
Squamous Cell Carcinoma Antigen: Clinical Application and Research Status

Abstract
1. Introduction
- Tumor size and volume (more tumor cells result in a larger amount of SCCA);
- Invasiveness of the primary tumor or recurrence;
- Lymph node metastasis (LNM) (secreted SCCA from tumor cells in lymph nodes is easily detected in the bloodstream [12]);
- Distant metastasis (circulating tumor cells enable easy detection of secreted SCCA in blood tests [13]);
- Impairment of immunosurveillance.
2. SCCA Measurement
3. SCCA Levels in Cancer and Inflammation
3.1. Cervical Cancer
3.2. Lung Cancer
3.3. Neck and Head Cancer
3.4. Liver Cancer
3.5. Inflammation

{kind=link}
{kind=link}
{kind=link}
| Ref. | Marker | Disease | Sample Type | Sample Collection Time | Method | Cut-Off | Conclusion |
|---|---|---|---|---|---|---|---|
| Pontisso et al., 2004 [5] | SCCA1 variant | HCC | Tissues | At surgery | IHC | - | Diagnose HCC |
| Li et al., 2014 [6] | SCCA1/2, SCCA1 variant | HCC | Tissues | At surgery | RT-PCR Sequencing | - | Diagnose HCC |
| Lin et al., 2011 [12] | SCCA | OSCC | Serum | Preoperative | CLIA | 2.0 ng/mL | Predict metastasis, DFS and OS |
| Imai et al., 2015 [13] | SCCA | HNSCC | Serum | Pretreatment | CLIA | 1.1 ng/mL | Predict survival |
| Beneduce et al., 2005 [21] | SCCA-IgM | HCC | Serum | Pretreatment | EIA/WB | 120 AU/mL | Diagnose HCC |
| Ryu et al., 2015 [26] | SCCA | CSCC | Serum | Pretreatment Posttreatment | - | 1.86 ng/mL 0.9 ng/mL | Predict recurrence |
| Choi et al., 2020 [27] | SCCA | CSCC (stage IB-IVA | Serum | Pretreatment Treatment Recurrence | IRA | 4 ng/mL 1.5 ng/mL 4 ng/mL | Predict recurrence and survival |
| Zhu et al., 2021 [28] | SCCA | Early CSCC | Serum | Preoperative | CLIA | 1.5 ng/mL | Predict LNM and survival |
| Lekskul et al., 2015 [29] | SCCA | CSCC (stage IB2-IVA | Serum | Pretreatment | CLIA | 1.5 ng/mL | Predict pelvic and paraaortic LNM |
| Chen et al., 2020 [30] | SCCA | CSCC | Serum | Pretreatment posttreatment | ECLIA | 3.9 ng/mL 2.7 ng/mL | Evaluate the LNM and prognosis of CSCC who received neoadjuvant chemotherapy |
| Wang et al., 2019 [32] | SCCA | CSCC | Serum | Posttreatment | CLIA | 1.8 ng/mL | Predict treatment failure and poor survival of CSCC who received concurrent chemoradiotherapy |
| Salvatici et al., 2016 [33] | SCCA | CSCC (stage I-II) | Serum | Posttreatment | CLIA | 1.5 ng/mL | Early diagnosis of recurrence |
| Ye et al., 2020 [34] | SCCA | CSCC (stage IB1-IIA2) | Serum | day 0 (the day before surgery)/postoperative day 4, weeks 2–4, months 2–4 and months 5–7 | Single molecule assay (Simoa) prototype immunoassay | 2.49/0.66, 0.61, 0.72, and 0.71 ng/mL | Predict disease aggressiveness and treatment response |
| Chang et al., 2020 [36] | SCCA | CSCC | Serum | Pretreatment Posttreatment | - | - | Predict relapse and death |
| Reesink-Peters et al., 2005 [37] | SCCA | Early CSCC | Serum | CLIA | 1.9 ng/mL | Predict tumor relapse, and guide adjuvant therapies | |
| Guo et al., 2020 [38] | SCCA | CSCC with intermediate-risk factor | Serum | Preoperative | ELISA | 6.09 ng/mL | Predict the use of adjuvant chemotherapy |
| Yuan et al., 2021 [39] | SCCA | CSCC (stage IB-IIA) | Serum | Pretreatment | CLIA | 6.09 ng/mL | Guide adjuvant therapies |
| Oike et al., 2021 [40] | SCCA | CSCC (stage IB-IVA) | Serum | During follow-up | CLIA | 1.5 ng/mL | Improve the quality of follow-up and monitor renal dysfunction |
| Kinoshita et al., 2014 [42] | SCCA | SqCC | Serum | Presurgery | - | 1.5 ng/mL | Predict prognosis of resected peripheral-SqCC |
| Urquhart et al., 2013 [43] | SCCA1 | NSCLC (stage IV) | Tissues | Pretherapy | IHC | IHC score ≥ 2 | Predict resistance to PtC |
| Yasumatsu et al., 2019 [46] | SCCA2 | HNSCC | Serum | Pretreatment | CLIA | 1.5 ng/mL | Predict progression and guide management of HNSCC |
| Wu et al., 2020 [47] | SCCA1 | OSCC | Cell Tissues | - | WB | - | Provide target for OSCC gene therapy. |
| van Schaik et al., 2019 [49] | SCCA | HNSCC | FNA sample | Pretreatment | CLIA | 0.3 μg/mL | Diagnose HNSCC in cervical lymph nodes. |
| Yamashita et al., 2016 [50] | SCCA | Nasal IP | Serum | Presurgery/postsurgery | CLIA | 1.5 ng/mL | Distinguish new and recurrent IP from inflammatory diseases. |
| Promsopa et al., 2021 [51] | SCCA | IP | Serum | Presurgery/postsurgery | CLIA | 1.5 ng/mL | Distinguish IP from patients with nasal polyps and rhinitis. |
| Yasumatsu et al., 2018 [52] | SCCA1/2 | Sinonasal SCC and IP | Serum Tissue | Pretherapy | CLIA | 1.5 ng/mL | Distinguish sinonasal IP from squamous cell carcinoma |
| van Zijl et al., 2017 [53] | SCCA | Sinonasal IP | Serum | Pretreatment/posttreatment | microparticle enhanced immuno assay | 2.6/0.8 | Predict IP recurrence |
| Turato et al., 2019 [54] | SCCA1 SCCA-IgM | EAC | Serum Tissue | At surgery | ELISA IHC | 156 AU/mL | Predict immune surveillance impairment and reduced chemosensitivity |
| Trerotoli et al., 2009 [56] | SCCA | HCC | Tissue | Pretherapy | ELISA IHC | - | Early diagnosis of HCC |
| Bui et al., 2018 [59] | SCCA-IgM | Liver diseases | Serum | Presurgery | ELISA | - | Monitor cirrhosis in an Asian cohort of patients. |
| Giannelli et al., 2007 [57] | SCCA-IgM | HCC | Serum | Pretherapy Posttherapy | ELISA | - | Increase the accuracy of HCC diagnosis, especially when AFP values in 20–200 ng/mL. |
| Guarino et al., 2017 [60] | SCCA-IgM | HCC | Serum | at baseline (T0) and one month after treatment (T1) | ELISA | 120 AU/mL | Predict the outcome of therapy |
| Martini et al., 2015 [61] | SCCA-IgM | HCV-infected patients | Serum | Pretherapy Posttherapy | ELISA | - | Identify HCV-infected with a high risk of disease progression and HCC |
| Biasiolo et al., 2016 [64] | SCCA-IgM | Liver cirrhosis | Serum | During follow-up | ELISA | 156 AU/mL | Predict and manage cirrhotic patients at higher risk of HCC development. |
| Khattab et al., 2020 [66] | SCCA2 | Lichen planus | Serum | Pretherapy | ELISA | - | Diagnose lichen planus and predict disease severity |
| Watanabe et al., 2016 [67] | SCCA2 | Psoriasis | Serum Biopsy sample Cellular lysates | serial examinations | ELISA IHC WB | - | Associate with disease severity and reflects treatment efficacy |
| Takeuchi et al., 2019 [68] | SCCA1/2 | Pediatric atopic dermatitis | Serum | Pretherapy | - | - | Diagnose pediatric atopic dermatitis in the Ishigaki cohort. |
3.6. Others
4. Combination of SCCA with Other Markers in Clinical Practice
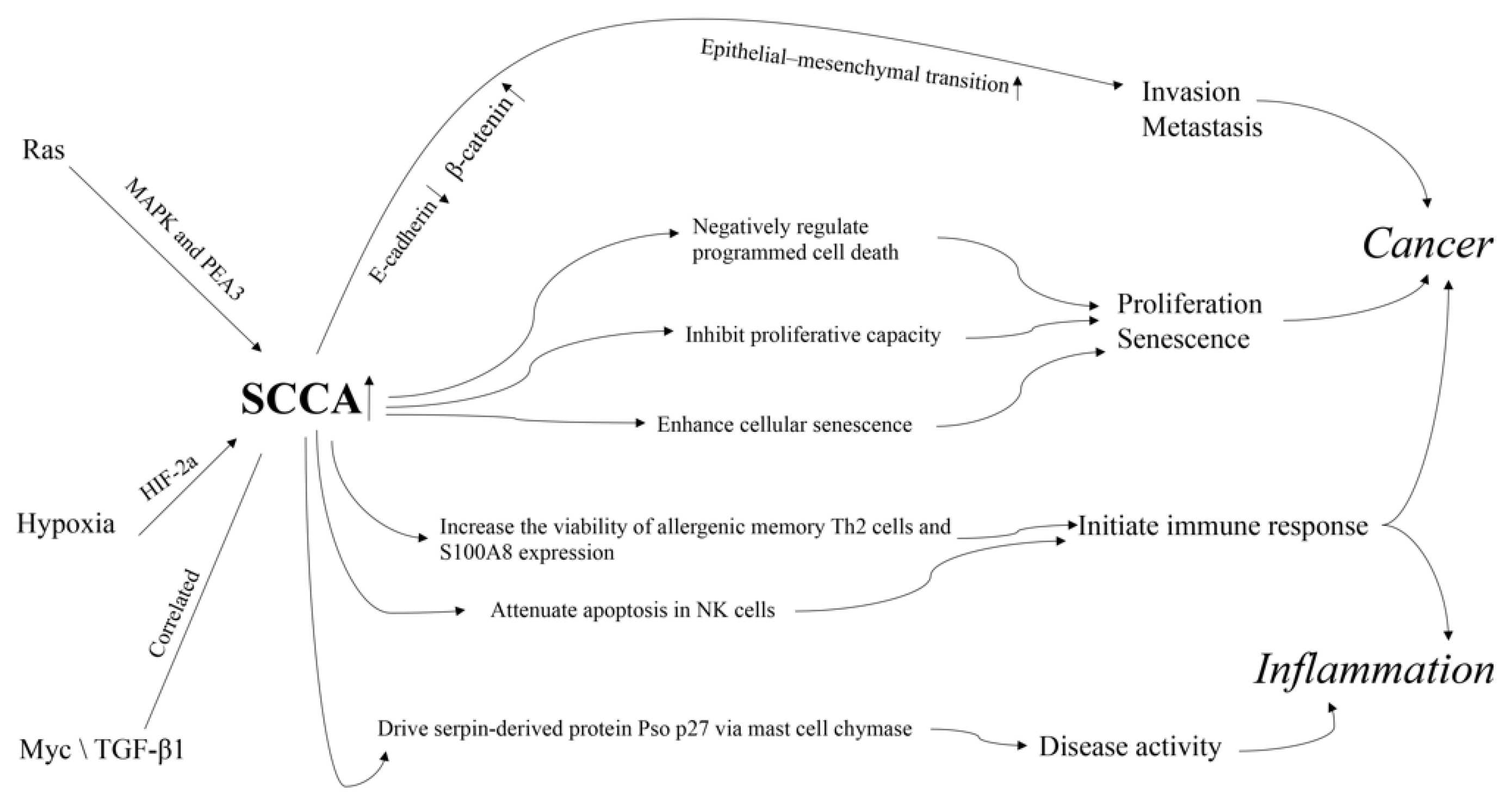
5. Related Mechanisms
6. Conclusions
- Differences in the primary site or stage distribution;
- Different measurement methods;
- Different cutoff values for SCCA;
- Different distributions of SCCA isoforms, including SCCA1, SCCA2, and SCCA–IgM;
- Ethnic biases.
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kato, H.; Torigoe, T. Radioimmunoassay for tumor antigen of human cervical squamous cell carcinoma. Cancer 1977, 40, 1621–1628. [Google Scholar] [CrossRef]
- Sun, Y.; Sheshadri, N.; Zong, W.X. SERPINB3 and B4: From biochemistry to biology. Semin. Cell Dev. Biol. 2017, 62, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Nagaya, T.; Torigoe, T. Heterogeneity of a tumor antigen TA-4 of squamous cell carcinoma in relation to its appearance in the circulation. Gan 1984, 75, 433–435. [Google Scholar] [PubMed]
- Stelzer, G.; Rosen, N.; Plaschkes, I.; Zimmerman, S.; Twik, M.; Fishilevich, S.; Stein, T.I.; Nudel, R.; Lieder, I.; Mazor, Y.; et al. The GeneCards suite: From gene data mining to disease genome sequence analyses. Curr. Protoc. Bioinform. 2016, 54, 1.30.1–1.30.33. [Google Scholar] [CrossRef] [PubMed]
- Pontisso, P.; Calabrese, F.; Benvegnu, L.; Lise, M.; Belluco, C.; Ruvoletto, M.G.; Marino, M.; Valente, M.; Nitti, D.; Gatta, A.; et al. Overexpression of squamous cell carcinoma antigen variants in hepatocellular carcinoma. Br. J. Cancer 2004, 90, 833–837. [Google Scholar] [CrossRef]
- Li, S.; Gao, Y.; Yang, B.; Liang, Z.; Wang, Y.; Zhai, D.; Jing, L.; Liu, T.; Wang, F.; Du, Z.; et al. Squamous cell carcinoma antigen 1 and 2 mRNA and a new variant expressed in hepatocellular carcinoma. Neoplasma 2014, 61, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Wang, J.; Zhang, L. Serum SCCA levels in patients suffering cancers or other diseases. In Progress in Molecular Biology and Translational Science; Elsevier: Amsterdam, The Netherlands, 2019; pp. 165–175. [Google Scholar]
- Chen, H.; Tian, L.; Chen, J.; Sun, P.; Han, R.; Wu, X.; Dai, S. Evaluation of 2 commercially systems for detection of serum squamous cell carcinoma antigen in pan squamous cell carcinoma. Cancer Control 2020, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kesimer, M.; Scull, M.; Brighton, B.; DeMaria, G.; Burns, K.; O’Neal, W.; Pickles, R.J.; Sheehan, J.K. Characterization of exosome-like vesicles released from human tracheobronchial ciliated epithelium: A possible role in innate defense. FASEB J. 2009, 23, 1858–1868. [Google Scholar] [CrossRef]
- Quarta, S.; Vidalino, L.; Turato, C.; Ruvoletto, M.; Calabrese, F.; Valente, M.; Cannito, S.; Fassina, G.; Parola, M.; Gatta, A.; et al. SERPINB3 induces epithelial-mesenchymal transition. J. Pathol. 2010, 221, 343–356. [Google Scholar] [CrossRef] [PubMed]
- Petty, R.D.; Kerr, K.M.; Murray, G.I.; Nicolson, M.C.; Rooney, P.H.; Bissett, D.; Collie-Duguid, E.S. Tumor transcriptome reveals the predictive and prognostic impact of lysosomal protease inhibitors in non-small-cell lung cancer. J. Clin. Oncol. 2006, 24, 1729–1744. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lin, W.H.; Chen, I.H.; Wei, F.C.; Huang, J.J.; Kang, C.J.; Hsieh, L.L.; Wang, H.M.; Huang, S.F. Clinical significance of preoperative squamous cell carcinoma antigen in oral-cavity squamous cell carcinoma. Laryngoscope 2011, 121, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Imai, R.; Takenaka, Y.; Yasui, T.; Nakahara, S.; Yamamoto, Y.; Hanamoto, A.; Takemoto, N.; Fukusumi, T.; Cho, H.; Yamamoto, M.; et al. Prognostic significance of serum squamous cell carcinoma antigen in patients with head and neck cancer. Acta Otolaryngol. 2015, 135, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Derakhshan, S.; Poosti, A.; Razavi, A.E.; Moosavi, M.A.; Mahdavi, N.; Naieni, F.B.; Hesari, K.K.; Rahpeima, A. Evaluation of squamous cell carcinoma antigen 1 expression in oral squamous cell carcinoma (tumor cells and peritumoral T-lymphocytes) and verrucous carcinoma and comparison with normal oral mucosa. J. Appl. Oral Sci. 2021, 29, e20210374. [Google Scholar] [CrossRef] [PubMed]
- Crombach, G.; Scharl, A.; Vierbuchen, M.; Wurz, H.; Bolte, A. Detection of squamous cell carcinoma antigen in normal squamous epithelia and in squamous cell carcinomas of the uterine cervix. Cancer 1989, 63, 1337–1342. [Google Scholar] [CrossRef]
- Herman, D.S.; Ranjitkar, P.; Yamaguchi, D.; Grenache, D.G.; Greene, D.N. Endogenous alkaline phosphatase interference in cardiac troponin I and other sensitive chemiluminescence immunoassays that use alkaline phosphatase activity for signal amplification. Clin. Biochem. 2016, 49, 1118–1121. [Google Scholar] [CrossRef] [PubMed]
- Mori, E.; Kurano, M.; Tobita, A.; Shimosaka, H.; Yatomi, Y. Existence of a squamous cell carcinoma antigen-immunoglobulin complex causes a deviation between squamous cell carcinoma antigen concentrations determined using two different immunoassays: First report of squamous cell carcinoma antigen coupling with immunoglobulin A. Ann. Clin. Biochem. 2017, 54, 655–663. [Google Scholar] [PubMed]
- Holdenrieder, S.; Molina, R.; Qiu, L.; Zhi, X.; Rutz, S.; Engel, C.; Kasper-Sauer, P.; Dayyani, F.; Korse, C.M. Technical and clinical performance of a new assay to detect squamous cell carcinoma antigen levels for the differential diagnosis of cervical, lung, and head and neck cancer. Tumor Biol. 2018, 40, 1–13. [Google Scholar] [CrossRef]
- Ohta, S.; Shibata, R.; Nakao, Y.; Azuma, Y.; Taniguchi, K.; Arima, K.; Suzuki, S.; Shiraishi, H.; Iwasaka, T.; Izuhara, K. The usefulness of combined measurements of squamous cell carcinoma antigens 1 and 2 in diagnosing atopic dermatitis. Ann. Clin. Biochem. 2012, 49, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, J.; Uh, Y.; Kim, H.S.; Lee, J.H. Comparison Between a Manual Squamous Cell Carcinoma Antigen Assay and an Automated Assay in a Clinical Setting. Lab. Med. 2018, 49, 254–258. [Google Scholar] [CrossRef]
- Beneduce, L.; Castaldi, F.; Marino, M.; Quarta, S.; Ruvoletto, M.; Benvegnu, L.; Calabrese, F.; Gatta, A.; Pontisso, P.; Fassina, G. Squamous cell carcinoma antigen-immunoglobulin M complexes as novel biomarkers for hepatocellular carcinoma. Cancer 2005, 103, 2558–2565. [Google Scholar] [CrossRef]
- Mirpour, S.; Mhlanga, J.C.; Logeswaran, P.; Russo, G.; Mercier, G.; Subramaniam, R.M. The role of PET/CT in the management of cervical cancer. AJR Am. J. Roentgenol. 2013, 201, W192–W205. [Google Scholar] [CrossRef] [PubMed]
- Mittra, E.; El-Maghraby, T.; Rodriguez, C.A.; Quon, A.; McDougall, I.R.; Gambhir, S.S.; Iagaru, A. Efficacy of 18F-FDG PET/CT in the evaluation of patients with recurrent cervical carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1952–1959. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.Y.; Fan, W.; Zhang, X.; Liang, P.Y.; Lin, X.P.; Zhang, Y.R.; Li, Y.H. Complementary roles of squamous cell carcinoma antigen and (18)F-FDG PET/CT in suspected recurrence of cervical squamous cell cancer. J. Cancer 2015, 6, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Qi, C.; He, S.; Cai, L.; Zhang, L.; Ding, H.; Chen, Y. A study on the clinical value of (18)F-fluorodeoxyglucose positron emission tomography/computed tomography combined with serum squamous cell carcinoma antigen in diagnosing recurrence/metastases in patients with early metaphase cervical cancer. Oncol. Lett. 2021, 22, 746. [Google Scholar] [CrossRef]
- Ryu, H.K.; Baek, J.S.; Kang, W.D.; Kim, S.M. The prognostic value of squamous cell carcinoma antigen for predicting tumor recurrence in cervical squamous cell carcinoma patients. Obstet. Gynecol. Sci. 2015, 58, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Yu, M.; Jeong, S.; Lee, J.H. Can serial evaluation of serum SCC-Ag-level predict tumor recurrence and patient survival in squamous-cell carcinoma of uterine cervix treated with definitive chemoradiotherapy? A multi-institutional analysis. Int. J. Clin. Oncol. 2020, 25, 1405–1411. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Zhang, W.; Wang, X.; Jiao, L.; Chen, L.; Jiang, J. Predictive value of preoperative serum squamous cell carcinoma antigen level for lymph node metastasis in early-stage cervical squamous cell carcinoma. Medicine 2021, 100, e26960. [Google Scholar] [CrossRef] [PubMed]
- Lekskul, N.; Charakorn, C.; Lertkhachonsuk, A.A.; Rattanasiri, S.; Israngura Na Ayudhya, N. The level of squamous cell carcinoma antigen and lymph node metastasis in locally advanced cervical cancer. Asian Pac. J. Cancer Prev. 2015, 16, 4719–4722. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Jiao, L.; Ren, F.; Wang, D.B. Clinical value of serum squamous cell carcinoma antigen levels in predicting chemosensitivity, lymph node metastasis, and prognosis in patients with cervical squamous cell carcinoma. BMC Cancer 2020, 20, 423. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Wang, W.; Wang, Y.; Liu, C.; Wang, P. The role of squamous cell carcinoma antigen (SCC Ag) in outcome prediction after concurrent chemoradiotherapy and treatment decisions for patients with cervical cancer. Radiat. Oncol. 2019, 14, 146. [Google Scholar] [CrossRef]
- Wang, W.; Liu, X.; Hou, X.; Lian, X.; Liu, Z.; Shen, J.; Sun, S.; Yan, J.; Miao, Z.; Wang, D.; et al. Posttreatment squamous cell carcinoma antigen predicts treatment failure in patients with cervical squamous cell carcinoma treated with concurrent chemoradiotherapy. Gynecol. Oncol. 2019, 155, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Salvatici, M.; Achilarre, M.T.; Sandri, M.T.; Boveri, S.; Vanna, Z.; Landoni, F. Squamous cell carcinoma antigen (SCC-Ag) during follow-up of cervical cancer patients: Role in the early diagnosis of recurrence. Gynecol. Oncol. 2016, 142, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.; Sun, X.; Kang, B.; Wu, F.; Zheng, Z.; Xiang, L.; Lesenechal, M.; Heskia, F.; Liang, J.; Yang, H. The kinetic profile and clinical implication of SCC-Ag in squamous cervical cancer patients undergoing radical hysterectomy using the Simoa assay: A prospective observational study. BMC Cancer 2020, 20, 138. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, S.W.; Kim, J.R.; Kim, Y.S.; Yoon, M.S.; Jeong, S.; Kim, J.H.; Lee, J.Y.; Eom, K.Y.; Jeong, B.K.; et al. Tumour size, volume, and marker expression during radiation therapy can predict survival of cervical cancer patients: A multi-institutional retrospective analysis of KROG 16-01. Gynecol. Oncol. 2017, 147, 577–584. [Google Scholar] [CrossRef]
- Chang, C.; Chen, J.; Huang, C.H.; Lee, W.Y.; Hsu, L.C.; Chiang, A.J. Time-dependent squamous cell carcinoma antigen in prediction of relapse and death of patients with cervical cancer. J. Low. Genit. Tract Dis. 2020, 24, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Reesink-Peters, N.; van der Velden, J.; Ten Hoor, K.A.; Boezen, H.M.; de Vries, E.G.; Schilthuis, M.S.; Mourits, M.J.; Nijman, H.W.; Aalders, J.G.; Hollema, H.; et al. Preoperative serum squamous cell carcinoma antigen levels in clinical decision making for patients with early-stage cervical cancer. J. Clin. Oncol. 2005, 23, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.T.; Bi, X.H.; Lei, T.; Lv, X.; Yao, G.; Chen, Y.; Liu, C. Preoperative SCC-Ag as a predictive marker for the use of adjuvant chemotherapy in cervical squamous cell carcinoma with intermediate-risk factors. BMC Cancer 2020, 20, 441. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Z.; Cao, D.; Zhang, Y.; Shen, K.; Yang, J.; Yu, M.; Zhou, H. Could adjuvant chemotherapy improve prognosis for cervical cancer patients with elevated pretreatment serum squamous-cell carcinoma antigen? Risk Manag. Healthc Policy 2021, 14, 109–116. [Google Scholar] [CrossRef]
- Oike, T.; Oike, T.; Ando, K.; Iwase, A.; Ohno, T. The Non-Cancer Specific Elevation of the Serum Squamous Cell Carcinoma Antigen during the Post-Radiotherapy Follow-Up of Cervical Cancer Patients. Diagnostics 2021, 11, 1585. [Google Scholar] [CrossRef] [PubMed]
- Kagohashi, K.; Satoh, H.; Ishikawa, H.; Ohtsuka, M.; Sekizawa, K. A re-evaluation of squamous cell carcinoma antigen (SCC) as a serum marker for non-small cell lung cancer. Med. Oncol. 2008, 25, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, T.; Ohtsuka, T.; Hato, T.; Goto, T.; Kamiyama, I.; Tajima, A.; Emoto, K.; Hayashi, Y.; Kohno, M. Prognostic factors based on clinicopathological data among the patients with resected peripheral squamous cell carcinomas of the lung. J. Thorac. Oncol. 2014, 9, 1779–1787. [Google Scholar] [CrossRef] [PubMed]
- Urquhart, G.; Kerr, K.M.; Nicolson, M.; Loo, P.S.; Sharma, R.; Shrimali, R.; Petty, R.D. Serpin b3 is associated with poor survival after chemotherapy and is a potential novel predictive biomarker in advanced non-small-cell lung cancer. J. Thorac. Oncol. 2013, 8, 1502–1509. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kagohashi, K.; Satoh, H.; Kurishima, K.; Kadono, K.; Ishikawa, H.; Ohtsuka, M.; Sekizawa, K. Squamous cell carcinoma antigen in lung cancer and nonmalignant respiratory diseases. Lung 2008, 186, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Zanatta, E.; Martini, A.; Scarpieri, E.; Biasiolo, A.; Ortolan, A.; Benvenuti, F.; Cozzi, F.; Pontisso, P.; Doria, A. Squamous cell carcinoma antigen-IgM (SCCA-IgM) is associated with interstitial lung disease in systemic sclerosis. Jt. Bone Spine 2020, 87, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Yasumatsu, R.; Nakano, T.; Hashimoto, K.; Kogo, R.; Wakasaki, T.; Nakagawa, T. The clinical value of serum squamous cell carcinoma antigens 1 and 2 in head and neck squamous cell carcinoma. Auris Nasus Larynx 2019, 46, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Guo, Q.; Zhang, G.; Zhao, L.; Lv, Y.; Wang, J.; Liu, J.; Shi, W. Study on the targeted therapy of oral squamous cell carcinoma with a plasmid expressing PE38KDEL toxin under control of the SERPINB3 promoter. Cancer Med. 2020, 9, 2213–2222. [Google Scholar] [CrossRef]
- Travassos, D.C.; Fernandes, D.; Massucato, E.M.S.; Navarro, C.M.; Bufalino, A. Squamous cell carcinoma antigen as a prognostic marker and its correlation with clinicopathological features in head and neck squamous cell carcinoma: Systematic review and meta-analysis. J. Oral Pathol. Med. 2018, 47, 3–10. [Google Scholar] [CrossRef] [PubMed]
- van Schaik, J.E.; Muller Kobold, A.C.; van der Laan, B.; van der Vegt, B.; van Hemel, B.M.; Plaat, B.E.C. Squamous cell carcinoma antigen concentration in fine needle aspiration samples: A new method to detect cervical lymph node metastases of head and neck squamous cell carcinoma. Head Neck 2019, 41, 2561–2565. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Uehara, T.; Hasegawa, M.; Deng, Z.; Matayoshi, S.; Kiyuna, A.; Kondo, S.; Maeda, H.; Ganaha, A.; Suzuki, M. Squamous cell carcinoma antigen as a diagnostic marker of nasal inverted papilloma. Am. J. Rhinol. Allergy 2016, 30, 122–127. [Google Scholar] [CrossRef]
- Promsopa, C.; Suwansri, S.; Khuntikij, P. The serum squamous cell carcinoma antigen level in inverted sinonasal papilloma and nasal polyps patients. World J. Otorhinolaryngol. Head Neck Surg. 2021, 7, 23–27. [Google Scholar] [CrossRef]
- Yasumatsu, R.; Nakano, T.; Sato, M.; Jiroumaru, R.; Hashimoto, K.; Kogo, R.; Wakasaki, T.; Nakashima, T.; Nakagawa, T. Combination of serum squamous cell carcinoma antigens 1 and 2 as potential diagnostic marker for sinonasal squamous cell carcinoma and inverted papilloma. Head Neck 2018, 40, 2583–2589. [Google Scholar] [CrossRef] [PubMed]
- van Zijl, F.; Monserez, D.A.; Korevaar, T.I.M.; Bugter, O.; Wieringa, M.H.; Baatenburg de Jong, R.J.; Hardillo, J.A.U. Postoperative value of serum squamous cell carcinoma antigen as a predictor of recurrence in sinonasal inverted papilloma. Clin. Otolaryngol. 2017, 42, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Turato, C.; Scarpa, M.; Kotsafti, A.; Cappon, A.; Quarta, S.; Biasiolo, A.; Cavallin, F.; Trevellin, E.; Guzzardo, V.; Fassan, M.; et al. Squamous cell carcinoma antigen 1 is associated to poor prognosis in esophageal cancer through immune surveillance impairment and reduced chemosensitivity. Cancer Sci. 2019, 110, 1552–1563. [Google Scholar] [CrossRef] [PubMed]
- Montagnana, M.; Danese, E.; Lippi, G. Squamous cell carcinoma antigen in hepatocellular carcinoma: Ready for the prime time? Clin. Chim. Acta 2015, 445, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Trerotoli, P.; Fransvea, E.; Angelotti, U.; Antonaci, G.; Lupo, L.; Mazzocca, A.; Mangia, A.; Antonaci, S.; Giannelli, G. Tissue expression of Squamous Cellular Carcinoma Antigen (SCCA) is inversely correlated to tumor size in HCC. Mol. Cancer 2009, 8, 29. [Google Scholar] [CrossRef] [PubMed]
- Giannelli, G.; Fransvea, E.; Trerotoli, P.; Beaugrand, M.; Marinosci, F.; Lupo, L.; Nkontchou, G.; Dentico, P.; Antonaci, S. Clinical validation of combined serological biomarkers for improved hepatocellular carcinoma diagnosis in 961 patients. Clin. Chim. Acta 2007, 383, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Wang, Z.J.; Chen, L.H.; Dong, W.Z. Diagnostic value of serum squamous cell carcinoma antigen for hepatocellular carcinoma: A systematic review and meta-analysis. Scand. J. Clin. Lab. Investig. 2017, 77, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Bui Huu, H.; Ha Thuc, N.; Thi Le, H.P.; Thi Thanh, T.D.; Luong Bac, A.; Tiribelli, C.; Pontisso, P.; Gallotta, A.; Paneghetti, L.; Fassina, G. Characterization of SCCA-IgM as a biomarker of liver disease in an Asian cohort of patients. Scand. J. Clin. Lab. Investig. 2018, 78, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Guarino, M.; Di Costanzo, G.G.; Gallotta, A.; Tortora, R.; Paneghetti, L.; Auriemma, F.; Tuccillo, C.; Fassina, G.; Caporaso, N.; Morisco, F. Circulating SCCA-IgM complex is a useful biomarker to predict the outcome of therapy in hepatocellular carcinoma patients. Scand. J. Clin. Lab. Investig. 2017, 77, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Martini, A.; Fattovich, G.; Guido, M.; Bugianesi, E.; Biasiolo, A.; Ieluzzi, D.; Gallotta, A.; Fassina, G.; Merkel, C.; Gatta, A.; et al. HCV genotype 3 and squamous cell carcinoma antigen (SCCA)-IgM are independently associated with histological features of NASH in HCV-infected patients. J. Viral Hepat. 2015, 22, 800–808. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Bettini, S.; Bordigato, E.; Milan, G.; Dal Pra, C.; Favaretto, F.; Belligoli, A.; Sanna, M.; Serra, R.; Foletto, M.; Prevedello, L.; et al. SCCA-IgM as a potential biomarker of non-alcoholic fatty liver disease in patients with obesity, prediabetes and diabetes undergoing sleeve gastrectomy. Obes. Facts 2019, 12, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Biasiolo, A.; Trotta, E.; Fasolato, S.; Ruvoletto, M.; Martini, A.; Gallotta, A.; Fassina, G.; Angeli, P.; Gatta, A.; Pontisso, P. Squamous cell carcinoma antigen-IgM is associated with hepatocellular carcinoma in patients with cirrhosis: A prospective study. Dig. Liver Dis. 2016, 48, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Shi, X.; Wang, Y.; Zhao, Y. Serum squamous cell carcinoma antigen in psoriasis: A potential quantitative biomarker for disease severity. Dermatology 2018, 234, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Khattab, F.M.; Samir, M.A. Measurement of squamous cell carcinoma antigen 2 in lichen planus patients. J. Cosmet. Dermatol. 2020, 19, 1780–1784. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Yamaguchi, Y.; Komitsu, N.; Ohta, S.; Azuma, Y.; Izuhara, K.; Aihara, M. Elevation of serum squamous cell carcinoma antigen 2 in patients with psoriasis: Associations with disease severity and response to the treatment. Br. J. Dermatol. 2016, 174, 1327–1336. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, S.; Furusyo, N.; Ono, J.; Azuma, Y.; Takemura, M.; Esaki, H.; Yamamura, K.; Mitamura, Y.; Tsuji, G.; Kiyomatsu-Oda, M.; et al. Serum squamous cell carcinoma antigen (SCCA)-2 correlates with clinical severity of pediatric atopic dermatitis in Ishigaki cohort. J. Dermatol. Sci. 2019, 95, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Marchioni, M.; Berardinelli, F.; De Nunzio, C.; Spiess, P.; Porpiglia, F.; Schips, L.; Cindolo, L. New insight in penile cancer. Minerva Urol. Nefrol. 2018, 70, 559–569. [Google Scholar] [CrossRef] [PubMed]
- Kommu, S.; Hadway, P.; Watkin, N. Squamous cell carcinoma antigen as a biomarker for penile cancer. BJU Int. 2005, 95, 478–479. [Google Scholar] [CrossRef]
- Touloupidis, S.; Zisimopoulos, A.; Giannakopoulos, S.; Papatsoris, A.G.; Kalaitzis, C.; Thanos, A. Clinical usage of the squamous cell carcinoma antigen in patients with penile cancer. Int. J. Urol. 2007, 14, 174–176. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Ye, D.W.; Yao, X.D.; Zhang, S.L.; Dai, B.; Zhang, H.L.; Shen, Y.J. The value of squamous cell carcinoma antigen in the prognostic evaluation, treatment monitoring and followup of patients with penile cancer. J. Urol. 2008, 180, 2019–2023. [Google Scholar] [CrossRef] [PubMed]
- Zargar-Shoshtari, K.; Sharma, P.; Spiess, P.E. Insight into novel biomarkers in penile cancer: Redefining the present and future treatment paradigm? Urol. Oncol. 2018, 36, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, K.; Kumamoto, Y.; Tsukamoto, T. Expression of squamous cell carcinoma-associated antigen in bladder cancer cells—A comparative study with the expression of proliferating cell nuclear antigen (PCNA). Nihon Hinyokika Gakkai Zasshi 1994, 85, 589–598. [Google Scholar] [PubMed]
- Hoshi, S.; Numahata, K.; Morozumi, K.; Katumata, Y.; Kuromoto, A.; Takai, Y.; Hoshi, K.; Bilim, V.; Sasagawa, I. Bladder cancer metastasis producing beta-human chorionic gonadotropin, squamous cell carcinoma antigen, granulocyte-colony stimulating factor, and parathyroid hormone-related protein. IJU Case Rep. 2018, 14, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Muniz, T.P.; Sorotsky, H.; Kanjanapan, Y.; Rose, A.A.N.; Araujo, D.V.; Fortuna, A.; Ghazarian, D.; Kamil, Z.S.; Pugh, T.; Mah, M.; et al. Genomic landscape of malignant peripheral nerve sheath tumor–like melanoma. J. Investig. Dermatol. 2021, 141, 2470–2479. [Google Scholar] [CrossRef]
- Guo, S.; Yang, B.; Liu, H.; Li, Y.; Li, S.; Ma, L.; Liu, J.; Guo, W. Serum expression level of squamous cell carcinoma antigen, highly sensitive C-reactive protein, and CA-125 as potential biomarkers for recurrence of cervical cancer. J. Cancer Res. Ther. 2017, 13, 689–692. [Google Scholar] [CrossRef] [PubMed]
- Adel, M.; Tsao, C.K.; Wei, F.C.; Chien, H.T.; Lai, C.H.; Liao, C.T.; Wang, H.M.; Fan, K.H.; Kang, C.J.; Chang, J.T.; et al. Preoperative SCC antigen, CRP serum levels, and lymph node density in oral squamous cell carcinoma. Medicine 2016, 95, e3149. [Google Scholar] [CrossRef]
- Li, Z.S.; Yao, K.; Li, Y.H.; Chen, J.P.; Deng, C.Z.; Zhao, Q.; Chen, P.; Wang, B.; Mi, Q.W.; Liu, Z.W.; et al. Clinical significance of preoperative C-reactive protein and squamous cell carcinoma antigen levels in patients with penile squamous cell carcinoma. BJU Int. 2016, 118, 272–278. [Google Scholar] [CrossRef]
- Wu, L.L.; Liu, X.; Huang, W.; Lin, P.; Long, H.; Zhang, L.J.; Ma, G.W. Preoperative squamous cell carcinoma antigen and albumin serum levels predict the survival of patients with stage T1-3N0M0 esophageal squamous cell carcinoma: A retrospective observational study. J. Cardiothorac. Surg. 2020, 15, 115. [Google Scholar] [CrossRef]
- Ali, L.H.; Higazi, A.M.; Moness, H.M.; Farag, N.M.; Saad, Z.M.; Moukareb, H.A.; Soliman, W.; El Sagheer, G.; Abd El Hamid, S.R.; Abdl Hamid, H. Clinical significances and diagnostic utilities of both miR-215 and squamous cell carcinoma antigen-IgM versus alpha-fetoprotein in Egyptian patients with hepatitis C virus-induced hepatocellular carcinoma. Clin. Exp. Gastroenterol. 2019, 12, 51–66. [Google Scholar] [CrossRef]
- Wen, Y.F.; Cheng, T.T.; Chen, X.L.; Huang, W.J.; Peng, H.H.; Zhou, T.C.; Lin, X.D.; Zeng, L.S. Elevated circulating tumor cells and squamous cell carcinoma antigen levels predict poor survival for patients with locally advanced cervical cancer treated with radiotherapy. PLoS ONE 2018, 13, e0204334. [Google Scholar]
- Hashimoto, K.; Kiyoshima, T.; Matsuo, K.; Ozeki, S.; Sakai, H. Effect of SCCA1 and SCCA2 on the suppression of TNF-alpha-induced cell death by impeding the release of mitochondrial cytochrome c in an oral squamous cell carcinoma cell line. Tumor Biol. 2005, 26, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Zhai, L.; Qian, L.; Huang, D.; Ding, Y.; Xiang, H.; Liu, X.; Thompson, J.W.; Liu, J.; He, Y.H.; et al. Switching off IMMP2L signaling drives senescence via simultaneous metabolic alteration and blockage of cell death. Cell Res. 2018, 28, 625–643. [Google Scholar] [CrossRef] [PubMed]
- Catanzaro, J.M.; Sheshadri, N.; Pan, J.A.; Sun, Y.; Shi, C.; Li, J.; Powers, R.S.; Crawford, H.C.; Zong, W.X. Oncogenic Ras induces inflammatory cytokine production by upregulating the squamous cell carcinoma antigens SerpinB3/B4. Nat. Commun. 2014, 5, 3729. [Google Scholar] [CrossRef] [PubMed]
- Sheshadri, N.; Catanzaro, J.M.; Bott, A.J.; Sun, Y.; Ullman, E.; Chen, E.I.; Pan, J.A.; Wu, S.; Crawford, H.C.; Zhang, J.; et al. SCCA1/SERPINB3 promotes oncogenesis and epithelial-mesenchymal transition via the unfolded protein response and IL6 signaling. Cancer Res. 2014, 74, 6318–6329. [Google Scholar] [CrossRef] [PubMed]
- Turato, C.; Buendia, M.A.; Fabre, M.; Redon, M.J.; Branchereau, S.; Quarta, S.; Ruvoletto, M.; Perilongo, G.; Grotzer, M.A.; Gatta, A.; et al. Over-expression of SERPINB3 in hepatoblastoma: A possible insight into the genesis of this tumour? Eur. J. Cancer 2012, 48, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Turato, C.; Vitale, A.; Fasolato, S.; Ruvoletto, M.; Terrin, L.; Quarta, S.; Ramirez Morales, R.; Biasiolo, A.; Zanus, G.; Zali, N.; et al. SERPINB3 is associated with TGF-beta1 and cytoplasmic beta-catenin expression in hepatocellular carcinomas with poor prognosis. Br. J. Cancer 2014, 110, 2708–2715. [Google Scholar] [CrossRef] [PubMed]
- Shamji, M.H.; Temblay, J.N.; Cheng, W.; Byrne, S.M.; Macfarlane, E.; Switzer, A.R.; Francisco, N.D.C.; Olexandra, F.; Jacubczik, F.; Durham, S.R.; et al. Antiapoptotic serine protease inhibitors contribute to survival of allergenic TH2 cells. J. Allergy Clin. Immunol. 2018, 142, 569–581.e565. [Google Scholar] [CrossRef] [PubMed]
- Sivaprasad, U.; Kinker, K.G.; Ericksen, M.B.; Lindsey, M.; Gibson, A.M.; Bass, S.A.; Hershey, N.S.; Deng, J.; Medvedovic, M.; Khurana Hershey, G.K. SERPINB3/B4 contributes to early inflammation and barrier dysfunction in an experimental murine model of atopic dermatitis. J. Investig. Dermatol. 2015, 135, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Vidalino, L.; Doria, A.; Quarta, S.; Zen, M.; Gatta, A.; Pontisso, P. SERPINB3, apoptosis and autoimmunity. Autoimmun. Rev. 2009, 9, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Riaz, N.; Havel, J.J.; Kendall, S.M.; Makarov, V.; Walsh, L.A.; Desrichard, A.; Weinhold, N.; Chan, T.A. Recurrent SERPINB3 and SERPINB4 mutations in patients who respond to anti-CTLA4 immunotherapy. Nat. Genet. 2016, 48, 1327–1329. [Google Scholar] [CrossRef] [PubMed]
- Iversen, O.J.; Lysvand, H.; Slupphaug, G. Pso p27, a SERPINB3/B4-derived protein, is most likely a common autoantigen in chronic inflammatory diseases. Clin. Immunol. 2017, 174, 10–17. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, H. Squamous Cell Carcinoma Antigen: Clinical Application and Research Status. Diagnostics 2022, 12, 1065. https://doi.org/10.3390/diagnostics12051065
Zhu H. Squamous Cell Carcinoma Antigen: Clinical Application and Research Status. Diagnostics. 2022; 12(5):1065. https://doi.org/10.3390/diagnostics12051065
Chicago/Turabian StyleZhu, Huange. 2022. "Squamous Cell Carcinoma Antigen: Clinical Application and Research Status" Diagnostics 12, no. 5: 1065. https://doi.org/10.3390/diagnostics12051065
APA StyleZhu, H. (2022). Squamous Cell Carcinoma Antigen: Clinical Application and Research Status. Diagnostics, 12(5), 1065. https://doi.org/10.3390/diagnostics12051065