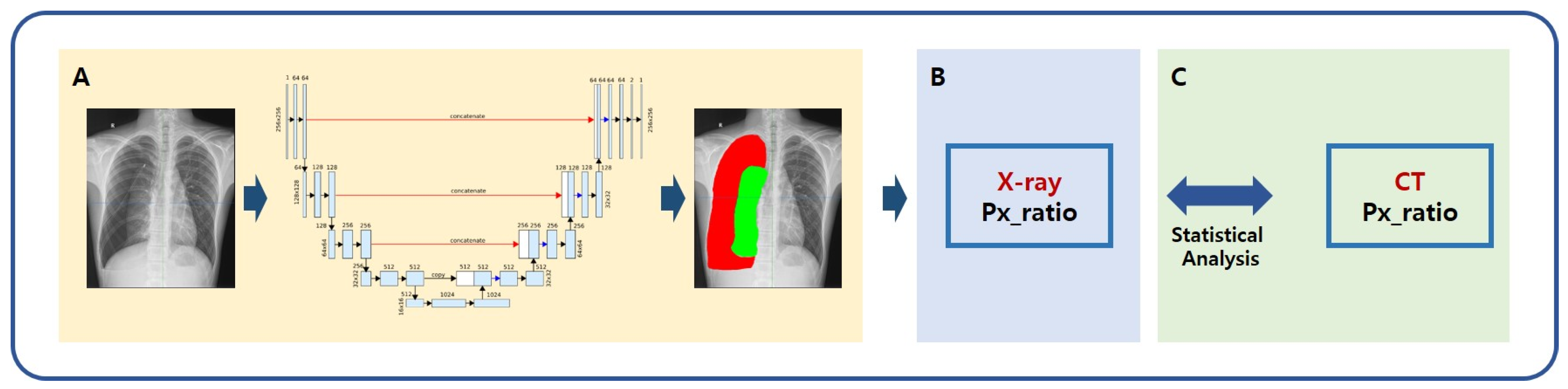
2.3. AI Modeling for Pneumothorax
2.3.1. Deep Learning Architecture with the Images Preprocessing Method
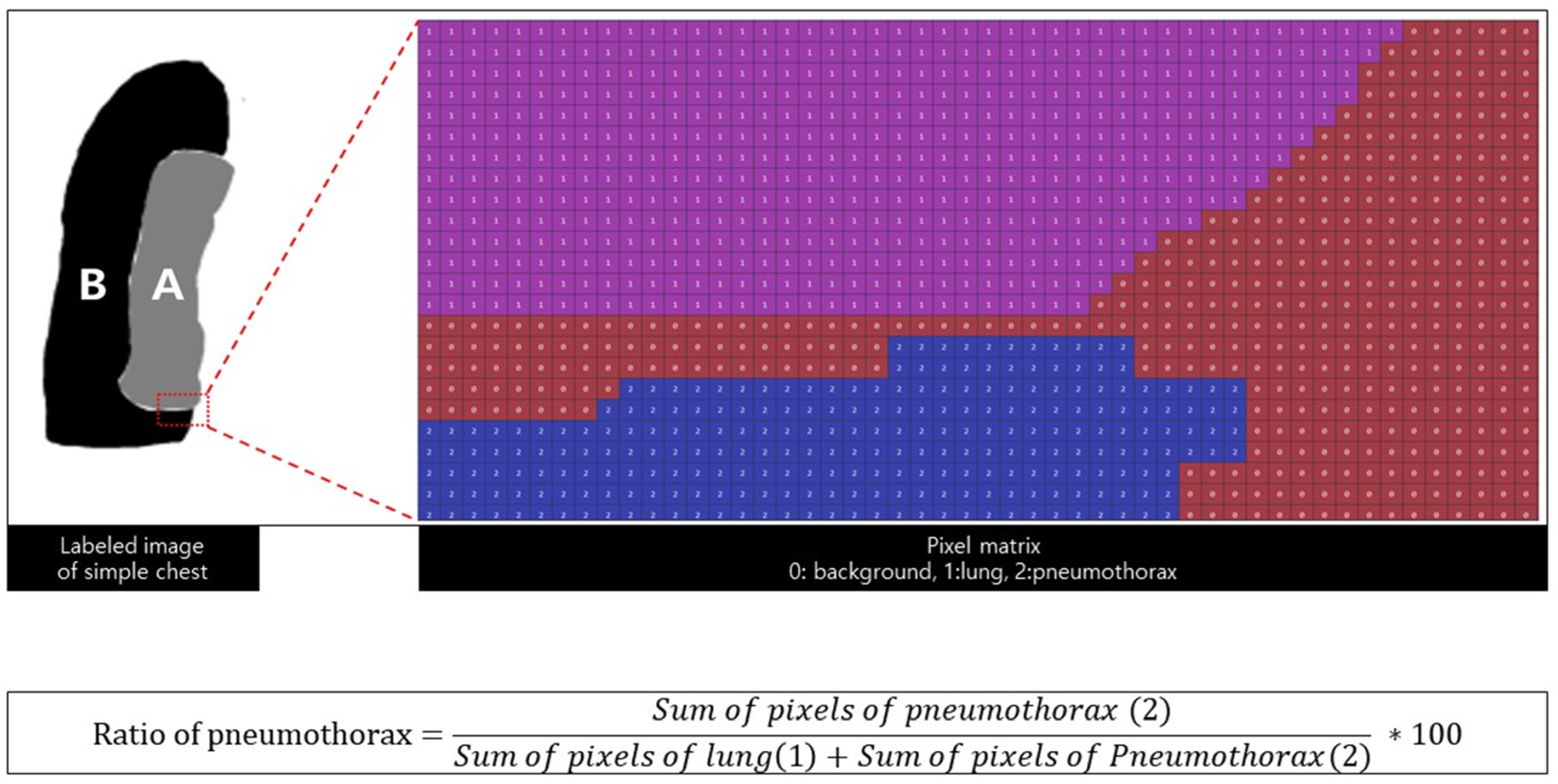
2.3.2. Quantification of Pneumothorax
2.3.3. Statistical Analysis
2.3.4. Performance Evaluation
3. Results
3.1. Patient Characteristics
3.2. Classification by Deep Learning Models
3.3. Quantification of Pneumothorax
3.4. Clinical Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, D.; Shin, H.J.; Kim, S.W.; Hong, J.M.; Lee, K.S.; Lee, S.H. Psychological Problems of Pneumothorax According to Resilience, Stress, and Post-Traumatic Stress. Psychiatry Investig. 2017, 14, 795–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nam, S.H.; Kim, K.W.; Kim, S.W.; Kim, S.W.; Hong, J.M.; Kim, D. Fate of Spontaneous Pneumothorax from Middle to Old Age: How to Overcome an Irritating Recurrence? J. Thorac. Dis. 2019, 11, 4782–4789. [Google Scholar] [CrossRef] [PubMed]
- Mendogni, P.; Vannucci, J.; Ghisalberti, M.; Anile, M.; Aramini, B.; Congedo, M.T.; Nosotti, M.; Bertolaccini, L.; D’Ambrosio, A.E.; Collaborators of the Pneumothorax Working Group; on behalf of the Italian Society for Thoracic Surgery (endorsed by the Italian Ministry of Health) Collaborators of the Pneumothorax Working Group. Epidemiology and Management of Primary Spontaneous Pneumothorax: A Systematic Review. Interact. Cardiovasc. Thorac. Surg. 2020, 30, 337–345. [Google Scholar] [CrossRef]
- Rim, T.; Bae, J.S.; Yuk, Y.S. Life-Threatening Simultaneous Bilateral Spontaneous Tension Pneumothorax—A Case Report. Korean J. Thorac. Cardiovasc. Surg. 2011, 44, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Ahn, H.Y.; Kim, Y.D.; Hoseok, I.; Cho, J.S.; Lee, J. Location of Ruptured Bullae in Secondary Spontaneous Pneumothorax. Korean J. Thorac. Cardiovasc. Surg. 2017, 50, 424–429. [Google Scholar] [CrossRef] [Green Version]
- Matsuoka, K.; Ito, A.; Murata, Y.; Kuwata, T.; Takasaki, C.; Imanishi, N.; Matsuoka, T.; Nagai, S.; Ueda, M.; Miyamoto, Y. Four Cases of Contralateral Pneumothorax After Pneumonectomy. Ann. Thorac. Surg. 2014, 98, 1461–1463. [Google Scholar] [CrossRef]
- Palmaers, T.; Frank, P.; Eismann, H.; Sieg, L.; Leffler, A.; Schmitt, H.; Scholler, A. Catheterization of the Subclavian Vein and the Risk of Pneumothorax: Mechanical Ventilation Increases the Risk of Pneumothorax During Infraclavicular Landmark-Guided Subclavian Vein Puncture: A Prospective Randomized Study. Anaesthesist 2019, 68, 309–316. [Google Scholar] [CrossRef]
- Kim, E.; Kim, H.J.; Hong, D.M.; Park, H.P.; Bahk, J.H. Influence of Mechanical Ventilation on the Incidence of Pneumothorax During Infraclavicular Subclavian Vein Catheterization: A Prospective Randomized Noninferiority Trial. Anesth. Analg. 2016, 123, 636–640. [Google Scholar] [CrossRef]
- Miller, J.D.; Carlo, W.A. Pulmonary Complications of Mechanical Ventilation in Neonates. Clin. Perinatol. 2008, 35, 273–281. [Google Scholar] [CrossRef]
- Plewa, M.C.; Ledrick, D.; Sferra, J.J. Delayed Tension Penumothorax Complicating Central Venous Catheterization and Positive Pressure Ventilation. Am. J. Emerg. Med. 1995, 13, 532–535. [Google Scholar] [CrossRef]
- Narula, N.; Siddiqui, F.; Siddiqui, A.H.; Man, W.C.; Chalhoub, M. Delayed Pneumothorax: A Potential Complication of Transbronchial Lung Biopsy. Respir. Med. Case Rep. 2018, 23, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.J.; Ahmed, A.; D’Souza, D.; Awad, H. Delayed Diagnosis of Contralateral Tension Pneumothorax During Robotic Lung Wedge Resection. J. Clin. Anesth. 2018, 45, 30–31. [Google Scholar] [CrossRef] [PubMed]
- Mnih, V.; Kavukcuoglu, K.; Silver, D.; Rusu, A.A.; Veness, J.; Bellemare, M.G.; Graves, A.; Riedmiller, M.; Fidjeland, A.K.; Ostrovski, G.; et al. Human-Level Control Through Deep Reinforcement Learning. Nature 2015, 518, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J.W.L. Artificial Intelligence in Radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef]
- MacDuff, A.; Arnold, A.; Harvey, J.; BTS Pleural Disease Guideline Group. Management of Spontaneous Pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010, 65 (Suppl. 2), ii18–ii31. [Google Scholar] [CrossRef] [Green Version]
- Baumann, M.H.; Strange, C.; Heffner, J.E.; Light, R.; Kirby, T.J.; Klein, J.; Luketich, J.D.; Panacek, E.A.; Sahn, S.A.; AACP Pneumothorax Consensus Group. Management of Spontaneous Pneumothorax: An American College of Chest Physicians Delphi Consensus Statement. Chest 2001, 119, 590–602. [Google Scholar] [CrossRef]
- Filosso, P.L.; Guerrera, F.; Sandri, A.; Roffinella, M.; Solidoro, P.; Ruffini, E.; Oliaro, A. Errors and Complications in Chest Tube Placement. Thorac. Surg. Clin. 2017, 27, 57–67. [Google Scholar] [CrossRef]
- Bintcliffe, O.J.; Hallifax, R.J.; Edey, A.; Feller-Kopman, D.; Lee, Y.C.G.; Marquette, C.H.; Tschopp, J.M.; West, D.; Rahman, N.M.; Maskell, N.A. Spontaneous Pneumothorax: Time to Rethink Management? Lancet Respir. Med. 2015, 3, 578–588. [Google Scholar] [CrossRef]
- Kholiavchenko, M.; Sirazitdinov, I.; Kubrak, K.; Badrutdinova, R.; Kuleev, R.; Yuan, Y.; Vrtovec, T.; Ibragimov, B. Contour-Aware Multi-Label Chest X-Ray Organ Segmentation. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 425–436. [Google Scholar] [CrossRef]
- Novikov, A.A.; Lenis, D.; Major, D.; Hladuvka, J.; Wimmer, M.; Buhler, K. Fully Convolutional Architectures for Multiclass Segmentation in Chest Radiographs. IEEE Trans. Med. Imaging 2018, 37, 1865–1876. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.W.; Kim, S.E.; Choi, E.Y.; Hong, K.S.; Oh, T.H.; Kim, U.J.; Kang, S.J.; Park, K.H.; Jung, S.I.; Kim, D.Y.; et al. Risk Factors and a Scoring System to Predict ARDS in Patients with COVID-19 Pneumonia in Korea: A Multicenter Cohort Study. Dis. Markers 2021, 2021, 8821697. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Yin, X.; Zhang, T.; Feng, Y.; Zhao, Y.; Jin, M.; Peng, M.; Xing, C.; Li, F.; Wang, Z.; et al. Detection and Semiquantitative Analysis of Cardiomegaly, Pneumothorax, and Pleural Effusion on Chest Radiographs. Radiol. Artif. Intell. 2021, 3, e200172. [Google Scholar] [CrossRef] [PubMed]
- Noppen, M.; De Keukeleire, T. Pneumothorax. Respiration 2008, 76, 121–127. [Google Scholar] [CrossRef]
- Kircher, L.T.; Swartzel, R.L. Spontaneous Pneumothorax and Its Treatment. J. Am. Med. Assoc. 1954, 155, 24–29. [Google Scholar] [CrossRef]
- Islam, S.; Rehana, H.; Asaduzzaman, S.; Hossen, S.M.; Hossain, R.; Bhuiyan, T.; Uddin, M.S.; Akter, N. Automated Risk Prediction by Measuring Pneumothorax Size Using Deep Learning. In Proceedings of the 2020 IEEE Region 10 Symposium (TENSYMP), Dhaka, Bangladesh, 5–7 June 2020; Volume 2020. [Google Scholar] [CrossRef]
- Röhrich, S.; Schlegl, T.; Bardach, C.; Prosch, H.; Langs, G. Deep Learning Detection and Quantification of Pneumothorax in Heterogeneous Routine Chest Computed Tomography. Eur. Radiol. Exp. 2020, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutierrez, G. Artificial Intelligence in the Intensive Care Unit. Crit. Care 2020, 24, 101. [Google Scholar] [CrossRef] [Green Version]
- Sahn, S.A.; Heffner, J.E. Spontaneous Pneumothorax. N. Engl. J. Med. 2000, 342, 868–874. [Google Scholar] [CrossRef] [Green Version]
- Hoi, K.; Turchin, B.; Kelly, A.M. How Accurate Is the Light Index for Estimating Pneumothorax Size? Australas. Radiol. 2007, 51, 196–198. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | Value |
|---|---|
| No. of patients | 96 |
| Age | 32.85 ± 14.57 |
| Sex | |
| Male | 77 (80.2%) |
| Female | 19 (19.8%) |
| Manufacturers | |
| Philips Medical Systems | 50 (52.1%) |
| GE Healthcare | 31 (32.3%) |
| DongKang | 10 (10.4%) |
| FUJIFILM Corporation | 3 (3.1%) |
| Samsung Electronics | 2 (2.1%) |
| Thoracostomy before chest CT | |
| Yes (training set) | 67 (69.8%) |
| No (test set) | 29 (30.2%) |
| Class | Accuracy | Sensitivity | Specificity | PPV | NPV | DSC |
|---|---|---|---|---|---|---|
| Background | 97.23 | 99.23 | 89.64 | 97.32 | 96.85 | 98.26 |
| Lung | 96.15 | 83.57 | 98.97 | 94.78 | 96.41 | 88.83 |
| Pneumothorax | 97.81 | 69.18 | 98.56 | 55.92 | 99.18 | 61.84 |
| Variables | Ratio of Pneumothorax | MAE Compared to CT |
|---|---|---|
| Gold standard (CT) | 14.85 ± 15.25 | - |
| True label (chest radiograph) | 12.68 ± 8.7 | 5.41 |
| Predicted label (calculated by AI) | 16.38 ± 6.45 | 8.45 |
| Variables | Shapiro–Wilk Test | Wilcoxon Signed-Rank Test | ||
|---|---|---|---|---|
| Statistics | p-Value | Statistics (W) (p-Value *) | ||
| Gold standard | 0.7221 | <0.05 | 144 (0.11) | - |
| Predicted label | 0.7935 | <0.05 | 98 (<0.05) | |
| True label | 0.8299 | <0.05 | - | |
| Variables | Thoracostomy | Other Treatments |
|---|---|---|
| Gold standard | 30.0 ±22.5/Median: 28.8 | 10.0 ± 7.9/Median: 8.0 |
| True label | 18.5 ± 11.9/Median: 14.8 | 10.8 ± 6.6/Median 8.4 |
| Predicted label | 21.6 ± 9.7/Median 19.2 | 14.7 ± 4.1/Median 13.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Lee, J.-H.; Kim, S.-W.; Hong, J.-M.; Kim, S.-J.; Song, M.; Choi, J.-M.; Lee, S.-Y.; Yoon, H.; Yoo, J.-Y. Quantitative Measurement of Pneumothorax Using Artificial Intelligence Management Model and Clinical Application. Diagnostics 2022, 12, 1823. https://doi.org/10.3390/diagnostics12081823
Kim D, Lee J-H, Kim S-W, Hong J-M, Kim S-J, Song M, Choi J-M, Lee S-Y, Yoon H, Yoo J-Y. Quantitative Measurement of Pneumothorax Using Artificial Intelligence Management Model and Clinical Application. Diagnostics. 2022; 12(8):1823. https://doi.org/10.3390/diagnostics12081823
Chicago/Turabian StyleKim, Dohun, Jae-Hyeok Lee, Si-Wook Kim, Jong-Myeon Hong, Sung-Jin Kim, Minji Song, Jong-Mun Choi, Sun-Yeop Lee, Hongjun Yoon, and Jin-Young Yoo. 2022. "Quantitative Measurement of Pneumothorax Using Artificial Intelligence Management Model and Clinical Application" Diagnostics 12, no. 8: 1823. https://doi.org/10.3390/diagnostics12081823
APA StyleKim, D., Lee, J.-H., Kim, S.-W., Hong, J.-M., Kim, S.-J., Song, M., Choi, J.-M., Lee, S.-Y., Yoon, H., & Yoo, J.-Y. (2022). Quantitative Measurement of Pneumothorax Using Artificial Intelligence Management Model and Clinical Application. Diagnostics, 12(8), 1823. https://doi.org/10.3390/diagnostics12081823