
Observation of Chronic Graft-Versus-Host Disease Mouse Model Cornea with In Vivo Confocal Microscopy

 , , , ,
, , , , 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Mice
2.2. Bone Marrow Transplantation
2.3. In Vivo Confocal Microscopy
2.4. Fluorescein Staining on the Ocular Surface
2.5. Cotton Thread Test
2.6. Cell Count in the Cornea
2.7. Histological Analysis
2.8. cGVHD Patients
2.9. Statistical Analysis
3. Results
3.1. The Observation of Mouse Cornea by IVCM
3.1.1. Serial Changes of Corneal Findings Observed by In Vivo Confocal Microscopy
3.1.2. Neovascularization
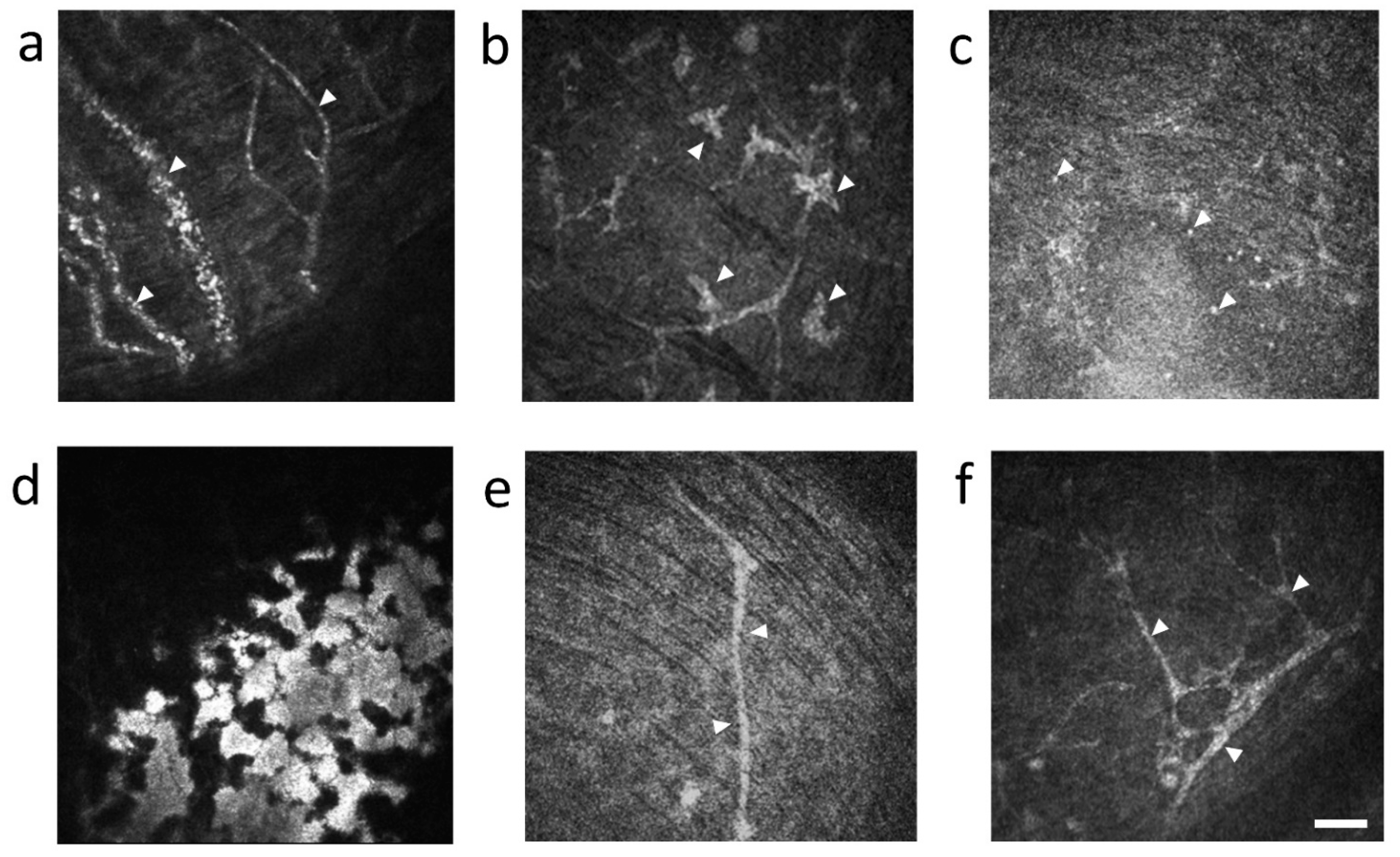
3.1.3. Characteristic Cell Types in the Cornea
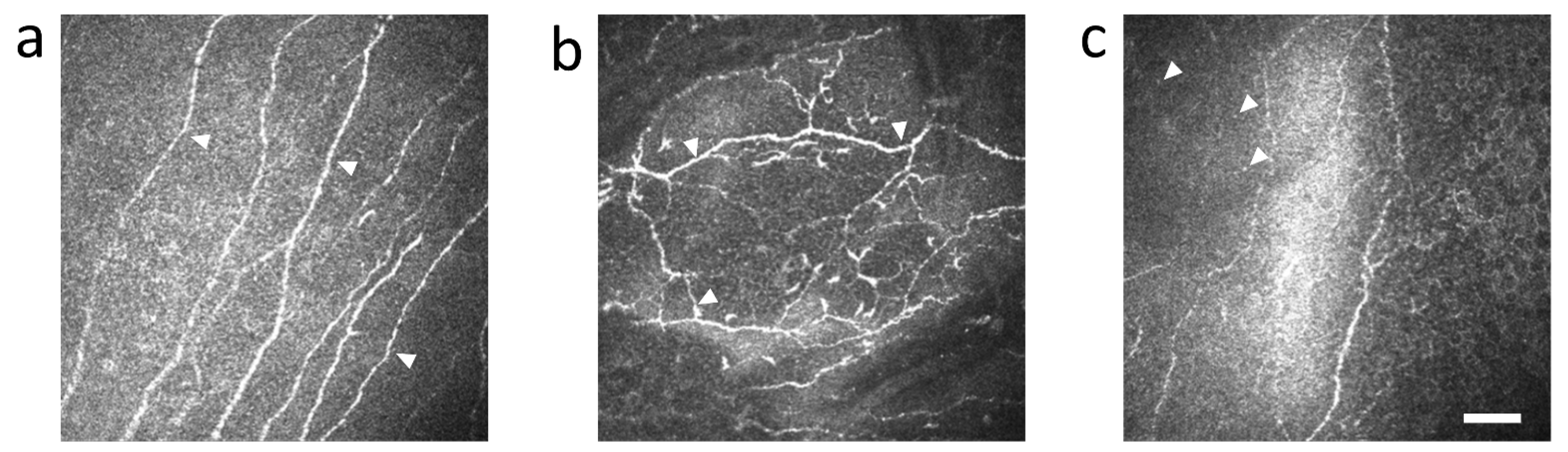
3.1.4. The Change of Nerve Fibers
3.2. Serial Changes of Corneal Fluorescein Staining and Tear Fluid Volume
3.3. Histopathological Findings of Cornea and Lacrimal Gland in Syngeneic and Allogeneic Mice
3.4. cGVHD Patients
4. Discussion
5. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GVHD | Graft-versus-host disease |
| HSCT | Hematopoietic stem cell transplantation |
| BMT | Bone marrow transplantation |
| NIH | National Institute of Health |
| IVCM | In vivo confocal microscopy |
| DED | Dry eye disease |
| RPMI | Roswell Park Memorial Institute |
| ACK | ammonium-chloride-potassium |
| HRT2-RCM | Heidelberg Retina Tomograph 2 Rostock Cornea Module |
| PMMA | poly-methyl-methacrylate |
| CFS | Corneal fluorescein staining |
| HE | Hematoxylin & Eosin |
| NGF | Nerve growth factor |
References
- Jagasia, M.H.; Greinix, H.T.; Arora, M.; Williams, K.M.; Wolff, D.; Cowen, E.W.; Palmer, J.; Weisdorf, D.; Treister, N.S.; Cheng, G.S.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol. Blood Marrow Transplant. 2015, 21, 389–401.e381. [Google Scholar] [CrossRef] [Green Version]
- Sato, S.; Shimizu, E.; He, J.; Ogawa, M.; Asai, K.; Yazu, H.; Rusch, R.; Yamane, M.; Yang, F.; Fukuda, S.; et al. Positive Effects of Oral Antibiotic Administration in Murine Chronic Graft-Versus-Host Disease. Int. J. Mol. Sci. 2021, 22, 3745. [Google Scholar] [CrossRef]
- Hayashi, S.; Shimizu, E.; Uchino, M.; Yazu, H.; Aketa, N.; Tsubota, K.; Ogawa, Y. The Overlap Syndrome: A Case Report of Chronic Graft-Versus-Host Disease after the Development of a Pseudomembrane. Cornea 2020, 40, 1188. [Google Scholar] [CrossRef] [PubMed]
- Zeiser, R.; Blazar, B.R. Pathophysiology of Chronic Graft-versus-Host Disease and Therapeutic Targets. N. Engl. J. Med. 2017, 377, 2565–2579. [Google Scholar] [CrossRef] [PubMed]
- Filipovich, A.H.; Weisdorf, D.; Pavletic, S.; Socie, G.; Wingard, J.R.; Lee, S.J.; Martin, P.; Chien, J.; Przepiorka, D.; Couriel, D.; et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol. Blood Marrow Transplant. 2005, 11, 945–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, Y.; Okamoto, S.; Wakui, M.; Watanabe, R.; Yamada, M.; Yoshino, M.; Ono, M.; Yang, H.Y.; Mashima, Y.; Oguchi, Y.; et al. Dry eye after haematopoietic stem cell transplantation. Br. J. Ophthalmol. 1999, 83, 1125–1130. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, E.; Ogawa, Y.; Saijo, Y.; Yamane, M.; Uchino, M.; Kamoi, M.; Fukui, M.; Yang, F.; He, J.; Mukai, S.; et al. Commensal microflora in human conjunctiva; characteristics of microflora in the patients with chronic ocular graft-versus-host disease. Ocul. Surf. 2019, 17, 265–271. [Google Scholar] [CrossRef]
- Shimizu, E.; Aketa, N.; Yazu, H.; Uchino, M.; Kamoi, M.; Sato, Y.; Tsubota, K.; Ogawa, Y. Corneal higher-order aberrations in eyes with chronic ocular graft-versus-host disease. Ocul. Surf. 2020, 18, 98–107. [Google Scholar] [CrossRef]
- Inamoto, Y.; Valdés-Sanz, N.; Ogawa, Y.; Alves, M.; Berchicci, L.; Galvin, J.; Greinix, H.; Hale, G.A.; Horn, B.; Kelly, D.; et al. Ocular graft-versus-host disease after hematopoietic cell transplantation: Expert review from the Late Effects and Quality of Life Working Committee of the CIBMTR and Transplant Complications Working Party of the EBMT. Bone Marrow Transplant. 2019, 54, 662–673. [Google Scholar] [CrossRef]
- Uchino, M.; Ogawa, Y.; Uchino, Y.; Mori, T.; Okamoto, S.; Tsubota, K. Comparison of stem cell sources in the severity of dry eye after allogeneic haematopoietic stem cell transplantation. Br. J. Ophthalmol. 2012, 96, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Shikari, H.; Antin, J.H.; Dana, R. Ocular graft-versus-host disease: A review. Surv. Ophthalmol. 2013, 58, 233–251. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, A.; Yoshita, T.; Sugiyama, K. In vivo findings of the bulbar/palpebral conjunctiva and presumed meibomian glands by laser scanning confocal microscopy. Cornea 2005, 24, 985–988. [Google Scholar] [CrossRef]
- Sterenczak, K.A.; Stache, N.; Bohn, S.; Allgeier, S.; Köhler, B.; Bartschat, A.; George, C.; Guthoff, R.F.; Stachs, O.; Stachs, A. Burst of Corneal Dendritic Cells during Trastuzumab and Paclitaxel Treatment. Diagnostics 2021, 11, 838. [Google Scholar] [CrossRef]
- Williams, B.M.; Borroni, D.; Liu, R.; Zhao, Y.; Zhang, J.; Lim, J.; Ma, B.; Romano, V.; Qi, H.; Ferdousi, M.; et al. An artificial intelligence-based deep learning algorithm for the diagnosis of diabetic neuropathy using corneal confocal microscopy: A development and validation study. Diabetologia 2020, 63, 419–430. [Google Scholar] [CrossRef] [Green Version]
- He, J.; Ogawa, Y.; Mukai, S.; Saijo-Ban, Y.; Kamoi, M.; Uchino, M.; Yamane, M.; Ozawa, N.; Fukui, M.; Mori, T.; et al. In Vivo Confocal Microscopy Evaluation of Ocular Surface with Graft-Versus-Host Disease-Related Dry Eye Disease. Sci. Rep. 2017, 7, 10720. [Google Scholar] [CrossRef]
- Zhang, Y.; McCormick, L.L.; Desai, S.R.; Wu, C.; Gilliam, A.C. Murine sclerodermatous graft-versus-host disease, a model for human scleroderma: Cutaneous cytokines, chemokines, and immune cell activation. J. Immunol. 2002, 168, 3088–3098. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, E.; Ogawa, Y.; Yazu, H.; Aketa, N.; Yang, F.; Yamane, M.; Sato, Y.; Kawakami, Y.; Tsubota, K. “Smart Eye Camera”: An innovative technique to evaluate tear film breakup time in a murine dry eye disease model. PLoS ONE 2019, 14, e0215130. [Google Scholar] [CrossRef]
- Sung, M.S.; Li, Z.; Cui, L.; Choi, J.S.; Choi, W.; Park, M.J.; Park, S.H.; Yoon, K.C. Effect of Topical 5-Aminoimidazole-4-carboxamide-1-β-d-Ribofuranoside in a Mouse Model of Experimental Dry Eye. Investig. Ophthalmol. Vis. Sci. 2015, 56, 3149–3158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Z.; Liu, X.; Zhou, T.; Wang, Y.; Bai, L.; He, H.; Liu, Z. A mouse dry eye model induced by topical administration of benzalkonium chloride. Mol. Vis. 2011, 17, 257–264. [Google Scholar] [PubMed]
- Yaguchi, S.; Ogawa, Y.; Shimmura, S.; Hatou, S.; Nakamura, S.; Inaba, T.; Imada, T.; Ozawa, Y.; Kawakami, Y.; Ishida, S.; et al. Presence and physiologic function of the renin-angiotensin system in mouse lacrimal gland. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5416–5425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, Y.; Morikawa, S.; Okano, H.; Mabuchi, Y.; Suzuki, S.; Yaguchi, T.; Sato, Y.; Mukai, S.; Yaguchi, S.; Inaba, T.; et al. MHC-compatible bone marrow stromal/stem cells trigger fibrosis by activating host T cells in a scleroderma mouse model. eLife 2016, 5, e09394. [Google Scholar] [CrossRef]
- Yaguchi, S.; Ogawa, Y.; Shimmura, S.; Kawakita, T.; Hatou, S.; Satofuka, S.; Nakamura, S.; Imada, T.; Miyashita, H.; Yoshida, S.; et al. Angiotensin II type 1 receptor antagonist attenuates lacrimal gland, lung, and liver fibrosis in a murine model of chronic graft-versus-host disease. PLoS ONE 2013, 8, e64724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez, R.L.; Perez-Simon, J.A.; Caballero-Velazquez, T.; Flores, T.; Carrancio, S.; Herrero, C.; Blanco, B.; Gutierrez-Cosio, S.; Canete-Campos, C.; Cruz Gonzalez, F.; et al. Limbus damage in ocular graft-versus-host disease. Biol. Blood Marrow Transplant. 2011, 17, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Perez, V.L.; Barsam, A.; Duffort, S.; Urbieta, M.; Barreras, H.; Lightbourn, C.; Komanduri, K.V.; Levy, R.B. Novel Scoring Criteria for the Evaluation of Ocular Graft-versus-Host Disease in a Preclinical Allogeneic Hematopoietic Stem Cell Transplantation Animal Model. Biol. Blood Marrow Transplant. 2016, 22, 1765–1772. [Google Scholar] [CrossRef] [Green Version]
- Yamane, M.; Sato, S.; Shimizu, E.; Shibata, S.; Hayano, M.; Yaguchi, T.; Kamijuku, H.; Ogawa, M.; Suzuki, T.; Mukai, S.; et al. Senescence-associated secretory phenotype promotes chronic ocular graft-vs-host disease in mice and humans. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2020, 34, 10778–10800. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Kim, S.K.; Dana, R.; Clayton, J.; Jain, S.; Rosenblatt, M.I.; Perez, V.L.; Shikari, H.; Riemens, A.; Tsubota, K. International Chronic Ocular Graft-vs-Host-Disease (GVHD) Consensus Group: Proposed diagnostic criteria for chronic GVHD (Part I). Sci. Rep. 2013, 3, 3419. [Google Scholar] [CrossRef] [PubMed]
- Riesner, K.; Shi, Y.; Jacobi, A.; Kräter, M.; Kalupa, M.; McGearey, A.; Mertlitz, S.; Cordes, S.; Schrezenmeier, J.F.; Mengwasser, J.; et al. Initiation of acute graft-versus-host disease by angiogenesis. Blood 2017, 129, 2021–2032. [Google Scholar] [CrossRef] [Green Version]
- Penack, O.; Henke, E.; Suh, D.; King, C.G.; Smith, O.M.; Na, I.K.; Holland, A.M.; Ghosh, A.; Lu, S.X.; Jenq, R.R.; et al. Inhibition of neovascularization to simultaneously ameliorate graft-vs-host disease and decrease tumor growth. J. Natl. Cancer Inst. 2010, 102, 894–908. [Google Scholar] [CrossRef]
- Leonhardt, F.; Grundmann, S.; Behe, M.; Bluhm, F.; Dumont, R.A.; Braun, F.; Fani, M.; Riesner, K.; Prinz, G.; Hechinger, A.K.; et al. Inflammatory neovascularization during graft-versus-host disease is regulated by alphav integrin and miR-100. Blood 2013, 121, 3307–3318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chauhan, S.K.; Dana, R. Role of Th17 cells in the immunopathogenesis of dry eye disease. Mucosal. Immunol. 2009, 2, 375–376. [Google Scholar] [CrossRef] [Green Version]
- Tsubota, K.; Pflugfelder, S.C.; Liu, Z.; Baudouin, C.; Kim, H.M.; Messmer, E.M.; Kruse, F.; Liang, L.; Carreno-Galeano, J.T.; Rolando, M.; et al. Defining Dry Eye from a Clinical Perspective. Int. J. Mol. Sci. 2020, 21, 9271. [Google Scholar] [CrossRef]
- Zhang, M.; Chen, J.; Luo, L.; Xiao, Q.; Sun, M.; Liu, Z. Altered corneal nerves in aqueous tear deficiency viewed by in vivo confocal microscopy. Cornea 2005, 24, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Villani, E.; Galimberti, D.; Viola, F.; Mapelli, C.; Ratiglia, R. The cornea in Sjogren’s syndrome: An in vivo confocal study. Investig. Ophthalmol. Vis. Sci. 2007, 48, 2017–2022. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, J.L.; Cooke, K.R.; Teshima, T. The pathophysiology of acute graft-versus-host disease. Int. J. Hematol. 2003, 78, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Wolff, D.; Radojcic, V.; Lafyatis, R.; Cinar, R.; Rosenstein, R.K.; Cowen, E.W.; Cheng, G.S.; Sheshadri, A.; Bergeron, A.; Williams, K.M.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: IV. The 2020 Highly morbid forms report. Transplant. Cell. Ther. 2021. [Google Scholar] [CrossRef]
- Kitko, C.L.; Pidala, J.; Schoemans, H.M.; Lawitschka, A.; Flowers, M.E.; Cowen, E.W.; Tkaczyk, E.; Farhadfar, N.; Jain, S.; Steven, P.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: IIa. The 2020 Clinical Implementation and Early Diagnosis Working Group Report. Transplant. Cell. Ther. 2021, 27, 545–557. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, S.; Sato, S.; Taniguchi, H.; Shimizu, E.; He, J.; Hayashi, S.; Negishi, K.; Ogawa, Y.; Shimmura, S. Observation of Chronic Graft-Versus-Host Disease Mouse Model Cornea with In Vivo Confocal Microscopy. Diagnostics 2021, 11, 1515. https://doi.org/10.3390/diagnostics11081515
Shimizu S, Sato S, Taniguchi H, Shimizu E, He J, Hayashi S, Negishi K, Ogawa Y, Shimmura S. Observation of Chronic Graft-Versus-Host Disease Mouse Model Cornea with In Vivo Confocal Microscopy. Diagnostics. 2021; 11(8):1515. https://doi.org/10.3390/diagnostics11081515
Chicago/Turabian StyleShimizu, Shota, Shinri Sato, Hiroko Taniguchi, Eisuke Shimizu, Jingliang He, Shunsuke Hayashi, Kazuno Negishi, Yoko Ogawa, and Shigeto Shimmura. 2021. "Observation of Chronic Graft-Versus-Host Disease Mouse Model Cornea with In Vivo Confocal Microscopy" Diagnostics 11, no. 8: 1515. https://doi.org/10.3390/diagnostics11081515
APA StyleShimizu, S., Sato, S., Taniguchi, H., Shimizu, E., He, J., Hayashi, S., Negishi, K., Ogawa, Y., & Shimmura, S. (2021). Observation of Chronic Graft-Versus-Host Disease Mouse Model Cornea with In Vivo Confocal Microscopy. Diagnostics, 11(8), 1515. https://doi.org/10.3390/diagnostics11081515