
Feasibility of Cell-Free DNA Measurement from the Earlobe during Physiological Exercise Testing

 , and
, and
Abstract
:1. Introduction
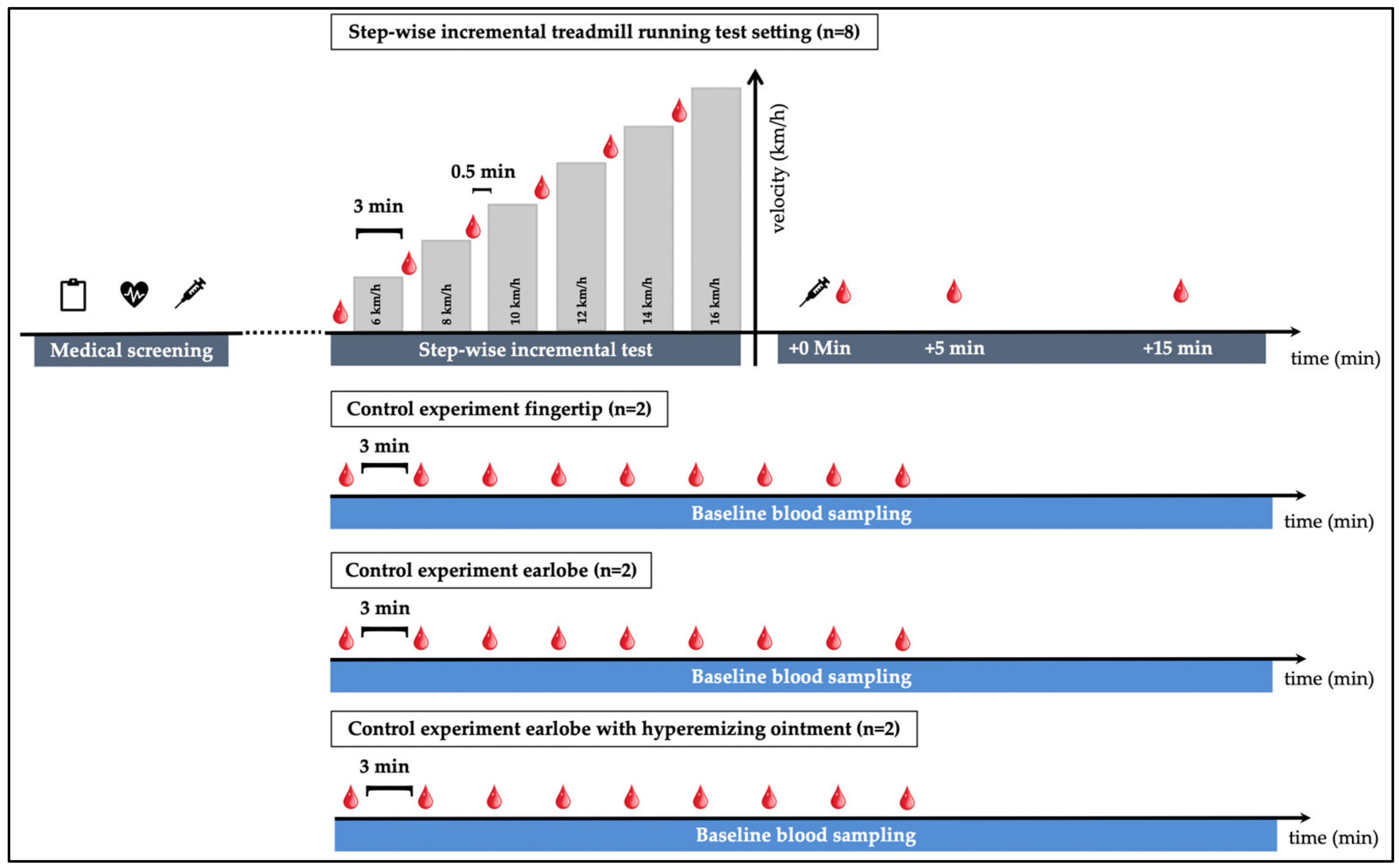
2. Materials and Methods
2.1. Ethical Approval
2.2. Subjects, Setting
2.3. Quantification of cfDNA and Lactate
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
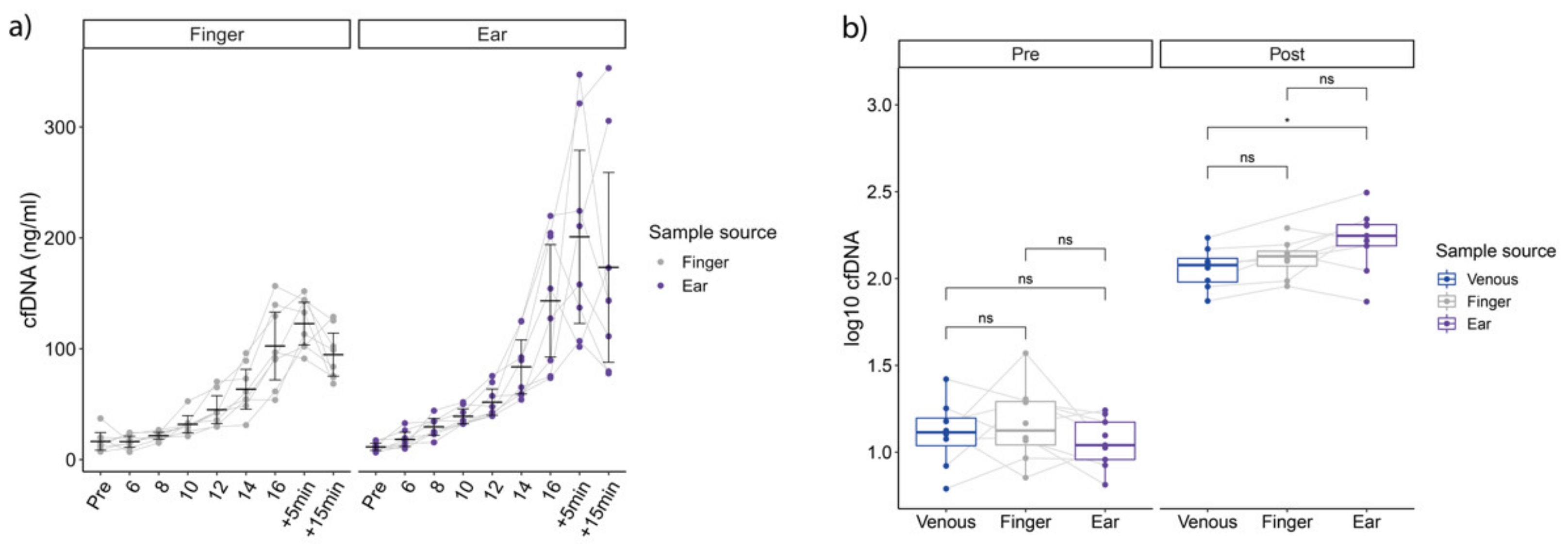
3.2. cfDNA during Exercise
3.3. cfDNA Kinetics at Rest
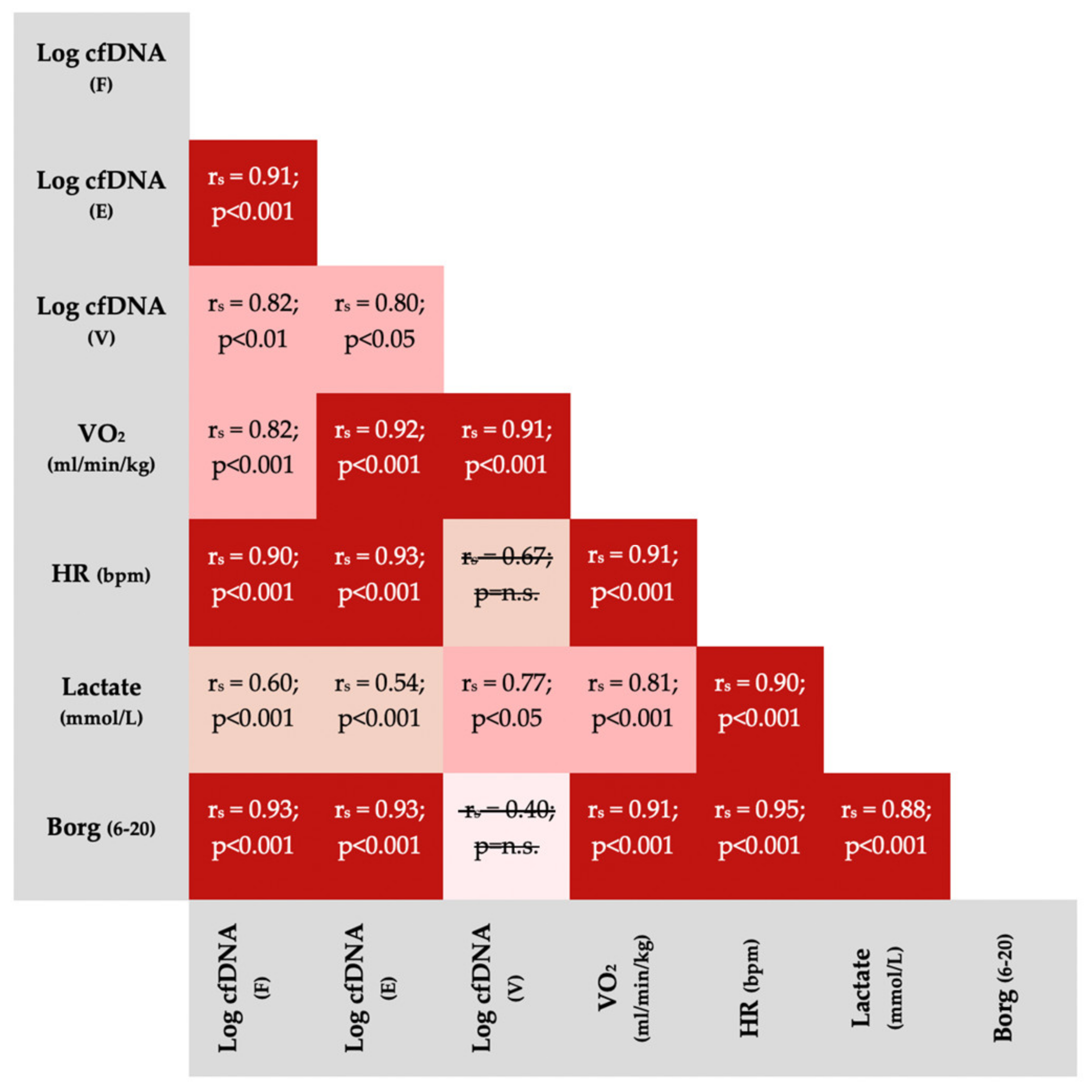
3.4. Correlations between Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mandel, P.; Metais, P. Nuclear Acids In Human Blood Plasma. C. R. Seances Soc. Biol. Fil. 1948, 142, 241–243. [Google Scholar] [PubMed]
- Van der Vaart, M.; Pretorius, P.J. Circulating DNA. Its origin and fluctuation. Ann. N. Y. Acad. Sci. 2008, 1137, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Stroun, M.; Anker, P.; Lyautey, J.; Lederrey, C.; Maurice, P.A. Isolation and characterization of DNA from the plasma of cancer patients. Eur. J. Cancer Clin. Oncol. 1987, 23, 707–712. [Google Scholar] [CrossRef]
- Schwarzenbach, H.; Muller, V.; Milde-Langosch, K.; Steinbach, B.; Pantel, K. Evaluation of cell-free tumour DNA and RNA in patients with breast cancer and benign breast disease. Mol Biosyst. 2011, 7, 2848–2854. [Google Scholar] [CrossRef]
- Leon, S.A.; Shapiro, B.; Sklaroff, D.M.; Yaros, M.J. Free DNA in the serum of cancer patients and the effect of therapy. Cancer Res. 1977, 37, 646–650. [Google Scholar] [PubMed]
- Tan, E.M.; Schur, P.H.; Carr, R.I.; Kunkel, H.G. Deoxybonucleic acid (DNA) and antibodies to DNA in the serum of patients with systemic lupus erythematosus. J. Clin. Invest. 1966, 45, 1732–1740. [Google Scholar] [CrossRef]
- Rainer, T.H.; Wong, L.K.S.; Lam, W.; Yuen, E.; Lam, N.Y.L.; Metreweli, C.; Lo, Y.D. Prognostic use of circulating plasma nucleic acid concentrations in patients with acute stroke. Clin Chem. 2003, 49, 562–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, A.; Wort, S.J.; Thomas, H.; Collinson, P.; Bennett, E.D. Plasma DNA concentration as a predictor of mortality and sepsis in critically ill patients. Crit. Care 2006, 10, R60. [Google Scholar] [CrossRef] [Green Version]
- Van der Vaart, M.; Pretorius, P.J. The origin of circulating free DNA. Clin. Chem. 2007, 53, 2215. [Google Scholar] [CrossRef] [Green Version]
- Beiter, T.; Fragasso, A.; Hudemann, J.; Schild, M.; Steinacker, J.; Mooren, F.C.; Niess, A.M. Neutrophils release extracellular DNA traps in response to exercise. J. Appl. Physiol. 2014, 117, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Breitbach, S.; Tug, S.; Simon, P. Circulating cell-free DNA: An up-coming molecular marker in exercise physiology. Sports Med. 2012, 42, 565–586. [Google Scholar] [CrossRef] [PubMed]
- Haller, N.; Ehlert, T.; Schmidt, S.; Ochmann, D.; Sterzing, B.; Grus, F.; Simon, P. Circulating, Cell-free DNA for Monitoring Player Load in Professional Football. Int. J. Sports Physiol. Perform. 2018, 14, 718–726. [Google Scholar] [CrossRef] [PubMed]
- Beiter, T.; Fragasso, A.; Hartl, D.; Niess, A.M. Neutrophil Extracellular Traps: A Walk on the Wild Side of Exercise Immunology. Sports Med. 2014, 45, 625–640. [Google Scholar] [CrossRef]
- Neuberger, E.W.I.; Sontag, S.; Brahmer, A.; Philippi, K.F.A.; Radsak, M.P.; Wagner, W.; Simon, P. Physical activity specifically evokes release of cell-free DNA from granulocytes thereby affecting liquid biopsy. Clin. Epigenetics. 2022, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Haller, N.; Tug, S.; Breitbach, S.; Jorgensen, A.; Simon, P. Increases in Circulating, Cell-Free DNA During Aerobic Running Depend on Intensity and Duration. Int. J. Sports Physiol. Perform. 2016, 12, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Andreatta, M.V.; Curty, V.M.; Coutinho, J.V.S.; Santos, M.A.A.; Vassallo, P.F.; de Sousa, N.F.; Barauna, V.G. Cell-Free DNA as an Earlier Predictor of Exercise-Induced Performance Decrement Related to Muscle Damage. Int. J. Sports Physiol. Perform. 2018, 13, 953–956. [Google Scholar] [CrossRef]
- Haller, N.; Helmig, S.; Taenny, P.; Petry, J.; Schmidt, S.; Simon, P. Circulating, cell-free DNA as a marker for exercise load in intermittent sports. PLoS ONE. 2018, 13, e0191915. [Google Scholar] [CrossRef] [Green Version]
- Breitbach, S.; Sterzing, B.; Magallanes, C.; Tug, S.; Simon, P. Direct measurement of cell-free DNA from serially collected capillary plasma during incremental exercise. J. Appl. Physiol. 2014, 117, 119–130. [Google Scholar] [CrossRef] [Green Version]
- Forsyth, J.J.; Farrally, M.R. A comparison of lactate concentration in plasma collected from the toe, ear, and fingertip after a simulated rowing exercise. Br. J. Sports Med. 2000, 34, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Dickhuth, H.H.; Yin, L.; Niess, A.; Rocker, K.; Mayer, F.; Heitkamp, H.C.; Horstmann, T. Ventilatory, lactate-derived and catecholamine thresholds during incremental treadmill running: Relationship and reproducibility. Int. J. Sports Med. 1999, 20, 122–127. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, E.W.I.; Brahmer, A.; Ehlert, T.; Kluge, K.; Philippi, K.F.A.; Boedecker, S.C.; Boedecker, S.C.; Weinmann-Menke, J.; Simon, P. Validating quantitative PCR assays for cfDNA detection without DNA extraction in exercising SLE patients. Sci. Rep. 2021, 11, 13581. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Beiter, T.; Fragasso, A.; Hudemann, J.; Niess, A.M.; Simon, P. Short-term treadmill running as a model for studying cell-free DNA kinetics in vivo. Clin. Chem. 2011, 57, 633–636. [Google Scholar] [CrossRef] [Green Version]
- Aucamp, J.; Bronkhorst, A.J.; Badenhorst, C.P.S.; Pretorius, P.J. The diverse origins of circulating cell-free DNA in the human body: A critical re-evaluation of the literature. Biol. Rev. Camb. Philos. Soc. 2018, 93, 1649–1683. [Google Scholar] [CrossRef] [PubMed]
- Tug, S.; Helmig, S.; Deichmann, E.R.; Schmeier-Jurchott, A.; Wagner, E.; Zimmermann, T.; Radsak, M.; Giacca, M.; Simon, P. Exercise-induced increases in cell free DNA in human plasma originate predominantly from cells of the haematopoietic lineage. Exerc. Immunol. Rev. 2015, 21, 164–173. [Google Scholar]
- Yang, Z.W.; Yang, S.H.; Chen, L.; Qu, J.; Zhu, J.; Tang, Z. Comparison of blood counts in venous, fingertip and arterial blood and their measurement variation. Clin. Lab. Haematol. 2001, 23, 155–159. [Google Scholar] [CrossRef]
- Schalk, E.; Heim, M.U.; Koenigsmann, M.; Jentsch-Ullrich, K. Use of capillary blood count parameters in adults. Vox Sanguinis. 2007, 93, 348–353. [Google Scholar] [CrossRef]
- Daae, L.; Halvorsen, S.; Mathisen, P.; Mironska, K. A comparison between haematological parameters in ‘capillary’and venous blood from healthy adults. Scand. J. Clin. and Lab. Investig. 1988, 48, 723–726. [Google Scholar]
- Goggs, R.; Jeffery, U.; LeVine, D.N.; Li, R.H.L. Neutrophil-Extracellular Traps, Cell-Free DNA, and Immunothrombosis in Companion Animals: A Review. Vet. Pathol. 2020, 57, 6–23. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, J.; Kirsner, R. Pathophysiology of acute wound healing. Clin. Dermatol. 2007, 25, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Canedo-Dorantes, L.; Canedo-Ayala, M. Skin Acute Wound Healing: A Comprehensive Review. Int. J. Inflamm. 2019, 2019, 370631. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, T.V.; Reinert, T.; Christensen, E.; Sethi, H.; Birkenkamp-Demtroder, K.; Gogenur, M.; Zimmermann, B.G.; Dyrskjot, L.; Andersen, C.L. The effect of surgical trauma on circulating free DNA levels in cancer patients-implications for studies of circulating tumor DNA. Mol. Oncol. 2020, 14, 1670–1679. [Google Scholar] [CrossRef]
- Konishi, S.; Narita, T.; Hatakeyama, S.; Yoneyama, T.; Yoneyama, M.S.; Tobisawa, Y.; Noro, D.; Sato, T.; Togashi, K.; Okamoto, T.; et al. Utility of total cell-free DNA levels for surgical damage evaluation in patients with urological surgeries. Sci. Rep. 2021, 11, 22103. [Google Scholar] [CrossRef]
- Meites, S.; Levitt, M. Skin-puncture and blood-collecting techniques for infants. Clin. Chem. 1979, 25, 183–189. [Google Scholar] [CrossRef]
- Nishimura, F.; Uno, N.; Chiang, P.C.; Kaku, N.; Morinaga, Y.; Hasegawa, H.; Yanagihara, K. The Effect of In Vitro Hemolysis on Measurement of Cell-Free DNA. J. Appl. Lab. Med. 2019, 4, 235–240. [Google Scholar] [CrossRef]
- Skinner, J.S.; Mclellan, T.H. The Transition from Aerobic to Anaerobic Metabolism. Res. Q. Exerc. Sport 1980, 51, 234–248. [Google Scholar] [CrossRef]
- Jamnick, N.A.; Pettitt, R.W.; Granata, C.; Pyne, D.B.; Bishop, D.J. An Examination and Critique of Current Methods to Determine Exercise Intensity. Sports Med. 2020, 50, 1729–1756. [Google Scholar] [CrossRef]
- Farrell, P.A.; Wilmore, J.H.; Coyle, E.F.; Billing, J.E.; Costill, D.L. Plasma lactate accumulation and distance running performance. Med. Sci. Sports 1979, 11, 338–344. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All Tests (n = 8) | Test (n = 5) | Retest (n = 3) | Control Experiment (n = 6) |
|---|---|---|---|---|
| Anthropometric variables | ||||
| Age (yrs.) | 28 (2) | 28 (2) | 28 (1) | 31 (13.3) |
| Body weight (kg) | 78.1 (4.3) | 80.5 (1.9) | 76.7 (4.7) | 84.2 (6.0) |
| Body height (cm) | 185.6 (3.1) | 186.1 (3.2) | 185.3 (2.9) | 181.3 (10.9) |
| Body mass index (kg/m2) | 23.5 (2.4) | 23.7 | 23.6 (3.1) | 26 (4.2) |
| Physiological variables | ||||
| lactate threshold (km/h) | 12.3 (1.1) | 12.3 (1.2) | 12.5 (0.8) | |
| lactate at baseline (mmol/L) | 1.2 (0.4) | 1.1 (0.5) | 1.4 (0.4) | |
| lactate maximum in incremental test (mmol/L) | 11.3 (2.6) | 10.8 (3.1) | 12.1 (1.6) | |
| heart rate at start of incremental test (beats/min) | 72 (11) | 71 (11) | 75 (14) | |
| heart rate maximum in incremental test (beats/min) | 188 (6) | 188 (6) | 189 (8) | |
| cfDNA venous before incremental test (ng/mL) | 12.2 (3.9) | 10.8 (4.2) | 14.2 (3.2) | |
| cfDNA venous after incremental test (ng/mL) * | 110.6 (25) | 96.7 (21.4) | 119.5 (5.9) | |
| cfDNA venous mean fold-change (post to pre) | 9.6 (2.1) | 9.8 (2.8) | 9.7 (0.9) | |
| cfDNA finger before incremental test (ng/mL) | 16.4 (9.5) | 14.1 (5.9) | 20.3 (14.6) | |
| cfDNA finger after incremental test (ng/mL) | 134.2 (33.2) | 129. 6 (41.9) | 141.8 (13.7) | |
| cfDNA finger mean fold-change (post to pre) | 10.1 (4.7) | 10.5 (5.1) | 9.3 (4.9) | |
| cfDNA earlobe before incremental test (ng/mL) | 11.5 (3.9) | 13.2 (3.7) | 8.6 (2.2) | |
| cfDNA earlobe after incremental test (ng/mL) | 163.2 (49.8) | 167.3 (56.5) | 156.5 (46.8) | |
| cfDNA earlobe mean fold change (post to pre) | 15.3 (6.3) | 12.8 (4.1) | 19.4 (8) | |
| Borg scale at exhaustion | 19.6 (0.6) | 19.6 (0.5) | 19.6 (0.6) | |
| Maximal oxygen consumption (VO2max) ** | 51.8 (6.5) | 50.7 (7.4) | 54.5 (3.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haller, N.; Tomaskovic, A.; Stöggl, T.; Simon, P.; Neuberger, E. Feasibility of Cell-Free DNA Measurement from the Earlobe during Physiological Exercise Testing. Diagnostics 2022, 12, 1379. https://doi.org/10.3390/diagnostics12061379
Haller N, Tomaskovic A, Stöggl T, Simon P, Neuberger E. Feasibility of Cell-Free DNA Measurement from the Earlobe during Physiological Exercise Testing. Diagnostics. 2022; 12(6):1379. https://doi.org/10.3390/diagnostics12061379
Chicago/Turabian StyleHaller, Nils, Aleksandar Tomaskovic, Thomas Stöggl, Perikles Simon, and Elmo Neuberger. 2022. "Feasibility of Cell-Free DNA Measurement from the Earlobe during Physiological Exercise Testing" Diagnostics 12, no. 6: 1379. https://doi.org/10.3390/diagnostics12061379
APA StyleHaller, N., Tomaskovic, A., Stöggl, T., Simon, P., & Neuberger, E. (2022). Feasibility of Cell-Free DNA Measurement from the Earlobe during Physiological Exercise Testing. Diagnostics, 12(6), 1379. https://doi.org/10.3390/diagnostics12061379