
Alveolar Soft Part Sarcoma of the Uterus: Clinicopathological and Molecular Characteristics


Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Selection and Clinicopathological Data Collection
2.2. Immunohistochemical Staining
2.3. Special Staining
2.4. Nucleic Acid Extraction
2.5. NGS
3. Case Presentation
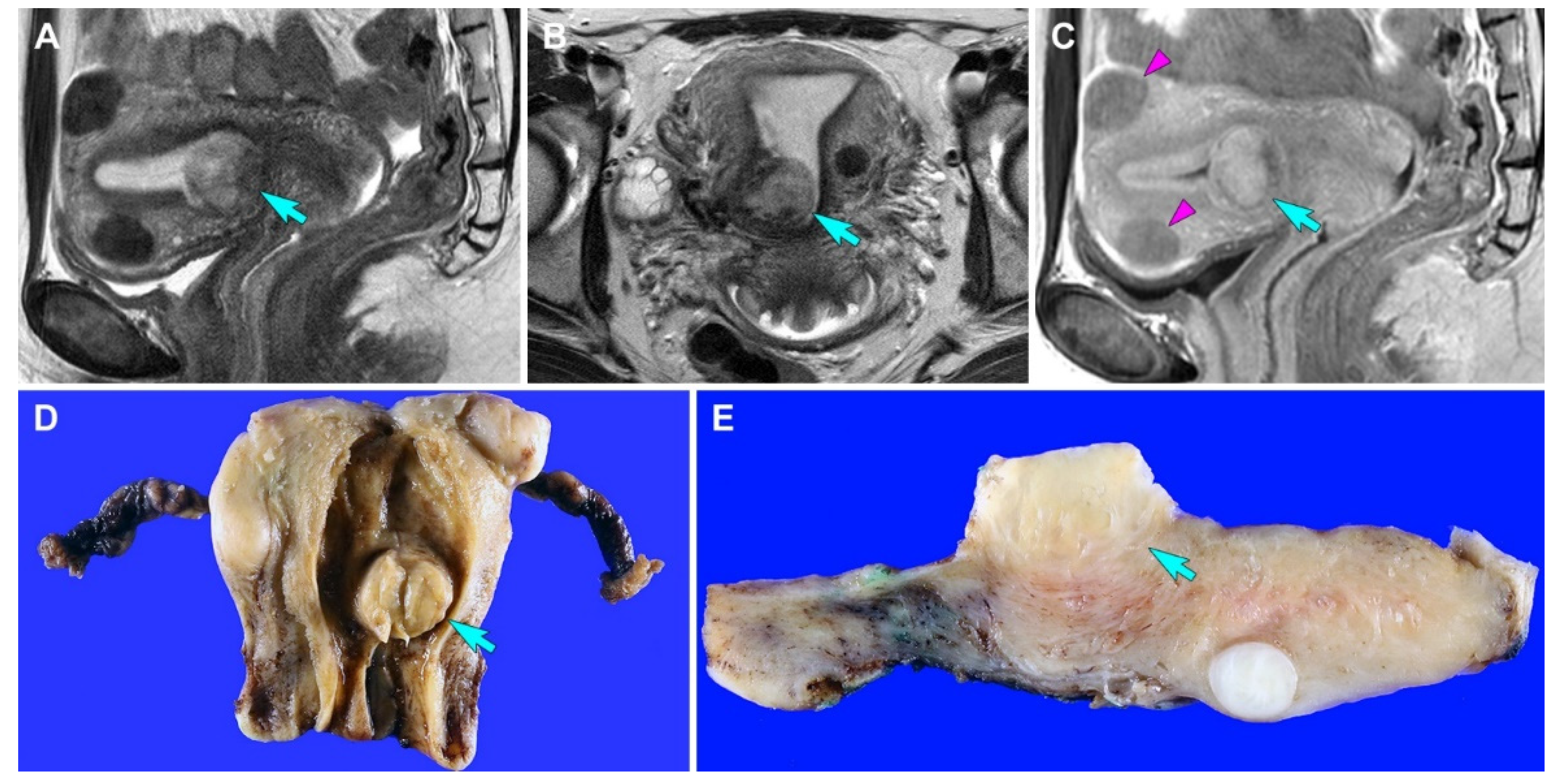
3.1. Case 1: Primary ASPS of the Uterine Corpus
3.1.1. Clinical Presentation
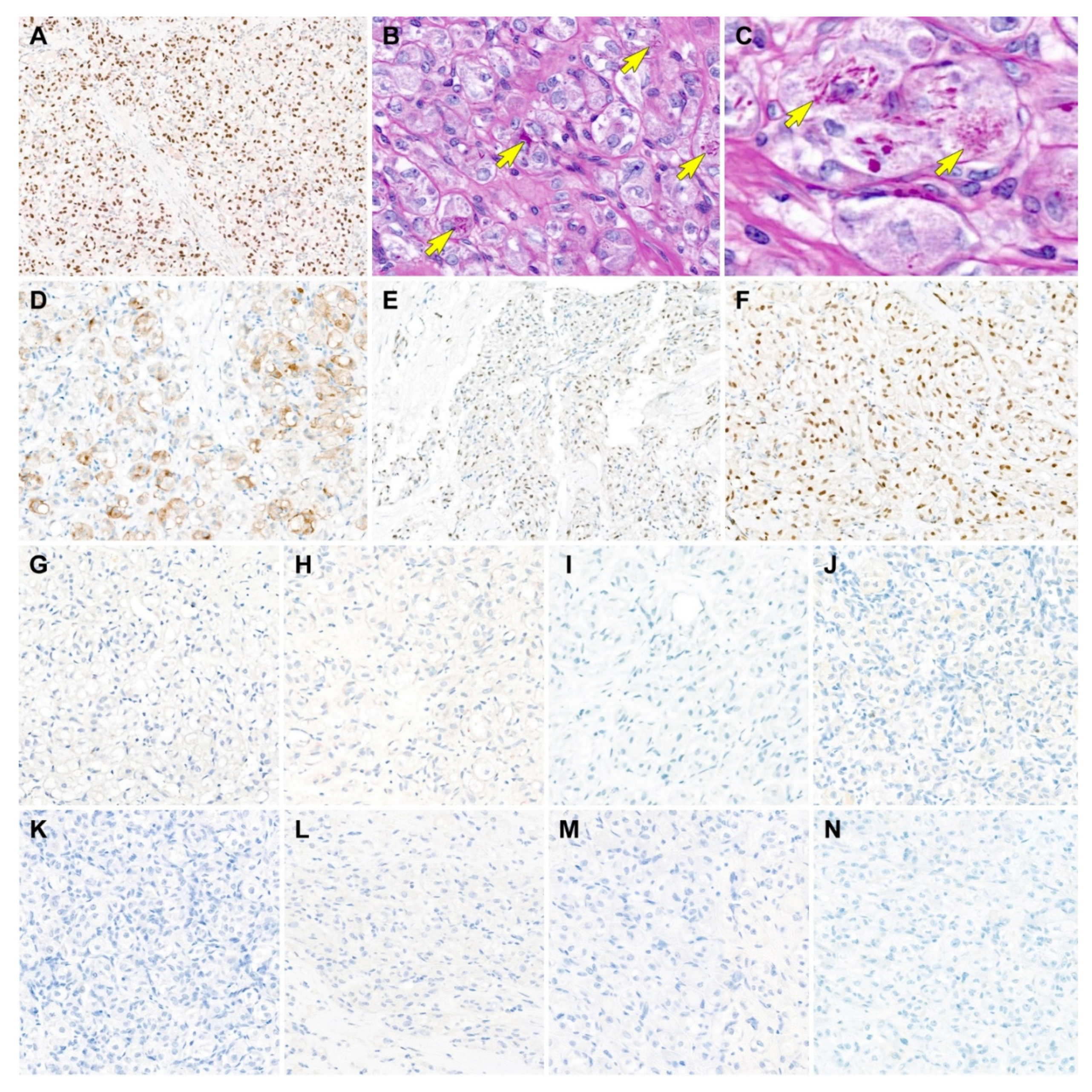
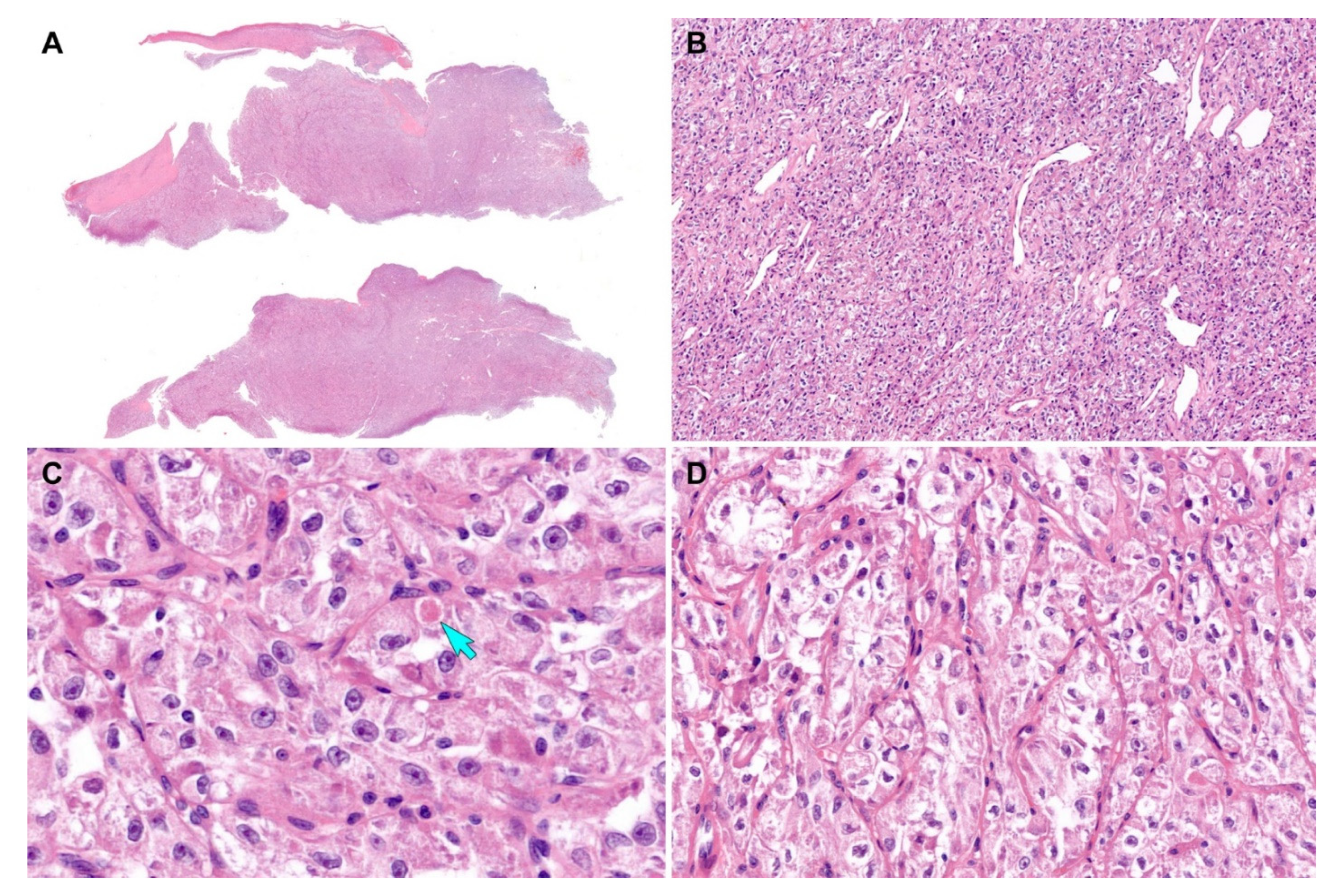
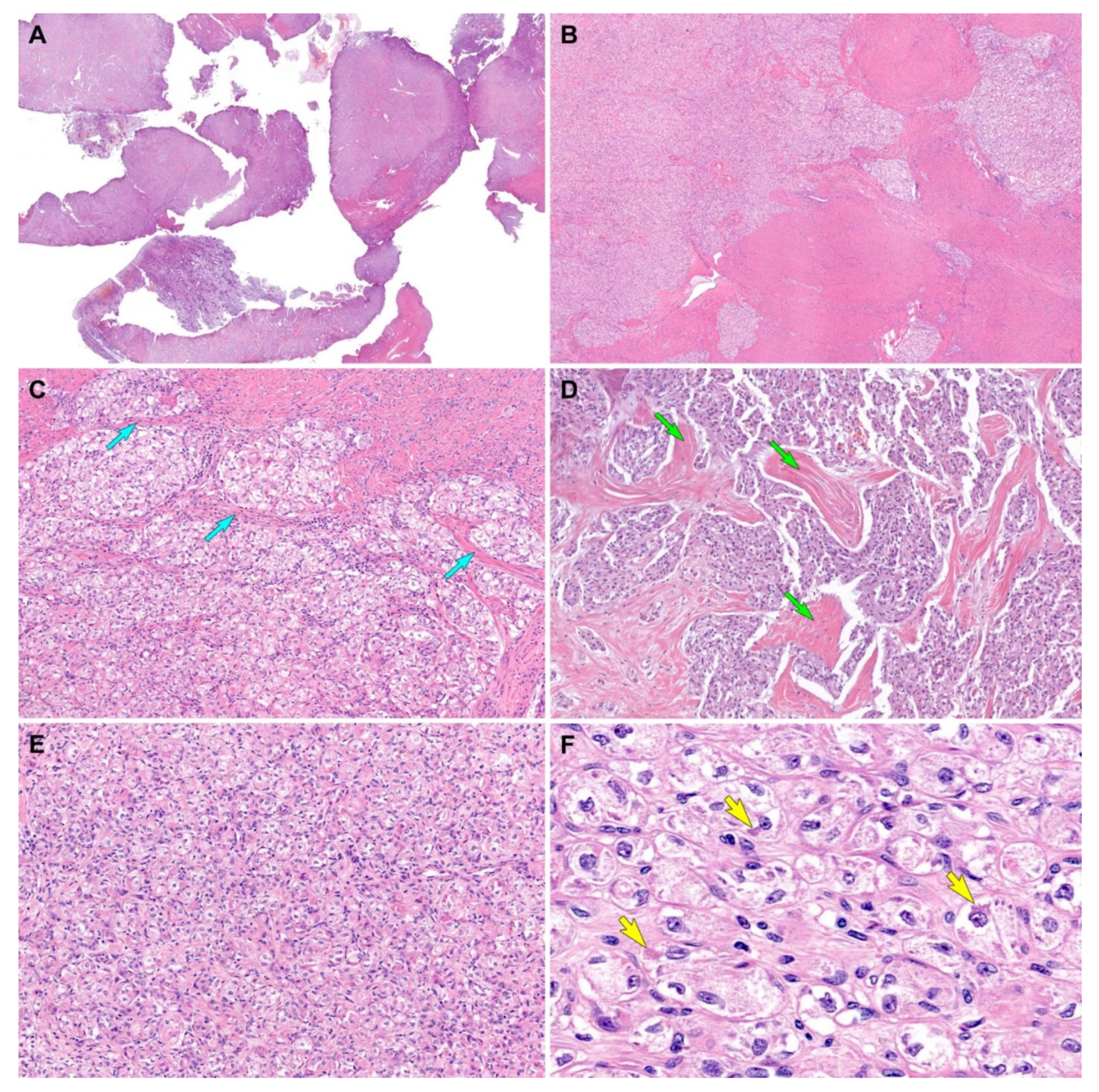
3.1.2. Pathological Findings
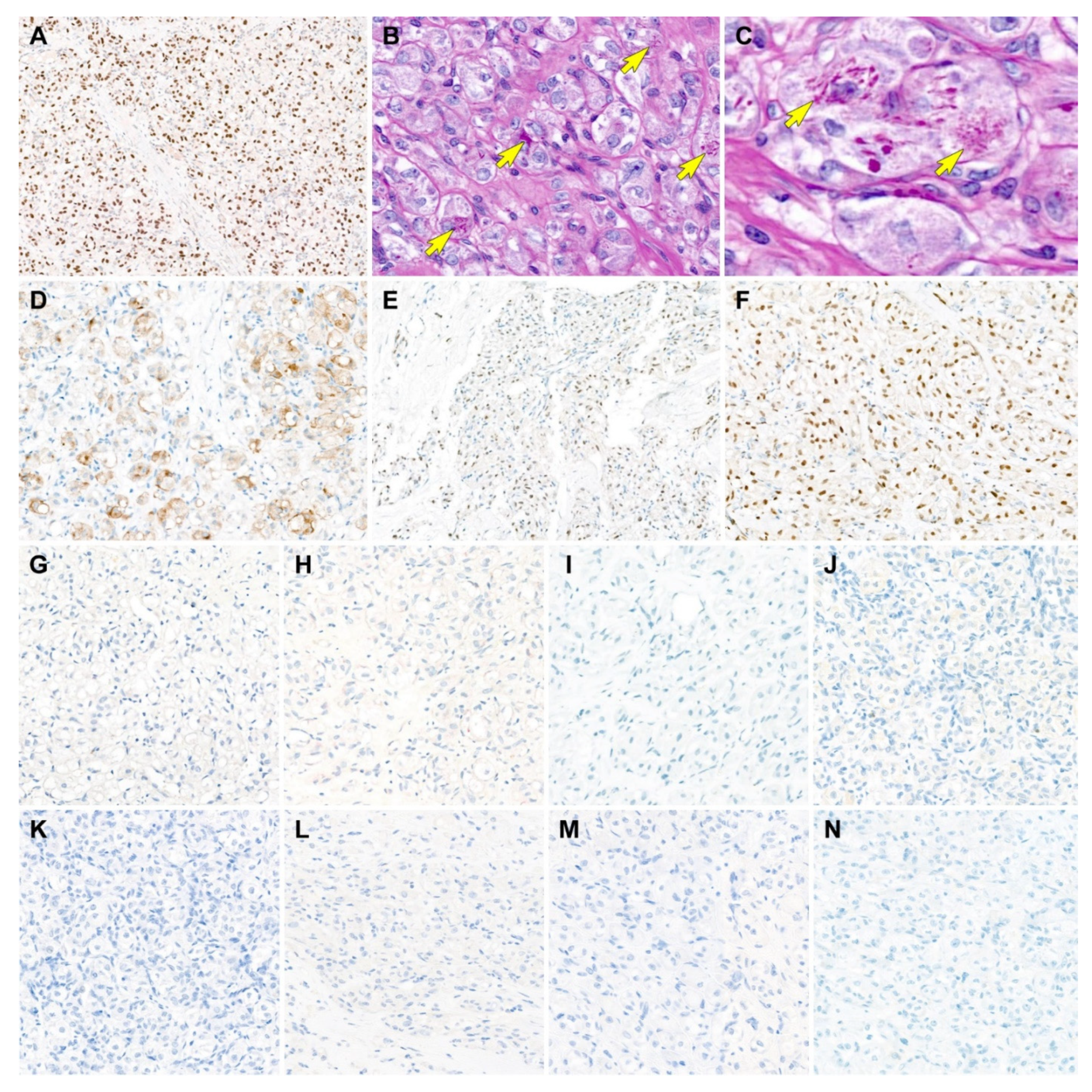
3.1.3. Results of Immunostaining and Special Staining
3.1.4. NGS Results
3.2. Case 2: Primary ASPS of the Uterine Cervix
3.2.1. Clinical Presentation
3.2.2. Pathological Findings
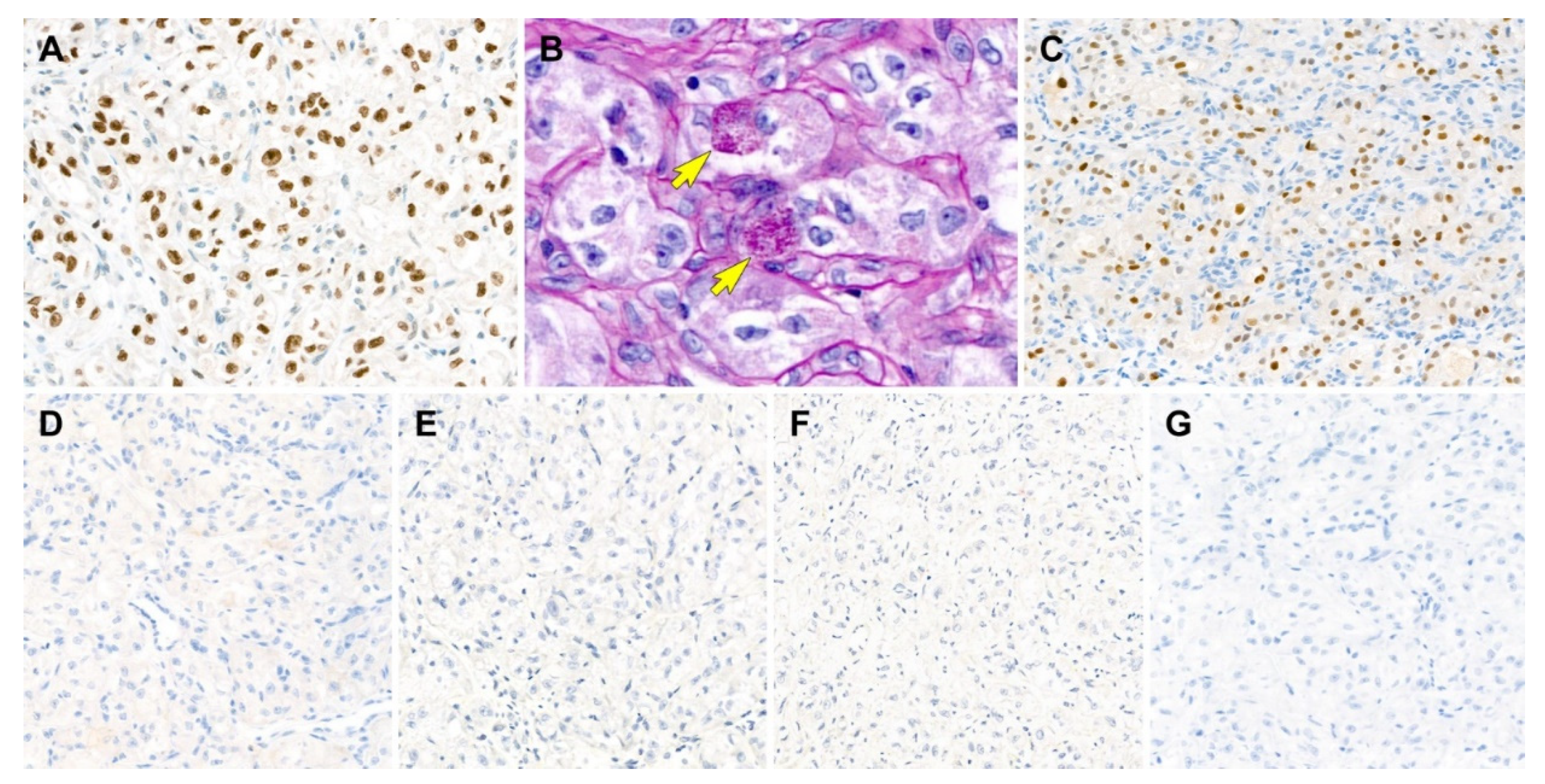
3.2.3. Results of Special Staining and Immunostaining
3.2.4. NGS Results
3.3. Post-Operative Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paoluzzi, L.; Maki, R.G. Diagnosis, prognosis, and treatment of alveolar soft-part sarcoma: A review. JAMA Oncol. 2019, 5, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Gomez, M.; Whiting, K.; Naous, R. Alveolar soft part sarcoma presenting as a uterine polyp: A case report. SAGE Open Med. Case Rep. 2020, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, X.; Li, Y.; Xue, X.; Zhou, H.; Hou, L. The current management of alveolar soft part sarcomas. Medicine 2021, 100, e26805. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Jacobson, A.; Harmon, D.C.; Choy, E.; Hornicek, F.J.; Raskin, K.A.; Chebib, I.A.; DeLaney, T.F.; Chen, Y.L. Prognostic factors in alveolar soft part sarcoma: A SEER analysis. J. Surg. Oncol. 2016, 113, 581–586. [Google Scholar] [CrossRef]
- Na, K.; Kim, H.S. Clinicopathologic and molecular characteristics of mesonephric adenocarcinoma arising from the uterine body. Am. J. Surg. Pathol. 2019, 43, 12–25. [Google Scholar] [CrossRef]
- Chang, S.; Hur, J.Y.; Choi, Y.L.; Lee, C.H.; Kim, W.S. Current status and future perspectives of liquid biopsy in non-small cell lung cancer. J. Pathol. Transl. Med. 2020, 54, 204–212. [Google Scholar] [CrossRef]
- Chang, S.; Shim, H.S.; Kim, T.J.; Choi, Y.L.; Kim, W.S.; Shin, D.H.; Kim, L.; Park, H.S.; Lee, G.K.; Lee, C.H.; et al. Molecular biomarker testing for non-small cell lung cancer: Consensus statement of the Korean Cardiopulmonary Pathology Study Group. J. Pathol. Transl. Med. 2021, 55, 181–191. [Google Scholar] [CrossRef]
- Choi, S.; Cho, J.; Lee, S.E.; Baek, C.H.; Kim, Y.K.; Kim, H.J.; Ko, Y.H. Adenocarcinoma of the minor salivary gland with concurrent MAML2 and EWSR1 alterations. J. Pathol. Transl. Med. 2021, 55, 132–138. [Google Scholar] [CrossRef]
- Jang, Y.; Jung, H.; Kim, H.N.; Seo, Y.; Alsharif, E.; Nam, S.J.; Kim, S.W.; Lee, J.E.; Park, Y.H.; Cho, E.Y.; et al. Clinicopathologic characteristics of HER2-positive pure mucinous carcinoma of the breast. J. Pathol. Transl. Med. 2020, 54, 95–102. [Google Scholar] [CrossRef]
- Lee, J.; Cho, Y.; Choi, K.H.; Hwang, I.; Oh, Y.L. Metastatic leiomyosarcoma of the thyroid gland: Cytologic findings and differential diagnosis. J. Pathol. Transl. Med. 2021, 55, 360–365. [Google Scholar] [CrossRef]
- Choi, S.; Joo, J.W.; Do, S.I.; Kim, H.S. Endometrium-limited metastasis of extragenital malignancies: A challenge in the diagnosis of endometrial curettage specimens. Diagnostics 2020, 10, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.; Jung, Y.Y.; Kim, H.S. Serous carcinoma of the endometrium with mesonephric-like differentiation initially misdiagnosed as uterine mesonephric-like adenocarcinoma: A case report with emphasis on the immunostaining and the identification of splice site TP53 mutation. Diagnostics 2021, 11, 717. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Kim, B.G.; Song, S.Y.; Kim, H.S. Ovarian gynandroblastoma with a juvenile granulosa cell tumor component in a postmenopausal woman. Diagnostics 2020, 10, 537. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Choi, S.; Do, S.I.; Lee, S.H.; Yoon, N.; Kim, H.S. Clinicopathological characteristics of pleomorphic high-grade squamous intraepithelial lesion of the uterine cervix: A single-institutional series of 31 cases. Diagnostics 2020, 10, 595. [Google Scholar] [CrossRef]
- Park, S.; Bae, G.E.; Kim, J.; Kim, H.S. Mesonephric-like differentiation of endometrial endometrioid carcinoma: Clinicopathological and molecular characteristics distinct from those of uterine mesonephric-like adenocarcinoma. Diagnostics 2021, 11, 1450. [Google Scholar] [CrossRef]
- Park, S.; Kim, H.S. Primary retroperitoneal mucinous carcinoma with carcinosarcomatous mural nodules: A case report with emphasis on its histological features and immunophenotype. Diagnostics 2020, 10, 580. [Google Scholar] [CrossRef]
- Kim, S.W.; Do, S.I.; Na, K. External validation of ALK and ROS1 fusions detected using an Oncomine Comprehensive Assay. Anticancer Res. 2021, 41, 4609–4617. [Google Scholar] [CrossRef]
- Kim, H.; Na, K.; Bae, G.E.; Kim, H.S. Mesonephric-like adenocarcinoma of the uterine corpus: Comprehensive immunohistochemical analyses using markers for mesonephric, endometrioid and serous tumors. Diagnostics 2021, 11, 2042. [Google Scholar] [CrossRef]
- Koh, H.H.; Park, E.; Kim, H.S. Mesonephric-like adenocarcinoma of the ovary: Clinicopathological and molecular characteristics. Diagnostics 2022, 12, 326. [Google Scholar] [CrossRef]
- Lee, H.; Kim, H.; Kim, H.S. Mesonephric adenocarcinoma of the vagina harboring TP53 mutation. Diagnostics 2022, 12, 119. [Google Scholar] [CrossRef]
- Lee, Y.; Choi, S.; Kim, H.S. Extraskeletal mesenchymal chondrosarcoma of the uterus. Diagnostics 2022, 12, 643. [Google Scholar] [CrossRef]
- Tsuji, K.; Ishikawa, Y.; Imamura, T. Technique for differentiating alveolar soft part sarcoma from other tumors in paraffin-embedded tissue: Comparison of immunohistochemistry for TFE3 and CD147 and of reverse transcription polymerase chain reaction for ASPSCR1-TFE3 fusion transcript. Hum. Pathol. 2012, 43, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Argani, P.; Lal, P.; Hutchinson, B.; Lui, M.Y.; Reuter, V.E.; Ladanyi, M. Aberrant nuclear immunoreactivity for TFE3 in neoplasms with TFE3 gene fusions: A sensitive and specific immunohistochemical assay. Am. J. Surg. Pathol. 2003, 27, 750–761. [Google Scholar] [CrossRef] [PubMed]
- Kasashima, S.; Minato, H.; Kobayashi, M.; Ueda, Y.; Oda, Y.; Hashimoto, S.; Inoue, M. Alveolar soft part sarcoma of the endometrium with expression of CD10 and hormone receptors. APMIS 2007, 115, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Vishwajeet, V.; Elhence, P.; Singh, P.; Ghuman, N.K. Alveolar soft part sarcoma of uterine corpus in a young female: A case report with review of literature. Int. J. Gynecol. Pathol. 2021, 40, 272–277. [Google Scholar] [CrossRef]
- Schoolmeester, J.K.; Carlson, J.; Keeney, G.L.; Fritchie, K.J.; Oliva, E.; Young, R.H.; Nucci, M.R. Alveolar soft part sarcoma of the female genital tract: A morphologic, immunohistochemical, and molecular cytogenetic study of 10 cases with emphasis on its distinction from morphologic mimics. Am. J. Surg. Pathol. 2017, 41, 622–632. [Google Scholar] [CrossRef]
- Ryu, A.; Mun, S.T.; Lee, H.J.; Kim, N.S. Recurrent alveolar soft part sarcoma of the uterine cervix. J. Obstet. Gynaecol. 2017, 37, 1099–1101. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, Y.; Liu, Y.; Liu, C. Alveolar soft part sarcoma of uterine cervix in a postmenopausal woman: A case report and review of literature. Int. J. Clin. Exp. Pathol. 2017, 10, 9812–9815. [Google Scholar]
- Zhang, L.L.; Tang, Q.; Wang, Z.; Zhang, X.S. Alveolar soft part sarcoma of the uterine corpus with pelvic lymph node metastasis: Case report and literature review. Int. J. Clin. Exp. Pathol. 2012, 5, 715–719. [Google Scholar]
- Roma, A.A.; Yang, B.; Senior, M.E.; Goldblum, J.R. TFE3 immunoreactivity in alveolar soft part sarcoma of the uterine cervix: Case report. Int. J. Gynecol. Pathol. 2005, 24, 131–135. [Google Scholar] [CrossRef]
- Williams, A.; Bartle, G.; Sumathi, V.P.; Meis, J.M.; Mangham, D.C.; Grimer, R.J.; Kindblom, L.G. Detection of ASPL/TFE3 fusion transcripts and the TFE3 antigen in formalin-fixed, paraffin-embedded tissue in a series of 18 cases of alveolar soft part sarcoma: Useful diagnostic tools in cases with unusual histological features. Virchows Arch. 2011, 458, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, K.; Ichikawa, R.; Ishii, R.; Oe, S.; Kato, R.; Kobayashi, Y.; Kuroda, M.; Udagawa, Y. A case of primary alveolar soft part sarcoma of the uterine cervix and a review of the literature. Int. J. Clin. Oncol. 2011, 16, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J. Alveolar soft part sarcoma of the uterine cervix: A case report and review of the literature. Korean J. Pathol. 2014, 48, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.; Jiang, W.; He, Y.; Li, L. Primary alveolar soft part sarcoma of the uterine cervix: A case report and literature review. Int. J. Clin. Exp. Pathol. 2014, 7, 8223–8226. [Google Scholar]
- Tsuda, M.; Davis, I.J.; Argani, P.; Shukla, N.; McGill, G.G.; Nagai, M.; Saito, T.; Lae, M.; Fisher, D.E.; Ladanyi, M. TFE3 fusions activate MET signaling by transcriptional up-regulation, defining another class of tumors as candidates for therapeutic MET inhibition. Cancer Res. 2007, 67, 919–929. [Google Scholar] [CrossRef] [Green Version]
- Jun, H.J.; Lee, J.; Lim, D.H.; Park, J.O.; Ahn, G.; Seo, S.W.; Sung, K.S.; Lim, D.H.; Yoo, K.H.; Choi, Y.L. Expression of MET in alveolar soft part sarcoma. Med. Oncol. 2010, 27, 459–465. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Clone | Company | Dilution |
|---|---|---|---|
| CD10 | 56C6 | Novocastra (Leica Biosystems, Buffalo Grove, IL, USA) | 1:100 |
| Pan-CK | AE1/AE3 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:500 |
| Desmin | D33 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:200 |
| ER | 6F11 | Novocastra (Leica Biosystems, Buffalo Grove, IL, USA) | 1:300 |
| PR | 16 | Novocastra (Leica Biosystems, Buffalo Grove, IL, USA) | 1:1200 |
| Ki-67 | MIB1 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:200 |
| HMB-45 | HMB45 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:80 |
| TFE3 | MRQ-37 | Cell Marque (Rocklin, CA, USA) | 1:20 |
| Melan-A | A103 | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:80 |
| Synaptophysin | DAKO-SYNAP | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:400 |
| S100 | Polyclonal | Dako (Agilent Technologies, Santa Clara, CA, USA) | 1:5000 |
| MET | SP44 | Ventana (Roche, Darmstadt, Germany) | Prediluted |
| Characteristic | Case 1 | Case 2 |
|---|---|---|
| Tumor location | Uterine corpus | Uterine cervix |
| Age at diagnosis | 27 years | 10 years |
| Presenting symptom | Vaginal bleeding | Vaginal bleeding |
| Initial clinical impression | Leiomyoma | Cervical mass |
| Primary treatment | Myomectomy | Mass excision |
| Definite treatment | TH, BS | TH |
| Hysterectomy diagnosis | 2.5 cm residual ASPS | No residual ASPS |
| Post-operative treatment | None | None |
| Disease-free survival | 2 months | 4 months |
| Gross appearance | Polypoid mass | Polypoid mass |
| Histological growth pattern | Mainly solid | Mainly solid |
| Myometrial or cervical stromal involvement | Superficial myometrium | NA |
| PAS-D | Rod-shaped crystalloids | Coarse granular materials |
| TFE3 (staining %) | Positive (100) | Positive (100) |
| ER (staining %) | Positive (30) | NA |
| PR (staining %) | Positive (90) | Positive (80) |
| CD10 (staining %) | Positive (70) | Negative (0) |
| HMB45 (staining %) | Negative (0) | Negative (0) |
| Melan-A (staining %) | Negative (0) | Negative (0) |
| Desmin (staining %) | Negative (0) | Negative (0) |
| S100 (staining %) | Negative (0) | Negative (0) |
| Pan-CK (staining %) | Negative (0) | Negative(0) |
| PAX8 (staining %) | Negative (0) | NA |
| Synaptophysin (staining %) | Negative (0) | NA |
| MET (staining %) | Negative (0) | NA |
| ASPSCR1–TFE3 fusion | Detected | Detected |
| No | Year Published | Authors | Age (Years) | Tumor Location | Tumor Size (cm) | Treatment | LN Metastasis | Follow-Up | DFS (Months) | Survival Status | Growth Pattern | TFE3 IHC | ASPSCR1–TFE3 Fusion |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2005 | Roma et al. [30] | 39 | Cervix | 0.2 | TH | NA | NA | Recent | Alive | Nested | + | NA |
| 2 | 2007 | Kasahima et al. [24] | 50 | Corpus | 1.9 | TH, BSO, PLND | Absent | NED | 38 | Alive | Nested | + | NA |
| 3 | 2011 | Williams et al. [31] | 31 | Cervix | 3.0 | Excision | NA | NED | 36 | Alive | NA | + | Detected |
| 4 | 2011 | Hasegawa et al. [32] | 56 | Cervix | 8.0 | TH, BSO | NA | NED | 66 | Alive | Nested | + | Detected |
| 5 | 2012 | Zhang et al. [29] | 57 | Corpus | 2.4 | TH, BSO, PLND | Present | NED | 9 | Alive | Nested | + | NA |
| 6 | 2014 | Lee [33] | 17 | Cervix | 1.6 | Wide excision | NA | Recurred | 40 | Alive | Nested | + | NA |
| 7 | 2014 | Feng et al. [34] | 21 | Cervix | 5.0 | TH, BSO, PLND | Absent | NED | 3 | Alive | Nested | + | Detected |
| 8 | 2017 | Schoolmeester et al. [26] | 37 | Cervix | 2.2 | TH, BSO, PLND | Absent | NED | 1 | Alive | Nested | + | Detected |
| 9 | 2017 | Schoolmeester et al. [26] | 45 | Cervix | 0.7 | TH | NA | NA | Recent | Alive | Nested | + | Detected |
| 10 | 2017 | Schoolmeester et al. [26] | 32 | Corpus | NA | TH, BSO | NA | NED | 8 | Alive | Nested | + | Detected |
| 11 | 2017 | Schoolmeester et al. [26] | 33 | Corpus | NA | NA | NA | NA | NA | NA | Solid | + | Detected |
| 12 | 2017 | Schoolmeester et al. [26] | 23 | Corpus | NA | Curettage | NA | NED | 9 | Alive | Nested | + | Detected |
| 13 | 2017 | Schoolmeester et al. [26] | 31 | Uterus | NA | TH | NA | NED | 35 | Alive | Solid | + | Detected |
| 14 | 2017 | Schoolmeester et al. [26] | 68 | Uterus | NA | TH | NA | NED | 15 | Alive | Nested | + | Detected |
| 15 | 2017 | Zhang et al. [28] | 68 | Cervix | 1.0 | RH | NA | NA | NA | Alive | Nested | + | NA |
| 16 | 2020 | Gomez et al. [2] | 20 | Corpus | 3.5 | TH | NA | NED | NA | Alive | Nested | + | Detected |
| 17 | 2021 | Vishwajeet et al. [25] | 24 | Corpus | 2.4 | Mass excision | NA | NED | NA | Alive | Nested | + | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Na, K.; Woo, H.Y.; Kim, H.-S. Alveolar Soft Part Sarcoma of the Uterus: Clinicopathological and Molecular Characteristics. Diagnostics 2022, 12, 1102. https://doi.org/10.3390/diagnostics12051102
Lee Y, Na K, Woo HY, Kim H-S. Alveolar Soft Part Sarcoma of the Uterus: Clinicopathological and Molecular Characteristics. Diagnostics. 2022; 12(5):1102. https://doi.org/10.3390/diagnostics12051102
Chicago/Turabian StyleLee, Yurimi, Kiyong Na, Ha Young Woo, and Hyun-Soo Kim. 2022. "Alveolar Soft Part Sarcoma of the Uterus: Clinicopathological and Molecular Characteristics" Diagnostics 12, no. 5: 1102. https://doi.org/10.3390/diagnostics12051102
APA StyleLee, Y., Na, K., Woo, H. Y., & Kim, H.-S. (2022). Alveolar Soft Part Sarcoma of the Uterus: Clinicopathological and Molecular Characteristics. Diagnostics, 12(5), 1102. https://doi.org/10.3390/diagnostics12051102