
Stability of OCT and OCTA in the Intensive Therapy Unit Setting

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Acquisition Devices
2.3. Scanning Protocol
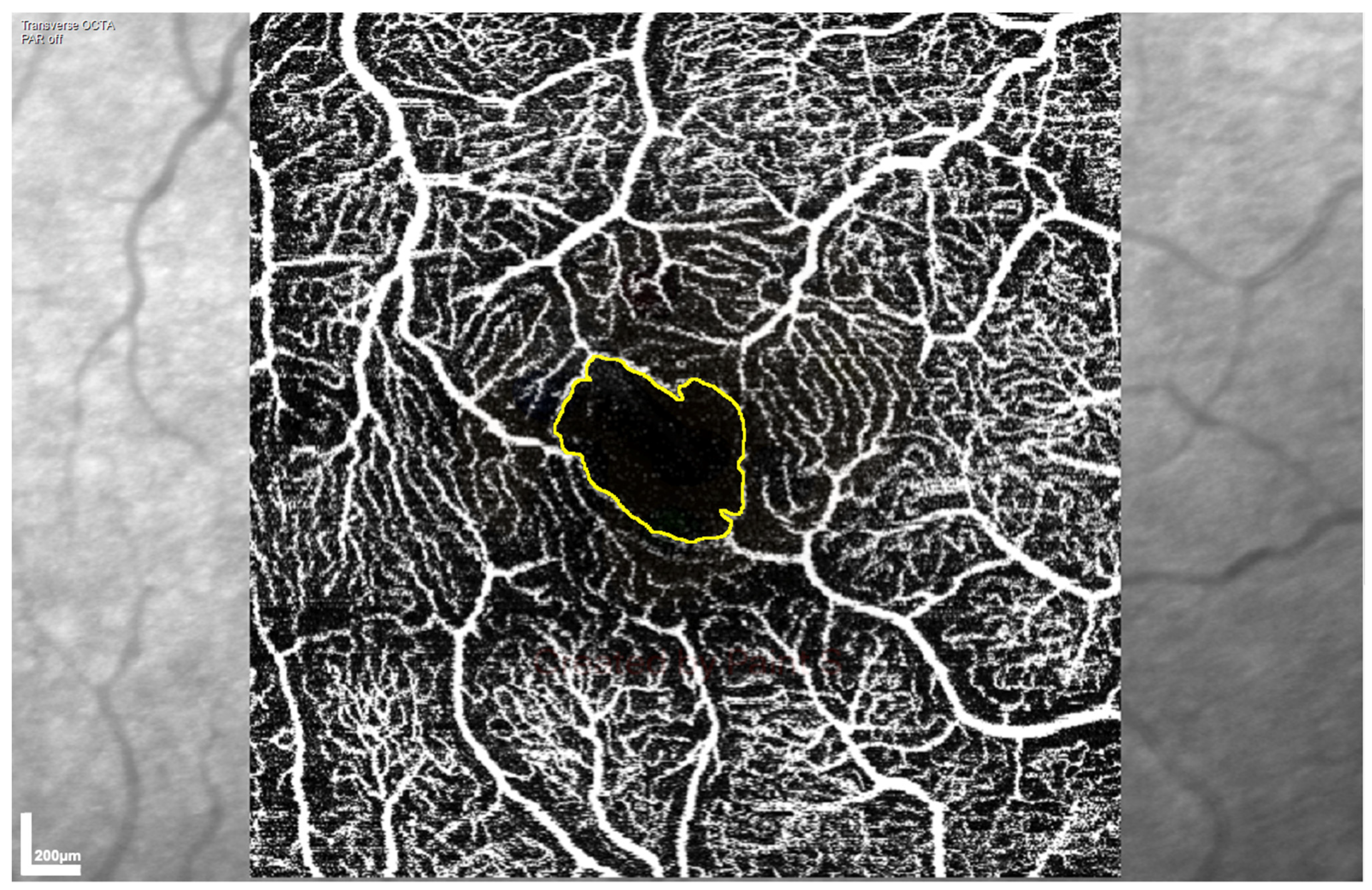
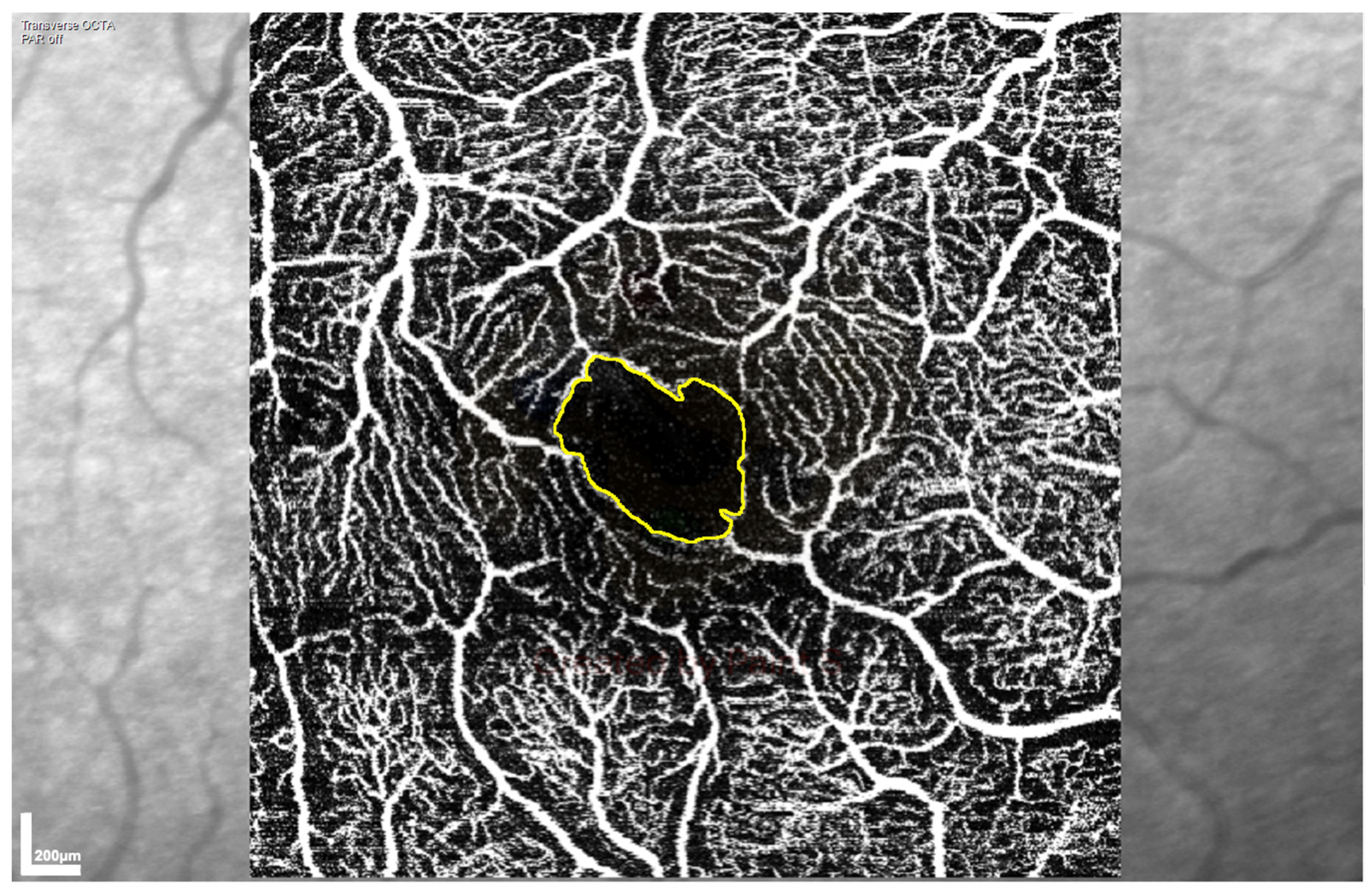
2.4. OCTA Analysis
2.5. RNFL and Macular Ganglion Cell Layer (GCL) Analysis
2.6. Statistics
3. Results
3.1. Agreement of SVP and ICP Measures between Pre- and Post-Op Scans
3.2. Agreement of RNFL, GCL, and Total Retinal Thickness between Pre- and Post-Op Scans
3.3. RNFL Thickness Increased Post-Op
3.4. ICP SFD and GCL Thickness Were Lower in Left than Right Eyes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Adhi, M.; Duker, J.S. Optical coherence tomography--current and future applications. Curr. Opin. Ophthalmol. 2013, 24, 213–221. [Google Scholar] [CrossRef] [Green Version]
- Kashani, A.H.; Chen, C.-L.; Gahm, J.K.; Zheng, F.; Richter, G.M.; Rosenfeld, P.J.; Shi, Y.; Wang, R.K. Optical coherence tomography angiography: A comprehensive review of current methods and clinical applications. Prog. Retin. Eye Res. 2017, 60, 66–100. [Google Scholar] [CrossRef] [PubMed]
- Courtie, E.; Veenith, T.; Logan, A.; Denniston, A.K.; Blanch, R.J. Retinal blood flow in critical illness and systemic disease: A review. Ann. Intensive Care 2020, 10, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Kwapong, W.R.; Ye, H.; Peng, C.; Zhuang, X.; Wang, J.; Shen, M.; Lu, F. Retinal Microvascular Impairment in the Early Stages of Parkinson’s Disease. Investig. Opthalmol. Vis. Sci. 2018, 59, 4115. [Google Scholar] [CrossRef] [Green Version]
- Lad, E.M.; Mukherjee, D.; Stinnett, S.S.; Cousins, S.W.; Potter, G.G.; Burke, J.R.; Farsiu, S.; Whitson, H.E. Evaluation of inner retinal layers as biomarkers in mild cognitive impairment to moderate Alzheimer’s disease. PLoS ONE 2018, 13, e0192646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Querques, G.; Borrelli, E.; Sacconi, R.; De Vitis, L.; Leocani, L.; Santangelo, R.; Magnani, G.; Comi, G.; Bandello, F. Functional and morphological changes of the retinal vessels in Alzheimer’s disease and mild cognitive impairment. Sci. Rep. 2019, 9, 63. [Google Scholar] [CrossRef] [Green Version]
- Patton, N.; Aslam, T.; Macgillivray, T.; Pattie, A.; Deary, I.J.; Dhillon, B. Retinal vascular image analysis as a potential screening tool for cerebrovascular disease: A rationale based on homology between cerebral and retinal microvasculatures. J. Anat. 2005, 206, 319–348. [Google Scholar] [CrossRef]
- Alnawaiseh, M. Evaluation of ocular perfusion in patients with atrial fibrillation using optical coherence tomography angiography. Invest. Ophthalmol. Vis. Sci. 2019, 60, 4570. [Google Scholar]
- Arnould, L.; Guenancia, C. The EYE-MI Pilot Study: A Prospective Acute Coronary Syndrome Cohort Evaluated With Retinal Optical Coherence Tomography Angiography. Investig. Opthalmol. Vis. Sci. 2018, 59, 4299. [Google Scholar] [CrossRef] [Green Version]
- Terheyden, J.H. Impaired retinal capillary perfusion assessed by optical coherence tomography angiography in patients with recent systemic hypertensive crisis. Investig. Ophthalmol. Vis. Sci. 2019, 60, 4573. [Google Scholar]
- Nakayama, L. Retinal Avascular Foveal Zone as an systemic biomarker to evaluate inflammatory bowel disease control. Invest. Ophthalmol. Vis. Sci. 2019, 60, 4572. [Google Scholar] [CrossRef] [Green Version]
- Park, J. Microcirculatory alterations in hemorrhagic shock and sepsis with optical coherence tomography. Crit. Care Med. 2016, 44, 2016. [Google Scholar] [CrossRef]
- Alnawaiseh, M.; Ertmer, C.; Seidel, L.; Arnemann, P.H.; Lahme, L.; Kampmeier, T.-G.; Rehberg, S.W.; Heiduschka, P.; Eter, N.; Hessler, M. Feasibility of optical coherence tomography angiography to assess changes in retinal microcirculation in ovine haemorrhagic shock. Crit. Care 2018, 22, 138. [Google Scholar] [CrossRef] [Green Version]
- Lin, B.R. Characterizing changes in retinal perfusion in high risk pregnancies with optical coherence tomography angiography. Invest. Ophthalmol. Vis. Sci. 2019, 60, 4566. [Google Scholar]
- Helmy, O. Detection of early retinal vascular structural changes of pre-eclamptic patients using optical coherence tomography angiography. Invest. Ophthalmol. Vis. Sci. 2019, 60, 4575. [Google Scholar]
- Bäckman, C.G.; Ahlberg, M. Group meetings after critical illness—Giving and receiving strength. Intensive Crit. Care Nurs. 2018, 46, 86–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aliaga, M.; Forel, J.-M.; De Bourmont, S.; Jung, B.; Thomas, G.; Mahul, M.; Bisbal, M.; Nougaret, S.; Hraiech, S.; Roch, A.; et al. Diagnostic yield and safety of CT scans in ICU. Intensive Care Med. 2015, 41, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Kale, A.U.; Capewell, N.; Talbot, N.; Ahmed, S.; Keane, P.A.; Mollan, S.; Belli, A.; Blanch, R.J.; Veenith, T.; et al. Optical coherence tomography (OCT) in unconscious and systemically unwell patients using a mobile OCT device: A pilot study. BMJ Open 2019, 9, e030882. [Google Scholar] [CrossRef] [Green Version]
- Tan, A.C.S. An overview of the clinical applications of optical coherence tomography angiography. Eye 2018, 32, 262–286. [Google Scholar] [CrossRef] [Green Version]
- Zahid, S.; Dolz-Marco, R.; Freund, K.B.; Balaratnasingam, C.; Dansingani, K.; Gilani, F.; Mehta, N.; Young, E.; Klifto, M.R.; Chae, B.; et al. Fractal dimensional analysis of optical coherence tomography angiography in eyes with diabetic retinopathy. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4940–4947. [Google Scholar] [CrossRef] [PubMed]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria; Available online: https://www.r-project.org/ (accessed on 1 March 2021).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Revelle, W. psych: Procedures for Psychological, Psychometric, and Personality Research. 2020. Available online: https://cran.r-project.org/web/packages/psych/psych.pdf (accessed on 1 March 2021).
- Coscas, F.; Sellam, A.; Glacet-Bernard, A.; Jung, C.; Goudot, M.; Miere, A.; Souied, E.H. Normative data for vascular density in superficial and deep capillary plexuses of healthy adults assessed by optical coherence tomography angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT211–OCT223. [Google Scholar] [CrossRef] [PubMed]
- Venugopal, J.P.; Rao, H.L.; Weinreb, R.N.; Pradhan, Z.S.; Dasari, S.; Riyazuddin, M.; Puttiah, N.K.; Rao, D.A.S.; Devi, S.; Mansouri, K.; et al. Repeatability of vessel density measurements of optical coherence tomography angiography in normal and glaucoma eyes. Br. J. Ophthalmol. 2018, 102, 352–357. [Google Scholar] [CrossRef]
- Fang, D.; Tang, F.Y.; Huang, H.; Cheung, C.Y.; Chen, H. Repeatability, interocular correlation and agreement of quantitative swept-source optical coherence tomography angiography macular metrics in healthy subjects. Br. J. Ophthalmol. 2019, 103, 415–420. [Google Scholar] [CrossRef]
- Eastline, M.; Munk, M.R.; Wolf, S.; Schaal, K.B.; Ebneter, A.; Tian, M.; Giannakaki-Zimmermann, H.; Zinkernagel, M.S. Repeatability of wide-field optical coherence tomography angiography in normal retina. Transl. Vis. Sci. Technol. 2019, 8. [Google Scholar] [CrossRef]
- Al-Sheikh, M.; Tepelus, T.C.; Nazikyan, T.; Sadda, S.R. Repeatability of automated vessel density measurements using optical coherence tomography angiography. Br. J. Ophthalmol. 2017, 101, 449–452. [Google Scholar] [CrossRef]
- Garrity, S.T.; Iafe, N.A.; Phasukkijwatana, N.; Chen, X.; Sarraf, D. Quantitative analysis of three distinct retinal capillary plexuses in healthy eyes using optical coherence tomography angiography. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5548–5555. [Google Scholar] [CrossRef] [Green Version]
- Shahlaee, A.; Pefkianaki, M.; Hsu, J.; Ho, A.C. Measurement of Foveal Avascular Zone Dimensions and its Reliability in Healthy Eyes Using Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2016, 161, 50–55.e1. [Google Scholar] [CrossRef]
- Liu, G.; Keyal, K.; Wang, F. Interocular Symmetry of Vascular Density and Association with Central Macular Thickness of Healthy Adults by Optical Coherence Tomography Angiography. Sci. Rep. 2017, 7, 16297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawji, M.; Flanagan, J. Intraocular and interocular symmetry in normal retinal capillary perfusion. J. Glaucoma 2001, 10, 440–441. [Google Scholar] [CrossRef]
- Shinohara, Y.; Kashima, T.; Akiyama, H.; Shimoda, Y.; Li, D.; Kishi, S. Evaluation of Fundus Blood Flow in Normal Individuals and Patients with Internal Carotid Artery Obstruction Using Laser Speckle Flowgraphy. PLoS ONE 2017, 12, e0169596. [Google Scholar] [CrossRef] [Green Version]
- Landa, G.; Jangi, A.A.; Garcia, P.M.T.; Rosen, R.B. Initial report of quantification of retinal blood flow velocity in normal human subjects using the Retinal Functional Imager (RFI). Int. Ophthalmol. 2012, 32, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Albayrak, R.; Degirmenci, B.; Acar, M.; Haktanir, A.; Colbay, M.; Yaman, M. Doppler sonography evaluation of flow velocity and volume of the extracranial internal carotid and vertebral arteries in healthy adults. J. Clin. Ultrasound 2007, 35, 27–33. [Google Scholar] [CrossRef]
- Burlakoti, A.; Kumaratilake, J.; Taylor, J.; Henneberg, M. Asymmetries of total arterial supply of cerebral hemispheres do not exist. Heliyon 2019, 5, e01086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mwanza, J.C.; Durbin, M.K.; Budenz, D.L. Interocular symmetry in peripapillary retinal nerve fiber layer thickness measured with the cirrus HD-OCT in healthy eyes. Am. J. Ophthalmol. 2011, 151, 514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budenz, D.L. Symmetry between the right and left eyes of the normal retinal nerve fiber layer measured with optical coherence tomography (an AOS thesis). Trans. Am. Ophthalmol. Soc. 2008, 106, 252–275. [Google Scholar] [PubMed]
- Hua, Y.; Voorhees, A.P.; Sigal, I.A. Cerebrospinal fluid pressure: Revisiting factors influencing optic nerve head biomechanics. Investig. Ophthalmol. Vis. Sci. 2018, 59, 154–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardon, L.P.; Cheng, H.; Chettry, P.; Patel, N.B. Optic nerve head morphological changes over 12 hours in seated and head-down tilt postures. Investig. Ophthalmol. Vis. Sci. 2020, 61, 21. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.G.; Mader, T.H.; Gibson, C.R.; Tarver, W.; Rabiei, P.; Riascos, R.F.; Galdamez, L.A.; Brunstetter, T. Spaceflight associated neuro-ocular syndrome (SANS) and the neuro-ophthalmologic effects of microgravity: A review and an update. NPJ Microgravity 2020, 6, 7. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Retinal Vessel Layer | Measure | Timepoint | Mean | 95% Confidence Interval | Standard Error | p Value |
|---|---|---|---|---|---|---|
| Superficial vascular plexus | Skeletal fractal dimension | 1 | 1.602 | 1.584 to 1.621 | 0.009 | 0.08 |
| 2 and 3 | 1.625 | 1.608 to 1.642 | 0.008 | |||
| Skeletal vessel density | 1 | 0.068 | 0.063 to 0.074 | 0.003 | 0.29 | |
| 2 and 3 | 0.072 | 0.067 to 0.077 | 0.002 | |||
| FAZ area (mm2) | 1 | 0.433 | 0.405 to 0.461 | 0.014 | 0.20 | |
| 2 and 3 | 0.408 | 0.382 to 0.434 | 0.013 | |||
| FAZ perimeter (mm) | 1 | 2.678 | 2.565 to 2.791 | 0.056 | 0.53 | |
| 2 and 3 | 2.628 | 2.525 to 2.732 | 0.052 | |||
| Intermediate capillary plexus | Skeletal fractal dimension | 1 | 1.603 | 1.582 to 1.624 | 0.010 | 0.211 |
| 2 and 3 | 1.621 | 1.603 to 1.640 | 0.009 | |||
| Skeletal vessel density | 1 | 0.067 | 0.062 to 0.072 | 0.003 | 0.98 | |
| 2 and 3 | 0.067 | 0.063 to 0.072 | 0.002 | |||
| FAZ area (mm2) | 1 | 0.271 | 0.256 to 0.285 | 0.007 | 0.06 | |
| 2 and 3 | 0.252 | 0.239 to 0.265 | 0.006 | |||
| FAZ perimeter (mm) | 1 | 2.294 | 2.201 to 2.387 | 0.046 | 0.41 | |
| 2 and 3 | 2.242 | 2.158 to 2.325 | 0.042 |
| Retinal Vessel Layer | Measure | Eye | Intraclass Correlation Coefficient | 95% Confidence Interval |
|---|---|---|---|---|
| Superficial vascular plexus | Skeletal fractal dimension | OS | 0.30 | 0.06 to 0.56 |
| OD | 0.22 | −0.01 to 0.49 | ||
| Skeletal vessel density | OS | 0.47 | 0.23 to 0.69 | |
| OD | 0.33 | 0.08 to 0.59 | ||
| FAZ area | OS | 0.86 | 0.75 to 0.93 | |
| OD | 0.81 | 0.67 to 0.91 | ||
| FAZ perimeter | OS | 0.85 | 0.73 to 0.92 | |
| OD | 0.62 | 0.39 to 0.80 | ||
| Intermediate capillary plexus | Skeletal fractal dimension | OS | 0.08 | −0.13 to 0.35 |
| OD | 0.06 | −0.14 to 0.35 | ||
| Skeletal vessel density | OS | 0.33 | 0.09 to 0.59 | |
| OD | 0.12 | −0.10 to 0.41 | ||
| FAZ area | OS | 0.88 | 0.78 to 0.94 | |
| OD | 0.92 | 0.85 to 0.96 | ||
| FAZ perimeter | OS | 0.87 | 0.77 to 0.94 | |
| OD | 0.90 | 0.82 to 0.95 |
| Retinal Layer | Measure | Eye | Intraclass Correlation Coefficient | 95% Confidence Interval |
|---|---|---|---|---|
| Retinal nerve fibre layer | Nasal superior | OS | 0.97 | 0.94 to 0.98 |
| OD | 0.97 | 0.94 to 0.99 | ||
| Nasal | OS | 0.87 | 0.75 to 0.94 | |
| OD | 0.88 | 0.78 to 0.94 | ||
| Nasal inferior | OS | 0.76 | 0.60 to 0.88 | |
| OD | 0.96 | 0.92 to 0.98 | ||
| Temporal inferior | OS | 0.96 | 0.92 to 0.98 | |
| OD | 0.98 | 0.95 to 0.99 | ||
| Temporal | OS | 0.95 | 0.92 to 0.98 | |
| OD | 0.98 | 0.95 to 0.99 | ||
| Temporal superior | OS | 0.99 | 0.98 to 0.99 | |
| OD | 0.81 | 0.68 to 0.91 | ||
| Global | OS | 0.96 | 0.91 to 0.98 | |
| OD | 0.98 | 0.95 to 0.99 | ||
| Ganglion cell layer | Outer superior | OS | 0.90 | 0.68 to 0.96 |
| OD | 0.93 | 0.86 to 0.96 | ||
| Inner superior | OS | 0.61 | 0.39 to 0.78 | |
| OD | 0.81 | 0.67 to 0.91 | ||
| Outer nasal | OS | 0.82 | 0.69 to 0.91 | |
| OD | 0.94 | 0.88 to 0.97 | ||
| Inner nasal | OS | 0.60 | 0.38 to 0.78 | |
| OD | 0.87 | 0.76 to 0.93 | ||
| Outer inferior | OS | 0.78 | 0.63 to 0.89 | |
| OD | 0.91 | 0.84 to 0.96 | ||
| Inner inferior | OS | 0.72 | 0.55 to 0.86 | |
| OD | 0.76 | 0.59 to 0.88 | ||
| Outer temporal | OS | 0.83 | 0.70 to 0.92 | |
| OD | 0.83 | 0.70 to 0.92 | ||
| Inner temporal | OS | 0.55 | 0.33 to 0.75 | |
| OD | 0.67 | 0.47 to 0.83 | ||
| Central | OS | 0.93 | 0.88 to 0.97 | |
| OD | 0.82 | 0.69 to 0.91 |
| Vascular Plexus | Blood Flow Measure | Eye | Mean Value ± Standard Error | OS/OD Difference | p Value |
|---|---|---|---|---|---|
| Superficial vascular plexus | Skeletal fractal dimension | OS | 1.542 ± 0.024 | 0.022 | 0.08 |
| OD | 1.564 ± 0.012 | ||||
| Skeletal vessel density | OS | 0.049 ± 0.007 | 0.005 | 0.14 | |
| OD | 0.054 ± 0.004 | ||||
| FAZ area | OS | 0.344 ± 0.040 | 0.016 | 0.40 | |
| OD | 0.328 ± 0.019 | ||||
| FAZ perimeter | OS | 2.425 ± 0.162 | 0.038 | 0.62 | |
| OD | 2.387 ± 0.076 | ||||
| Intermediate capillary plexus | Skeletal fractal dimension | OS | 1.545 ± 0.027 | 0.028 | 0.05 |
| OD | 1.573 ± 0.014 | ||||
| Skeletal vessel density | OS | 0.051 ± 0.007 | 0.006 | 0.07 | |
| OD | 0.057 ± 0.003 | ||||
| FAZ area | OS | 0.195 ± 0.020 | 0.011 | 0.06 | |
| OD | 0.184 ± 0.010 | ||||
| FAZ perimeter | OS | 2.044 ± 0.129 | 0.167 | 0.01 | |
| OD | 1.877 ± 0.062 |
| Retinal Layer | Location | Eye | Mean Thickness (μm) ± Standard Error | OS/OD Difference (μm) | p Value |
|---|---|---|---|---|---|
| Retinal nerve fibre layer | Nasal superior | OS | 139.759 ± 5.469 | 10.474 | 0.0004 |
| OD | 129.285 ± 2.771 | ||||
| Nasal | OS | 79.998 ± 2.832 | 2.816 | 0.054 | |
| OD | 82.814 ± 1.435 | ||||
| Nasal inferior | OS | 138.714 ± 6.188 | 1.711 | 0.587 | |
| OD | 137.003 ± 3.136 | ||||
| Temporal superior | OS | 138.219 ± 5.808 | 8.790 | 0.004 | |
| OD | 147.009 ± 2.943 | ||||
| Temporal | OS | 68.864 ± 1.839 | 2.737 | 0.005 | |
| OD | 71.601 ± 0.932 | ||||
| Temporal inferior | OS | 148.000 ± 4.418 | 3.290 | 0.147 | |
| OD | 144.710 ± 2.239 | ||||
| Global | OS | 107.942 ± 1.270 | 0.368 | 0.569 | |
| OD | 108.310 ± 0.643 | ||||
| Macular ganglion cell layer | Outer superior | OS | 27.442 ± 0.957 | 1.032 | 0.033 |
| OD | 28.474 ± 0.474 | ||||
| Inner superior | OS | 44.600 ± 1.516 | 0.710 | 0.348 | |
| OD | 45.310 ± 0.751 | ||||
| Outer nasal | OS | 31.320 ± 1.087 | 1.738 | 0.002 | |
| OD | 29.582 ± 0.538 | ||||
| Inner nasal | OS | 42.193 ± 1.800 | 1.499 | 0.097 | |
| OD | 43.692 ± 0.891 | ||||
| Outer inferior | OS | 28.054 ± 1.088 | 0.089 | 0.869 | |
| OD | 27.965 ± 0.539 | ||||
| Inner inferior | OS | 45.432 ± 1.635 | 0.844 | 0.301 | |
| OD | 44.588 ± 0.810 | ||||
| Outer temporal | OS | 31.834 ± 1.291 | 0.771 | 0.233 | |
| OD | 32.605 ± 0.640 | ||||
| Inner temporal | OS | 43.139 ± 1.600 | 1.222 | 0.128 | |
| OD | 41.917 ± 0.793 | ||||
| Central | OS | 20.244 ± 1.047 | 0.690 | 0.188 | |
| OD | 19.554 ± 0.518 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Courtie, E.F.; Kale, A.U.; Hui, B.T.K.; Liu, X.; Capewell, N.I.; Bishop, J.R.B.; Whitehouse, T.; Veenith, T.; Logan, A.; Denniston, A.K.; et al. Stability of OCT and OCTA in the Intensive Therapy Unit Setting. Diagnostics 2021, 11, 1516. https://doi.org/10.3390/diagnostics11081516
Courtie EF, Kale AU, Hui BTK, Liu X, Capewell NI, Bishop JRB, Whitehouse T, Veenith T, Logan A, Denniston AK, et al. Stability of OCT and OCTA in the Intensive Therapy Unit Setting. Diagnostics. 2021; 11(8):1516. https://doi.org/10.3390/diagnostics11081516
Chicago/Turabian StyleCourtie, Ella F., Aditya U. Kale, Benjamin T. K. Hui, Xiaoxuan Liu, Nicholas I. Capewell, Jonathan R. B. Bishop, Tony Whitehouse, Tonny Veenith, Ann Logan, Alastair K. Denniston, and et al. 2021. "Stability of OCT and OCTA in the Intensive Therapy Unit Setting" Diagnostics 11, no. 8: 1516. https://doi.org/10.3390/diagnostics11081516
APA StyleCourtie, E. F., Kale, A. U., Hui, B. T. K., Liu, X., Capewell, N. I., Bishop, J. R. B., Whitehouse, T., Veenith, T., Logan, A., Denniston, A. K., & Blanch, R. J. (2021). Stability of OCT and OCTA in the Intensive Therapy Unit Setting. Diagnostics, 11(8), 1516. https://doi.org/10.3390/diagnostics11081516