
18F-Fluciclovine Positron Emission Tomography in Prostate Cancer: A Systematic Review and Diagnostic Meta-Analysis

 ,
,  and
and 
Abstract
1. Introduction
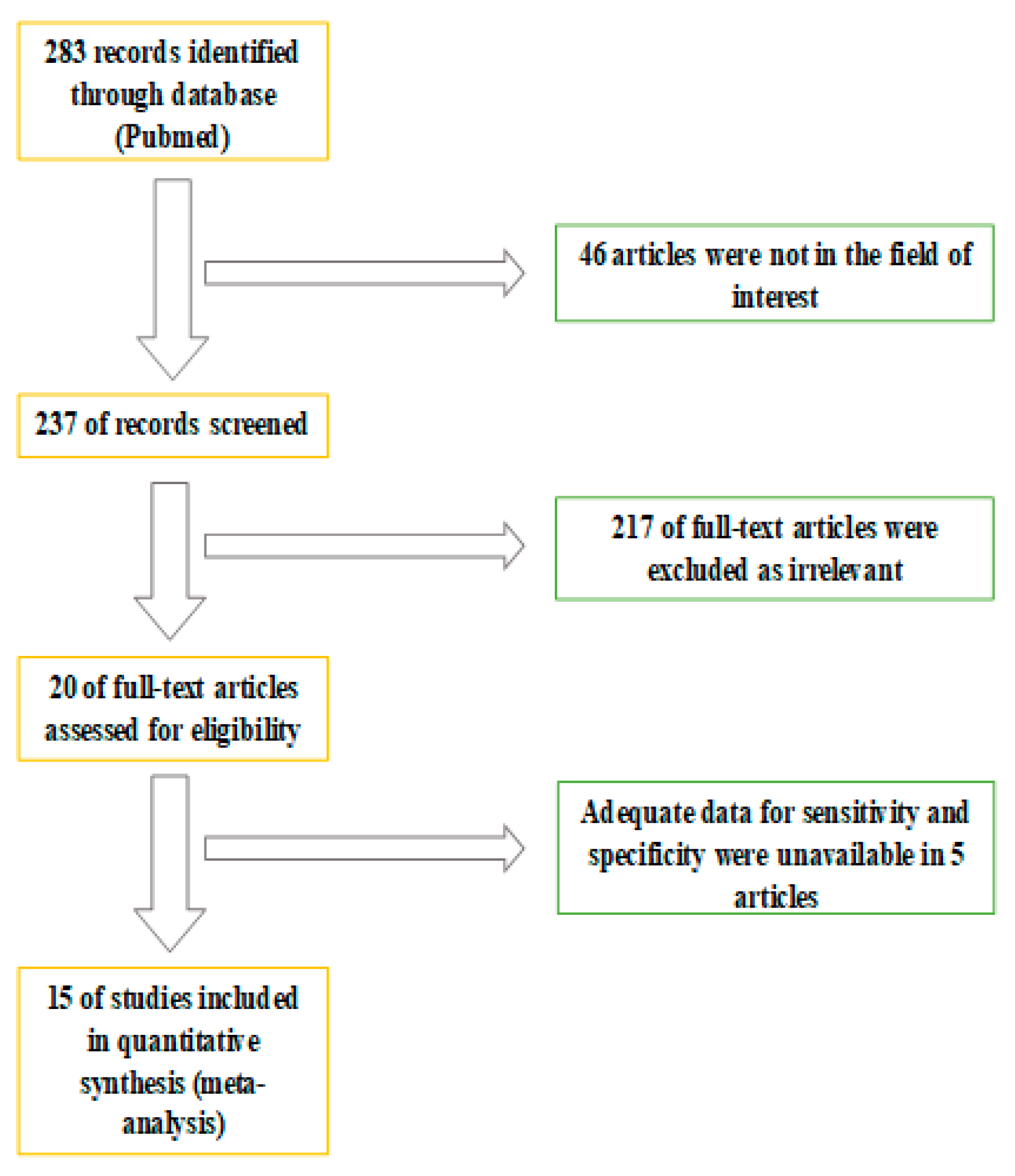
2. Materials and Methods
3. Results
3.1. Patient Population
3.2. Diagnostic Performance of 18F-Fluciclovine PET/CT in Different Clinical Setting
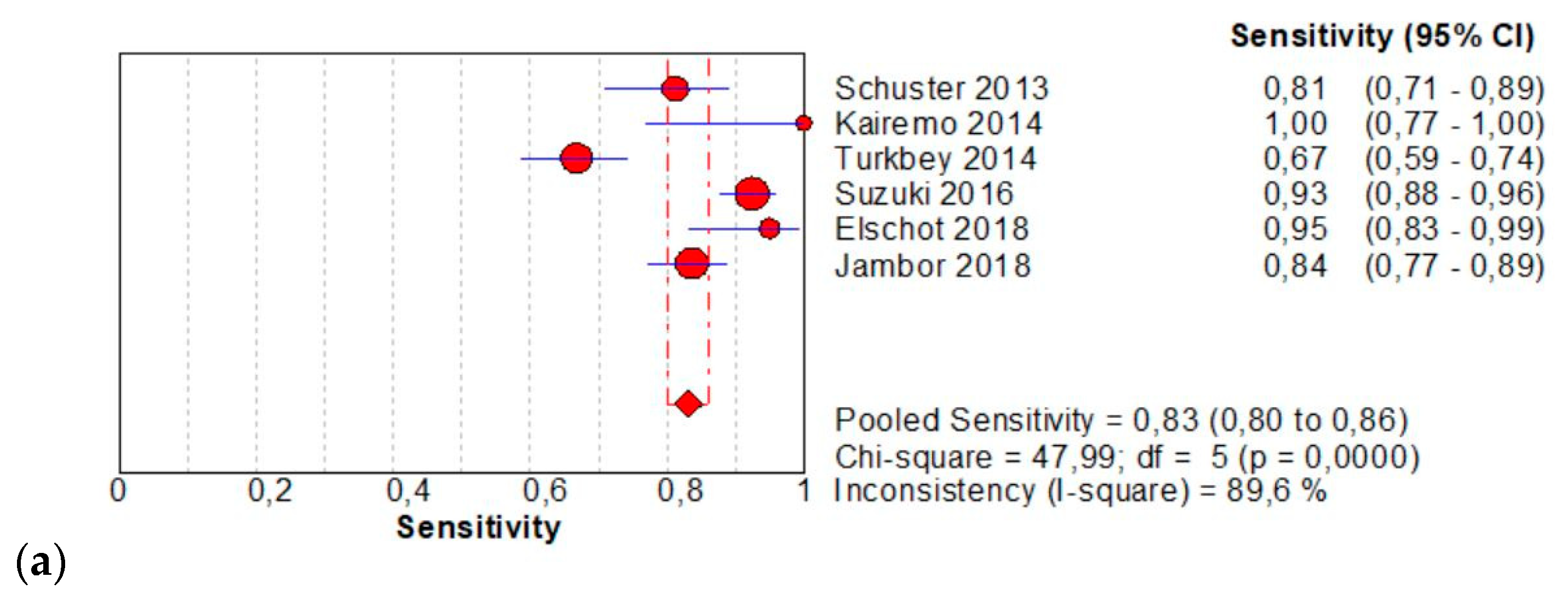
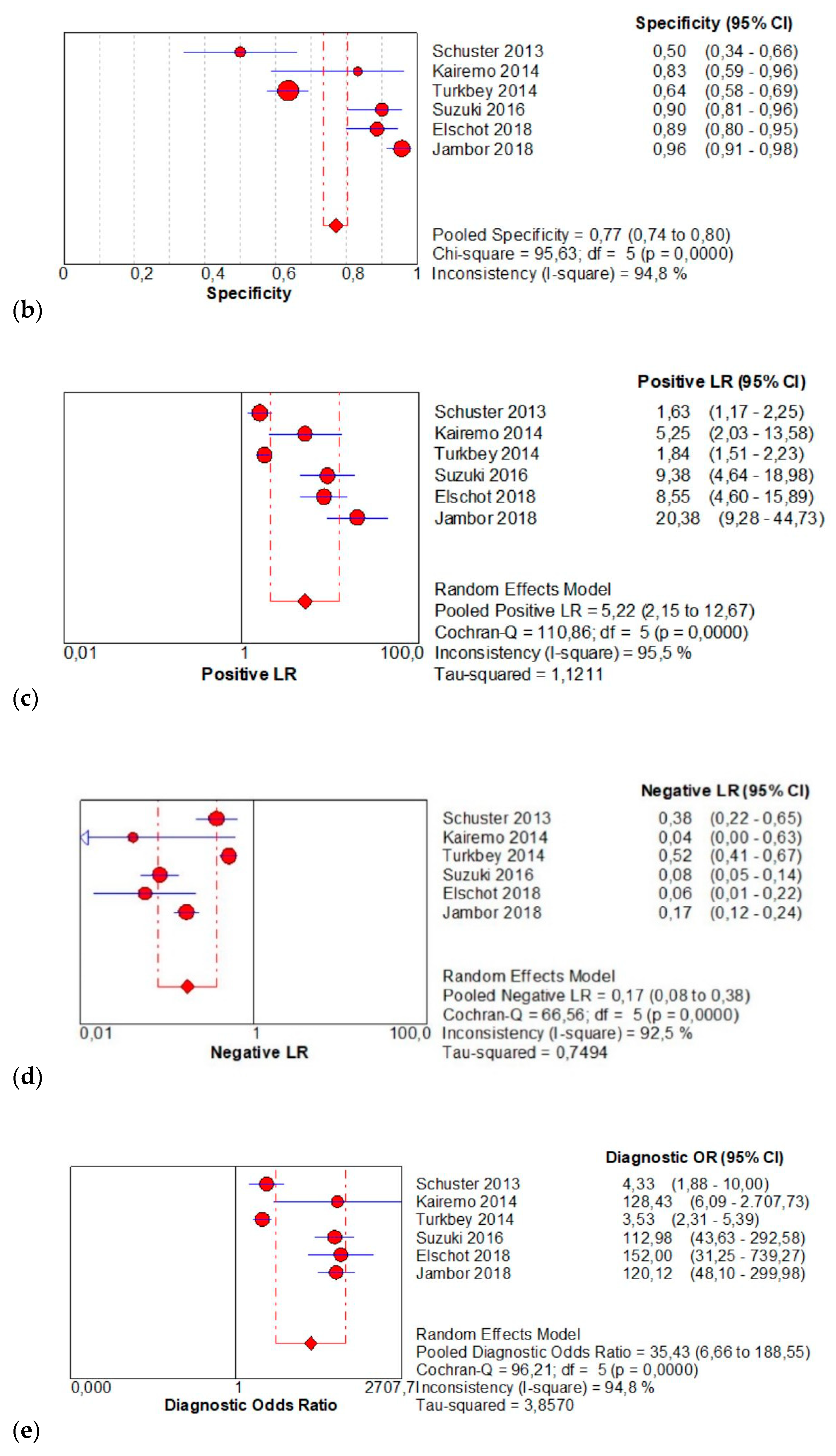
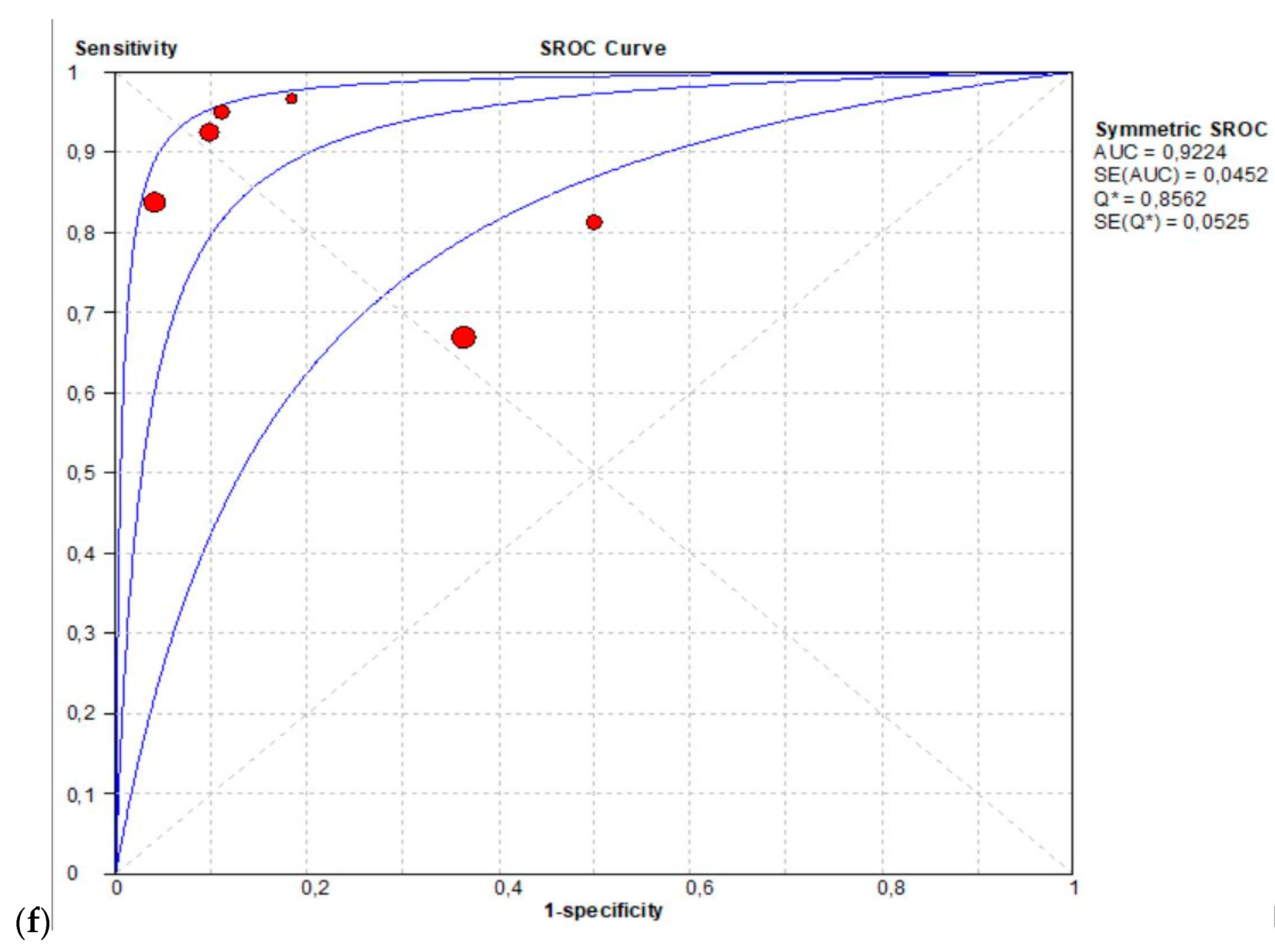
3.2.1. Detection of Primary Prostate Cancer Lesion
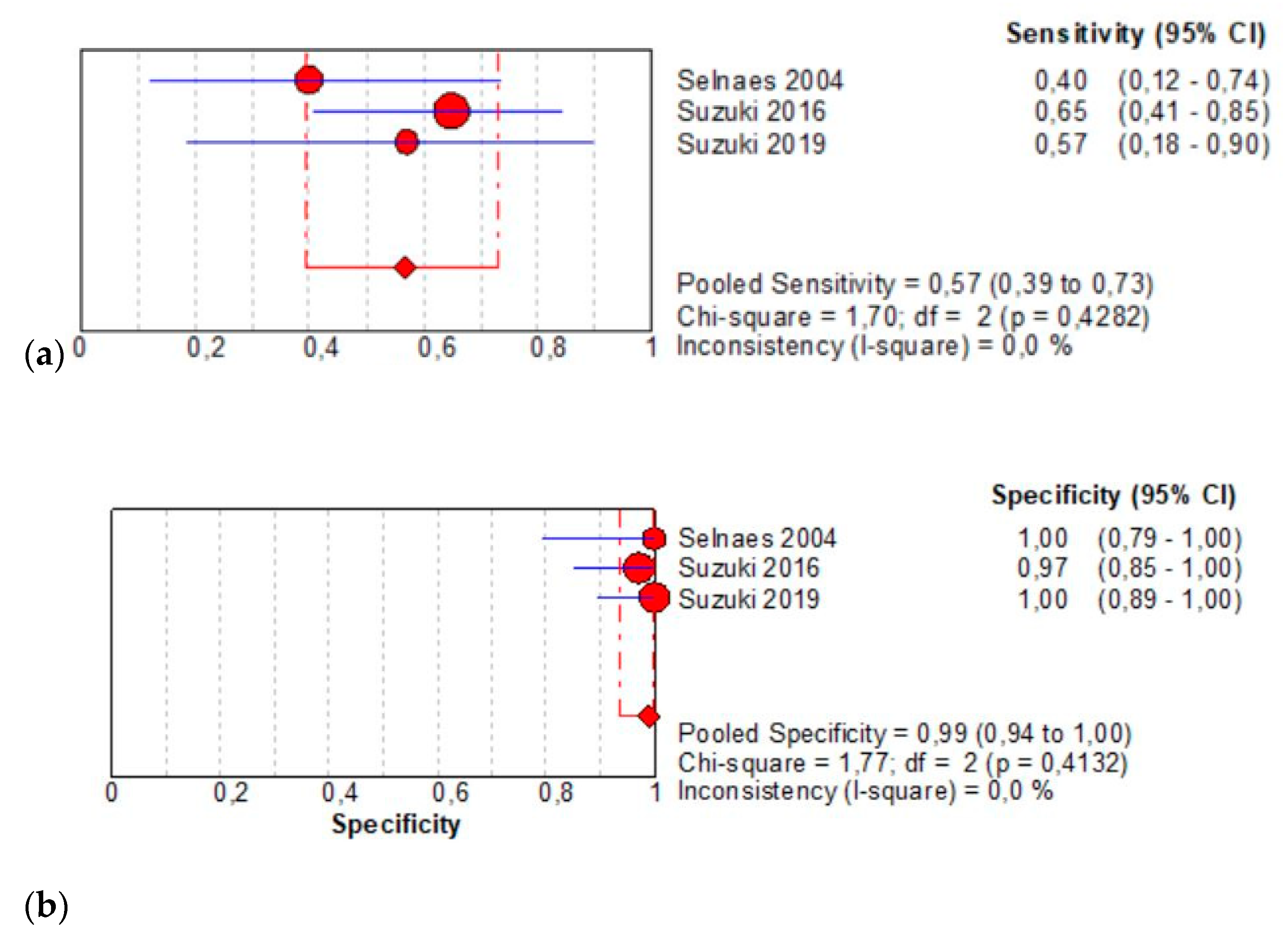
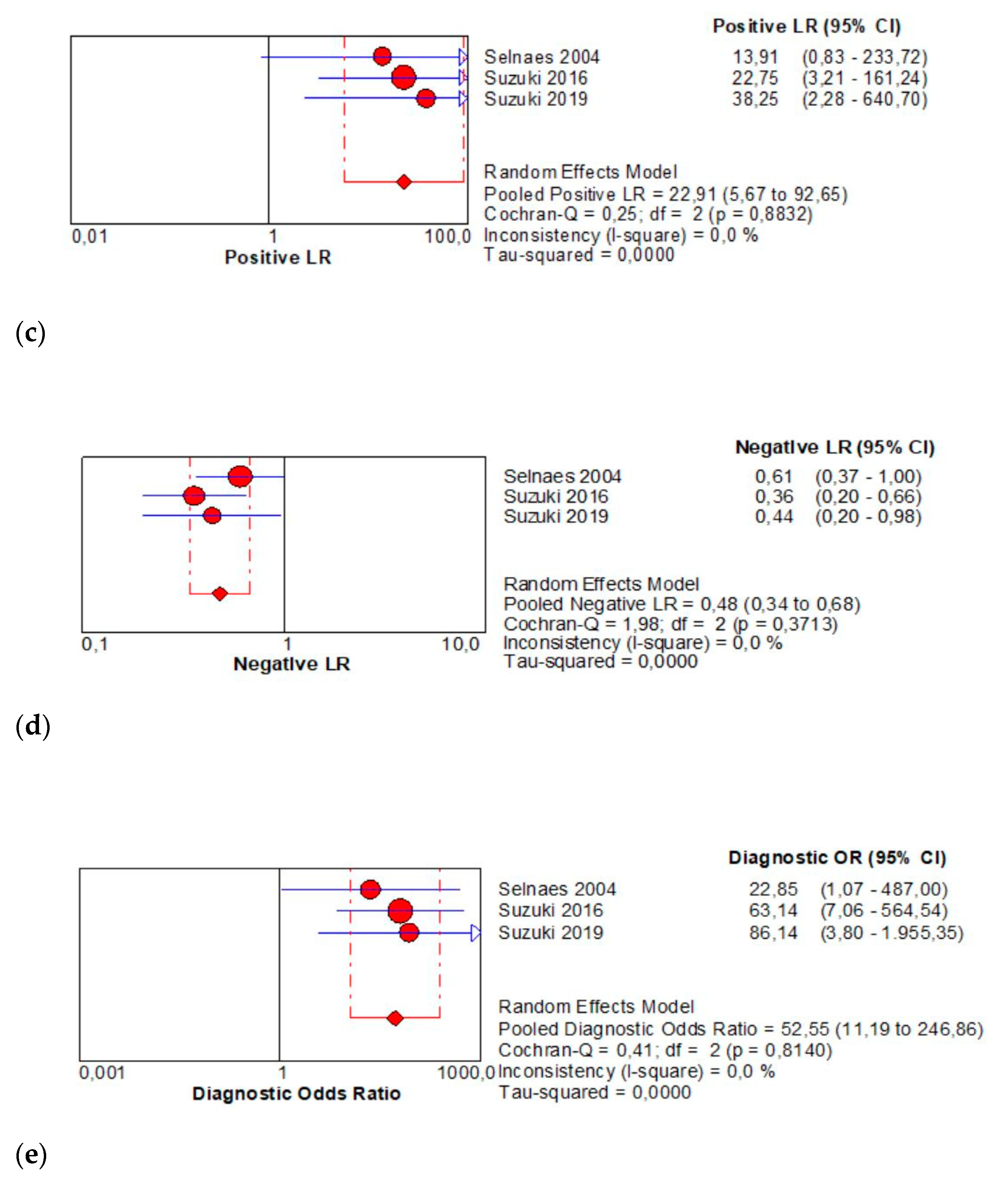
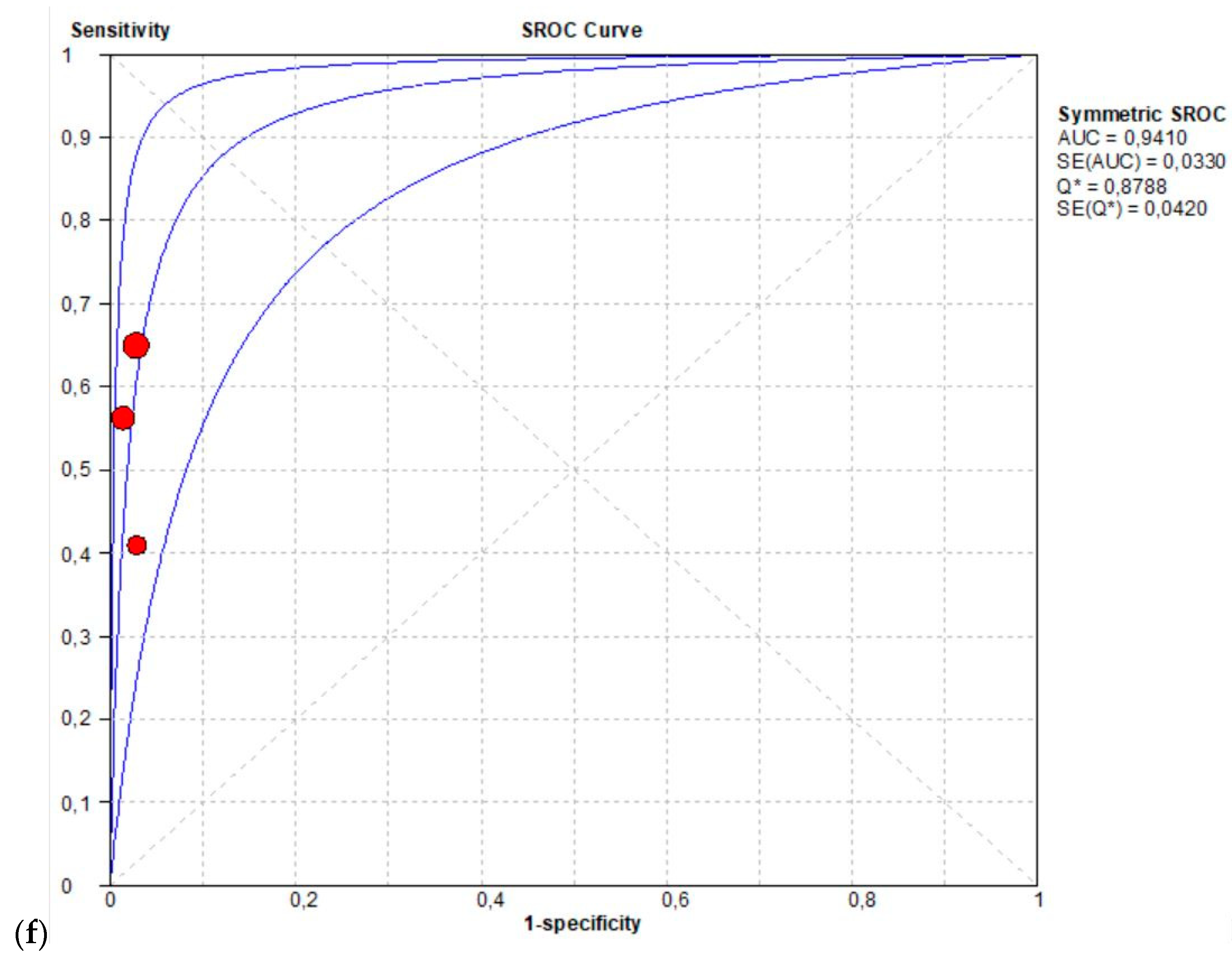
3.2.2. Preoperative LN Staging
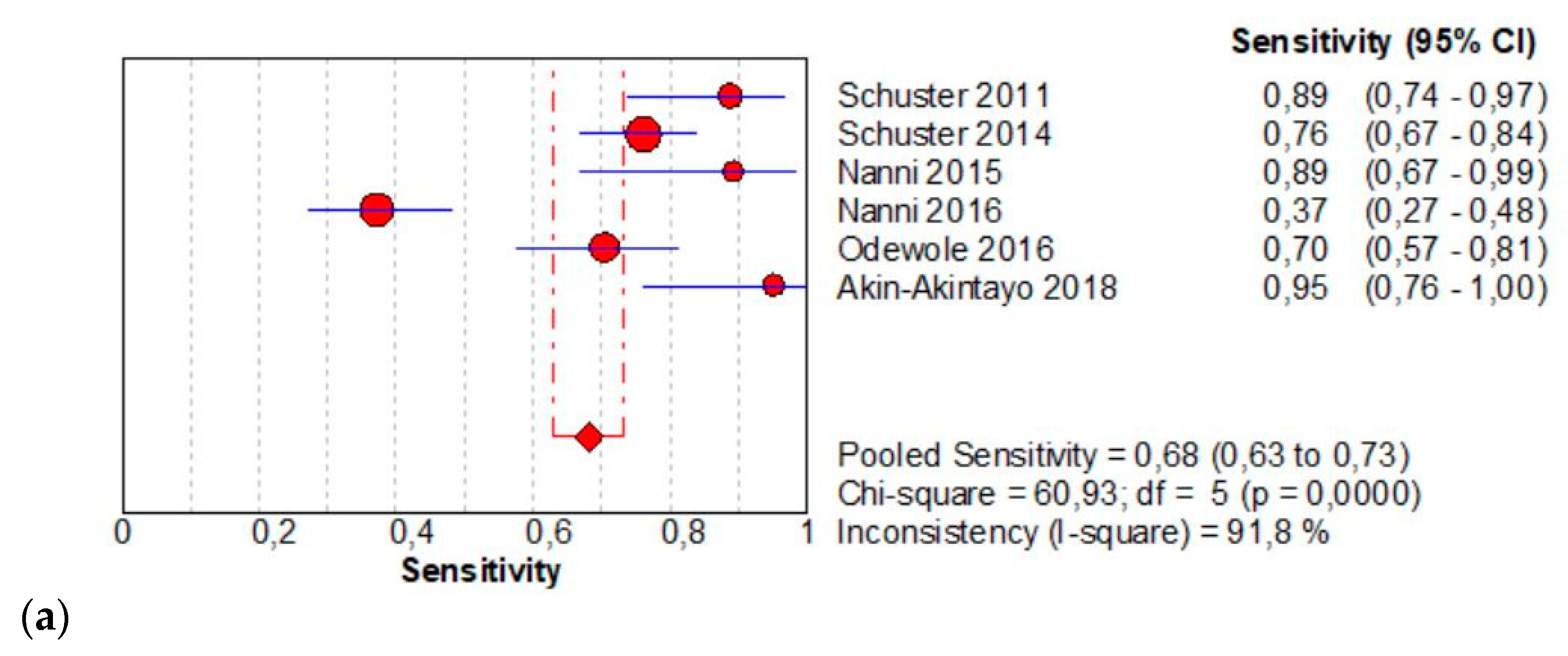
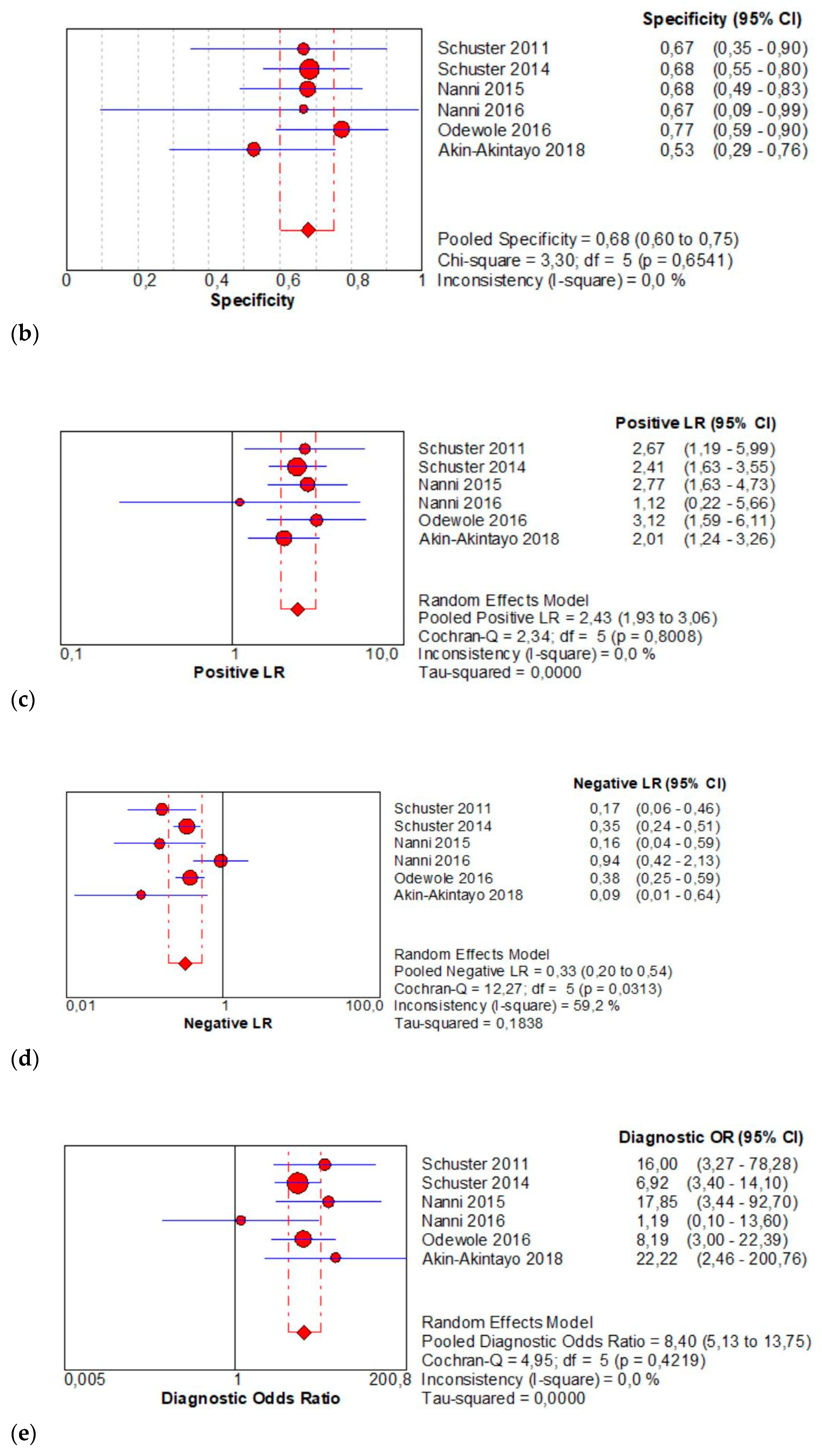
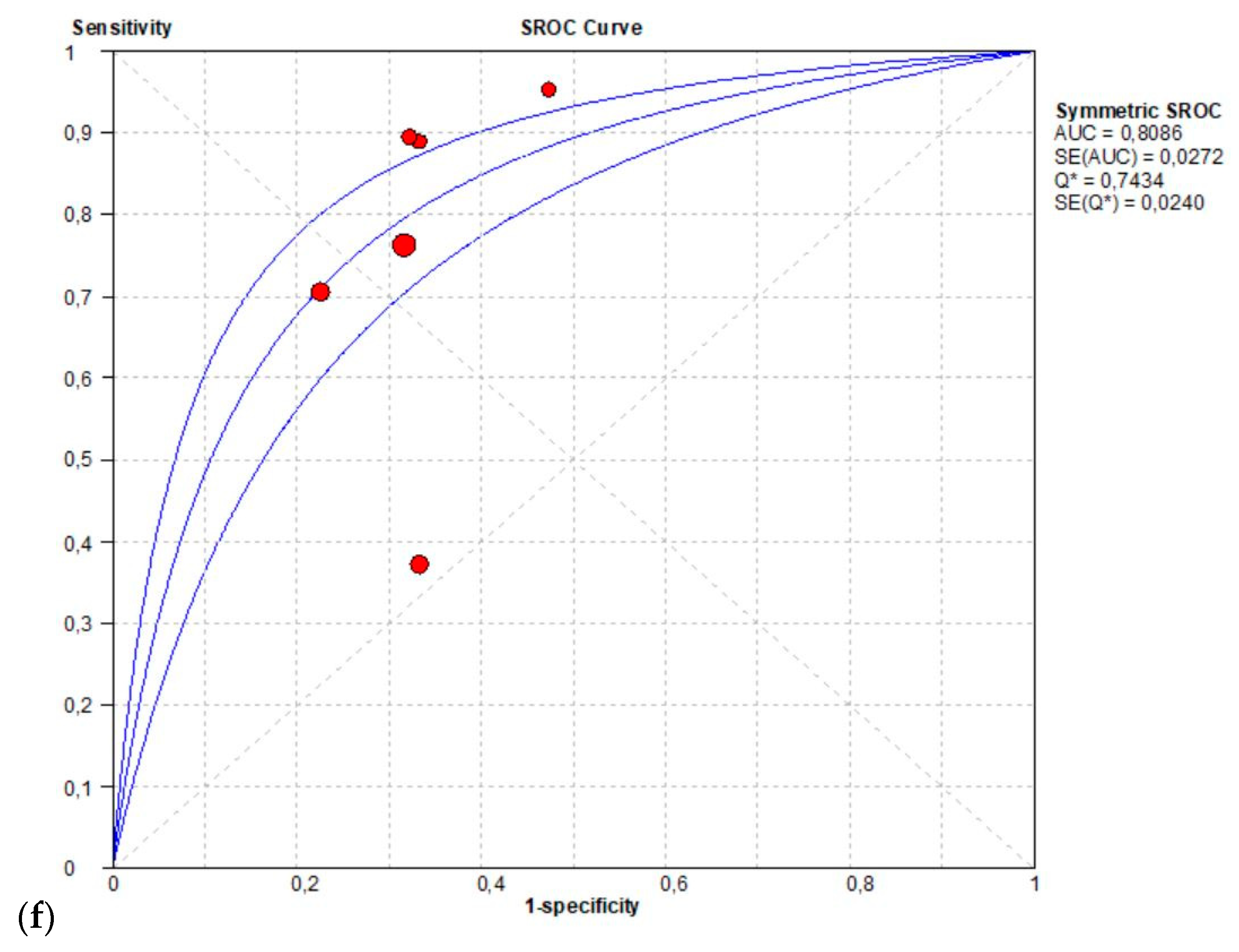
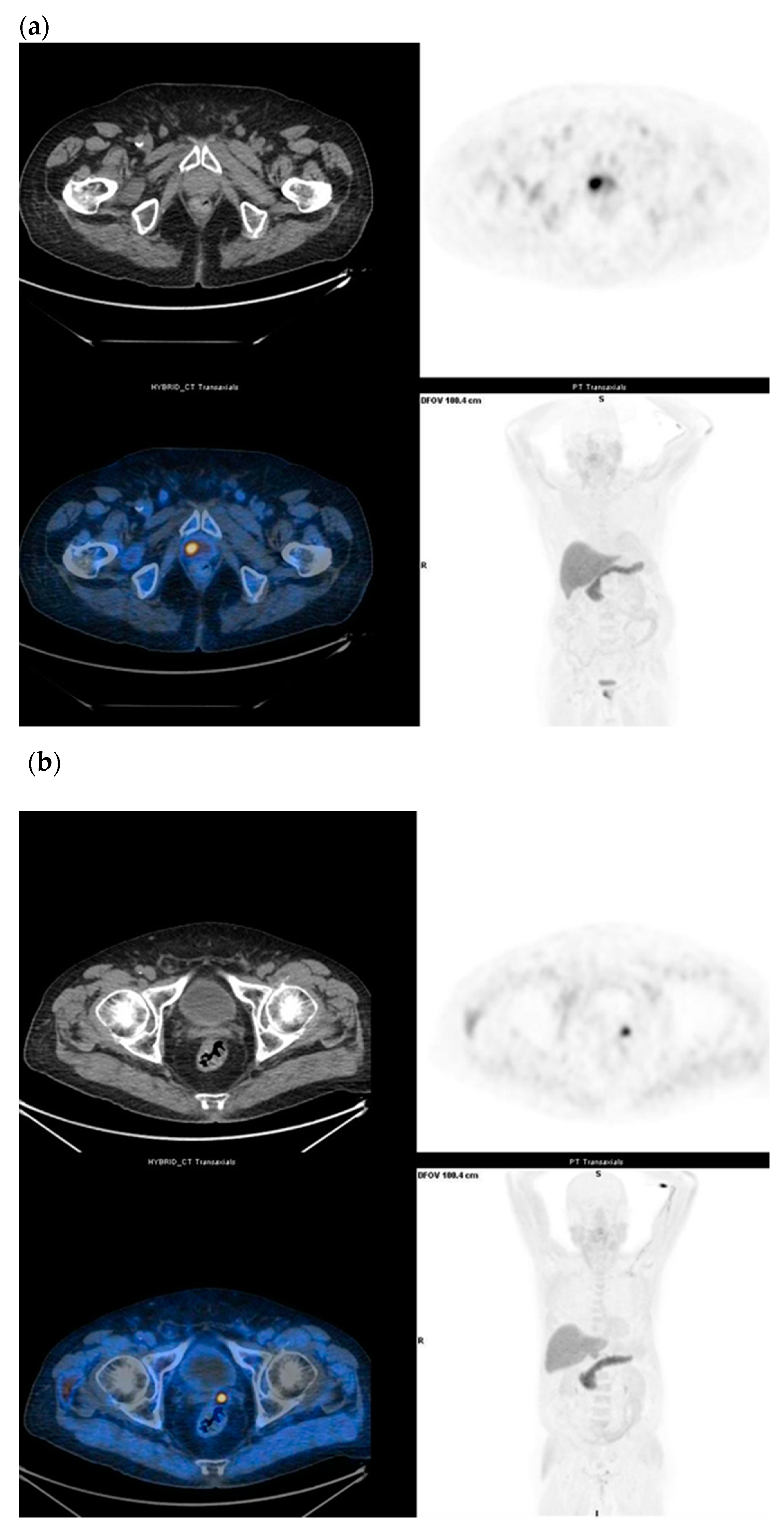
3.2.3. Detection of Recurrent Disease
3.2.4. Evaluation of Bone Metastases
3.2.5. Evaluation of Heterogeneity in Meta-Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataran, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, 359–386. [Google Scholar] [CrossRef]
- Haas, G.P.; Delongchamps, N.; Brawley, O.W.; Wang, C.Y.; De la Roza, G. The worldwide epidemiology of prostate cancer: Perspectives from autopsy studies. Can. J. Urol. 2008, 15, 3866–3871. [Google Scholar]
- Bell, K.J.; Del Mar, C.; Wright, G.; Dickinson, J.; Glasziou, P. Prevalence of incidental prostate cancer: A systematic review of autopsy studies. Int. J. Cancer 2015, 137, 1749–1757. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Cornford, P.; van den Bergh, R.C.N.; Briers, E.; De Santis, M.; Fanti, S.; Gillessen, S.; Grummet, J.; Henry, A.M.; Lam, T.B.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. EAU Guidelines. In Proceedings of the EAU Annual Congress Amsterdam, 20–24 March 2020; ISBN 978-94-92671-07-3. [Google Scholar]
- Ono, M.; Oka, S.; Okudaira, H.; Nakanishi, T.; Mizolami, A.; Kobayashi, M.; Schuster, D.M.; Goodman, M.M.; Shirakami, Y.; Kawai, K. [(14)C] fluciclovine (alias anti-[(14)C] FACBC) uptake and ASCT2 expression in castration-resistant prostate cancer cells. Nucl. Med. Biol. 2015, 42, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Miller, M. Axumin (fluciclovine F 18) Imaging & Interpretation Manual. v2.0 Final; Blue Earth Diagnostics Ltd.: Oxford, UK, 2019; pp. 1–21. [Google Scholar]
- Schuster, D.M.; Nanni, C.; Fanti, S.; Oka, S.; Okudaira, H.; Inoue, Y.; Sorensen, J.; Owenius, R.; Chovke, P.; Turkbey, B.; et al. Anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid: Physiologic uptake patterns, incidental findings, and variants that may simulate disease. J. Nucl. Med. 2014, 55, 1986–1992. [Google Scholar] [CrossRef]
- Tade, F.I.; Cohen, M.A.; Styblo, T.M.; Odewole, O.A.; Holbrook, A.I.; Newell, M.S.; Savir-Baruch, B.; Li, X.B.; Goodman, M.M.; Nye, J.A.; et al. Anti3-18F-FACBC (fluciclovine) PET/CT of breast cancer: An exploratory study. J. Nucl. Med. 2016, 57, 1357–1363. [Google Scholar] [CrossRef]
- Mapelli, P.; Incerti, E.; Ceci, F.; Castellucci, P.; Fanti, S.; Picchio, M. 11C- or 18F-choline PET/CT for imaging evaluation of biochemical recurrence of prostate cancer. J. Nucl. Med. 2016, 57, 43–48S. [Google Scholar]
- Calais, J.; Ceci, F.; Eiber, M.; Hope, T.A.; Hofman, M.S.; Rischpler, C.; Bach-Gansmo, T.; Nanni, C.; Savir-Baruch, B.; Elashoff, D.; et al. (18)F-fluciclovine PET-CT and (68) Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: A prospective, single-centre, single-arm, comparative imaging trial. Lancet Oncol. 2019, 20, 1286–1294. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Odewole, O.A.; Tade, F.I.; Nieh, P.T.; Savir-Baruch, B.; Jani, A.B.; Master, V.A.; Rossi, P.J.; Halkar, R.K.; Osunkoya, A.O.; Akin-Akintayo, O.; et al. Recurrent prostate cancer detection with anti-3-[18F] FACBC PET/CT: Comparison with CT. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1773–1783. [Google Scholar] [CrossRef]
- Schuster, D.M.; Taleghani, P.A.; Nieh, P.T.; Master, V.A.; Amzat, R.; Savir-Baruch, B.; Halkar, R.K.; Fox, T.; Osunkoya, A.O.; Moreno, C.S.; et al. Characterization of primary prostate carcinoma by anti-1-amino-2-[18F]-fluoro cyclobutane-1-carboxylic acid (anti-3-[18F] FACBC) uptake. Am. J. Nucl. Med. Mol. Imaging 2013, 3, 85–96. [Google Scholar] [PubMed]
- Kairemo, K.; Rasulova, N.; Partanen, K.; Joensuu, T. Preliminary clinical experience of trans-1-amino-3-(18)F-fluorocyclobutanecarboxylic Acid (anti-(18)F-FACBC) PET/CT imaging in prostate cancer patients. BioMed Res. Int. 2014, 2014, 1–7. [Google Scholar]
- Turkbey, B.; Mena, E.; Shih, J.; Pinto, P.A.; Merino, M.J.; Lindenberg, M.L.; Bernardo, M.; McKinney, Y.L.; Adler, S.; Owenius, R.; et al. Localized prostate cancer detection with 18F FACBC PET/CT: Comparison with MR imaging and histopathologic analysis. Radiology 2014, 270, 849–856. [Google Scholar] [CrossRef]
- Suzuki, H.; Inoue, Y.; Fujimoto, H.; Yonese, J.; Tanabe, K.; Fukasawa, S.; Inoue, T.; Saito, S.; Ueno, M.; Otaka, A. Diagnostic performance and safety of NMK36 (trans-1-amino-3-[18F] fluorocyclobutanecarboxylic acid)—PET/CT in primary prostate cancer: Multicenter Phase IIb clinical trial. Jpn. J. Clin. Oncol. 2016, 46, 152–162. [Google Scholar] [CrossRef]
- Elschot, M.; Selnæs, K.M.; Sandsmark, E.; Krüger-Stokke, B.; Størkersen, Ø.; Giskeødegård, G.F.; Tessem, M.; Moestue, S.A.; Bertilsson, H.; Bathen, T.F. Combined 18F-fluciclovine PET/MRI shows potential for detection and characterization of high-risk prostate cancer. J. Nucl. Med. 2018, 59, 762–768. [Google Scholar] [CrossRef]
- Jambor, I.; Kuisma, A.; Kahkonen, E.; Kemppainen, J.; Merisaari, H.; Eskola, O.; Teuho, J.; Montoya Perez, I.; Pesola, M.; Aronen, H.J.; et al. Prospective evaluation of 18F-FACBC PET/CT and PET/MRI versus multiparametric MRI in intermediate—to high—risk prostate cancer patients (FLUCIPRO trial). Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 355–364. [Google Scholar] [CrossRef]
- Selnæs, K.M.; Kruger-Stokke, B.; Elschot, M.; Willoch, F.; Størkersen, Ø.; Sandsmark, E.; Moestue, S.A.; Tessem, M.; Halvorsen, D.; Kjøbli, E.; et al. 18F-Fluciclovine PET/MRI for preoperative lymph node staging in high-risk prostate cancer patients. Eur. Radiol. 2018, 28, 3151–3159. [Google Scholar] [CrossRef]
- Suzuki, H.; Jinnouchi, S.; Kaji, Y.; Kishida, T.; Kinoshita, H.; Yamaguchi, S.; Tobe, T.; Okamura, T.; Kawakita, M.; Furukawa, J.; et al. Diagnostic performance of 18F-fluciclovine PET/CT for regional lymph node metastases in patients with primary prostate cancer: A multicenter phase II clinical trial. Jpn. J. Clin. Oncol. 2019, 49, 803–811. [Google Scholar]
- Schuster, D.M.; Savir-Baruch, B.; Nieh, P.T.; Master, V.A.; Halkar, R.K.; Rossi, P.J.; Lewis, M.M.; Nye, J.A.; Yu, W.; Bowman, F.D.; et al. Detection of recurrent prostate carcinoma with anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid PET/CT and 111In-capromab pendetide SPECT/CT. Radiology 2011, 259, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Schuster, D.M.; Nieh, P.T.; Jani, A.B.; Amzat, R.; Bowman, F.D.; Haslkar, R.K.; Master, V.A.; Nye, J.A.; Odewole, O.A.; Osunkoya, A.O.; et al. Anti-3-[18F] FACBC positron emission tomography-computerized tomography and 111In-capromab pendetide single photon emission computerized tomography-computerized tomography for recurrent prostate carcinoma: Results of a prospective clinical trial. J. Urol. 2014, 191, 1446–1453. [Google Scholar] [CrossRef] [PubMed]
- Nanni, C.; Schiavina, R.; Brunocilla, E.; Boschi, S.; Borghesi, M.; Zanoni, L.; Pettinato, C.; Martorana, G.; Fanti, S. 18F-fluciclovine PET/CT for the detection of prostate cancer relapse: A comparison to 11C-choline PET/ CT. Clin. Nucl. Med. 2015, 40, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Nanni, C.; Zanoni, L.; Pultrone, C.; Schiavina, R.; Brunocilla, E.; Lodi, F.; Malizia, C.; Ferrari, M.; Rigatti, P.; Fonti, C.; et al. 18F-FACBC (anti1-amino-3-18F-fluorocyclobutane-1-carboxylic acid) versus 11C-choline PET/CT in prostate cancer relapse: Results of a prospective trial. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1601–1610. [Google Scholar] [CrossRef]
- Akin-Akintayo, O.; Tade, F.; Mittal, P.; Moreni, C.; NIeh, P.T.; Rossi, P.; Patil, D.; Halkar, R.; Fei, B.; Master, V.; et al. Prospective evaluation of 18F-Fluciclovine PET-CT and MRI in detection of recurrent prostate cancer in non-prostatectomy patients. Eur. J. Radiol. 2018, 102, 1–8. [Google Scholar] [PubMed]
- Chen, B.; Wei, P.; Macapinlac, H.A.; Lu, Y. Comparison of 18F-Fluciclovine PET/CT and 99mTc-MDP bone scan in detection of bone metastasis in prostate cancer. Nuc. Med. Commun. 2019, 40, 940–946. [Google Scholar]
- Bach-Gansmo, T.; Nanni, C.; Nieh, P.Y.; Zanoni, L.; Bogsrud, T.V.; Sletten, H.; Korsan, K.A.; Kieboom, K.J.; Tade, F.I.; Odewole, O.; et al. Multisite experience of the safety, detection rate and diagnostic performance of Fluciclovine (18F) Positron Emission Tomography/Computerized Tomography Imaging in the staging of biochemically recurrent prostate cancer. J. Urol. 2017, 197, 676–683. [Google Scholar] [CrossRef]
- De Visschere, P.J.L.; Standaert, C.; Fütterer, J.J.; Villeirs, G.M.; Panebianco, V.; Walz, J.; Maurer, T.; Hadaschik, B.A.; Leucovet, F.E.; Giannarini, G.; et al. A Systematic Review on the Role of Imaging in Early Recurrent Prostate Cancer. Eur. Urol. Oncol. 2019, 2, 47–76. [Google Scholar] [CrossRef] [PubMed]
- Pernthaler, B.; Kuinik, R.; Gstettner, C.; Salamon, S.; Aigner, R.M.; Kvaternik, H. A perspective head-to-head comparison of 18F-fluciclovine with 68Ga-PSMA-11 in biochemical recurrence of prostate cancer in PET/CT. Clin. Nucl. Med. 2019, 44, 566–573. [Google Scholar] [CrossRef]
- Bin, X.; Yong, S.; Kong, Q.F.; Zhao, S.; Zhang, G.Y.; Wu, J.P.; Chen, S.Q.; Zhu, W.D.; Pan, K.H.; Du, M.L.; et al. Diagnostic performance of PET/CT using 18F-FACBC in prostate cancer: A meta-analysis. Front Oncol. 2020, 9, 1–9. [Google Scholar] [CrossRef]
- Laudicella, R.; Albano, D.; Alongi, P.; Argiroffi, G.; Bauckneht, M.; Baldari, S.; Bertagna, F.; Boero, M.; De Vincentis, G.; Del Sole, A.; et al. (18) F-Facbc in Prostate Cancer: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 1348. [Google Scholar] [CrossRef]
- Kim, S.-J.; Lee, S. The role of (18) F-fluciclovine PET in the management of prostate cancer: A systematic review and meta-analysis. Clin. Radiol. 2019, 74, 886–892. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain | Patient Selection | Index Test | Reference Standard | Flow and Timing |
|---|---|---|---|---|
| Description | Describe methods of patient selection. Describe included patients (previous testing, presentation, intended use of index test and setting) | Describe the index test and how it was conducted and interpreted | Describe the reference standard and how it was conducted and interpreted | Describe any patients who did not receive the index tests or reference standard or who were excluded from the 2 × 2 table. Describe the interval and any interventions between index tests and the reference standard |
| Signaling questions (yes, no, unclear) | Was a consecutive or random sample of patients enrolled? Was a case-control design avoided? Did the study avoid inappropriate exclusions? | Were the index test results interpreted without knowledge of the results of the reference standard? If a threshold was used, was it pre-specified? | Is the reference standard likely to correct classify the target condition? Were the reference standard results interpreted without knowledge of the results of the index test? | Was there an appropriate interval between index tests and reference standard? Did all patients receive a reference standard? Did all patients receive the same reference standard? Were all patients included in the analysis? |
| Risk of bias | Could the selection of patients have introduced bias? | Could the conduct or interpretation of the index test have introduced bias? | Could the reference standard, its conduct or its interpretation have introduced bias? | Could the patient flow have introduced bias? |
| Concerns about applicability (high, low, unclear) | Are there concerns that the included patients do not match the review question? | Are there concerns that the index tests, its conduct, or its interpretation differ from the review question? | Are there concerns that the target condition as defined by the reference standard does not match the review question? |
| First Author, Year | True + | False + | False − | True − | Sensitivity (95% CI) | Specificity (95% CI) | No Pts | Age | PSA ng/mL | GS |
|---|---|---|---|---|---|---|---|---|---|---|
| Diagnosis of primary PCa | ||||||||||
| Schuster 2013 | 65 | 20 | 15 | 20 | 0.81 (0.7–1.00) | 0.50 (0.34–0.65) | 10 | 60.8 | 8.2 | 6–10 |
| Kairemo 2014 | 14 | 3 | 0 | 15 | 1.00 (0.77–1.00) | 0.83 (0.59–0.96) | 26 | 68.1 | 7.9 | 7.1 |
| Turkbey 2014 | 99 | 99 | 49 | 173 | 0.67 (0.59–0.74) | 0.64 (0.58–0.69) | 22 | 62.2 | 13.5 | 6–9 |
| Suzuki 2016 | 173 | 7 | 14 | 64 | 0.93 (0.88–0.96) | 0.90 (0.81–0.96) | 68 | 67.3 | 88.6 | 6–10 |
| Elschot 2018 | 38 | 9 | 2 | 72 | 0.95 (0.83–0.99) | 0.89 (0.79–0.95) | 28 | 66 | n.a. | n.a. |
| Jambor 2018 | 139 | 6 | 27 | 140 | 0.84 (0.77–0.89) | 0.96 (0.91–0.98) | 32 | 65 | 12.0 | 7 |
| Preoperative LN staging | ||||||||||
| Selnaes 2018 | 4 | 0 | 6 | 16 | 0.40 (0.12–0.73) | 1.00 (0.79–1.00) | 28 | 66.2 | 14.6 | 7–11 |
| Suzuki 2016 | 13 | 1 | 7 | 34 | 0.65 (0.40–0.84) | 0.97 (0.85–0.99) | 68 | 67.3 | 88.6 | 6–10 |
| Suzuki 2019 | 4 | 0 | 3 | 33 | 0.57 (0.18–0.90) | 0.85 (0.68–0.95) | 28 | 69 | 12.8 | 7–10 |
| Detection of recurrent disease | ||||||||||
| Schuster 2011 | 32 | 4 | 4 | 8 | 0.89 (0.74–0.97) | 0.67 (0.35–0.90) | 93 | 68.3 | 6.6 | n.a. |
| Schuster 2014 | 77 | 19 | 24 | 41 | 0.76 (0.67–0.84) | 0.68 (0.55–0.80) | 28 | 68 | 9.8 | 7 |
| Nanni 2015 | 17 | 10 | 2 | 21 | 0.89 (0.67–0.99) | 0.68 (0.49–0.83) | 50 | 67 | 3.2 | n.a. |
| Nanni 2016 | 32 | 1 | 54 | 2 | 0.37 (0.27–0.48) | 0.67 (0.09–0.99) | 89 | 69 | 6.9 | n.a. |
| Odewole 2016 | 43 | 7 | 18 | 24 | 0.70 (0.57–0.81) | 0.77 (0.59–0.90) | 53 | 67.5 | 7.2 | n.a. |
| Akin-Akintayo 2018 | 20 | 9 | 1 | 10 | 0.95 (0.76–1.00) | 0.53 (0.29–0.76) | 24 | 70.8 | 8.5 | 7 |
| Detection of bone metastases | ||||||||||
| Chen Bo 2019 | 8 | 13 | 3 | 0 | 1 (0.77–1) | 0.98 (0.92–1) | 26 | 70 | 1.3 | 6–10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biscontini, G.; Romagnolo, C.; Cottignoli, C.; Palucci, A.; Fringuelli, F.M.; Caldarella, C.; Ceci, F.; Burroni, L. 18F-Fluciclovine Positron Emission Tomography in Prostate Cancer: A Systematic Review and Diagnostic Meta-Analysis. Diagnostics 2021, 11, 304. https://doi.org/10.3390/diagnostics11020304
Biscontini G, Romagnolo C, Cottignoli C, Palucci A, Fringuelli FM, Caldarella C, Ceci F, Burroni L. 18F-Fluciclovine Positron Emission Tomography in Prostate Cancer: A Systematic Review and Diagnostic Meta-Analysis. Diagnostics. 2021; 11(2):304. https://doi.org/10.3390/diagnostics11020304
Chicago/Turabian StyleBiscontini, Giuseppina, Cinzia Romagnolo, Chiara Cottignoli, Andrea Palucci, Fabio Massimo Fringuelli, Carmelo Caldarella, Francesco Ceci, and Luca Burroni. 2021. "18F-Fluciclovine Positron Emission Tomography in Prostate Cancer: A Systematic Review and Diagnostic Meta-Analysis" Diagnostics 11, no. 2: 304. https://doi.org/10.3390/diagnostics11020304
APA StyleBiscontini, G., Romagnolo, C., Cottignoli, C., Palucci, A., Fringuelli, F. M., Caldarella, C., Ceci, F., & Burroni, L. (2021). 18F-Fluciclovine Positron Emission Tomography in Prostate Cancer: A Systematic Review and Diagnostic Meta-Analysis. Diagnostics, 11(2), 304. https://doi.org/10.3390/diagnostics11020304