
Ultrasound-Guided Trans-Uterine Cavity Core Needle Biopsy of Uterine Myometrial Tumors to Differentiate Sarcoma from a Benign Lesion—Description of the Method and Review of the Literature




Abstract
:1. Introduction
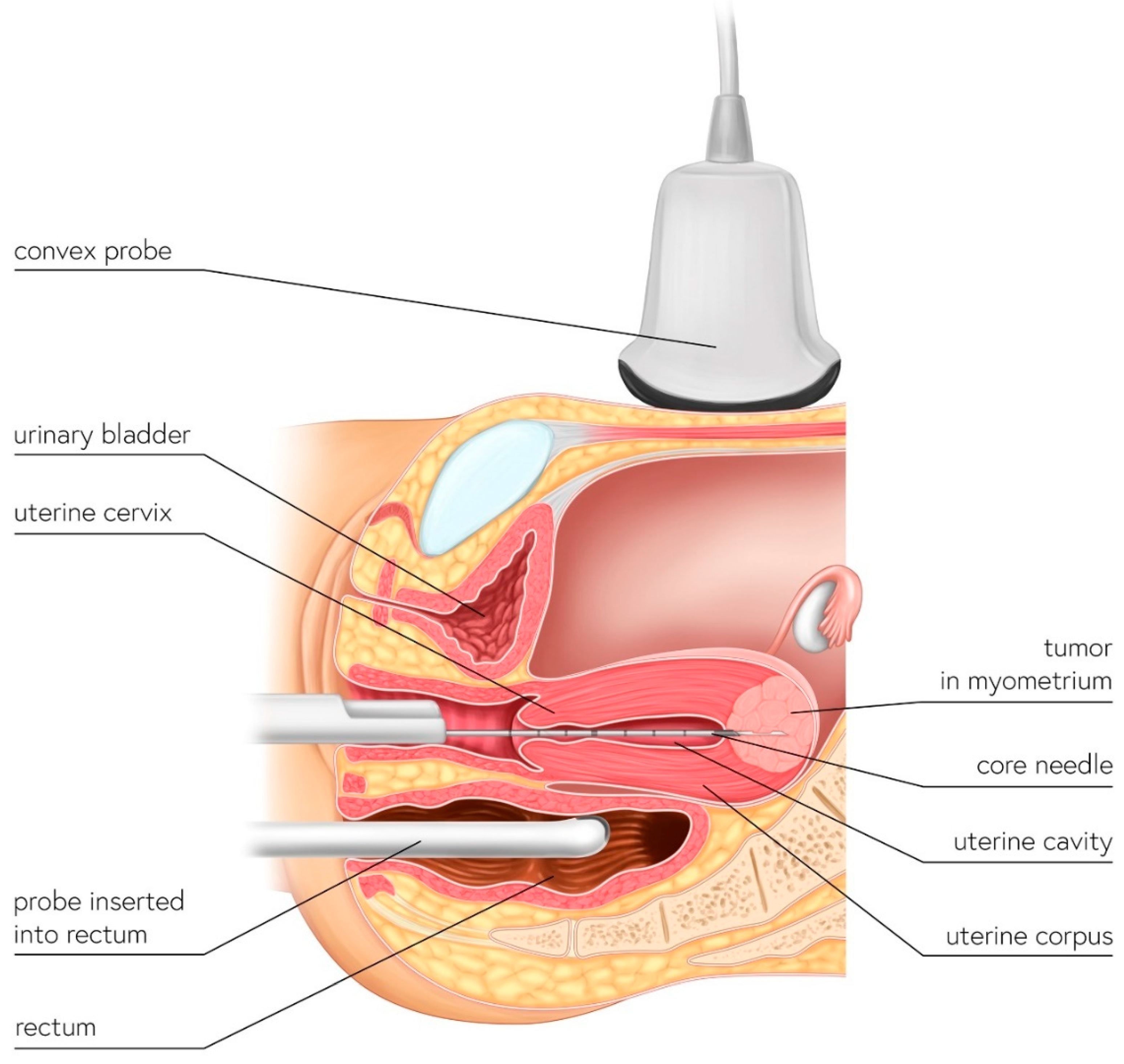
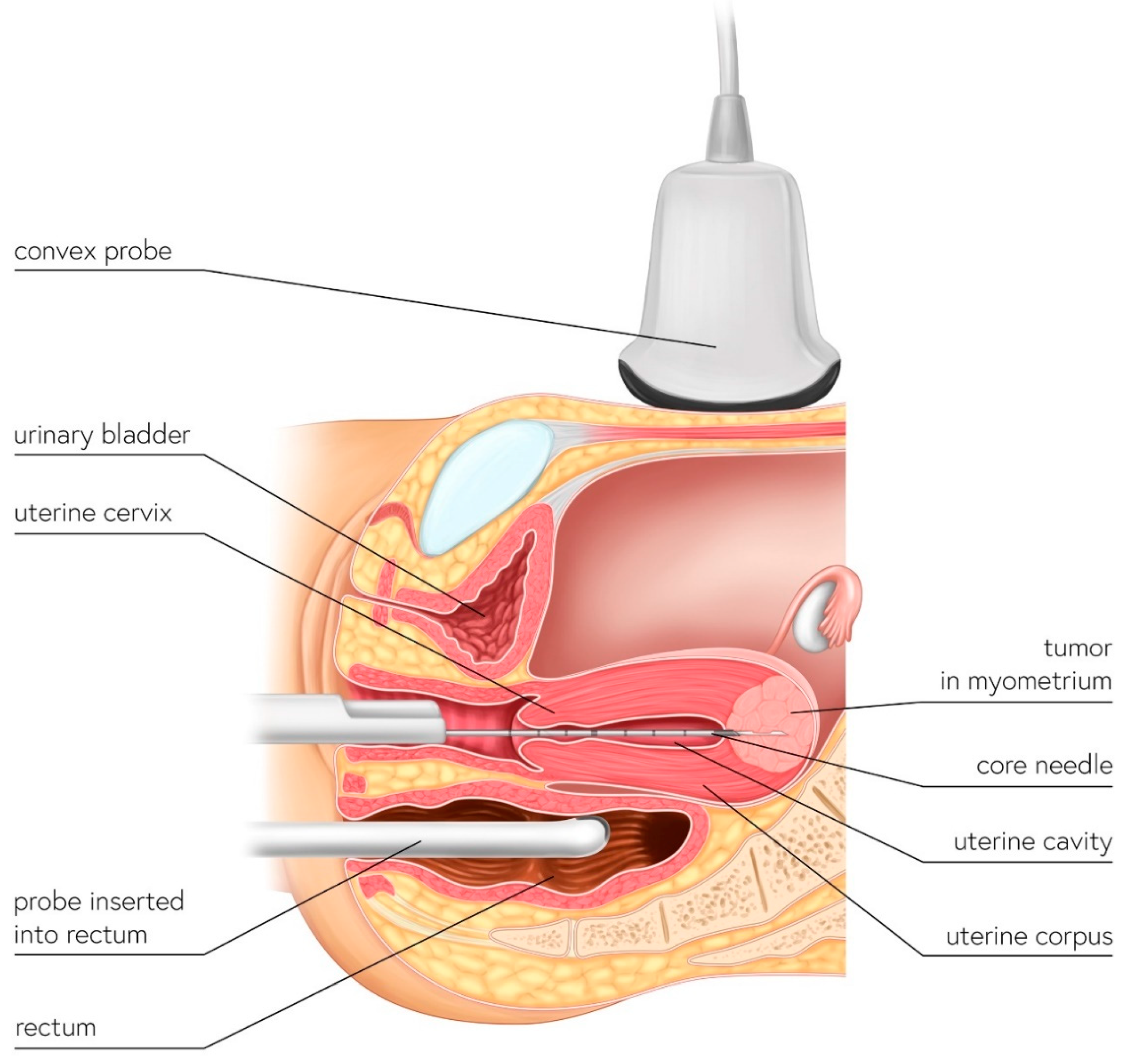
2. The UG-TUC Core Needle Biopsy Technique
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number (Age, Years Old) | Ultrasound Diagnosis of Uterine Lesion | Figure | Initial Treatment/ Histological Diagnosis Required (Doctor’s Decision) | Initial Patient’s Willingness to Undergo Surgery for the Uterine Lesion | Histology from Core Needle Biopsy | Patient Decision to Undergo Surgery for the Uterine Lesion | Histology from Definitive Surgery | Did Core Needle Biopsy Provided Additional Information to Ultrasound | Did Core Needle Biopsy Provided Useful Information for the Clinical Management |
|---|---|---|---|---|---|---|---|---|---|
| 1 (44) | Typical uterine lesion (myoma) | Figure A1 | No | Yes | Leiomyoma, cellular variant (UG-TUC core needle biopsy) | Yes (lesion enlarged during follow-up) | Leiomyoma, cellular variant | No | Yes |
| 2 (36) | Sarcoma suspicion | Figure A2 | Yes | Tumorectomy, uterus preservation (young age) | LMS (UG-TUC core needle biopsy) | Yes | LMS | No | Yes |
| 3 (37) | Atypical uterine lesion | Figure A3 | Yes | No | Lipoleiomyoma (UG-TUC core needle biopsy) | No | - | Yes | Yes |
| 4 (56) | Atypical uterine lesion | Figure A4 | Yes | Yes | Leiomyoma (transvaginal ultrasound guided core needle biopsy) | Yes | Leiomyoma and adenomyosis | Yes | No |
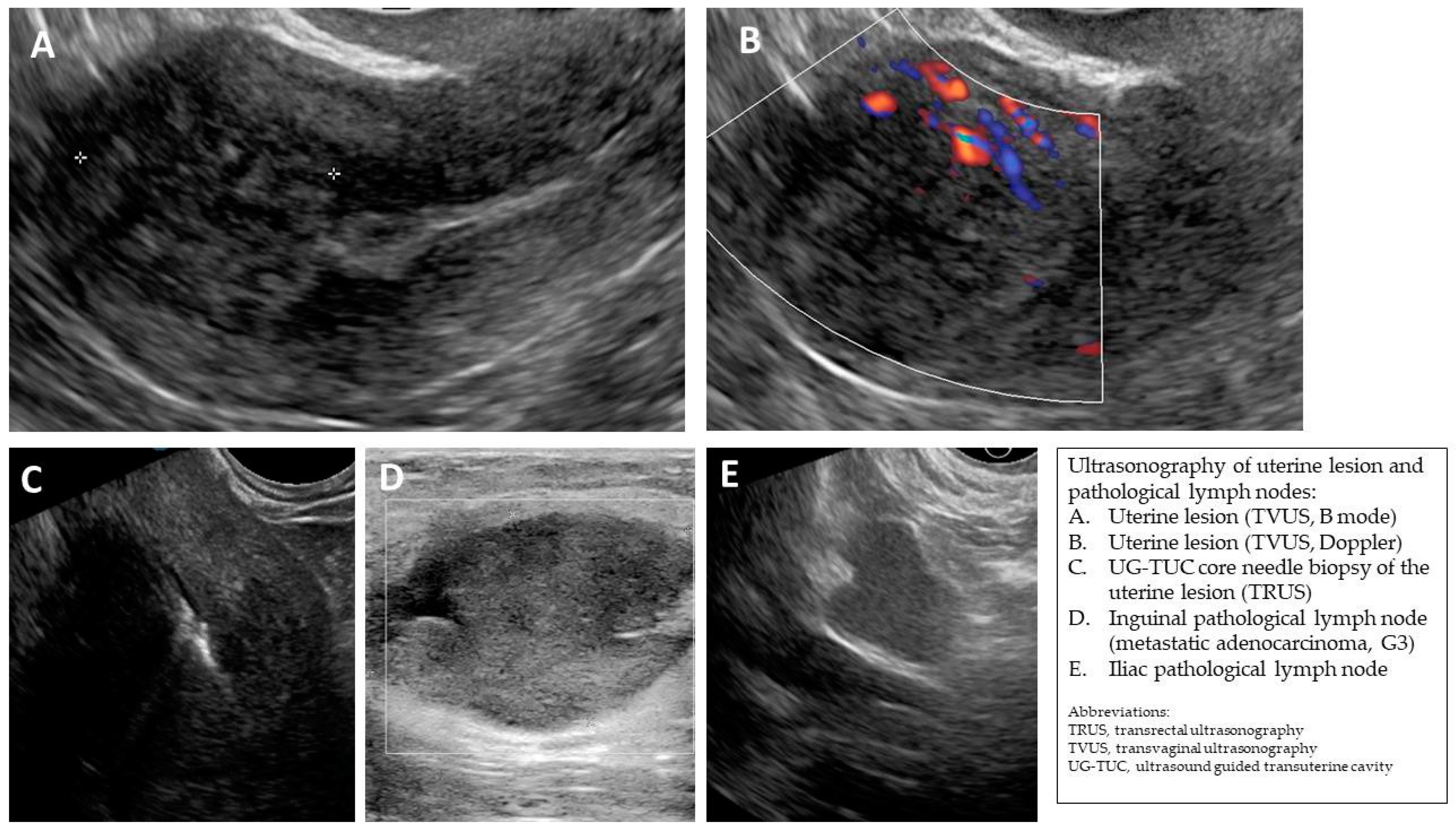
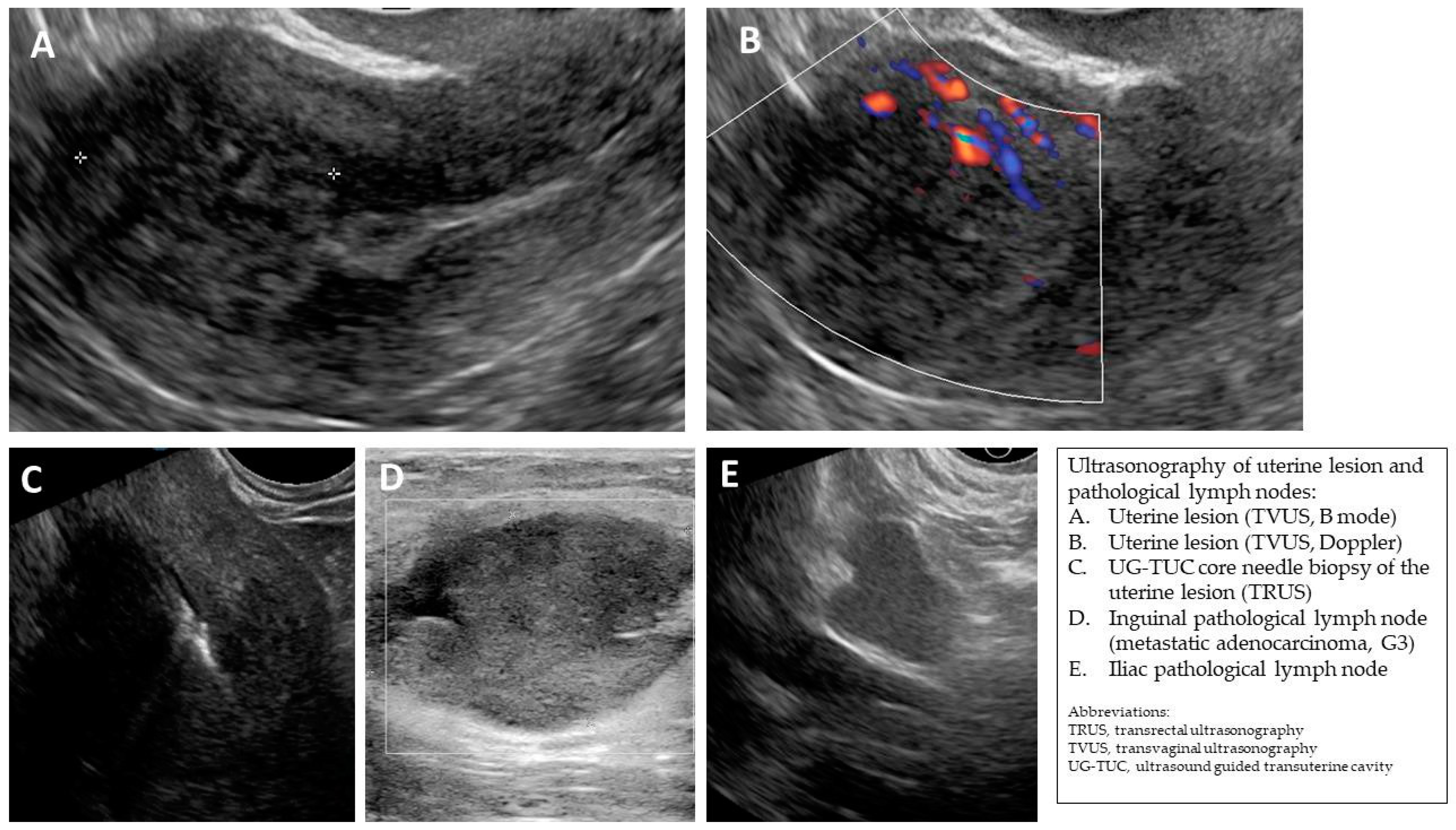
| 5 (50) | Atypical uterine lesion (metastatic adenocarcinoma G3 in inguinal lymph node) | Figure A5 | Yes | No | Leiomyoma (UG-TUC core needle biopsy) | No | Uterus / tumor not resected because primary urological carcinoma was diagnosed | Yes | Yes |
| 6 (38) | Atypical uterine lesion | Figure A6 | Yes | No | Leiomyoma, epithelioid variant (UG-TUC core needle biopsy) | Yes (lesion enlarged during follow-up) | Leiomyoma, epithelioid variant | Yes | Yes |
| 7 (29) | Atypical uterine lesion | Figure A7 | Yes | Yes | Leiomyoma (UG-TUC core needle biopsy) | Yes | Leiomyoma with signs of degenerations | Yes | Yes |
| 8 (52) | Atypical uterine lesion | Figure A8 | Yes | Yes | Total abdominal hysterectomy performed without core need biopsy, because of patients age and lesion ultrasound pattern recognition. Note: frozen section result: leiomyoma | Yes | STUMP | - | - |



References
- Bulun, S.E. Uterine Fibroids. N. Engl. J. Med. 2013, 369, 1344–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raspagliesi, F.; Maltese, G.; Bogani, G.; Fucà, G.; Lepori, S.; De Iaco, P.; Perrone, M.; Scambia, G.; Cormio, G.; Bogliolo, S.; et al. Morcellation worsens survival outcomes in patients with undiagnosed uterine leiomyosarcomas: A retrospective MITO group study. Gynecol. Oncol. 2016, 144, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Bretthauer, M.; Goderstad, J.M.; Løberg, M.; Emilsson, L.; Ye, W.; Adami, H.-O.; Kalager, M. Uterine morcellation and survival in uterine sarcomas. Eur. J. Cancer 2018, 101, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Kho, K.A.; Nezhat, C.H. Evaluating the Risks of Electric Uterine Morcellation. JAMA J. Am. Med. Assoc. 2014, 311, 905–906. [Google Scholar] [CrossRef]
- Halaska, M.J.; Haidopoulos, D.; Guyon, F.; Morice, P.; Zapardiel, I.; Kesic, V.; Council, E.S.G.O. European Society of Gynecological Oncology Statement on Fibroid and Uterine Morcellation. Int. J. Gynecol. Cancer 2017, 27, 189–192. [Google Scholar] [CrossRef]
- Gronchi, A.; Miah, A.B.; Dei Tos, A.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Blay, J.Y.; Bolle, S.; et al. Soft tissue and visceral sarcomas: ESMO–EURACAN–GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 32, 1348–1365. [Google Scholar] [CrossRef]
- Kubik-Huch, R.A.; Weston, M.; Nougaret, S.; Leonhardt, H.; Thomassin-Naggara, I.; Horta, M.; Cunha, T.M.; Maciel, C.; Rockall, A.; Forstner, R. European Society of Urogenital Radiology (ESUR) Guidelines: MR Imaging of Leiomyomas. Eur. Radiol. 2018, 28, 3125–3137. [Google Scholar] [CrossRef] [Green Version]
- Bonvalot, S.; Gronchi, A.; Hohenberger, P.; Litiere, S.; Pollock, R.; Raut, C.; Rutkowski, P.; Strauss, D.; Swallow, C.; Coevorden, F.; et al. Management of primary retroperitoneal sarcoma (RPS) in the adult: A consensus approach from the Trans-Atlantic RPS Working Group. Ann. Surg. Oncol. 2015, 22, 256–263. [Google Scholar] [CrossRef]
- Amant, F.; Van den Bosch, T.; Vergote, I.; Timmerman, D. Morcellation of uterine leiomyomas: A plea for patient triage. Lancet Oncol. 2015, 16, 1454–1456. [Google Scholar] [CrossRef]
- Zikan, M.; Fischerova, D.; Pinkavova, I.; Dundr, P.; Cibula, D. Ultrasound-guided tru-cut biopsy of abdominal and pelvic tumors in gynecology. Ultrasound Obstet. Gynecol. 2010, 36, 767–772. [Google Scholar] [CrossRef]
- Epstein, E.; Van Calster, B.; Timmerman, D.; Nikman, S. Subjective ultrasound assessment, the ADNEX model and ultrasound-guided tru-cut biopsy to differentiate disseminated primary ovarian cancer from metastatic non-ovarian cancer. Ultrasound Obstet. Gynecol. 2016, 47, 110–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.J.; Kim, C.K.; Park, B.K. Ultrasound-Guided Transvaginal Core Biopsy of Pelvic Masses: Feasibility, Safety, and Short-Term Follow-Up. Am. J. Roentgenol. 2016, 206, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Mascilini, F.; Quagliozzi, L.; Moro, F.; Moruzzi, M.C.; De Blasis, I.; Paris, V.; Scambia, G.; Fagotti, A.; Testa, A.C. Role of transvaginal ultrasound-guided biopsy in gynecology. Int. J. Gynecol. Cancer 2019, 30, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Van Houdt, W.; Schrijver, A.; Cohen-Hallaleh, R.; Memos, N.; Fotiadis, N.; Smith, M.; Hayes, A.; Van Coevorden, F.; Strauss, D. Needle tract seeding following core biopsies in retroperitoneal sarcoma. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 1740–1745. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Cliby, W.A.; Aletti, G.D. Impact of morcellation on survival outcomes of patients with unexpected uterine leiomyosarcoma: A systematic review and meta-analysis. Gynecol. Oncol. 2015, 137, 167–172. [Google Scholar] [CrossRef]
- George, S.; Ms, C.B.; Serrano, C.; Oduyebo, T.; Rauh-Hain, J.A.; Del Carmen, M.G.; Demetri, G.D.; Muto, M.G. Retrospective cohort study evaluating the impact of intraperitoneal morcellation on outcomes of localized uterine leiomyosarcoma. Cancer 2014, 120, 3154–3158. [Google Scholar] [CrossRef]
- Xu, X.; Lin, H.; Wright, J.D.; Gross, C.P.; Boscoe, F.P.; Hutchison, L.M.; Schwartz, P.E.; Desai, V.B. Association Between Power Morcellation and Mortality in Women With Unexpected Uterine Cancer Undergoing Hysterectomy or Myomectomy. J. Clin. Oncol. 2019, 37, 3412–3424. [Google Scholar] [CrossRef]
- Einstein, M.H.; Barakat, R.R.; Chi, D.S.; Sonoda, Y.; Alektiar, K.M.; Hensley, M.L.; Abu-Rustum, N.R. Management of uterine malignancy found incidentally after supracervical hysterectomy or uterine morcellation for presumed benign disease. Int. J. Gynecol. Cancer 2008, 18, 1065–1070. [Google Scholar] [CrossRef]
- Oduyebo, T.; Rauh-Hain, A.J.; Meserve, E.E.; Seidman, M.; Hinchcliff, E.; George, S.; Quade, B.; Nucci, M.R.; Del Carmen, M.G.; Muto, M.G. The value of re-exploration in patients with inadvertently morcellated uterine sarcoma. Gynecol. Oncol. 2014, 132, 360–365. [Google Scholar] [CrossRef]
- Yasukawa, M.; Dainty, L.A.; Sugarbaker, P.H. Long-term outcomes after cytoreductive surgery and HIPEC for morcellated uterine leiomyosarcoma; A case series. Gynecol. Oncol. Rep. 2021, 36, 100741. [Google Scholar] [CrossRef]
- Littell, R.D.; Tucker, L.-Y.; Raine-Bennett, T.; Palen, T.E.; Zaritsky, E.; Neugebauer, R.; Embry-Schubert, J.; Lentz, S.E. Adjuvant gemcitabine-docetaxel chemotherapy for stage I uterine leiomyosarcoma: Trends and survival outcomes. Gynecol. Oncol. 2017, 147, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Fucà, G.; Fabbroni, C.; Mancari, R.; Manglaviti, S.; Bogani, G.; Fumagalli, E.; Bertulli, R.; Morosi, C.; Collini, P.; Raspagliesi, F.; et al. Anthracycline-based and gemcitabine-based chemotherapy in the adjuvant setting for stage I uterine leiomyosarcoma: A retrospective analysis at two reference centers. Clin. Sarcoma Res. 2020, 10, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Haak, L.V.D.; van der Eijk, A.C.; Sandberg, E.M.; Frank, G.P.G.M.; Ansink, K.; Pelger, R.C.M.; de Kroon, C.D.; Jansen, F.W. Towards spill-free in-bag morcellation: A health failure mode and effects analysis. Surg. Endosc. 2018, 32, 4357–4362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szabó, I.; Szánthó, A.; Papp, Z. Uterine sarcoma: Diagnosis with multiparameter sonographic analysis. Ultrasound Obstet. Gynecol. 1997, 10, 220–221. [Google Scholar] [CrossRef] [PubMed]
- Amant, F.; Coosemans, A.; Debiec-Rychter, M.; Timmerman, D.; Vergote, I. Clinical management of uterine sarcomas. Lancet Oncol. 2009, 10, 1188–1198. [Google Scholar] [CrossRef]
- Cacciatore, B.; Lehtovirta, P.; Wahlström, T.; Ylöstalo, P. Ultrasound findings in uterine mixed mullerian sarcomas and endometrial stromal sarcomas. Gynecol. Oncol. 1989, 35, 290–293. [Google Scholar] [CrossRef]
- Ludovisi, M.; Moro, F.; Pasciuto, T.; Di Noi, S.; Giunchi, S.; Savelli, L.; Pascual, M.A.; Sladkevicius, P.; Alcazar, J.L.; Franchi, D.; et al. Imaging in gynecological disease (15): Clinical and ultrasound characteristics of uterine sarcoma. Ultrasound Obstet. Gynecol. 2019, 54, 676–687. [Google Scholar] [CrossRef]
- Lakhman, Y.; Veeraraghavan, H.; Chaim, J.; Feier, D.; Goldman, D.A.; Moskowitz, C.S.; Nougaret, S.; Sosa, R.E.; Vargas, H.A.; Soslow, R.A.; et al. Differentiation of Uterine Leiomyosarcoma from Atypical Leiomyoma: Diagnostic Accuracy of Qualitative MR Imaging Features and Feasibility of Texture Analysis. Eur. Radiol. 2016, 27, 2903–2915. [Google Scholar] [CrossRef]
- Sahdev, A.; Sohaib, S.A.; Jacobs, I.; Shepherd, J.H.; Oram, D.H.; Reznek, R.H. MR Imaging of Uterine Sarcomas. Am. J. Roentgenol. 2001, 177, 1307–1311. [Google Scholar] [CrossRef]
- Kido, A.; Togashi, K.; Koyama, T.; Yamaoka, T.; Fujiwara, T.; Fujii, S. Diffusely Enlarged Uterus: Evaluation with MR Imaging. RadioGraphics 2003, 23, 1423–1439. [Google Scholar] [CrossRef]
- Koyama, T.; Togashi, K.; Konishi, I.; Ueda, H.; Kataoka, M.L.; Kobayashi, H.; Itoh, T.; Higuchi, T.; Fujii, S.; Konishi, J. MR imaging of endometrial stromal sarcoma: Correlation with pathologic findings. Am. J. Roentgenol. 1999, 173, 767–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goto, A.; Takeuchi, S.; Sugimura, K.; Maruo, T. Usefulness of Gd-DTPA contrast-enhanced dynamic MRI and serum determination of LDH and its isozymes in the differential diagnosis of leiomyosarcoma from degenerated leiomyoma of the uterus. Int. J. Gynecol. Cancer 2002, 12, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Kiyono, Y.; Tsujikawa, T.; Kurokawa, T.; Okazawa, H.; Kotsuji, F. Additional value of 16α-[18F]fluoro-17β-oestradiol PET for differential diagnosis between uterine sarcoma and leiomyoma in patients with positive or equivocal findings on [18F]fluorodeoxyglucose PET. Eur. J. Pediatr. 2011, 38, 1824–1831. [Google Scholar] [CrossRef] [PubMed]
- Sagae, S.; Yamashita, K.; Ishioka, S.; Nishioka, Y.; Terasawa, K.; Mori, M.; Yamashiro, K.; Kanemoto, T.; Kudo, R. Preoperative Diagnosis and Treatment Results in 106 Patients with Uterine Sarcoma in Hokkaido, Japan. Oncology 2004, 67, 33–39. [Google Scholar] [CrossRef]
- Kubo, T.; Furuta, T.; Johan, M.P.; Sakuda, T.; Ochi, M.; Adachi, N. A meta-analysis supports core needle biopsy by radiologists for better histological diagnosis in soft tissue and bone sarcomas. Medicine 2018, 97, e11567. [Google Scholar] [CrossRef]
- Almond, L.M.; Tirotta, F.; Tattersall, H.; Hodson, J.; Cascella, T.; Barisella, M.; Marchianò, A.; Greco, G.; Desai, A.; Ford, S.J.; et al. Diagnostic accuracy of percutaneous biopsy in retroperitoneal sarcoma. Br. J. Surg. 2019, 106, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Tulandi, T.; Ferenczy, A. Biopsy of Uterine Leiomyomata and Frozen Sections Before Laparoscopic Morcellation. J. Minim. Invasive Gynecol. 2014, 21, 963–966. [Google Scholar] [CrossRef]
- Croce, S.; Chibon, F. Molecular prognostication of uterine smooth muscle neoplasms: From CGH array to CINSARC signature and beyond. Genes, Chromosom. Cancer 2020, 60, 129–137. [Google Scholar] [CrossRef]
- Bosch, T.V.D.; Dueholm, M.; Leone, F.P.G.; Valentin, L.; Rasmussen, C.; Votino, A.; Van Schoubroeck, D.; Landolfo, C.; Installé, A.J.F.; Guerriero, S.; et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: A consensus opinion from the Morphological Uterus Sonographic Assessment (MUSA) group. Ultrasound Obstet. Gynecol. 2015, 46, 284–298. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stukan, M.; Rutkowski, P.; Smadja, J.; Bonvalot, S. Ultrasound-Guided Trans-Uterine Cavity Core Needle Biopsy of Uterine Myometrial Tumors to Differentiate Sarcoma from a Benign Lesion—Description of the Method and Review of the Literature. Diagnostics 2022, 12, 1348. https://doi.org/10.3390/diagnostics12061348
Stukan M, Rutkowski P, Smadja J, Bonvalot S. Ultrasound-Guided Trans-Uterine Cavity Core Needle Biopsy of Uterine Myometrial Tumors to Differentiate Sarcoma from a Benign Lesion—Description of the Method and Review of the Literature. Diagnostics. 2022; 12(6):1348. https://doi.org/10.3390/diagnostics12061348
Chicago/Turabian StyleStukan, Maciej, Piotr Rutkowski, Jeremy Smadja, and Sylvie Bonvalot. 2022. "Ultrasound-Guided Trans-Uterine Cavity Core Needle Biopsy of Uterine Myometrial Tumors to Differentiate Sarcoma from a Benign Lesion—Description of the Method and Review of the Literature" Diagnostics 12, no. 6: 1348. https://doi.org/10.3390/diagnostics12061348
APA StyleStukan, M., Rutkowski, P., Smadja, J., & Bonvalot, S. (2022). Ultrasound-Guided Trans-Uterine Cavity Core Needle Biopsy of Uterine Myometrial Tumors to Differentiate Sarcoma from a Benign Lesion—Description of the Method and Review of the Literature. Diagnostics, 12(6), 1348. https://doi.org/10.3390/diagnostics12061348
{kind=link}