
Compliance and Adherence to Pelvic Floor Exercise Therapy in People with Pelvic Floor Disorders: A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
Eligibility Criteria
2.3. Outcome Measures
2.3.1. Main Outcome
2.3.2. Secondary Outcomes
2.4. Data Extraction and Quality Assessment
2.5. Effects Measures
2.6. Data Synthesis and Analysis
3. Results
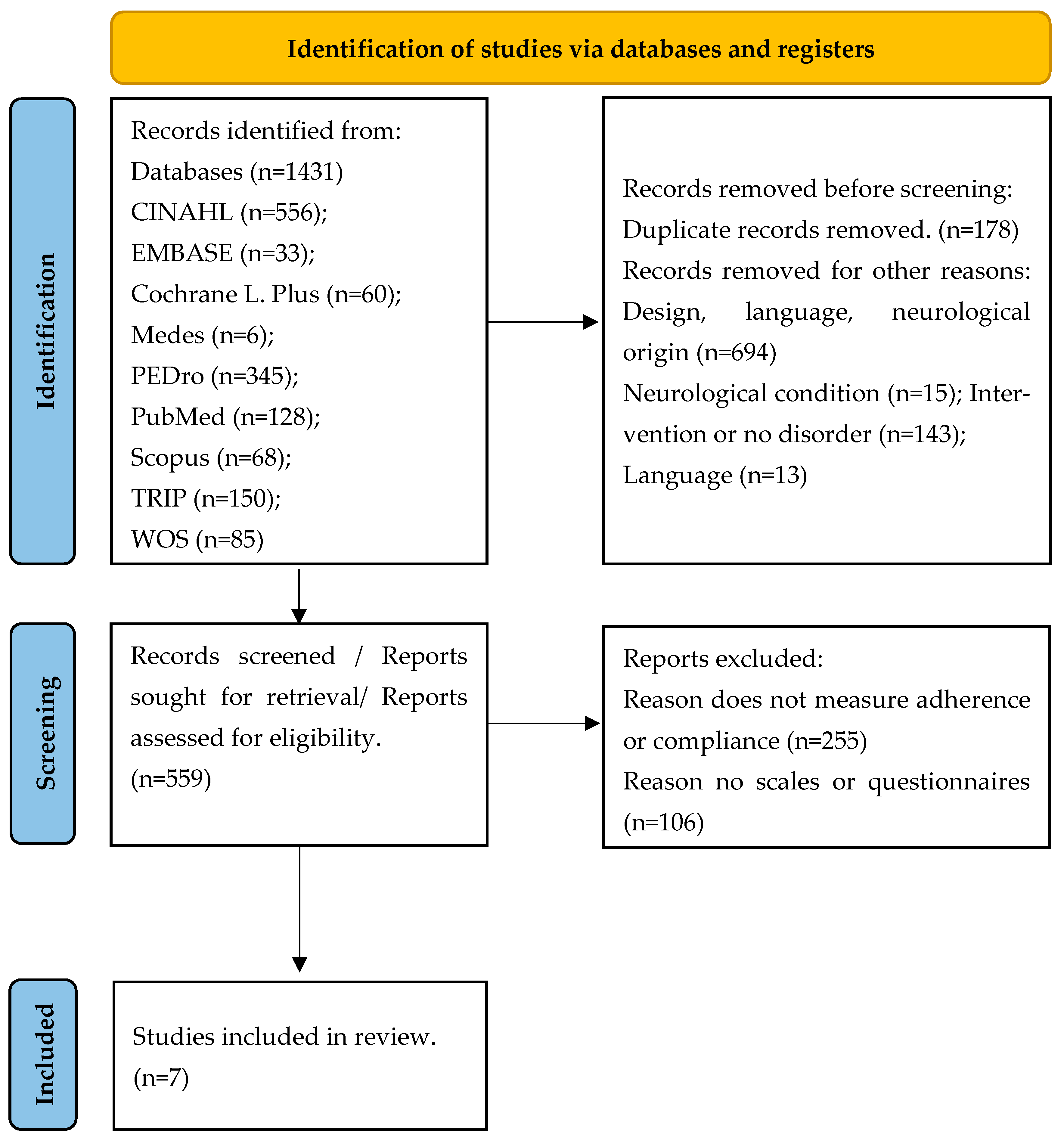
3.1. Flow of Trials Through the Review
3.2. Characteristics of the Included Studies
3.3. Quality Assessment
3.4. Main Outcome
3.5. Secondary Outcomes
3.6. Relationship Between Sexual Health and Secondary Outcomes
3.7. Relationship Between the Main and Secondary Outcomes
3.8. Results of the Quantitative Syntheses
3.9. Publication Bias Assessment
3.10. Evidence Synthesis
4. Discussion
4.1. Qualitative Analysis
4.2. Quantitative Analysis
4.3. The Challenge of Adherence
4.4. Clinical Implications
4.5. Limitations and Future Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Intervention | AND | Participants | AND | Outcome | AND | Design |
| (“Physical Therapy Modalities” OR “exercise therapy” OR “exercise” OR “Exercise Movement Techniques”) | (“Urinary Incontinence” OR “Pelvic Floor Disorders”) | (“Patient Compliance” OR “Treatment Adherence and Compliance”) | “effectiveness” |
| Database | Search Strategy |
|---|---|
| CINAHL | ((((“Patient Compliance” OR “Treatment Adherence and Compliance”) AND (“Physical Therapy Modalities” OR “exercise therapy” OR “exercise” OR “Exercise Movement Techniques”) AND (“Urinary Incontinence” OR “Pelvic Floor Disorders”) AND (“effectiveness”)))) Limit “academic publications” in source type. |
| EMBASE | (’pelvic floor disorder’/exp OR ’urine incontinence’/exp) AND (’physiotherapy’/exp OR ’exercise’/exp) AND patient compliance/exp AND randomized controlled trial/exp |
| The Cochrane Plus Library | ((((“Patient Compliance” OR “Treatment Adherence and Compliance”) AND (“Physical Therapy Modalities” OR “exercise therapy” OR “exercise” OR “Exercise Movement Techniques”) AND (“Urinary Incontinence” OR “Pelvic Floor Disorders”) AND (“effectiveness”)))) Limit “Randomized controlled Trial”. |
| Medes | (((((((((““Cooperación del paciente” “[todos]) OR ““Cumplimiento y adherencia al tratamiento” “[todos]) AND “ “Modalidades de Fisioterapia”“[todos]) OR “ “terapia por ejercicio” “[todos]) OR “ “ejercicio físico” “[todos]) OR “ “Técnicas de ejercicio con movimiento” “[todos]) AND “ “Incontinencia urinaria” “[todos]) OR ““Trastornos del suelo pélvico” “[todos]) AND ““efectividad”“[todos]) |
| PEDro | Therapy: strength training/Problem: incontinence/Body part: perineum or genitor-urinary system/Sub discipline: continence and women’s health/Topic: no appropriate value in this field/Method: Clinical Trial |
| PubMed | “Patient Compliance” OR “Treatment Adherence and Compliance” AND “Physical Therapy Modalities” OR “exercise therapy” OR “exercise” OR “Exercise Movement Techniques” AND “Urinary Incontinence” OR “Pelvic Floor Disorders” AND “effectiveness” Limit “Randomized controlled Trial”. |
| Scopus | “Patient Compliance” OR “Treatment Adherence and Compliance” AND “Physical Therapy Modalities” OR “exercise therapy” OR “exercise” OR “Exercise Movement Techniques” AND “Urinary Incontinence” OR “Pelvic Floor Disorders” AND “effectiveness” |
| TRIP | “Urinary incontinence” OR “pelvic floor disorders” AND “patient compliance” OR “treatment adherence AND compliance” AND “physical therapy modalities” OR “exercise therapy” OR “exercise” OR “exercise movement techniques” Limit Key primary research. |
| WOS Filtered by WOS categories: rehabilitation, sport sciences, gerontology, communication, obstetrics gynecology, urology nephrology, pediatrics, cultural studies, medicine research experimental. | ((((((((AB = (“Patient Compliance”)) OR AB = (“Treatment Adherence and Compliance”)) AND AB = (“Physical Therapy Modalities”)) OR AB = (“exercise therapy” )) OR AB = (“exercise”)) OR AB = (“Exercise Movement Techniques”)) AND AB = (“Urinary Incontinence”)) OR AB = (“Pelvic Floor Disorders”)) AND AB = (“effectiveness”) Limit “Clinical Trial”. |
| Database | Identified | Duplicated | Design | Language | Neurological Origin | Selected for Screening | No Pelvic Floor Muscle Training (PFMT) /Intervention Based on PMFT in Both Groups/No Pelvic Floor Disorder | Eliminated After Reading the Full Text for Not Measuring Adherence or Compliance | Eliminated for Not Measuring Adherence to Treatment by Scales or Questionnaires | Included in the Review |
|---|---|---|---|---|---|---|---|---|---|---|
| CINAHL | 556 | 3 | 509 | 11 | 1 | 32 | 29 | 3 | 0 | 0 |
| EMBASE | 33 | 11 | 13 | 0 | 1 | 8 | 3 | 4 | 1 | 0 |
| The Cochrane Plus Library | 60 | 41 | 5 | 0 | 0 | 14 | 9 | 2 | 3 | 0 |
| Medes * | 6 | 0 | 5 | 0 | 0 | 1 | 0 | 1 | 0 | 0 |
| PEDro ** | 345 | 35 | 1 | 11 | 12 | 286 | 22 | 179 | 82 | 3 |
| PubMed | 128 | 10 | 18 | 2 | 2 | 96 | 29 | 50 | 14 | 3 |
| Scopus | 68 | 27 | 35 | 0 | 0 | 6 | 0 | 2 | 3 | 1 |
| TRIP | 150 | 16 | 37 | 0 | 0 | 97 | 87 | 9 | 1 | 0 |
| WOS | 85 | 35 | 31 | 0 | 0 | 19 | 12 | 5 | 2 | 0 |
| TOTAL | 1431 | 178 | 654 | 24 | 16 | 559 | 191 | 255 | 106 | 7 |
| Treatment Compliance and Adherence | |||||
| Study | 1 mo.–2 mo. | 3 mo. | 6 mo. | 9 mo. | 12 mo. |
| Glazener et al. (2011) [47] | MAPS Q. | MAPS Q. Practice y—no | MAPS Q. | ||
| Glazener et al. (2001) [48] | Modified version Questionnaire [54]. | ||||
| Jaffar et al. (2022) [49] | EARS 21 points (KAP) Q Section 5 | ||||
| Sacomori et al. (2020) [50] | Q Validated Alewijnse D. et al. 2003) [55] | ||||
| Alagirisamy et al. (2022) [51] | (KAP) Q Section 5 | KAP Q (4 mo.) | |||
| Sahin et al. (2022) [52] | 100 mm VAS complete exercises (no in G3) | ||||
| Kaya et al. (2015) [53] | 100 mm VAS scale. Compliance. (1.5 mo.) | ||||
| Quality of Life | |||||
| Study | 1 mo.–2 mo. | 3 mo. | 6 mo. | 9 mo. | 12 mo. |
| Glazener et al. (2011) [47] | Q3 ICIQ | EQ-5D and SF-12 Q3 ICIQ | EQ-5D and SF-12 Q3 ICIQ | ||
| Glazener et al. (2001) [48] | HADS | ||||
| Jaffar et al. (2022) [49] | ICIQ-LUTSqol 1 mo. and 2 mo. | ||||
| Sacomori et al. (2020) [50] | ICIQ-UI SF Q3 ICIQ | ||||
| Alagirisamy et al. (2022) [51] | ICIQ-UI SF No specific data from Q3 | ICIQ-UI SF 4 mo. No specific data from Q3 | |||
| Sahin et al. (2022) [52] | KHQ baseline 2 mo. | ||||
| Kaya et al. (2015) [53] | UDI-6 + IIQ-7 baseline 6 weeks | ||||
| Severity | |||||
| Study | 1 mo.–2 mo. | 3 mo. | 6 mo. | 9 mo. | 12 mo. |
| Glazener et al. (2011) [47] | ICIQ-UI SF Q1-3 p.57 pad use | ICIQ-UI SF Q1-3 pad use | ICIQ-UI SF Q1-3 pad use | ICIQ-UI SF Q1-3 pad use | |
| Glazener et al. (2001) [48] | Question about frequency | ||||
| Jaffar et al. (2022) [49] | ICIQ-UI SF 1 mo. and 2 mo. | ||||
| Sacomori et al. (2020) [50] | ICIQ-UI SF | ||||
| Alagirisamy et al. (2022) [51] | ICIQ-UI SF | ICIQ-UI SF 4 mo. | |||
| Sahin et al. (2022) [52] | Baseline 2 mo. 24 h pad test/ ISI/UDI-6 | ||||
| Kaya et al. (2015) [53] | ISI baseline and 6 weeks | ||||
References
- Messelink, B.; Benson, T.; Berghmans, B.; Bø, K.; Corcos, J.; Fowler, C.; Laycock, J.; Lim, P.H.-C.; van Lunsen, R.; Lycklama á Nijeholt, G.; et al. Standardization of Terminology of Pelvic Floor Muscle Function and Dysfunction: Report from the Pelvic Floor Clinical Assessment Group of the International Continence Society. Neurourol. Urodyn. 2005, 24, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Ramírez García, I.; Blanco Ratto, L.; Kaufmann Frau, S. Rehabilitación Del Suelo Pélvico Femenino: Práctica Clínica Basada en la Evidencia; Médica Panamericana: Washington, DC, USA, 2014; ISBN 978-84-9110-475-9. [Google Scholar]
- Cohen, D.; Gonzalez, J.; Goldstein, I. The Role of Pelvic Floor Muscles in Male Sexual Dysfunction and Pelvic Pain. Sex. Med. Rev. 2016, 4, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Frawley, H.; Shelly, B.; Morin, M.; Bernard, S.; Bø, K.; Digesu, G.A.; Dickinson, T.; Goonewardene, S.; McClurg, D.; Rahnama’i, M.S.; et al. An International Continence Society (ICS) Report on the Terminology for Pelvic Floor Muscle Assessment. Neurourol. Urodyn. 2021, 40, 1217–1260. [Google Scholar] [CrossRef] [PubMed]
- Hage-Fransen, M.A.H.; Wiezer, M.; Otto, A.; Wieffer-Platvoet, M.S.; Slotman, M.H.; Nijhuis-van der Sanden, M.W.G.; Pool-Goudzwaard, A.L. Pregnancy- and Obstetric-related Risk Factors for Urinary Incontinence, Fecal Incontinence, or Pelvic Organ Prolapse Later in Life: A Systematic Review and Meta-analysis. Acta Obstet. Gynecol. Scand. 2021, 100, 373–382. [Google Scholar] [CrossRef]
- Mohedo, E.D.; Sánchez, E.M.M.; Serrano, C.M.S. Guía de Práctica Clínica Para Fisioterapeutas en la Incontinencia Urinaria Femenina, 1st ed.; Ilustra Colegio Oficial de Fisioterapeutas de Andalucía: Sevilla, Spain, 2013; ISBN 13978-84-616-4903-7. [Google Scholar]
- Milsom, I.; Altman, D.; Lapitan, M.C.; Nelson, R.; Sillen, U.; Thom, D. Epidemiology of Urinary (UI) and Faecal (FI) Incontinence and Pelvic Organ Prolapse (POP). Incontinence 2009, 15–107. Available online: https://www.ics.org/publications/ici_3/v1.pdf/chap5.pdf (accessed on 2 April 2025).
- D’Ancona, C.; Haylen, B.; Oelke, M.; Abranches-Monteiro, L.; Arnold, E.; Goldman, H.; Hamid, R.; Homma, Y.; Marcelissen, T.; Rademakers, K.; et al. The International Continence Society (ICS) Report on the Terminology for Adult Male Lower Urinary Tract and Pelvic Floor Symptoms and Dysfunction. Neurourol. Urodyn. 2019, 38, 433–477. [Google Scholar] [CrossRef]
- Kocjancic, E.; Chung, E.; Garzon, J.A.; Haylen, B.; Iacovelli, V.; Jaunarena, J.; Locke, J.; Millman, A.; Nahon, I.; Ohlander, S.; et al. International Continence Society (ICS) Report on the Terminology for Sexual Health in Men with Lower Urinary Tract (LUT) and Pelvic Floor (PF) Dysfunction. Neurourol. Urodyn. 2022, 41, 140–165. [Google Scholar] [CrossRef]
- Thüroff, J.W.; Abrams, P.; Andersson, K.-E.; Artibani, W.; Chapple, C.R.; Drake, M.J.; Hampel, C.; Neisius, A.; Schröder, A.; Tubaro, A. Guías EAU Sobre Incontinencia Urinaria. Actas Urol. Esp. 2011, 35, 373–388. [Google Scholar]
- Mazariego, C.G.; Egger, S.; King, M.T.; Juraskova, I.; Woo, H.; Berry, M.; Armstrong, B.K.; Smith, D.P. Fifteen Year Quality of Life Outcomes in Men with Localised Prostate Cancer: Population Based Australian Prospective Study. BMJ 2020, 371, m3503. [Google Scholar] [CrossRef]
- Bø, K.; Berghmans, B.; Mørkved, S.; Van Kampen, M. Evidence-Based Physical Therapy for the Pelvic Floor, 3rd ed.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2023; ISBN 978-0-7020-8308-2. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF). Available online: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (accessed on 1 May 2024).
- Tian, Z.; Wang, X.; Fu, L.; Du, Z.; Sun, Z. Impact of Female Stress Urinary Incontinence and Related Treatments on the Sexual Function of Male Partners: A Systematic Review and Meta-Analysis. J. Sex. Med. 2023, 20, 1069–1077. [Google Scholar] [CrossRef]
- Gupta, N.; Zebib, L.; Wittmann, D.; Nelson, C.J.; Salter, C.A.; Mulhall, J.P.; Byrne, N.; Nolasco, T.S.; Loeb, S. Understanding the Sexual Health Perceptions, Concerns, and Needs of Female Partners of Prostate Cancer Survivors. J. Sex. Med. 2023, 20, 651–660. [Google Scholar] [CrossRef]
- Dumoulin, C.; Cacciari, L.P.; Hay-Smith, E.J.C. Pelvic Floor Muscle Training versus No Treatment, or Inactive Control Treatments, for Urinary Incontinence in Women. Cochrane Database Syst. Rev. 2018, 10, CD005654. [Google Scholar] [CrossRef]
- Khandelwal, C. Diagnosis of Urinary Incontinence. Urin. Incontinence 2013, 87, 8. [Google Scholar]
- Anderson, C.A.; Omar, M.I.; Campbell, S.E.; Hunter, K.F.; Cody, J.D.; Glazener, C.M.A. Conservative Management for Postprostatectomy Urinary Incontinence. Cochrane Database Syst. Rev. 2015, 1, CD001843. [Google Scholar] [CrossRef] [PubMed]
- Mungovan, S.F.; Carlsson, S.V.; Gass, G.C.; Graham, P.L.; Sandhu, J.S.; Akin, O.; Scardino, P.T.; Eastham, J.A.; Patel, M.I. Preoperative Exercise Interventions to Optimize Continence Outcomes Following Radical Prostatectomy. Nat. Rev. Urol. 2021, 18, 259–281. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, R.; Fink, H.A.; Huckabay, C.; Monga, M.; Wilt, T.J. Pelvic Floor Muscle Training to Improve Urinary Incontinence after Radical Prostatectomy: A Systematic Review of Effectiveness. BJU Int. 2007, 100, 76–81. [Google Scholar] [CrossRef]
- Reimer, N.; Zopf, E.M.; Böwe, R.; Baumann, F.T. Effects of Exercise on Sexual Dysfunction in Patients with Prostate Cancer—A Systematic Review. J. Sex. Med. 2021, 18, 1899–1914. [Google Scholar] [CrossRef]
- Bø, K. Physiotherapy Management of Urinary Incontinence in Females. J. Physiother. 2020, 66, 147–154. [Google Scholar] [CrossRef]
- Johnson, E.E.; Mamoulakis, C.; Stoniute, A.; Omar, M.I.; Sinha, S. Conservative Interventions for Managing Urinary Incontinence after Prostate Surgery. Cochrane Database Syst. Rev. 2023, 2023, CD014799. [Google Scholar] [CrossRef]
- National Library of Medecine. Treatment Adherence and Compliance. Available online: http://id.nlm.nih.gov/mesh/D000074822 (accessed on 20 July 2022).
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner, E. Barriers to Treatment Adherence in Physiotherapy Outpatient Clinics: A Systematic Review. Man. Ther. 2010, 15, 220–228. [Google Scholar] [CrossRef]
- Rizzo, J. Patients’ Mental Models and Adherence to Outpatient Physical Therapy Home Exercise Programs. Physiother. Theory Pract. 2015, 31, 253–259. [Google Scholar] [CrossRef]
- Campbell, R. Why Don’t Patients Do Their Exercises? Understanding Non-Compliance with Physiotherapy in Patients with Osteoarthritis of the Knee. J. Epidemiol. Community Health 2001, 55, 132–138. [Google Scholar] [CrossRef] [PubMed]
- McLean, S.M.; Burton, M.; Bradley, L.; Littlewood, C. Interventions for Enhancing Adherence with Physiotherapy: A Systematic Review. Man. Ther. 2010, 15, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, T.S.; Mottola, M.F.; Barakat, R.; Prapavessis, H. Adherence Is a Key Factor for Interpreting the Results of Exercise Interventions. Physiotherapy 2021, 113, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Latorre, G.F.S.; de Fraga, R.; Seleme, M.R.; Mueller, C.V.; Berghmans, B. An Ideal E-Health System for Pelvic Floor Muscle Training Adherence: Systematic Review. Neurourol. Urodyn. 2019, 38, 63–80. [Google Scholar] [CrossRef]
- Navarro-Brazález, B.; Vergara-Pérez, F.; Prieto-Gómez, V.; Sánchez-Sánchez, B.; Yuste-Sánchez, M.J.; Torres-Lacomba, M. What Influences Women to Adhere to Pelvic Floor Exercises after Physiotherapy Treatment? A Qualitative Study for Individualized Pelvic Health Care. J. Pers. Med. 2021, 11, 1368. [Google Scholar] [CrossRef]
- Dumoulin, C.; Hay-Smith, J.; Frawley, H.; McClurg, D.; Alewijnse, D.; Bo, K.; Burgio, K.; Chen, S.-Y.; Chiarelli, P.; Dean, S.; et al. 2014 Consensus Statement on Improving Pelvic Floor Muscle Training Adherence: International Continence Society 2011 State-of-the-Science Seminar. Neurourol. Urodyn. 2015, 34, 600–605. [Google Scholar] [CrossRef]
- Venegas, M.; Carrasco, B.; Casas-Cordero, R. Factors Influencing Long-Term Adherence to Pelvic Floor Exercises in Women with Urinary Incontinence. Neurourol. Urodyn. 2018, 37, 1120–1127. [Google Scholar] [CrossRef]
- Bernardes, M.F.V.G.; da Mata, L.R.F.; Azevedo, C.; Izidoro, L.C.d.R.; de Oliveira, C.M.C.; Chianca, T.C.M. Effectiveness of systemic acupuncture in the control of urinary incontinence following radical prostatectomy: A randomized clinical trial. Rev. Esc. Enferm. USP 2022, 56, e20220135. [Google Scholar] [CrossRef]
- Torres-Lacomba, M.; Navarro-Brazález, B.; Yuste-Sánchez, M.J.; Sánchez-Sánchez, B.; Prieto-Gómez, V.; Vergara-Pérez, F. Women’s Experiences with Compliance with Pelvic Floor Home Exercise Therapy and Lifestyle Changes for Pelvic Organ Prolapse Symptoms: A Qualitative Study. J. Pers. Med. 2022, 12, 498. [Google Scholar] [CrossRef]
- Sawettikamporn, W.; Sarit-Apirak, S.; Manonai, J. Attitudes and Barriers to Pelvic Floor Muscle Exercises of Women with Stress Urinary Incontinence. BMC Women’s Health 2022, 22, 477. [Google Scholar] [CrossRef]
- Cobo, C.M.S.; Camarero, A.R.A. Claves para el diseño y validación de cuestionarios en Ciencias de la Salud. Enferm. Cardiol. 2019, 26, 69–73. [Google Scholar]
- Bø, K.; Hilde, G. Does It Work in the Long Term?—A Systematic Review on Pelvic Floor Muscle Training for Female Stress Urinary Incontinence: Long-Term Outcome of Pelvic Floor Muscle Training. Neurourol. Urodyn. 2013, 32, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.J., 3rd. Intravaginal Stimulation Randomized Trial. J. Urol. 1996, 155, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Manonai, J.; Harnsomboon, T.; Sarit-apirak, S.; Wattanayingcharoenchai, R.; Chittacharoen, A.; Suthutvoravut, S. Effect of Colpexin Sphere on Pelvic Floor Muscle Strength and Quality of Life in Women with Pelvic Organ Prolapse Stage I/II: A Randomized Controlled Trial. Int. Urogynecology J. 2012, 23, 307–312. [Google Scholar] [CrossRef]
- Ferro García, R.; García Ríos, M.C.; Vives Montero, M.C. Un análisis de la adherencia al tratamiento en fisioterapia. Fisioterapia 2004, 26, 333–339. [Google Scholar] [CrossRef]
- Fuentes-Aparicio, L.; Rejano-Campo, M.; Lopez-Bueno, L.; Marie Donnelly, G.; Balasch-Bernat, M. The Effect of an Abdominopelvic Exercise Program Alone versus in Addition to Postural Instructions on Pelvic Floor Muscle Function in Climacteric Women with Stress Urinary Incontinence. A Randomized Controlled Trial. Physiother. Theory Pract. 2023, 4, 738–749. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Gomez-Conesa, A.; Serrano, C.S.; Matamoros, D.C.; López-López, J.A. The Spanish Translation and Adaptation of the Pedro Scale. Physiotherapy 2015, 101, e463–e464. [Google Scholar] [CrossRef]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Sanabria, A.; Rigau, D.; Rotaeche, R.; Selva, A.; Marzo-Castillejo, M.; Alonso-Coello, P. Sistema GRADE: Metodología para la realización de recomendaciones para la práctica clínica. Atención Primaria 2015, 47, 48–55. [Google Scholar] [CrossRef]
- Glazener, C.; Boachie, C.; Buckley, B.; Cochran, C.; Dorey, G.; Grant, A.; Hagen, S.; Kilonzo, M.; McDonald, A.; McPherson, G.; et al. Urinary incontinence in men after formal one-to-one pelvic-floor muscle training following radical prostatectomy or transurethral resection of the prostate (MAPS): Two par-allel randomised controlled trials. Lancet 2011, 378, 328–337. [Google Scholar] [CrossRef]
- Glazener, C.M.; Herbison, G.P.; Wilson, P.D.; MacArthur, C.; Lang, G.D.; Gee, H.; Grant, A.M. Conservative Management of Persistent Postnatal Urinary and Faecal Incontinence: Randomised Controlled Trial. BMJ 2001, 323, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Jaffar, A.; Mohd Sidik, S.; Foo, C.N.; Muhammad, N.A.; Abdul Manaf, R.; Suhaili, N. Preliminary Effectiveness of mHealth App-Based Pelvic Floor Muscle Training among Pregnant Women to Improve Their Exercise Adherence: A Pilot Randomised Control Trial. Int. J. Environ. Res. Public Health 2022, 19, 2332. [Google Scholar] [CrossRef] [PubMed]
- Sacomori, C.; Zomkowski, K.; Dos Passos Porto, I.; Cardoso, F.L.; Sperandio, F.F. Adherence and Effectiveness of a Single Instruction of Pelvic Floor Exercises: A Randomized Clinical Trial. Int. Urogynecology J. 2020, 31, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Alagirisamy, P.; Sidik, S.M.; Rampal, L.; Ismail, S.I.F. Effectiveness of a Pelvic Floor Muscle Exercise Intervention in Improving Knowledge, Attitude, Practice, and Self-Efficacy among Pregnant Women: A Randomized Controlled Trial. Korean J. Fam. Med. 2022, 43, 42–55. [Google Scholar] [CrossRef]
- Sahin, U.K.; Acaroz, S.; Cirakoglu, A.; Benli, E.; Akbayrak, T. Effects of External Electrical Stimulation Added to Pelvic Floor Muscle Training in Women with Stress Urinary Incontinence: A Randomized Controlled Study. Neurourol. Urodyn. 2022, 8, 1781–1792. [Google Scholar] [CrossRef]
- Kaya, S.; Akbayrak, T.; Gursen, C.; Beksac, S. Short-Term Effect of Adding Pelvic Floor Muscle Training to Bladder Training for Female Urinary Incontinence: A Randomized Controlled Trial. Int. Urogynecology J. 2015, 26, 285–293. [Google Scholar] [CrossRef]
- Wilson, P.D.; Herbison, G.P. A Randomized Controlled Trial of Pelvic Floor Muscle Exercises to Treat Postnatal Urinary Incontinence. Int. Urogynecol. J. Pelvic Floor Dysfunct. 1998, 9, 257–264. [Google Scholar] [CrossRef]
- Alewijnse, D.; Mesters, I.; Metsemakers, J.; van den Borne, B. Predictors of Long-Term Adherence to Pelvic Floor Muscle Exercise Therapy among Women with Urinary Incontinence. Health Educ. Res. 2003, 18, 511–524. [Google Scholar] [CrossRef]
- Glazener, C.M.A.; MacArthur, C.; Hagen, S.; Elders, A.; Lancashire, R.; Herbison, G.P.; Wilson, P.D. Twelve-Year Follow-up of Conservative Management of Postnatal Urinary and Faecal Incontinence and Prolapse Outcomes: Randomised Controlled Trial. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 112–120. [Google Scholar] [CrossRef]
- Souto-Miranda, S.; Brazete Cruz, E.; Pires, D.; Ribeiro, F.; Cordeiro, N.; Jácome, C. Priorities in Physical Therapy Research: A Scoping Review. Braz. J. Phys. Ther. 2024, 28, 101135. [Google Scholar] [CrossRef]
- Burgio, K.L.; Locher, J.L.; Goode, P.S.; Hardin, J.M.; McDowell, B.J.; Dombrowski, M.; Candib, D. Behavioral vs Drug Treatment for Urge Urinary Incontinence in Older Women: A Randomized Controlled Trial. JAMA 1998, 280, 1995–2000. [Google Scholar] [CrossRef] [PubMed]
- Borello-France, D.F.; Zyczynski, H.M.; Downey, P.A.; Rause, C.R.; Wister, J.A. Effect of Pelvic-Floor Muscle Exercise Position on Continence and Quality-of-Life Outcomes in Women with Stress Urinary Incontinence. Phys. Ther. 2006, 86, 974–986. [Google Scholar] [PubMed]
- Sanchez-Salas, R.; Tourinho-Barbosa, R.; Sivaraman, A.; Borges, R.C.; Candela, L.; Cathala, N.; Mombet, A.; Marra, G.; Sanchez, L.R.; Boumezrag, C.B.; et al. Assessing the Efficacy of Pelvic Floor Muscle Training and Duloxetine on Urinary Continence Recovery Following Radical Prostatectomy: A Randomized Clinical Trial. Prostate 2024, 84, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, D.; Lampropoulou, S.; Giannitsas, K.; Skoura, A.; Fousekis, K.; Billis, E. Pelvic Floor Muscle Training: Novel versus Traditional Remote Rehabilitation Methods. A Systematic Review and Meta-Analysis on Their Effectiveness for Women with Urinary Incontinence. Neurourol. Urodyn. 2023, 42, 856–874. [Google Scholar] [CrossRef]

| Author/ Year/ Country | n/Participants/ Dysfunction | Intervention/ Follow Up | Outcomes Measures/Instruments |
|---|---|---|---|
| Glazener et al. (2011) [47] UK | n = 853 Men UI (SUI, MUI, UUI) 6 wk after RP prostate cancer or TURP in the case of BPH | 3 mo. EG: PFMT. Bladder training if IUU. CG: Standard care (non-expert advice on PFMT.) Follow up: 12 mo. | MO: subjective report of urinary continence at 12 mo. Primary cost-effectiveness measure: QALYs. SO: clinical outcomes: urinary outcomes (presence, frequency, and severity of incontinence, effect of incontinence on quality of life, use of pads and catheters, type of incontinence, urinary frequency, and nocturia); bowel outcomes (fecal incontinence, constipation, bowel urgency); sexual function (erectile function, ejaculation, change in sexual function) QoL, health service use for UI, other health service use, effects of interventions (PFMT use and lifestyle changes), and economic measures. ADH, Satisfaction with treatment. MAPS Questionnaire: ICI-SF/10-point scale ICI-Q/Short Form questionnaire-12 items (SF-12)/European Quality of Life-5 Dimensions (EQ-5D)/3 days urinary diary QALYs derived from responses to the EQ-5D and SF-12; and the effect of the intervention in changing health-related behavior and practice of PFMT and bladder training or urge suppression. |
| Glazener et al. (2001) [48] UK/New Zealand | n = 747 Women SUI/ UUI /MUI /FI persistent 3 months postpartum | 1 visit with reviews at 7 y 9 mo. EG: PFMT (5 mo. postpartum), bladder training, if necessary, at visit 7/9 mo. CG: peripartum preparation such as EG, (sometimes included PFMT) Follow up: 12 mo. EG: home-based PFMT/CG: nothing | Does not assess in the intervention. Follow up: MO: persistence and severity of UI 12 mo. postpartum. SO: PFMT performance, change in coexisting FI, well-being, and overall UI severity rating. Anxiety and depression. Other: PFMT use and frequency and pad use. UI Severity (at least 1 time/wk). FI Severity. HADS/ADH: questionnaire. |
| Jaffar et al. (2022) [49] Malaysia | n = 26 pregnant women >18 yr with SUI/MUI | 2 mo. EG: 8 wk behavioral change intervention PFMT KEPT app. (mHealth) GC: regular antenatal care. (APP after 8 wk). No follow-up | MO: PFMT ADH SO: UI, Symptomatic severity of UI, QoL, knowledge, attitude, practice, and self-efficacy of PFMT. (EARS)/ICIQ-UI SF/ICIQ-LUTSqol/validated scale/SESPPFE |
| Sacomori et al. (2020) [50] Brazil | n = 202 women > 18 yr postpartum period with a living child SUI | 1 individual postpartum session. EG: home-based PFMT during breastfeeding. CG: Routine postpartum hospital care (no PFMT) Follow up: 3 mo. EG: Unsupervised home-based PFMT/CG: none. | EG/CG Urinary symptoms before pregnancy/3rd trimester/3rd month postpartum after 1 session of PFMT training (ITT). QoL baseline/3º trimester. Follow up: (in abstract it appears as a primary measure QoL). MO: ADH (time spent exercising) and barriers to treatment. (EG) SO: Involuntary loss of urine and QoL Questionnaire/ICIQ-SF |
| Alagirisamy et al. (2022) [51] Malaysia | n = 170 women pregnancy- Postpartum UI | Before 22 wk gestation and up to 38 wk gestation. EG: PFMT + perinatal care. CG: Perinatal, ante, and postnatal hospital care (includes info UI/PFMT). Follow-up: 4–6 wk after delivery. | MO: knowledge, attitude, practice, and self-efficacy of PFMT. SO: Continence and UI Severity EG/CG at baseline and at 3 time points: 1T (28–30 wk gestation), 2T (36–38 wk gestation), and 3T (4–6 wk postpartum). KAP Q/SESPPFE/ICIQ-UI SF |
| Sahin et al. (2022) [52] Turkey | n = 60 Women UI SUI | 2 mo. Home-based PFMT. G1: EES G2: PFMT G3: EES + PFMT No follow-up. | Self-reported improvement/UI severity/symptomatic distress/QoL/UI episodes/strength, endurance/dysfunction ADH. 4 items Likert scale/KHQ/pad test/ISI/24 h urinary dairy/perineometry/PFDI-20. ADH: VAS scale |
| Kaya et al. (2015) [53] Turkey | n = 132 Women SUI UUI MUI | 6 wk. BT: bladder training. EG: BT + PFMT CG: BT No follow-up. | MO: Self-reported improvement SO: UI severity/symptomatic distress/QoL/average nº of UI episodes and urination per day/strength (PFMS) endurance (PFME). 4 items Likert scale/ISI/UDI-6/IIQ-7/3 24-h frequency-volume graph on three different days/diaries/perineometry. ADH: VAS |
| Study | Length | Freq. (Times/d) | Dosage |
|---|---|---|---|
| Glazener et al. (2011) [47] | 3 mo. F.U: 12 mo. | Daily (×2) | EG 3 maximum con. Up to 10 s/10 s rest. Decubitus, Sitting, and standing. |
| Glazener et al. (2001) [48] | Single session F.U:12 mo. | Daily | EG 8 to 10 sets of fast and slow con. Until 80–100 repetitions are reached. |
| Jaffar et al. (2022) [49] | 2 mo. | Daily (×3) | EG Beginner: 2 s con./Intermediate: 6 s con./Expert: 10 s. con./6 s rest × 10 rep. |
| Sacomori et al. (2020) [50] | Single intervention F.U:3 mo. | Daily (×2) | EG 10 reps. of 10 s of maximum intensity/10 rep. of 1 s. |
| Alagirisamy et al. (2022) [51] | 4 mo. F.U:1.5 mo. | No information. | No information. |
| Sahin et al. (2022) [52] | 2 mo. | Daily | (G2/G3) Home 1 set 10 fast 10 slow con. (5 s, hold 10 s/5 s). 2 1st week, 2 sets/d (20 fast and 20 slow). Every 2 weeks, 2 more sets were added, 8 sets (80 fast and 80 slow con./d at the end of 8th week. Sitting, supine, semi-squatting, and standing. |
| Kaya et al. (2015) [53] | 1.5 mo. | Daily | EG Home-based. Fast (2 s) and slow.1 slow con. 15 s (5 s con./5 s maintenance/5 s relaxation). 1 set 10 fast/10 slow. 1st wk 5 sets/d (5 × 10 fast and 10 slow) progressively >5 sets/wk: 30 in the 6th wk daily (300/300). Supine, sitting and standing. |
| Study | Randomized (n) | Participants Completed the Treatment Period-Dropped Out | % of Follow-Up Losses (Time Elapsed) |
|---|---|---|---|
| Glazener et al. (2011) [47] | RP n = 411 (EG = 205, CG =206) | RP n = 391 (EG = 196, CG = 195) RP n = 20 (EG = 9, CG = 11) | Total: 5% (12 mo.) RP: EG 4%, CG 5% |
| TUPR n = 442 (EG = 220, CG = 222) | TUPR n = 397 (EG = 194, CG = 203) TUPR n = 45 (EG = 26, CG = 19) | Total 10% (12 mo.) TUPR: EG 12%, CG 8.5% | |
| Glazener et al. (2001) [48] | n = 747 (EG = 371, CG = 376) | n = 692 (EG = 371; [Received intervention as allocated = 316 ITT], CG = 376) n = 223 (EG = 92, CG = 131) | Total: 30% (12 mo.) EG 25%, CG 35% |
| Jaffar et al. (2022) [49] | n = 26 (EG = 16, CG = 10) | n = 16 (EG = 10; [ITT = 13], CG = 6 [ITT = 10]) n = 12 (EG = 6, CG = 6) | Total: 46% (2 mo.) EG 37.5%, CG 60% |
| Sacomori et al. (2020) [50] | n = 202 (EG = 98, CG = 104) | n = 132 (EG = 67, CG = 65) n = 70 (EG = 31, CG = 39) | Total: 35% (3 mo.) EG 31%, CG 37.5% |
| Alagirisamy et al. (2022) [51] | n = 170 (EG = 85, CG = 85) ITT Modified analysis (EG = 65, CG = 59) | n = 21 (EG = 10, CG = 11) n = 149 (EG = 75, CG = 74) | Total: 87% (3 mo.) EG 88%, CG 87% |
| Sahin et al. (2022) [52] | n = 60 (G1 = 20, G2 = 20, G3 = 20) | n = 51 (G1 = 17, G2 = 17, G3 = 17) n = 9 (G1 = 3, G2 = 3, G3 = 3) | (No follow-up) Total: 15% EG 15%, CG 15% complete the intervention. |
| Kaya et al. (2015) [53] | n = 132 (EG = 67, CG = 65) | n = 108 (EG = 56, CG = 52) n = 24 (EG = 11, CG = 13) | (No follow up) Total: 18% EG 16%, CG 20% |
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Glazener et al. (2011) [47] | Y | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 |
| Glazener et al. (2001) [48] | Y | Y | Y | Y | N | N | N | N | Y | Y | Y | 6 |
| Jaffar et al. (2022) [49] | Y | Y | Y | Y | N | N | Y | N | Y | Y | Y | 7 |
| Sacomori et al. (2020) [50] | Y | Y | Y | Y | N | N | N | N | Y | Y | Y | 6 |
| Alagirisamy et al. (2022) [51] | Y | Y | Y | Y | Y | N | N | N | Y | Y | Y | 7 |
| Sahin et al. (2022) [52] | Y | Y | Y | Y | N | N | N | N | N | Y | Y | 5 |
| Kaya et al. (2015) [53] | Y | Y | Y | Y | N | N | N | N | N | Y | Y | 5 |
| Study | Instrument | Results Intervention Period. | Results Follow-Up Period. | Boosters’ Strategies |
|---|---|---|---|---|
| Glazener et al. (2011) [47] | Men after prostate surgery (MAPS) Questionnaire. Practice and frequency | PR EG: 92% attended at least 1 session, and 82% attended all 4 sessions. TURP EG: 86% attended at least 1 session, and 72% attended all 4. | Over 90% returned complete questionnaires. PFMT at 12 mo.: PR: EG > CG RP EG 67%/PR CG 50%. RR 1.30, 95% CI 1.09 to 1.53. TURP: EG > CG EG: 65%/TURP CG: 20% RR 3.20, 95% CI 2.37 to 4.32. | In both EG: Booklet with instructions and reminder for PFMT and bladder training. CG no |
| Glazener et al. (2001) [48] | Modified version of the questionnaire [54] Frequency and amount of exercise. | No data collected in this period | Response rate questionnaire EG 75%/CG 65% PFMT performance EG > CG 79%/48% p < 0.001 contractions per day and Mean nº /day GE > CG 20 (29) v 5 (15), 11 to 19, p < 0.001 | Visits at 7 and 9 months after delivery in EG. CG no |
| Jaffar et al. (2022) [49] | (EARS) Exercise adherence rate scale: 6 items PFMT practice (0–24) High score-high ADH. Forget/as often/do not move around/perform some, but not all, of my exercises/fit into a regular routine/perform less than recommended. KAP Q | EG: Minimal significant improvement in adherence to PFMT after 2 months of training (β = 0.033, p = 0.019). | No follow-up | Specific mobile APP (KEPT app) in the EG. With a progress chart and calendar. |
| Sacomori et al. (2020) [50] | Questionnaire[55] Time spent exercising and barriers to treatment. | No data collected in this period. | EG: 57 (85.1%) general ADH. % home-based PFMT: 32.3% 1–2 times/wk 49.3% 3–7 times/week Duration of exercise: 21 (31.3%) 3 mo. postpartum; rest 2 mo. | EG: Information leaflet for unsupervised home-based sessions. |
| Alagirisamy et al. (2022) [51] | Knowledge Attitude Practice (KAP) questionnaire (section practice 5 questions). | PFMT practise EG > CG (p < 0.001) Change from baseline in T1–T3 Significant increase in the practice score by 1.18 points (p = 0.038) from T1 to T3. | EG/CG marginal increase in the practice score (0, 65 points, p = 0.051) from the end of the 3rd trimester to the beginning of the postnatal period. | EG: Reminder messages and booster sessions. CG no |
| Sahin et al. (2022) [52] | 100 mm visual analog scale. 0 “never completed exercises”–10 “I performed all activities”. | 83%G2/91%G3 EES(G1) reported a high level of assistance. | No follow-up | Bi-weekly assistance. EES (for the EES and PFMT + EES group) was performed under the supervision of a physiotherapist 3 days a week in the clinic. |
| Kaya et al. (2015) [53] | 100 mm visual analog scale. 10 mm increments 0% no compliance to 100% full compliance. | High in EG Bladder Training (BT) +PFMT 85% (IQR = 75, 0–100%). | No follow-up | Brief instruction sheet on BT and/or PFMT. EG (PFMT + BT) diary of exercise. |
| Study | Symptomatic Severity Pre- and Post-Data in the Intervention/Follow-Up Period | Quality of Life Pre- and Post-Data in The Intervention/Follow-Up Period | Results in Terms of Sexual Health |
|---|---|---|---|
| Glazener et al. (2011) [47] | p > 0.05 between groups in both interventions. Decreased improvement. | p > 0.05 between groups | There was no evidence from MAPS that PFMT was effective for treating sexual dysfunction. |
| p > 0.05 between groups in both interventions. Decreased improvement. | p > 0.05 Improved QoL (because of the recovery from surgery) | ||
| Glazener et al. (2001) [48] | No data collected in this period | No data collected in this period | Possible improvement of sexual health indirectly through improvement of IU-FI severity. |
| Significant difference in favor of EG UI severity (X 2 = 9.49, p = 0.002). Use of sanitary towels (X 2 = 4.49, p = 0.034). Mean pad changes (t = −2.65, p = 0.008). Severity of FI (X 2 = 3.17, p = 0.075). | p > 0.05 in general well-being or depression. EG showed lower levels of anxiety (t = −2.08, p = 0.038). | ||
| Jaffar et al. (2022) [49] | UI severity: EG improves severity in the first month (β = −4.748, p = 0.049), but this improvement does not persist in the 2nd mo. | QoL: no improvement is shown in participants in the 1st and 2nd mo. | Possibly no improvement in sexual health. |
| No follow-up | No follow-up | ||
| Sacomori et al. (2020) [50] | p > 0.05 All urinary functions declined in 3rd trimester compared with before pregnancy. | p > 0.05 Improvement | Possible improvement of sexual health indirectly through improvement of quality of life in both groups |
| p > 0.05 All urinary functions improved in 3rd mo. postpartum | p > 0.05 (ICIQ-SF) Improvement | ||
| Alagirisamy et al. (2022) [51] | EG significant reduction in UI severity compared with CG, which increased (Late third trimester). p < 0.001 | Measured by self-reported ICIQ-UI-SF with severity | Possible improvement of sexual health in the EG indirectly through improvement of IU severity. Improvement was not observed in the self-reported UI |
| EG > CG with an estimated mean difference of change between 0.44 and 2.54 (p < 0.001). | Measured by self-reported ICIQ-UI-SF with severity | ||
| Sahin et al. (2022) [52] | Significant changes in all groups (p < 0.05). p > 0.05 between groups. All significant increases in Pelvic floor muscle strength and endurance (p < 0.001) but did not differ significantly among groups (p > 0.05) | Significant changes in all groups (p < 0.05) but did not significantly differ (p > 0.05), except for the incontinence impact subdomain (p < 0.05) G3 EES + PFMT > G1 EES/G3 PFMT | Possible improvement of sexual health directly through improvement of the quality of life in both groups. |
| No follow-up | No follow-up | ||
| Kaya et al. (2015) [53] | Global rating of improvement: EG > CG (100% vs. 82.7%, p = 0.001). Significant differences in EG for SUI (p = 0.001) and MUI (p = 0.038) but not for UUI (p = 0.352). | p > 0.05 between changes in symptom distress or QOL impact scores in MUI UUI QoL EG > CG (p = 0.045) SUI EG > CG Improve symptom distress (p = 0.001) or QOL impact scores (p = 0.005 and p = 0.040) (UDI-6 score/IIQ-7 score) | Possible improvement of sexual health in the EG indirectly through improvement of IU severity and QoL |
| No follow-up | No follow-up |
| Study | Scenario | Treatment Adherence and Compliance | Symptomatic Severity–Quality of Life |
|---|---|---|---|
| Glazener et al. (2011) [47] | 1 | Low adherence | No significant effect of intervention or improvement is observed in comparison with the inactive control group. |
| Glazener et al. (2001) [48] | 3 | Low adherence | Intervention favors the experimental group over the control group |
| Jaffar et al. (2022) [49] | NA | Showed minimal or significant improvement in adherence but did not show whether it was greater or lower than 80%. | No significant effect of intervention or improvement is observed in comparison with the inactive control group. |
| Sacomori et al. (2020) [50] | 2 | High adherence | No significant effect of intervention or improvement is observed in comparison with the inactive control group. |
| Alagirisamy et al. (2022) [51] | NA | Showed minimal or significant improvement in adherence but did not show whether it was greater or lower than 80%. | Intervention favors the experimental group over the control group |
| Sahin et al. (2022) [52] | 2 | High adherence | No significant effect of intervention or improvement is observed in comparison with the inactive control group. |
| Kaya et al. (2015) [53] | 4 | High adherence | Intervention favors the experimental group over the control group |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villa-Del-Pino, I.; Jiménez-Rejano, J.-J.; Rebollo-Salas, M.; Rodríguez-Domínguez, Á.-J.; Suárez-Serrano, C.-M. Compliance and Adherence to Pelvic Floor Exercise Therapy in People with Pelvic Floor Disorders: A Systematic Review and Meta-Analysis. Life 2025, 15, 613. https://doi.org/10.3390/life15040613
Villa-Del-Pino I, Jiménez-Rejano J-J, Rebollo-Salas M, Rodríguez-Domínguez Á-J, Suárez-Serrano C-M. Compliance and Adherence to Pelvic Floor Exercise Therapy in People with Pelvic Floor Disorders: A Systematic Review and Meta-Analysis. Life. 2025; 15(4):613. https://doi.org/10.3390/life15040613
Chicago/Turabian StyleVilla-Del-Pino, Inmaculada, José-Jesús Jiménez-Rejano, Manuel Rebollo-Salas, Álvaro-José Rodríguez-Domínguez, and Carmen-María Suárez-Serrano. 2025. "Compliance and Adherence to Pelvic Floor Exercise Therapy in People with Pelvic Floor Disorders: A Systematic Review and Meta-Analysis" Life 15, no. 4: 613. https://doi.org/10.3390/life15040613
APA StyleVilla-Del-Pino, I., Jiménez-Rejano, J.-J., Rebollo-Salas, M., Rodríguez-Domínguez, Á.-J., & Suárez-Serrano, C.-M. (2025). Compliance and Adherence to Pelvic Floor Exercise Therapy in People with Pelvic Floor Disorders: A Systematic Review and Meta-Analysis. Life, 15(4), 613. https://doi.org/10.3390/life15040613