
Forrest Classification for Bleeding Peptic Ulcer: A New Look at the Old Endoscopic Classification

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Preparation
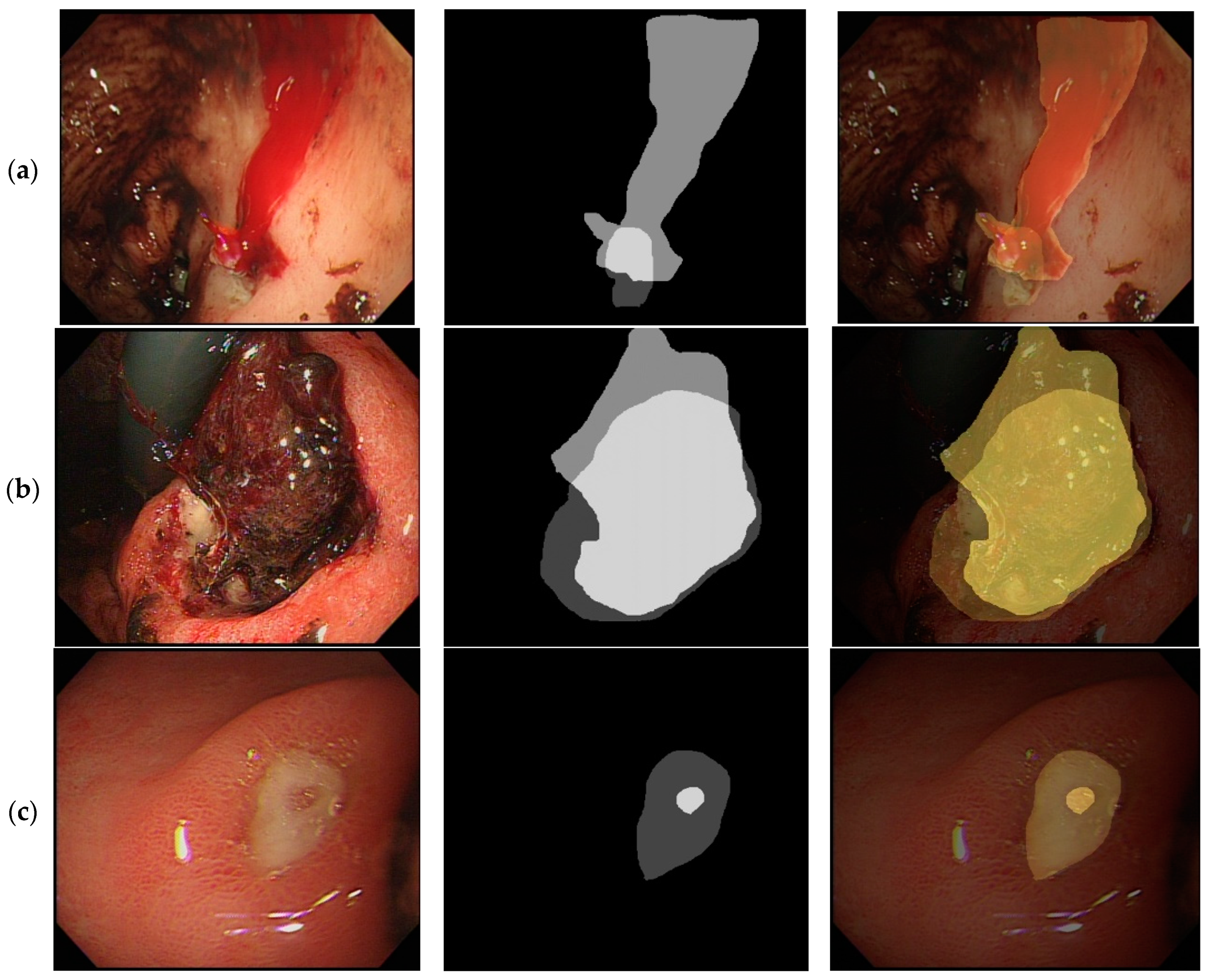
2.2. Process of Peptic Ulcer Image Segmentation
2.3. Evaluation of the Forrest Classification of Peptic Ulcers
2.4. Statistics
3. Results
3.1. Intra-Observer and Interobserver Agreement of the Obtained Images
3.2. Quantitative Analysis Comparing Endoscopic Images from Different Forrest Classifications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waddell, K.M.; Stanley, A.J.; Morris, A.J. Endoscopy for upper gastrointestinal bleeding: Where are we in 2017? Frontline Gastroenterol. 2017, 8, 94–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penny, H.A.; Kurien, M.; Wong, E.; Ahmed, R.; Ejenavi, E.; Lau, M.; Romaya, C.; Gohar, F.; Dear, K.L.; Kapur, K.; et al. Changing trends in the UK management of upper GI bleeding: Is there evidence of reduced UK training experience? Frontline Gastroenterol. 2016, 7, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gralnek, I.M.; Dumonceau, J.M.; Kuipers, E.J.; Lanas, A.; Sanders, D.S.; Kurien, M.; Rotondano, G.; Hucl, T.; Dinis-Ribeiro, M.; Marmo, R.; et al. Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015, 47, a1–a46. [Google Scholar] [CrossRef] [Green Version]
- Yen, H.H.; Wu, P.Y.; Chen, M.F.; Lin, W.C.; Tsai, C.L.; Lin, K.P. Current Status and Future Perspective of Artificial Intelligence in the Management of Peptic Ulcer Bleeding: A Review of Recent Literature. J. Clin. Med. 2021, 10, 3527. [Google Scholar] [CrossRef] [PubMed]
- Yen, H.-H.; Wu, P.-Y.; Su, P.-Y.; Yang, C.-W.; Chen, Y.-Y.; Chen, M.-F.; Lin, W.-C.; Tsai, C.-L.; Lin, K.-P. Performance Comparison of the Deep Learning and the Human Endoscopist for Bleeding Peptic Ulcer Disease. J. Med. Biol. Eng. 2021, 41, 504–513. [Google Scholar] [CrossRef]
- Forrest, J.A.; Finlayson, N.D.; Shearman, D.J. Endoscopy in gastrointestinal bleeding. Lancet 1974, 2, 394–397. [Google Scholar] [CrossRef]
- Mondardini, A.; Barletti, C.; Rocca, G.; Garripoli, A.; Sambataro, A.; Perotto, C.; Repici, A.; Ferrari, A. Non-variceal upper gastrointestinal bleeding and Forrest’s classification: Diagnostic agreement between endoscopists from the same area. Endoscopy 1998, 30, 508–512. [Google Scholar] [CrossRef]
- Barkun, A.N.; Almadi, M.; Kuipers, E.J.; Laine, L.; Sung, J.; Tse, F.; Leontiadis, G.I.; Abraham, N.S.; Calvet, X.; Chan, F.K.L.; et al. Management of Nonvariceal Upper Gastrointestinal Bleeding: Guideline Recommendations From the International Consensus Group. Ann. Intern. Med. 2019, 171, 805–822. [Google Scholar] [CrossRef] [Green Version]
- Sung, J.J.; Chiu, P.W.; Chan, F.K.L.; Lau, J.Y.; Goh, K.L.; Ho, L.H.; Jung, H.Y.; Sollano, J.D.; Gotoda, T.; Reddy, N.; et al. Asia-Pacific working group consensus on non-variceal upper gastrointestinal bleeding: An update 2018. Gut 2018, 67, 1757–1768. [Google Scholar] [CrossRef]
- Lu, Y.; Barkun, A.N.; Martel, M.; REASON Investigators. Adherence to guidelines: A national audit of the management of acute upper gastrointestinal bleeding. The REASON registry. Can. J. Gastroenterol. Hepatol. 2014, 28, 495–501. [Google Scholar] [CrossRef]
- Laine, L.; Freeman, M.; Cohen, H. Lack of uniformity in evaluation of endoscopic prognostic features of bleeding ulcers. Gastrointest. Endosc. 1994, 40, 411–417. [Google Scholar] [CrossRef]
- Freeman, M.L. Value of stigmata in decision-making in gastrointestinal haemorrhage. Best Pract. Res. Clin. Gastroenterol. 2000, 14, 411–425. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.-L.; Chou, K.-C.; Yen, H.-H. Stevens-Johnson syndrome: A rare complication of esomeprazole. Adv. Dig. Med. 2022, 9, 57–60. [Google Scholar] [CrossRef]
- Yen, H.H.; Yang, C.W.; Su, W.W.; Soon, M.S.; Wu, S.S.; Lin, H.J. Oral versus intravenous proton pump inhibitors in preventing re-bleeding for patients with peptic ulcer bleeding after successful endoscopic therapy. BMC Gastroenterol. 2012, 12, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bitar, S.M.; Moussa, M. The risk factors for the recurrent upper gastrointestinal hemorrhage among acute peptic ulcer disease patients in Syria: A prospective cohort study. Ann. Med. Surg. 2022, 74, 103252. [Google Scholar] [CrossRef]
- Hsiao, S.W.; Chen, M.W.; Yang, C.W.; Lin, K.H.; Chen, Y.Y.; Kor, C.T.; Huang, S.P.; Yen, H.H. A Nomogram for Predicting Laparoscopic and Endoscopic Cooperative Surgery during the Endoscopic Resection of Subepithelial Tumors of the Upper Gastrointestinal Tract. Diagnostics 2021, 11, 2160. [Google Scholar] [CrossRef]
- Chua, B.Q.Y.; Chong, V.W.S.; Teng, T.Z.J.; Chia, C.T.W.; Aung, M.O.; Shelat, V.G. Does technology-enhanced communication improve Helicobacter pylori eradication outcomes?—A meta-analysis. In Helicobacter; Wiley Online Library: New York, NY, USA, 2022; p. e12890. [Google Scholar] [CrossRef]
- Wang, T.E.; Wang, H.Y.; Lin, C.C.; Chen, T.Y.; Chang, C.W.; Chen, C.J.; Chen, M.J. Simulating a target lesion for endoscopic submucosal dissection training in an ex vivo pig model. Gastrointest. Endosc. 2011, 74, 398–402. [Google Scholar] [CrossRef]
- Mehta, V.; Kang, S.; Thoufeeq, M. The Role of Haemostasis Course in Increasing Knowledge and Skills in Managing Upper Gastrointestinal Bleed of the Delegates: A British Society of Gastroenterology’s Endoscopy Quality Improvement Programme, Yorkshire Project. Cureus 2021, 13, e15511. [Google Scholar] [CrossRef]
- Al-Rifaie, A.; Min, T.; Allam, D.; Smith, K.; Hurlstone, D.P.; Abdo, A.; Said, E.; Donnelly, M. Endoscopy training in upper GI bleeding for UK trainees in Khartoum, Sudan: South Yorkshire experience. Frontline Gastroenterol. 2020, 11, 496–497. [Google Scholar] [CrossRef]
- Lee, D.S.; Ahn, J.Y.; Lee, G.H. A Newly Designed 3-Dimensional Printer-Based Gastric Hemostasis Simulator with Two Modules for Endoscopic Trainees (with Video). Gut Liver 2019, 13, 415–420. [Google Scholar] [CrossRef] [Green Version]
- Siau, K.; Hawkes, N.D.; Dunckley, P. Training in Endoscopy. Curr. Treat. Options Gastroenterol. 2018, 16, 345–361. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.Y.; Sung, J.J.; Chan, A.C.; Lai, G.W.; Lau, J.T.; Ng, E.K.; Chung, S.C.; Li, A.K. Stigmata of hemorrhage in bleeding peptic ulcers: An interobserver agreement study among international experts. Gastrointest. Endosc. 1997, 46, 33–36. [Google Scholar] [CrossRef]
- Bour, B.; Person, B.; Cales, P.; Blanchi, A.; Burtin, P.; Oberti, F.; Boyer, J.; Kaassis, M.; Joundy, N.; Fort, J. Interobserver agreement on endoscopic diagnosis of bleeding peptic ulcers. Gastrointest. Endosc. 1997, 46, 27–32. [Google Scholar] [CrossRef]
- Freeman, M.L. Training endoscopists to recognize the stigmata of hemorrhage in bleeding ulcers. Endoscopy 1995, 27, 90–92. [Google Scholar] [CrossRef]
- de Groot, N.L.; van Oijen, M.G.; Kessels, K.; Hemmink, M.; Weusten, B.L.; Timmer, R.; Hazen, W.L.; van Lelyveld, N.; Vermeijden, R.R.; Curvers, W.L.; et al. Reassessment of the predictive value of the Forrest classification for peptic ulcer rebleeding and mortality: Can classification be simplified? Endoscopy 2014, 46, 46–52. [Google Scholar] [CrossRef]
- Xiaohua, H. Correlation between Endoscopic Morphology and Bleeding of Gastric Ulcer. J. Healthc. Eng. 2022, 2022, 2169551. [Google Scholar] [CrossRef]
- Lan, T.; Tong, H.; Qian, S.; Wei, B.; Huang, Z.; Wu, H.; Tan, Q.; Gao, J.; Bai, S.; Gong, H.; et al. Prophylactic transcatheter angiographic embolization reduces Forrest IIa ulcer rebleeding: A retrospective study. Medicine 2021, 100, e23855. [Google Scholar] [CrossRef]
- Kim, D.S.; Jung, Y.; Rhee, H.S.; Lee, S.J.; Jo, Y.G.; Kim, J.H.; Park, J.M.; Chung, I.K.; Cho, Y.S.; Lee, T.H.; et al. Usefulness of the Forrest Classification to Predict Artificial Ulcer Rebleeding during Second-Look Endoscopy after Endoscopic Submucosal Dissection. Clin. Endosc. 2016, 49, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Abdelrahim, M.; Saiga, H.; Maeda, N.; Hossain, E.; Ikeda, H.; Bhandari, P. Automated sizing of colorectal polyps using computer vision. Gut 2022, 71, 7–9. [Google Scholar] [CrossRef]
- Jha, D.; Ali, S.; Hicks, S.; Thambawita, V.; Borgli, H.; Smedsrud, P.H.; de Lange, T.; Pogorelov, K.; Wang, X.; Harzig, P.; et al. A comprehensive analysis of classification methods in gastrointestinal endoscopy imaging. Med. Image Anal. 2021, 70, 102007. [Google Scholar] [CrossRef]
- Ebigbo, A.; Mendel, R.; Probst, A.; Meinikheim, M.; Byrne, M.F.; Messmann, H.; Palm, C. Multimodal imaging for detection and segmentation of Barrett’s esophagus-related neoplasia using artificial intelligence. Endoscopy, 2021; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.Y.; Li, P.C.; Chang, R.F.; Chang, Y.Y.; Huang, S.P.; Chen, Y.Y.; Chang, W.Y.; Yen, H.H. Development and validation of a deep learning-based algorithm for colonoscopy quality assessment. Surg. Endosc. 2022; online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.Y.; Li, P.C.; Chang, R.F.; Yao, C.D.; Chen, Y.Y.; Chang, W.Y.; Yen, H.H. Deep learning-based endoscopic anatomy classification: An accelerated approach for data preparation and model validation. Surg. Endosc. 2021; online ahead of print. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rater | Intraclass Correlation | 95% Confidence INTERVAL |
|---|---|---|
| Experienced 1 | 0.95 | 0.94 to 0.97 |
| Experienced 2 | 0.95 | 0.93 to 0.97 |
| Junior 1 | 0.91 | 0.87 to 0.93 |
| Junior 2 | 0.92 | 0.89 to 0.94 |
| Junior 3 | 0.96 | 0.95 to 0.98 |
| Junior 4 | 0.97 | 0.95 to 0.98 |
| Experienced 1 | Experienced 2 | Junior 1 | Junior 2 | Junior 3 | Junior 4 | |
|---|---|---|---|---|---|---|
| Tutor a | 0.67 | 0.68 | 0.74 | 0.79 | 0.77 | 0.79 |
| Experienced 1 | 0.67 | 0.66 | 0.64 | 0.72 | 0.71 | |
| Experienced 2 | 0.68 | 0.64 | 0.65 | 0.71 | ||
| Junior 1 | 0.67 | 0.67 | 0.76 | |||
| Junior 2 | 0.86 | 0.74 | ||||
| Junior 3 | 0.73 |
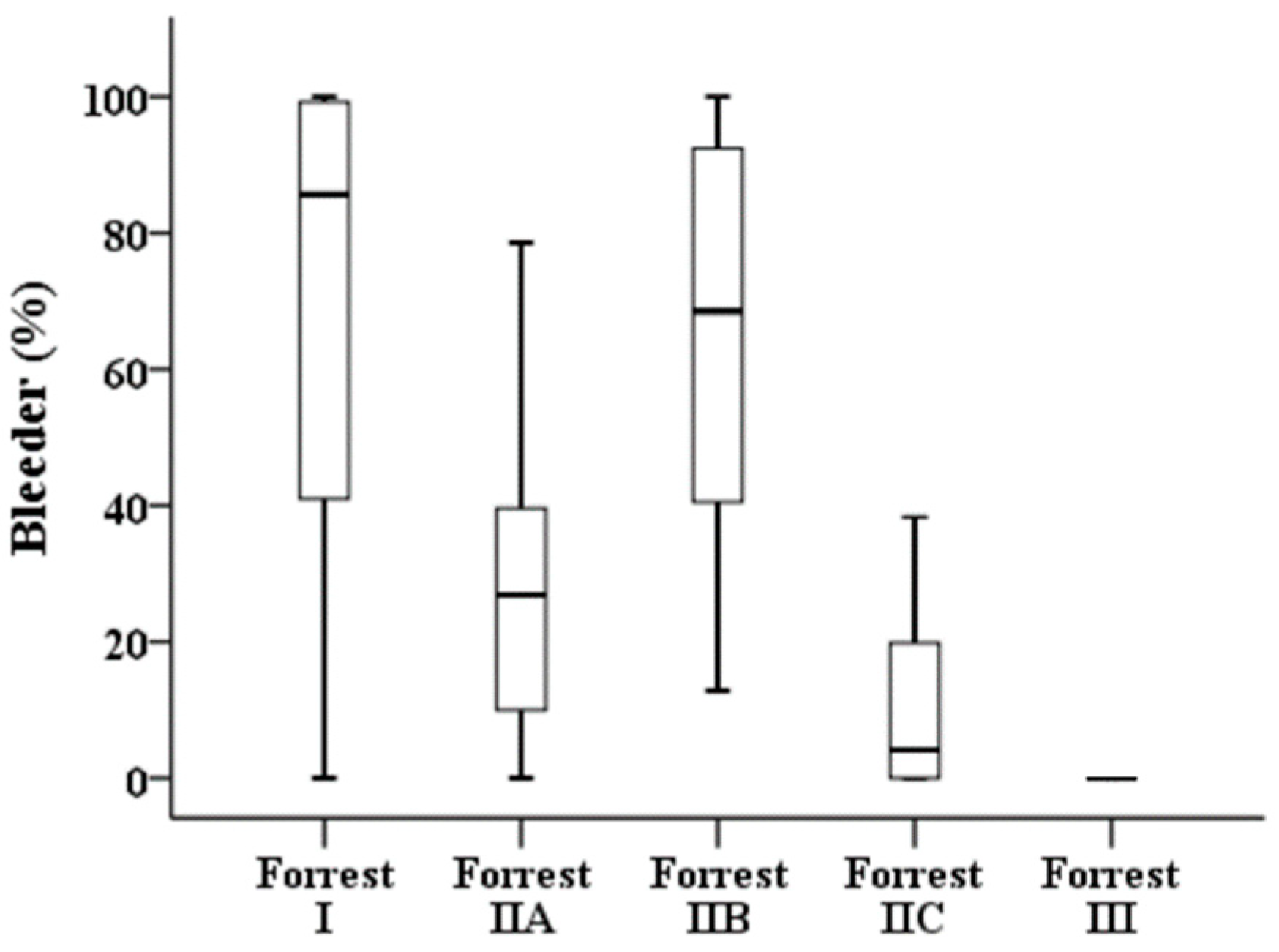
| All Patients (n = 276) | Forrest I (n = 54) | Forrest IIA (n = 44) | Forrest IIB (n = 18) | Forrest IIC (n = 53) | Forrest III (n = 107) | |
|---|---|---|---|---|---|---|
| Area of bleeder,%, median (IQR) | 4.56 (0–46.33) | 85.67 (40.97–99.23) | 26.88 (9.99–39.61) | 68.55 (40.52–92.4) | 4.11 (0–19.87) | 0 (0–0) |
| Comparison | Forrest I vs. Forrest IIA | Forrest I vs. Forrest IIB | Forrest I vs. Forrest IIC | Forrest I vs. Forrest III | Forrest IIA vs. Forrest IIB | |
| p-value a | 0.088 | 1.000 | <0.001 | <0.001 | <0.001 | |
| Comparison | Forrest IIA vs. Forrest IIC | Forrest IIA vs. Forrest III | Forrest IIB vs. Forrest IIC | Forrest IIB vs. Forrest III | Forrest IIC vs. Forrest III | |
| p-value a | 0.019 | <0.001 | <0.001 | <0.001 | <0.001 | |
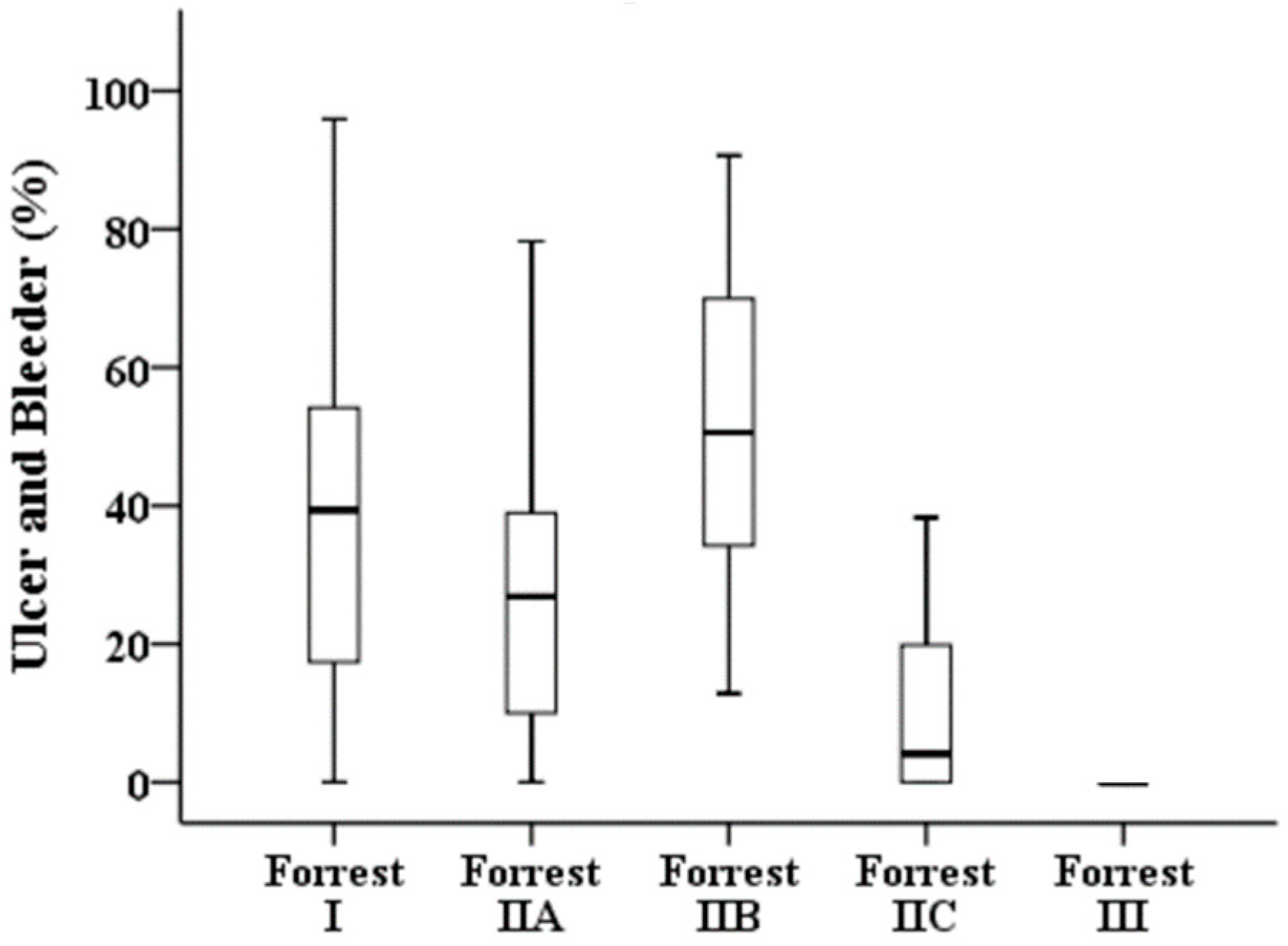
| Overlapping area of ulcer and bleeder,%, median (IQR) | 4.22 (0–35.07) | 39.38 (17.4–54.19) | 26.88 (9.99–38.94) | 50.57 (34.22–69.94) | 4.11 (0–19.87) | 0 (0–0) |
| Comparison | Forrest I vs. Forrest IIA | Forrest I vs. Forrest IIB | Forrest I vs. Forrest IIC | Forrest I vs. Forrest III | Forrest IIA vs. Forrest IIB | |
| p-value a | 1.000 | 1.000 | <0.001 | <0.001 | 0.536 | |
| Comparison | Forrest IIA vs. Forrest IIC | Forrest IIA vs. Forrest III | Forrest IIB vs. Forrest IIC | Forrest IIB vs. Forrest III | Forrest IIC vs. Forrest III | |
| p-value a | 0.007 | <0.001 | <0.001 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, H.-H.; Wu, P.-Y.; Wu, T.-L.; Huang, S.-P.; Chen, Y.-Y.; Chen, M.-F.; Lin, W.-C.; Tsai, C.-L.; Lin, K.-P. Forrest Classification for Bleeding Peptic Ulcer: A New Look at the Old Endoscopic Classification. Diagnostics 2022, 12, 1066. https://doi.org/10.3390/diagnostics12051066
Yen H-H, Wu P-Y, Wu T-L, Huang S-P, Chen Y-Y, Chen M-F, Lin W-C, Tsai C-L, Lin K-P. Forrest Classification for Bleeding Peptic Ulcer: A New Look at the Old Endoscopic Classification. Diagnostics. 2022; 12(5):1066. https://doi.org/10.3390/diagnostics12051066
Chicago/Turabian StyleYen, Hsu-Heng, Ping-Yu Wu, Tung-Lung Wu, Siou-Ping Huang, Yang-Yuan Chen, Mei-Fen Chen, Wen-Chen Lin, Cheng-Lun Tsai, and Kang-Ping Lin. 2022. "Forrest Classification for Bleeding Peptic Ulcer: A New Look at the Old Endoscopic Classification" Diagnostics 12, no. 5: 1066. https://doi.org/10.3390/diagnostics12051066
APA StyleYen, H.-H., Wu, P.-Y., Wu, T.-L., Huang, S.-P., Chen, Y.-Y., Chen, M.-F., Lin, W.-C., Tsai, C.-L., & Lin, K.-P. (2022). Forrest Classification for Bleeding Peptic Ulcer: A New Look at the Old Endoscopic Classification. Diagnostics, 12(5), 1066. https://doi.org/10.3390/diagnostics12051066