
Posterior Fossa Tumours in the First Year of Life: A Two-Centre Retrospective Study

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Management of Hydrocephalus
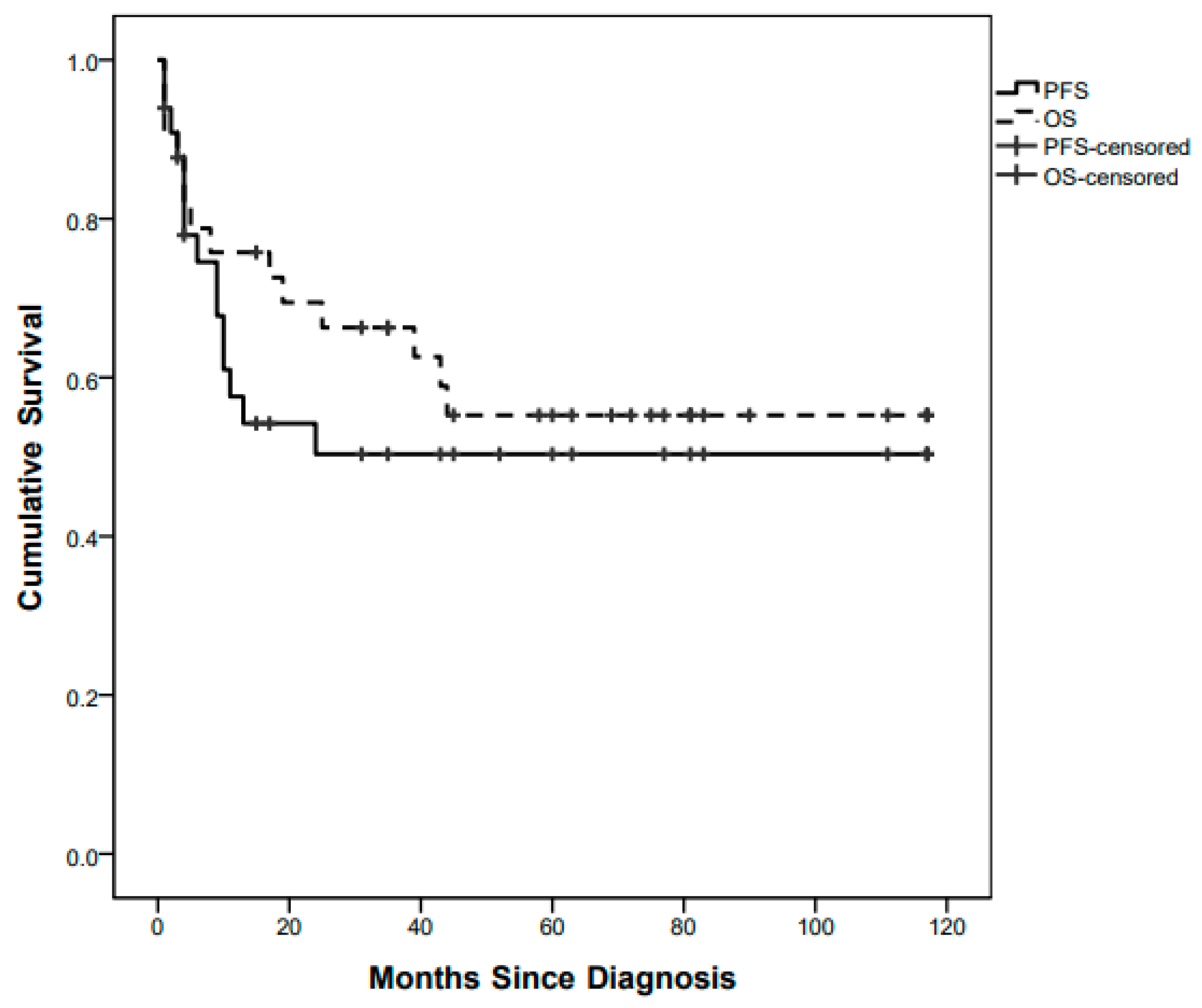
3.2. Survival Outcome
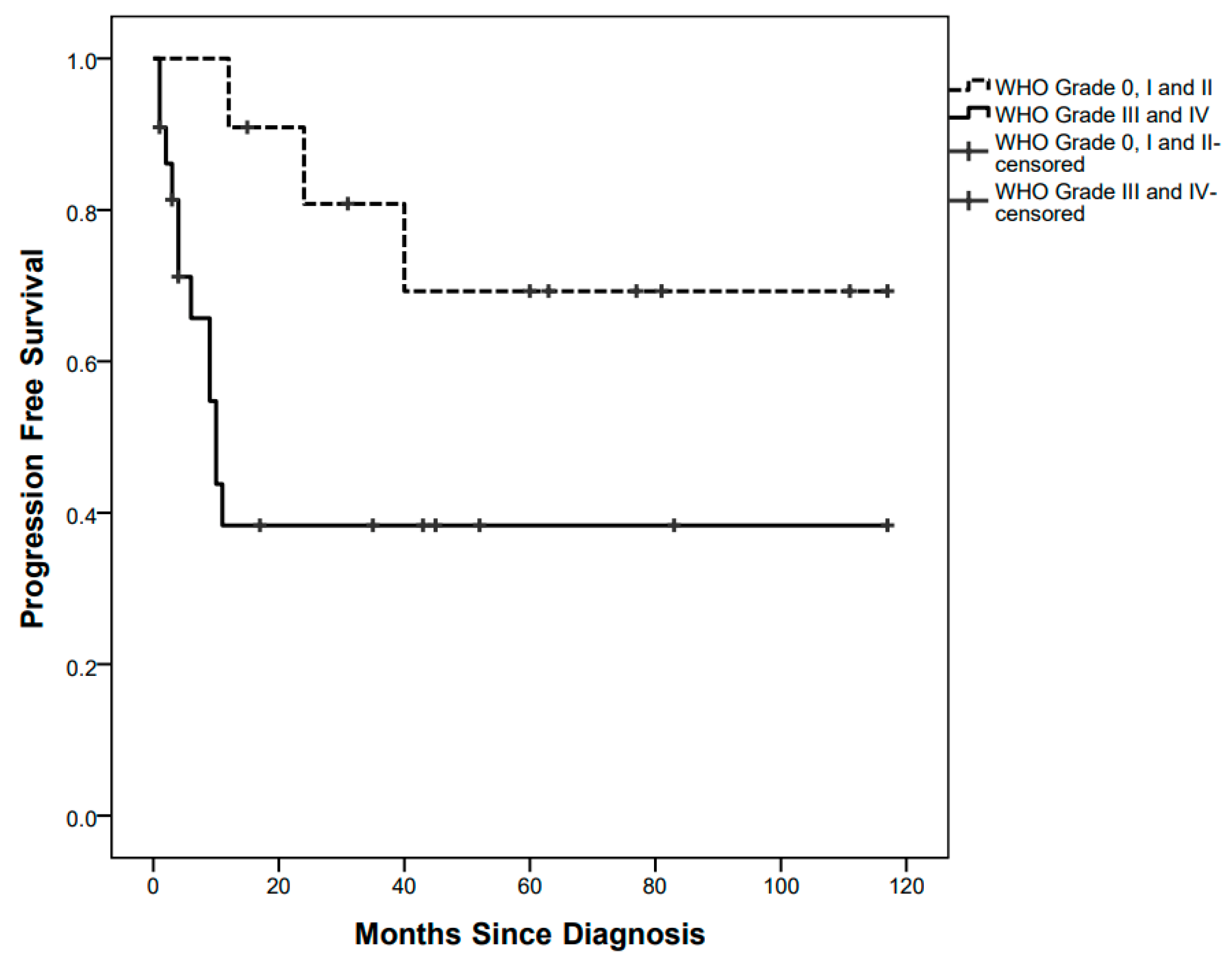
3.3. Treatment Details and Outcome Stratified by WHO Grade
3.3.1. Grade 0 (One Patient)
3.3.2. Grade I (Eight Patients)
3.3.3. Grade II (Two Patients)
3.3.4. Grade III (Five Patients)
3.3.5. Grade IV (17 Patients)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stiller, C.A.; Bayne, A.M.; Chakrabarty, A.; Kenny, T.; Chumas, P. Incidence of childhood CNS tumours in Britain and variation in rates by definition of malignant behaviour: Population-based study. BMC Cancer 2019, 19, 139. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.; Naushahi, M.; Bernard, A.; Campbell, R. Epidemiology of paediatric central nervous system tumours in Queensland, Australia. J. Clin. Neurosci. 2021, 92, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014–2018. Neuro-Oncology 2021, 23, iii1–iii105. [Google Scholar] [CrossRef]
- Lannering, B.; Sandström, P.-E.; Holm, S.; Lundgren, J.; Pfeifer, S.; Samuelsson, U.; Strömberg, B.; Gustafsson, G.; Swedish Childhood CNS Tumor Working Group (VCTB). Classification, incidence and survival analyses of children with CNS tumours diagnosed in Sweden 1984-2005. Acta Paediatr. 2009, 98, 1620–1627. [Google Scholar] [CrossRef] [PubMed]
- Arora, R.S.; Alston, R.D.; Eden, T.O.B.; Estlin, E.J.; Moran, A.; Birch, J.M. Age-incidence patterns of primary CNS tumors in children, adolescents, and adults in England. Neuro-Oncology 2009, 11, 403–413. [Google Scholar] [CrossRef]
- Bishop, A.J.; McDonald, M.W.; Chang, A.L.; Esiashvili, N. Infant brain tumors: Incidence, survival, and the role of radiation based on Surveillance, Epidemiology, and End Results (SEER) Data. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 341–347. [Google Scholar] [CrossRef]
- Alves, C.A.P.F.; Löbel, U.; Martin-Saavedra, J.S.; Toescu, S.; Tsunemi, M.H.; Teixeira, S.R.; Mankad, K.; Hargrave, D.; Jacques, T.S.; da Costa Leite, C.; et al. A diagnostic algorithm for posterior fossa tumors in children: A validation study. AJNR Am. J. Neuroradiol. 2021, 42, 961–968. [Google Scholar] [CrossRef]
- Al-Hussaini, M.; Swaidan, M.; Al-Jumaily, U.; Musharbash, A. Central nervous system tumors in the first year of life: A clinical and pathologic experience from a single cancer center. Childs Nerv. Syst. 2013, 29, 1883–1891. [Google Scholar] [CrossRef]
- Mehrotra, N.; Shamji, M.F.; Vassilyadi, M.; Ventureyra, E.C.G. Intracranial tumors in first year of life: The CHEO experience. Childs Nerv. Syst. 2009, 25, 1563–1569. [Google Scholar] [CrossRef]
- Ceglie, G.; Vinci, M.; Carai, A.; Rossi, S.; Colafati, G.S.; Cacchione, A.; Tornesello, A.; Miele, E.; Locatelli, F.; Mastronuzzi, A. Infantile/Congenital High-Grade Gliomas: Molecular Features and Therapeutic Perspectives. Diagnostics 2020, 10, 648. [Google Scholar] [CrossRef]
- Simone, V.; Rizzo, D.; Cocciolo, A.; Caroleo, A.M.; Carai, A.; Mastronuzzi, A.; Tornesello, A. Infantile brain tumors: A review of literature and future perspectives. Diagnostics 2021, 11, 670. [Google Scholar] [CrossRef] [PubMed]
- Jaing, T.-H.; Wu, C.-T.; Chen, S.-H.; Hung, P.-C.; Lin, K.-L.; Jung, S.-M.; Tseng, C.-K. Intracranial tumors in infants: A single institution experience of 22 patients. Childs Nerv. Syst. 2011, 27, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Goethe, E.A.; Gadgil, N.; Stormes, K.; Wassef, A.; LoPresti, M.; Lam, S. Predicting dysphagia in children undergoing surgery for posterior fossa tumors. Childs Nerv. Syst. 2020, 36, 925–931. [Google Scholar] [CrossRef]
- Fąfara-Leś, A.; Kwiatkowski, S.; Maryńczak, L.; Kawecki, Z.; Adamek, D.; Herman-Sucharska, I.; Kobylarz, K. Torticollis as a first sign of posterior fossa and cervical spinal cord tumors in children. Childs Nerv. Syst. 2014, 30, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Hicks, D.; Rafiee, G.; Schwalbe, E.C.; Howell, C.I.; Lindsey, J.C.; Hill, R.M.; Smith, A.J.; Adidharma, P.; Steel, C.; Richardson, S.; et al. The molecular landscape and associated clinical experience in infant medulloblastoma: Prognostic significance of second-generation subtypes. Neuropathol. Appl. Neurobiol. 2021, 47, 236–250. [Google Scholar] [CrossRef]
- Lu, V.M.; Di, L.; Eichberg, D.G.; Luther, E.M.; Shah, A.H.; Daniels, D.J.; Maher, O.M.; Niazi, T.N. Age of diagnosis clinically differentiates Atypical Teratoid/Rhabdoid Tumors diagnosed below age of 3 years: A database study. Childs Nerv. Syst. 2021, 37, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Hill, R.M.; Richardson, S.; Schwalbe, E.C.; Hicks, D.; Lindsey, J.C.; Crosier, S.; Rafiee, G.; Grabovska, Y.; Wharton, S.B.; Jacques, T.S.; et al. Time, pattern, and outcome of medulloblastoma relapse and their association with tumour biology at diagnosis and therapy: A multicentre cohort study. Lancet Child Adolesc. Health 2020, 4, 865–874. [Google Scholar] [CrossRef]
- Faltermeier, C.; Chai, T.; Syed, S.; Lau, N.; Elkaim, L.; Ibrahim, G.; Wang, A.; Weil, A.; Bendel, A.; Fallah, A.; et al. Survival of infants ≤ 24 months of age with brain tumors: A population-based study using the SEER database. PLoS ONE 2019, 14, e0223051. [Google Scholar] [CrossRef]
- Spennato, P.; Nicosia, G.; Quaglietta, L.; Donofrio, V.; Mirone, G.; Di Martino, G.; Guadagno, E.; del Basso de Caro, M.L.; Cascone, D.; Cinalli, G. Posterior fossa tumors in infants and neonates. Childs Nerv. Syst. 2015, 31, 1751–1772. [Google Scholar] [CrossRef]
- Klein, O.; Boussard, N.; Guerbouz, R.; Helleringer, M.; Joud, A.; Puget, S. Surgical approach to the posterior fossa in children, including anesthetic considerations and complications: The prone and the sitting position. Technical note. Neurochirurgie 2021, 67, 46–51. [Google Scholar] [CrossRef]
- Gnekow, A.K.; Walker, D.A.; Kandels, D.; Picton, S.; Perilongo, G.; Grill, J.; Stokland, T.; Sandstrom, P.E.; Warmuth-Metz, M.; Pietsch, T.; et al. A European randomised controlled trial of the addition of etoposide to standard vincristine and carboplatin induction as part of an 18-month treatment programme for childhood (≤16 years) low grade glioma—A final report. Eur. J. Cancer 2017, 81, 206–225. [Google Scholar] [CrossRef] [PubMed]
- Ritzmann, T.A.; Chapman, R.J.; Kilday, J.-P.; Thorp, N.; Modena, P.; Dineen, R.A.; Macarthur, D.; Mallucci, C.; Jaspan, T.; Pajtler, K.W.; et al. SIOP Ependymoma I: Final results, long term follow-up and molecular analysis of the trial cohort: A BIOMECA Consortium Study. Neuro-Oncology, 2022; Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Massimino, M.; Miceli, R.; Giangaspero, F.; Boschetti, L.; Modena, P.; Antonelli, M.; Ferroli, P.; Bertin, D.; Pecori, E.; Valentini, L.; et al. Final results of the second prospective AIEOP protocol for pediatric intracranial ependymoma. Neuro-Oncology 2016, 18, 1451–1460. [Google Scholar] [CrossRef] [PubMed]
- Seeringer, A.; Bartelheim, K.; Kerl, K.; Hasselblatt, M.; Leuschner, I.; Rutkowski, S.; Timmermann, B.; Kortmann, R.D.; Koscielniak, E.; Schneppenheim, R.; et al. Feasibility of intensive multimodal therapy in infants affected by rhabdoid tumors—Experience of the EU-RHAB registry. Klin. Padiatr. 2014, 226, 143–148. [Google Scholar] [CrossRef]
- Rivera-Luna, R.; Medina-Sanson, A.; Leal-Leal, C.; Pantoja-Guillen, F.; Zapata-Tarrés, M.; Cardenas-Cardos, R.; Barrera-Gómez, R.; Rueda-Franco, F. Brain tumors in children under 1 year of age: Emphasis on the relationship of prognostic factors. Childs Nerv. Syst. 2003, 19, 311–314. [Google Scholar] [CrossRef]
- Lopez-Rivera, V.; Dono, A.; Abdelkhaleq, R.; Sheth, S.A.; Chen, P.R.; Chandra, A.; Ballester, L.Y.; Esquenazi, Y. Treatment trends and overall survival in patients with grade II/III ependymoma: The role of tumor grade and location. Clin. Neurol. Neurosurg. 2020, 199, 106282. [Google Scholar] [CrossRef]
- Aras, Y.; Dölen, D.; İribasÇelik, A.; Kılıç, G.; Kebudi, R.; Ünverengil, G.; Sabancı, P.A.; İzgi, A.N. Effects of different molecular subtypes and tumor biology on the prognosis of medulloblastoma. Childs Nerv. Syst. 2021, 37, 3733–3742. [Google Scholar] [CrossRef]
- Qin, Q.; Huang, D.; Jiang, Y. Survival difference between brainstem and cerebellum medulloblastoma: The surveillance, epidemiology, and end results-based study. Medicine 2020, 99, e22366. [Google Scholar] [CrossRef]
- Klimo, P.; Nesvick, C.L.; Broniscer, A.; Orr, B.A.; Choudhri, A.F. Malignant brainstem tumors in children, excluding diffuse intrinsic pontine gliomas. J. Neurosurg. Pediatr. 2016, 17, 57–65. [Google Scholar] [CrossRef]
- Totapally, B.R.; Shah, A.H.; Niazi, T. Epidemiology and short-term surgical outcomes of children presenting with cerebellar tumors. Clin. Neurol. Neurosurg. 2018, 168, 97–101. [Google Scholar] [CrossRef]
- Toescu, S.M.; James, G.; Phipps, K.; Jeelani, O.; Thompson, D.; Hayward, R.; Aquilina, K. Intracranial neoplasms in the first year of life: Results of a third cohort of patients from a single institution. Neurosurgery 2019, 84, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Lassaletta, A.; Bouffet, E.; Mabbott, D.; Kulkarni, A.V. Functional and neuropsychological late outcomes in posterior fossa tumors in children. Childs Nerv. Syst. 2015, 31, 1877–1890. [Google Scholar] [CrossRef] [PubMed]
- Charalambides, C.; Dinopoulos, A.; Sgouros, S. Neuropsychological sequelae and quality of life following treatment of posterior fossa ependymomas in children. Childs Nerv. Syst. 2009, 25, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Lassaletta, A. Medulloblastoma in infants: The never-ending challenge. Lancet Oncol. 2018, 19, 720–721. [Google Scholar] [CrossRef]
- Baliga, S.; Gandola, L.; Timmermann, B.; Gail, H.; Padovani, L.; Janssens, G.O.; Yock, T.I. Brain tumors: Medulloblastoma, ATRT, ependymoma. Pediatr. Blood Cancer 2021, 68 (Suppl. 2), e28395. [Google Scholar] [CrossRef]
- Due-Tønnessen, B.J.; Helseth, E. Management of hydrocephalus in children with posterior fossa tumors: Role of tumor surgery. Pediatr. Neurosurg. 2007, 43, 92–96. [Google Scholar] [CrossRef]
- Sainte-Rose, C.; Cinalli, G.; Roux, F.E.; Maixner, R.; Chumas, P.D.; Mansour, M.; Carpentier, A.; Bourgeois, M.; Zerah, M.; Pierre-Kahn, A.; et al. Management of hydrocephalus in pediatric patients with posterior fossa tumors: The role of endoscopic third ventriculostomy. J. Neurosurg. 2001, 95, 791–797. [Google Scholar] [CrossRef]
- Ruggiero, C.; Cinalli, G.; Spennato, P.; Aliberti, F.; Cianciulli, E.; Trischitta, V.; Maggi, G. Endoscopic third ventriculostomy in the treatment of hydrocephalus in posterior fossa tumors in children. Childs Nerv. Syst. 2004, 20, 828–833. [Google Scholar] [CrossRef]
- Habib, H.A.M. Intraoperative precautionary insertion of external ventricular drainage catheters in posterior fossa tumors presenting with hydrocephalus. Alex. J. Med. 2014, 50, 333–340. [Google Scholar] [CrossRef][Green Version]
- El-Gaidi, M.A.; El-Nasr, A.H.A.; Eissa, E.M. Infratentorial complications following preresection CSF diversion in children with posterior fossa tumors. J. Neurosurg. Pediatr. 2015, 15, 4–11. [Google Scholar] [CrossRef]
- Kirkman, M.A.; Hayward, R.; Phipps, K.; Aquilina, K. Surgical decision-making in the management of childhood tumors of the CNS disseminated at presentation. J. Neurosurg. Pediatr. 2018, 21, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Elkatatny, A.M.; Zurakowski, D.; Goumnerova, L. 352 management strategies for hydrocephalus in pediatric posterior fossa brain tumor. Neurosurgery 2018, 65, 140. [Google Scholar] [CrossRef]
- Helmbold, L.J.; Kammler, G.; Regelsberger, J.; Fritzsche, F.S.; Emami, P.; Schüller, U.; Krajewski, K. Predictive factors associated with ventriculoperitoneal shunting after posterior fossa tumor surgery in children. Childs Nerv. Syst. 2019, 35, 779–788. [Google Scholar] [CrossRef]
- Pilotto, C.; Liguoro, I.; Scaravetti, S.; Passone, E.; D’Agostini, S.; Tuniz, F.; Skrap, M.; Cogo, P. Risk Factors of Persistent Hydrocephalus in Children with Brain Tumor: A Retrospective Analysis. Pediatr. Neurosurg. 2021, 56, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Pitsika, M.; Fletcher, J.; Coulter, I.C.; Cowie, C.J.A. A validation study of the modified Canadian Preoperative Prediction Rule for Hydrocephalus in children with posterior fossa tumors. J. Neurosurg. Pediatr. 2021, 28, 121–127. [Google Scholar] [CrossRef]
- Paunović, A.; Milisavljević, F.; Bošković, J. Evaluation of clinical characteristics as indicators for shunt procedure in patients with medulloblastoma: PS210. Porto Biomed. J. 2017, 2, 240–241. [Google Scholar] [CrossRef]
- Lin, C.-T.; Riva-Cambrin, J.K. Management of posterior fossa tumors and hydrocephalus in children: A review. Childs Nerv. Syst. 2015, 31, 1781–1789. [Google Scholar] [CrossRef] [PubMed]
- Ben Zvi, I.; Adegboyega, G.; Toescu, S.M.; Schwartz, N.; Kershenovich, A.; Toledano, H.; Michowiz, S.; Aquilina, K. Postoperative hydrocephalus management may cause delays in adjuvant treatment following paediatric posterior fossa tumour resection: A multicentre retrospective observational study. Childs Nerv. Syst. 2022, 38, 311–317. [Google Scholar] [CrossRef]
- Foreman, P.; McClugage, S.; Naftel, R.; Griessenauer, C.J.; Ditty, B.J.; Agee, B.S.; Riva-Cambrin, J.; Wellons, J. Validation and modification of a predictive model of postresection hydrocephalus in pediatric patients with posterior fossa tumors. J. Neurosurg. Pediatr. 2013, 12, 220–226. [Google Scholar] [CrossRef]
- Ghodsi, S.M.; Habibi, Z.; Hanaei, S.; Moradi, E.; Nejat, F. Brain tumors in infants. J. Pediatr. Neurosci. 2015, 10, 335–340. [Google Scholar] [CrossRef]
- Larouche, V.; Huang, A.; Bartels, U.; Bouffet, E. Tumors of the central nervous system in the first year of life. Pediatr. Blood Cancer 2007, 49, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Dhall, G.; O’Neil, S.H.; Ji, L.; Haley, K.; Whitaker, A.M.; Nelson, M.D.; Gilles, F.; Gardner, S.L.; Allen, J.C.; Cornelius, A.S.; et al. Excellent outcome of young children with nodular desmoplasticmedulloblastoma treated on “Head Start” III: A multi-institutional, prospective clinical trial. Neuro-Oncology 2020, 22, 1862–1872. [Google Scholar] [CrossRef] [PubMed]
- Benesch, M.; Bartelheim, K.; Fleischhack, G.; Gruhn, B.; Schlegel, P.G.; Witt, O.; Stachel, K.D.; Hauch, H.; Urban, C.; Quehenberger, F.; et al. High-dose chemotherapy (HDCT) with auto-SCT in children with Atypical Teratoid/Rhabdoid Tumors (AT/RT): A report from the European Rhabdoid Registry (EU-RHAB). Bone Marrow Transplant. 2014, 49, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.J.; Perkins, S.M.; Bradley, J.A.; Mahajan, A.; Marcus, K.J. Radiation therapy for infants with cancer. Pediatr. Blood Cancer 2021, 68 (Suppl. 2), e28700. [Google Scholar] [CrossRef] [PubMed]
- Tartaglione, T.; Izzo, G.; Alexandre, A.; Botto, A.; Di Lella, G.M.; Gaudino, S.; Caldarelli, M.; Colosimo, C. MRI findings of olivary degeneration after surgery for posterior fossa tumours in children: Incidence, time course and correlation with tumour grading. Radiol. Med. 2015, 120, 474–482. [Google Scholar] [CrossRef]
- Grønbæk, J.K.; Wibroe, M.; Toescu, S.; Frič, R.; Thomsen, B.L.; Møller, L.N.; Grillner, P.; Gustavsson, B.; Mallucci, C.; Aquilina, K.; et al. Postoperative speech impairment and surgical approach to posterior fossa tumours in children: A prospective European multicentre cohort study. Lancet Child. Adolesc. Health 2021, 5, 814–824. [Google Scholar] [CrossRef]
- Kulkarni, A.V.; Piscione, J.; Shams, I.; Bouffet, E. Long-term quality of life in children treated for posterior fossa brain tumors. J. Neurosurg. Pediatr. 2013, 12, 235–240. [Google Scholar] [CrossRef]
- Chieffo, D.P.R.; Arcangeli, V.; Moriconi, F.; Zanetti, C.; Frassanito, P.; Bianchi, F.; Massimi, L.; Tamburrini, G. Correlation between Pre- and Post-Surgical Findings for Long-Term Neurocognitive and Behaviour Development Due to Posterior Fossa Pilocytic Astrocytomas: The Trend after 10 Years. Diagnostics 2021, 11, 1489. [Google Scholar] [CrossRef]
- Piscione, P.J.; Bouffet, E.; Mabbott, D.J.; Shams, I.; Kulkarni, A.V. Physical functioning in pediatric survivors of childhood posterior fossa brain tumors. Neuro-Oncology 2014, 16, 147–155. [Google Scholar] [CrossRef]
- Gunn, M.E.; Lähdesmäki, T.; Malila, N.; Arola, M.; Grönroos, M.; Matomäki, J.; Lähteenmäki, P.M. Late morbidity in long-term survivors of childhood brain tumors: A nationwide registry-based study in Finland. Neuro-Oncology 2015, 17, 747–756. [Google Scholar] [CrossRef]
- Cohen-Cutler, S.; Olch, A.; Wong, K.; Malvar, J.; Sposto, R.; Kobierski, P.; Sura, A.; Constine, L.S.; Freyer, D.R. Surveillance for radiation-related late effects in childhood cancer survivors: The impact of using volumetric dosimetry. Cancer Med. 2021, 10, 905–913. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.K.; Mullins, W.A.; O’Neil, S.H.; Wilson, K. Neuropsychological differences between survivors of supratentorial and infratentorial brain tumours. J. Intellect. Disabil. Res. 2011, 55, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Toescu, S.M.; Samarth, G.; Layard Horsfall, H.; Issitt, R.; Margetts, B.; Phipps, K.P.; Jeelani, N.-U.-O.; Thompson, D.N.P.; Aquilina, K. Fourth ventricle tumors in children: Complications and influence of surgical approach. J. Neurosurg. Pediatr. 2020, 27, 52–61. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Picariello, S.; Spennato, P.; Roth, J.; Shimony, N.; Marini, A.; De Martino, L.; Nicosia, G.; Mirone, G.; De Santi, M.S.; Savoia, F.; et al. Posterior Fossa Tumours in the First Year of Life: A Two-Centre Retrospective Study. Diagnostics 2022, 12, 635. https://doi.org/10.3390/diagnostics12030635
Picariello S, Spennato P, Roth J, Shimony N, Marini A, De Martino L, Nicosia G, Mirone G, De Santi MS, Savoia F, et al. Posterior Fossa Tumours in the First Year of Life: A Two-Centre Retrospective Study. Diagnostics. 2022; 12(3):635. https://doi.org/10.3390/diagnostics12030635
Chicago/Turabian StylePicariello, Stefania, Pietro Spennato, Jonathan Roth, Nir Shimony, Alessandra Marini, Lucia De Martino, Giancarlo Nicosia, Giuseppe Mirone, Maria Serena De Santi, Fabio Savoia, and et al. 2022. "Posterior Fossa Tumours in the First Year of Life: A Two-Centre Retrospective Study" Diagnostics 12, no. 3: 635. https://doi.org/10.3390/diagnostics12030635
APA StylePicariello, S., Spennato, P., Roth, J., Shimony, N., Marini, A., De Martino, L., Nicosia, G., Mirone, G., De Santi, M. S., Savoia, F., Errico, M. E., Quaglietta, L., Costantini, S., & Cinalli, G. (2022). Posterior Fossa Tumours in the First Year of Life: A Two-Centre Retrospective Study. Diagnostics, 12(3), 635. https://doi.org/10.3390/diagnostics12030635