
The Contemporary Role of Speckle Tracking Echocardiography in Cirrhotic Cardiomyopathy

 , , ,
, , , 
Abstract
1. Introduction
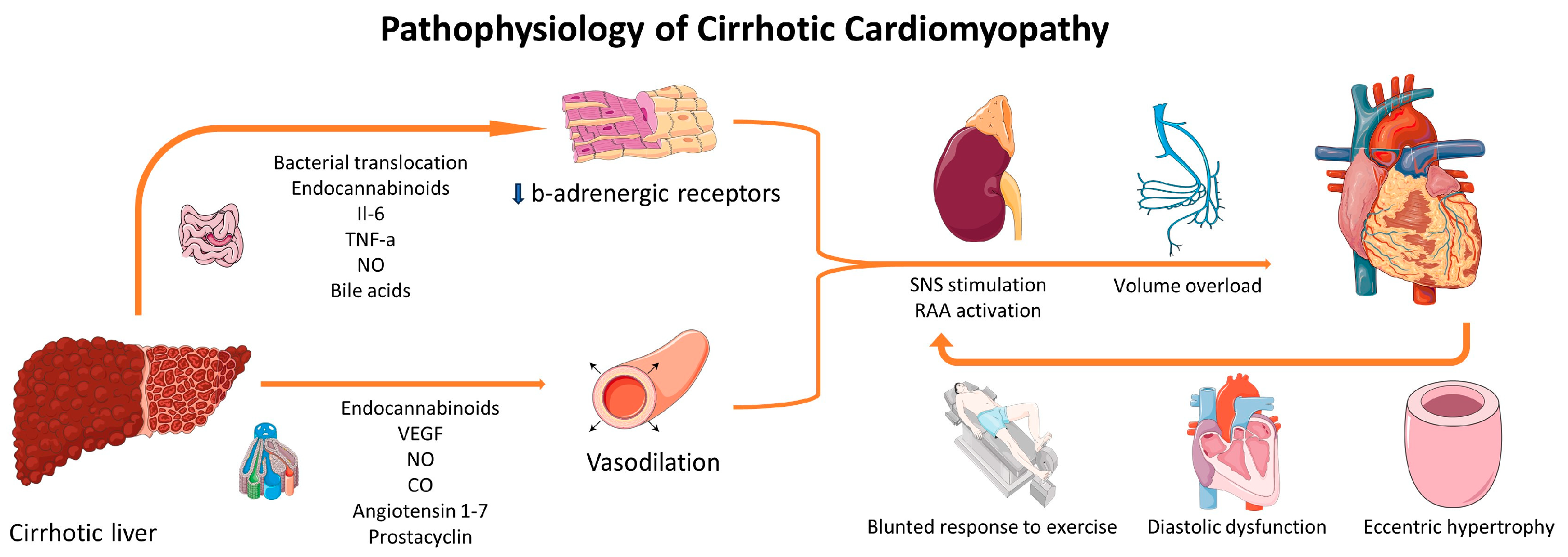
2. Pathophysiology of CCM
3. Diagnosis of CCM
4. How Different Are Left Ventricular Strain Values of Cirrhotic Patients When Compared to Controls?
5. Are Left Ventricular Strain Values Associated with Disease Severity and Prognosis?
6. In What Proportion of Cirrhotic Patients Do GLS Values Satisfy the Systolic Criterion for the Diagnosis of CCM?
7. Speckle Tracking Echocardiography for the Evaluation of Left Atrial Function in Cirrhotic Patients
8. Speckle Tracking Echocardiography for the Evaluation of Right Ventricular and Right Atrial Function in Cirrhotic Patients
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ma, Z.; Lee, S.S. Cirrhotic Cardiomyopathy: Getting to the Heart of the Matter. Hepatology 1996, 24, 451–459. [Google Scholar] [CrossRef]
- Wiese, S.; Hove, J.D.; Bendtsen, F.; Møller, S. Cirrhotic Cardiomyopathy: Pathogenesis and Clinical Relevance. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 177–186. [Google Scholar] [CrossRef]
- Bernardi, M.; Rubboli, A.; Trevisani, F.; Cancellieri, C.; Ligabue, A.; Baraldini, M.; Gasbarrini, G. Reduced Cardiovascular Responsiveness to Exercise-Induced Sympathoadrenergic Stimulation in Patients with Cirrhosis. J. Hepatol. 1991, 12, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Zardi, E.M.; Zardi, D.M.; Chin, D.; Sonnino, C.; Dobrina, A.; Abbate, A. Cirrhotic Cardiomyopathy in the Pre- and Post-Liver Transplantation Phase. J. Cardiol. 2016, 67, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Eimer, M.J.; Wright, J.M.; Wang, E.C.; Kulik, L.; Blei, A.; Flamm, S.; Beahan, M.; Bonow, R.O.; Abecassis, M.; Gheorghiade, M. Frequency and Significance of Acute Heart Failure Following Liver Transplantation. Am. J. Cardiol. 2008, 101, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the Management of Patients with Decompensated Cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef]
- Dimitroglou, Y.; Aggeli, C.; Alexopoulou, A.; Mavrogeni, S.; Tousoulis, D. Cardiac Imaging in Liver Transplantation Candidates: Current Knowledge and Future Perspectives. J. Clin. Med. 2019, 8, 2132. [Google Scholar] [CrossRef]
- Kalam, K.; Otahal, P.; Marwick, T.H. Prognostic Implications of Global LV Dysfunction: A Systematic Review and Meta-Analysis of Global Longitudinal Strain and Ejection Fraction. Heart 2014, 100, 1673–1680. [Google Scholar] [CrossRef]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc. Imaging 2018, 11, 260–274. [Google Scholar] [CrossRef]
- Izzy, M.; VanWagner, L.B.; Lin, G.; Altieri, M.; Findlay, J.Y.; Oh, J.K.; Watt, K.D.; Lee, S.S. Redefining Cirrhotic Cardiomyopathy for the Modern Era. Hepatology 2020, 71, 334–345. [Google Scholar] [CrossRef]
- Moller, S.; Hobolth, L.; Winkler, C.; Bendtsen, F.; Christensen, E. Determinants of the Hyperdynamic Circulation and Central Hypovolaemia in Cirrhosis. Gut 2011, 60, 1254–1259. [Google Scholar] [CrossRef]
- Abraldes, J.G.; Iwakiri, Y.; Loureiro-Silva, M.; Haq, O.; Sessa, W.C.; Groszmann, R.J. Mild Increases in Portal Pressure Upregulate Vascular Endothelial Growth Factor and Endothelial Nitric Oxide Synthase in the Intestinal Microcirculatory Bed, Leading to a Hyperdynamic State. Am. J. Physiol. Gastrointest. Liver Physiol. 2006, 290, G980–G987. [Google Scholar] [CrossRef] [PubMed]
- Iwakiri, Y.; Shah, V.; Rockey, D.C. Vascular Pathobiology in Chronic Liver Disease and Cirrhosis—Current Status and Future Directions. J. Hepatol. 2014, 61, 912–924. [Google Scholar] [CrossRef] [PubMed]
- Vilas-Boas, W.W.; Ribeiro-Oliveira, A., Jr.; Pereira, R.M.; Ribeiro, R.d.C.; Almeida, J.; Nadu, A.P.; e Silva, A.C.S.; dos Santos, R.A.S. Relationship between Angiotensin-(1-7) and Angiotensin II Correlates with Hemodynamic Changes in Human Liver Cirrhosis. World J. Gastroenterol. 2009, 15, 2512. [Google Scholar] [CrossRef] [PubMed]
- Batkai, S.; Jarai, Z.; Wagner, J.; Goparaju, S.; Varga, K.; Liu, J.; Wang, L.; Mirshahi, F.; Khanolkar, A.; Makriyannis, A.; et al. Endocannabinoids Acting at Vascular CB 1 Receptors Mediate the Vasodilated State in Advanced Liver Cirrhosis. Nat. Med. 2001, 7, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Hennenberg, M.; Trebicka, J.; Sauerbruch, T.; Heller, J. Mechanisms of Extrahepatic Vasodilation in Portal Hypertension. Gut 2008, 57, 1300–1314. [Google Scholar] [CrossRef]
- Stadlbauer, V.P.; Wright, G.A.K.; Banaji, M.; Mukhopadhya, A.; Mookerjee, R.; Moore, K.; Jalan, R.; Moore, K.; Jalan, R. Relationship Between Activation of the Sympathetic Nervous System and Renal Blood Flow Autoregulation in Cirrhosis. Gastroenterology 2008, 134, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Fasolato, S.; Rosi, S.; Angeli, P. Cardiac Dysfunction in Patients with Cirrhosis: Is the Systolic Component Its Main Feature? Eur. J. Gastroenterol. Hepatol. 2015, 27, 660–666. [Google Scholar] [CrossRef]
- Simões e Silva, A.C.; Miranda, A.S.; Rocha, N.P.; Teixeira, A.L. Renin Angiotensin System in Liver Diseases: Friend or Foe? World J. Gastroenterol. 2017, 23, 3396. [Google Scholar] [CrossRef]
- Ma, Z.; Miyamoto, A.; Lee, S.S. Role of Altered Beta-Adrenoceptor Signal Transduction in the Pathogenesis of Cirrhotic Cardiomyopathy in Rats. Gastroenterology 1996, 110, 1191–1198. [Google Scholar] [CrossRef]
- Wong, F.; Girgrah, N.; Graba, J.; Allidina, Y.; Liu, P.; Blendis, L. The Cardiac Response to Exercise in Cirrhosis. Gut 2001, 49, 268–275. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; Melenovsky, V.; Redfield, M.M.; Nishimura, R.A.; Borlaug, B.A. High-Output Heart Failure: A 15-Year Experience. J. Am. Coll. Cardiol. 2016, 68, 473–482. [Google Scholar] [CrossRef]
- Ortiz-Olvera, N.X.; Castellanos-Pallares, G.; Gómez-Jiménez, L.M.; Cabrera-Muñoz, M.L.; Méndez-Navarro, J.; Morán-Villota, S.; Dehesa-Violante, M. Anatomical Cardiac Alterations in Liver Cirrhosis: An Autopsy Study. Ann. Hepatol. 2011, 10, 321–326. [Google Scholar] [CrossRef]
- Wiese, S.; Hove, J.; Mo, S.; Mookerjee, R.P.; Petersen, C.L.; Vester-Andersen, M.K.; Mygind, N.D.; Goetze, J.P.; Kjær, A.; Bendtsen, F.; et al. Myocardial Extracellular Volume Quantified by Magnetic Resonance Is Increased in Cirrhosis and Related to Poor Outcome. Liver Int. 2018, 38, 1614–1623. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, M.; Devurgowda, D.; Vyas, T.; Shasthry, S.M.; Khumuckham, J.S.; Goyal, R.; Thomas, S.S.; Kumar, G. Left Ventricular Diastolic Dysfunction Is Associated with Renal Dysfunction, Poor Survival and Low Health Related Quality of Life in Cirrhosis. J. Clin. Exp. Hepatol. 2019, 9, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulou, A.; Papatheodoridis, G.; Pouriki, S.; Chrysohoou, C.; Raftopoulos, L.; Stefanadis, C.; Pectasides, D. Diastolic Myocardial Dysfunction Does Not Affect Survival in Patients with Cirrhosis. Transpl. Int. 2012, 25, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Collier, P.; Phelan, D.; Klein, A. A Test in Context: Myocardial Strain Measured by Speckle-Tracking Echocardiography. J. Am. Coll. Cardiol. 2017, 69, 1043–1056. [Google Scholar] [CrossRef]
- Stundiene, I.; Sarnelyte, J.; Norkute, A.; Aidietiene, S.; Liakina, V.; Masalaite, L.; Valantinas, J. Liver Cirrhosis and Left Ventricle Diastolic Dysfunction: Systematic Review. World J. Gastroenterol. 2019, 25, 4779–4795. [Google Scholar] [CrossRef]
- Almeida, J.G.; Fontes-Carvalho, R.; Sampaio, F.; Ribeiro, J.; Bettencourt, P.; Flachskampf, F.A.; Leite-Moreira, A.; Azevedo, A. Impact of the 2016 ASE/EACVI Recommendations on the Prevalence of Diastolic Dysfunction in the General Population. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 380–386. [Google Scholar] [CrossRef]
- Park, J.; Lee, J.; Kwon, A.; Choi, H.J.; Chung, H.S.; Hong, S.H.; Park, C.S.; Choi, J.H.; Chae, M.S. The 2016 ASE/EACVI Recommendations May Be Able to More Accurately Identify Patients at Risk for Diastolic Dysfunction in Living Donor Liver Transplantation. PLoS ONE 2019, 14, e0215603. [Google Scholar] [CrossRef]
- Marella, H.; Yedlapati, N.; Kothadia, J.P.; Mupparaju, V.K.; Marella, S.; Nair, S. Impact of Left Ventricular Diastolic Dysfunction on Liver Transplantation Outcomes Based on the Latest American Society of Echocardiography/European Association of Cardiovascular Imaging Recommendations. Clin. Exp. Hepatol. 2021, 7, 390–395. [Google Scholar] [CrossRef]
- Kazankov, K.; Holland-Fischer, P.; Andersen, N.H.; Torp, P.; Sloth, E.; Aagaard, N.K.; Vilstrup, H. Resting Myocardial Dysfunction in Cirrhosis Quantified by Tissue Doppler Imaging. Liver Int. 2011, 31, 534–540. [Google Scholar] [CrossRef]
- Sampaio, F.; Pimenta, J.; Bettencourt, N.; Fontes-Carvalho, R.; Silva, A.P.; Valente, J.; Bettencourt, P.; Fraga, J.; Gama, V. Systolic and Diastolic Dysfunction in Cirrhosis: A Tissue-Doppler and Speckle Tracking Echocardiography Study. Liver Int. 2013, 33, 1158–1165. [Google Scholar] [CrossRef]
- Altekin, R.E.; Caglar, B.; Karakas, M.S.; Ozel, D.; Deger, N.; Demir, I. Evaluation of Subclinical Left Ventricular Systolic Dysfunction Using Two-Dimensional Speckle- Tracking Echocardiography in Patients with Non- Alcoholic Cirrhosis. Hell. J. Cardiol. 2014, 55, 402–410. [Google Scholar]
- Chen, Y.; Chan, A.C.; Chan, S.C.; Chok, S.H.; Sharr, W.; Fung, J.; Liu, J.H.; Zhen, Z.; Sin, W.C.; Lo, C.M.; et al. A Detailed Evaluation of Cardiac Function in Cirrhotic Patients and Its Alteration with or without Liver Transplantation. J. Cardiol. 2016, 67, 140–146. [Google Scholar] [CrossRef]
- Pagourelias, E.D.; Sotiriou, P.; Papadopoulos, C.E.; Cholongitas, E.; Giouleme, O.; Vassilikos, V. Left Ventricular Myocardial Mechanics in Cirrhosis: A Speckle Tracking Echocardiographic Study. Echocardiography 2016, 33, 223–232. [Google Scholar] [CrossRef] [PubMed]
- İnci, S.D.; Sade, L.E.; Altın, C.; Pirat, B.; Pamukcu, H.E.; Yılmaz, S.; Müderrisoğlu, H. Subclinical Myocardial Dysfunction in Liver Transplant Candidates Determined Using Speckle-Tracking Imaging. Turk. Kardiyoloji Dernegi Arsivi 2019, 47, 638–645. [Google Scholar] [CrossRef]
- Rimbaş, R.C.; Baldea, S.M.; Guerra, R.D.G.A.; Visoiu, S.I.; Rimbaş, M.; Pop, C.S.; Vinereanu, D. New Definition Criteria of Myocardial Dysfunction in Patients with Liver Cirrhosis: A Speckle Tracking and Tissue Doppler Imaging Study. Ultrasound Med. Biol. 2018, 44, 562–574. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Yao, Y.; Lin, S.; He, Y.; Zhu, D.; Zhong, M. Feasibility and Discriminatory Value of Tissue Motion Annular Displacement in Sepsis-Induced Cardiomyopathy: A Single-Center Retrospective Observational Study. Crit. Care 2022, 26, 220. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-H.; Wu, L.-S.; Jeng, W.-J.; Cheng, Y.-F.; Ko, Y.-S.; Sheen, I.S.; Lin, C.-Y. In HCV-Related Liver Cirrhosis, Local Pulse Wave Velocity Increases and in Decompensated Patients Correlates with Poorer Survival. PLoS ONE 2019, 14, e0212770. [Google Scholar] [CrossRef] [PubMed]
- Poojary, M.S.; Samanth, J.; Nayak, K.; Shetty, S.; Nayak, S.K.; Rao, M.S. Evaluation of Subclinical Left Ventricular Systolic Dysfunction Using Two-Dimensional Speckle-Tracking Echocardiography in Patients with Child-Pugh A and B Cirrhosis: A Case-Control Study. Indian J. Gastroenterol. 2022, 41, 567–575. [Google Scholar] [CrossRef]
- Cao, Y.; Zhang, H.; Li, S.; Li, S.; Sun, S.; Chen, J.; Ye, T.; Zhang, X.; Yuan, J. Correlation Analysis between Myocardial Work Indices and Liver Function Classification in Patients with Hepatitis B Cirrhosis: A Study with Non-Invasive Left Ventricular Pressure-Strain Loop. Front. Cardiovasc. Med. 2023, 10, 1126590. [Google Scholar] [CrossRef]
- Kim, H.M.; Kim, H.-K.; Lee, J.-H.; Lee, Y.B.; Park, E.-A.; Park, J.-B.; Lee, S.-P.; Kim, Y.J.; Kim, Y.-J.; Yoon, J.-H.; et al. Myocardial Structural and Functional Changes in Patients with Liver Cirrhosis Awaiting Liver Transplantation: A Comprehensive Cardiovascular Magnetic Resonance and Echocardiographic Study. J. Cardiovasc. Magn. Reson. 2020, 22, 25. [Google Scholar] [CrossRef] [PubMed]
- von Köckritz, F.; Braun, A.; Schmuck, R.B.; Dobrindt, E.M.; Eurich, D.; Heinzel, F.R.; Pieske, B.; Escher, F.; Zhang, K. Speckle Tracking Analysis Reveals Altered Left Atrial and Ventricular Myocardial Deformation in Patients with End-Stage Liver Disease. J. Clin. Med. 2021, 10, 897. [Google Scholar] [CrossRef] [PubMed]
- Zamirian, M.; Afsharizadeh, F.; Moaref, A.; Abtahi, F.; Amirmoezi, F.; Attar, A. Reduced Myocardial Reserve in Cirrhotic Patients: An Evaluation by Dobutamine Stress Speckle Tracking and Tissue Doppler Imaging (TDI) Echocardiography. J. Cardiovasc. Thorac. Res. 2019, 11, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Ridjab, D.A.; Ivan, I.; Budiman, F.; Tenggara, R. Evaluation of Subclinical Ventricular Systolic Dysfunction Assessed Using Global Longitudinal Strain in Liver Cirrhosis: A Systematic Review, Meta-Analysis, and Meta-Regression. PLoS ONE 2022, 17, e0269691. [Google Scholar] [CrossRef]
- Soulaidopoulos, S.; Vlachou, M.; Cholongitas, E.; Giannakoulas, G.; Panagiotidis, T.; Drakopoulou, M.; Karvounis, H.; Goulis, I. Assessment of Biventricular Function in Patients with Hepatopulmonary Syndrome. Int. J. Cardiovasc. Imaging 2021, 37, 2891–2900. [Google Scholar] [CrossRef]
- Özdemir, E.; Demirdal, T.; Emren, S.V.; Tokaç, M. Evaluation of Early Myocardial Dysfunction with Strain Echocardiography in Chronic Hepatitis B Patients. Echocardiography 2019, 36, 696–701. [Google Scholar] [CrossRef]
- Isaak, A.; Praktiknjo, M.; Jansen, C.; Faron, A.; Sprinkart, A.M.; Pieper, C.C.; Chang, J.; Fimmers, R.; Meyer, C.; Dabir, D.; et al. Myocardial Fibrosis and Inflammation in Liver Cirrhosis: MRI Study of the Liver-Heart Axis. Radiology 2020, 297, 51–61. [Google Scholar] [CrossRef]
- Said, A.; Williams, J.; Holden, J.; Remington, P.; Gangnon, R.; Musat, A.; Lucey, M. Model for End Stage Liver Disease Score Predicts Mortality across a Broad Spectrum of Liver Disease. J. Hepatol. 2004, 40, 897–903. [Google Scholar] [CrossRef]
- Kamath, P.S.; Kim, W.R. The Model for End-Stage Liver Disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’amico, G.; Dickson, E.R.; Kim, W.R. A Model to Predict Survival in Patients with End-Stage Liver Disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Anish, P.; Jayaprasad, N.; Madhavan, S.; George, R. Echocardiographic Abnormalities in Patients with Cirrhosis and Relation to Disease Severity. Heart India 2019, 7, 26. [Google Scholar] [CrossRef]
- Dimitroglou, Y.; Aggeli, C.; Alexopoulou, A.; Alexopoulos, T.; Patsourakos, D.; Polytarchou, K.; Kastellanos, S.; Angelis, A.; Vasilieva, L.; Mani, I.; et al. Correlation of Global Longitudinal Strain with Disease Severity in Liver Cirrhosis. Eur. Heart J. Cardiovasc. Imaging 2021, 22, jeaa356-155. [Google Scholar] [CrossRef]
- Skouloudi, M.; Bonou, M.S.; Adamantou, M.; Parastatidou, D.; Kapelios, C.; Masoura, K.; Efstathopoulos, E.; Aggeli, C.; Papatheodoridis, G.V.; Barbetseas, J.; et al. Left Atrial Strain and Ventricular Global Longitudinal Strain in Cirrhotic Patients Using the New Criteria of Cirrhotic Cardiomyopathy Consortium. Liver Int. 2023, 43, 2727–2742. [Google Scholar] [CrossRef] [PubMed]
- Mechelinck, M.; Hartmann, B.; Hamada, S.; Becker, M.; Andert, A.; Ulmer, T.F.; Neumann, U.P.; Wirtz, T.H.; Koch, A.; Trautwein, C.; et al. Global Longitudinal Strain at Rest as an Independent Predictor of Mortality in Liver Transplant Candidates: A Retrospective Clinical Study. J. Clin. Med. 2020, 9, 2616. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, F.; Pimenta, J.; Bettencourt, N.; Fontes-Carvalho, R.; Silva, A.P.; Valente, J.; Bettencourt, P.; Fraga, J.; Gama, V. Left Atrial Function Is Impaired in Cirrhosis: A Speckle Tracking Echocardiographic Study. Hepatol. Int. 2014, 8, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Nazar, A.; Guevara, M.; Sitges, M.; Terra, C.; Solà, E.; Guigou, C.; Arroyo, V.; Ginès, P. LEFT Ventricular Function Assessed by Echocardiography in Cirrhosis: Relationship to Systemic Hemodynamics and Renal Dysfunction. J. Hepatol. 2013, 58, 51–57. [Google Scholar] [CrossRef]
- Jansen, C.; Cox, A.; Schueler, R.; Schneider, M.; Lehmann, J.; Praktiknjo, M.; Pohlmann, A.; Chang, J.; Manekeller, S.; Nickenig, G.; et al. Increased Myocardial Contractility Identifies Patients with Decompensated Cirrhosis Requiring Liver Transplantation. Liver Transplant. 2018, 24, 15–25. [Google Scholar] [CrossRef]
- Jansen, C.; Schröder, A.; Schueler, R.; Lehmann, J.; Praktiknjo, M.; Uschner, F.E.; Schierwagen, R.; Thomas, D.; Monteiro, S.; Nickenig, G.; et al. Left Ventricular Longitudinal Contractility Predicts Acute-on-Chronic Liver Failure Development and Mortality After Transjugular Intrahepatic Portosystemic Shunt. Hepatol. Commun. 2019, 3, 340–347. [Google Scholar] [CrossRef]
- Razpotnik, M.; Bota, S.; Wimmer, P.; Hackl, M.; Lesnik, G.; Alber, H.; Peck-Radosavljevic, M. The Prevalence of Cirrhotic Cardiomyopathy According to Different Diagnostic Criteria. Liver Int. 2021, 41, 1058–1069. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Frigo, A.C.; Piano, S.; Angeli, P. Prevalence and Prognostic Value of Cirrhotic Cardiomyopathy as Defined According to the Proposed New Classification. Clin. Exp. Hepatol. 2021, 7, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Dimitroglou, Y.; Tsartsalis, D.; Vasilieva, L.; Patsourakos, D.; Kalompatsou, A.; Alexopoulou, A.; Tousoulis, D.; Tsioufis, K.; Aggeli, C. HFA-PEFF Score as an Independent Predictor of 2-Year Mortality in Liver Cirrhosis Patients. Eur. J. Gastroenterol. Hepatol. 2023, 35, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Meucci, M.C.; Hoogerduijn Strating, M.M.; Butcher, S.C.; van Rijswijk, C.S.P.; Van Hoek, B.; Delgado, V.; Bax, J.J.; Tushuizen, M.E.; Marsan, N.A. Left Atrial Dysfunction Is an Independent Predictor of Mortality in Patients with Cirrhosis Treated by Transjugular Intrahepatic Portosystemic Shunt. Hepatol. Commun. 2022, 6, 3163–3174. [Google Scholar] [CrossRef] [PubMed]
- Silvestre, O.M.; Bacal, F.; de Souza Ramos, D.; Andrade, J.L.; Furtado, M.; Pugliese, V.; Belleti, E.; Andraus, W.; Carrilho, F.J.; Carneiro D’Albuquerque, L.A.; et al. Impact of the Severity of End-Stage Liver Disease in Cardiac Structure and Function. Ann. Hepatol. 2013, 12, 85–91. [Google Scholar] [CrossRef]
- Licata, A.; Corrao, S.; Petta, S.; Genco, C.; Cardillo, M.; Calvaruso, V.; Cabibbo, G.; Massenti, F.; Cammà, C.; Licata, G.; et al. NT pro BNP Plasma Level and Atrial Volume Are Linked to the Severity of Liver Cirrhosis. PLoS ONE 2013, 8, e68364. [Google Scholar] [CrossRef]
- Cesari, M.; Frigo, A.C.; Tonon, M.; Angeli, P. Cardiovascular Predictors of Death in Patients with Cirrhosis. Hepatology 2018, 68, 215–223. [Google Scholar] [CrossRef]
- Dimitroglou, Y.; Aggeli, C.; Alexopoulou, A.; Alexopoulos, T.; Patsourakos, D.; Polytarchou, K.; Kakiouzi, V.; Tsartsalis, D.; Valatsou, A.; Kastellanos, S.; et al. Left Atrial Reservoir Strain May Be a Load Independent Index of Diastolic Dysfunction in Liver Cirrhosis Patients. Eur. Heart J. Cardiovasc. Imaging 2022, 23, jeab289-039. [Google Scholar] [CrossRef]
- Wehmeyer, M.H.; Heuer, A.J.; Benten, D.; Püschel, K.; Sydow, K.; Lohse, A.W.; Lüth, S. High Rate of Cardiac Abnormalities in a Postmortem Analysis of Patients Suffering From Liver Cirrhosis. J. Clin. Gastroenterol. 2015, 49, 866–872. [Google Scholar] [CrossRef]
- Ali, A.; Sarwar, A.; Patwardhan, V.R.; Fraiche, A.M.; Tahir, M.M.; Luo, M.; Weinstein, J.L.; Hussain, M.S.; Curry, M.P.; Ahmed, M. Echocardiographic and Other Preprocedural Predictors of Heart Failure After TIPS Placement in Patients With Cirrhosis: A Single-Center 15-Year Analysis. AJR Am. J. Roentgenol. 2022, 219, 110–118. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Y.; Meng, X.; Zhu, W.; Lu, X. Assessment of Right Ventricular Longitudinal Strain by 2D Speckle Tracking Imaging Compared with RV Function and Hemodynamics in Pulmonary Hypertension. Int. J. Cardiovasc. Imaging 2017, 33, 1737–1748. [Google Scholar] [CrossRef] [PubMed]
- Hinojar, R.; Zamorano, J.L.; González Gómez, A.; García-Martin, A.; Monteagudo, J.M.; García Lunar, I.; Sanchez Recalde, A.; Fernández-Golfín, C. Prognostic Impact of Right Ventricular Strain in Isolated Severe Tricuspid Regurgitation. J. Am. Soc. Echocardiogr. 2023, 36, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Ghio, S.; Acquaro, M.; Agostoni, P.; Ambrosio, G.; Carluccio, E.; Castiglione, V.; Colombo, D.; D’Alto, M.; Delle Grottaglie, S.; Dini, F.L.; et al. Right Heart Failure in Left Heart Disease: Imaging, Functional, and Biochemical Aspects of Right Ventricular Dysfunction. Heart Fail. Rev. 2023, 28, 1009–1022. [Google Scholar] [CrossRef] [PubMed]
- Inciardi, R.M.; Abanda, M.; Shah, A.M.; Cikes, M.; Claggett, B.; Skali, H.; Vaduganathan, M.; Prasad, N.; Litwin, S.; Merkely, B.; et al. Right Ventricular Function and Pulmonary Coupling in Patients With Heart Failure and Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2023, 82, 489–499. [Google Scholar] [CrossRef]
- Zhang, K.; Braun, A.; Von Koeckritz, F.; Schmuck, R.B.; Teegen, E.M.; Cuspidi, C.; Heinzel, F.; Pieske, B.; Tadic, M. Right Heart Remodeling in Patients with End-Stage Alcoholic Liver Cirrhosis: Speckle Tracking Point of View. J. Clin. Med. 2019, 8, 1285. [Google Scholar] [CrossRef]

{kind=link}
| 2005 Montreal Criteria | |
|---|---|
| Systolic criteria (at least one) |
|
| Diastolic criteria (at least one) |
|
| Supportive data |
|
| 2019 Cirrhotic Cardiomyopathy Consortium Criteria | |
| Systolic criteria (at least one) |
|
| Diastolic criteria (more than 50%) |
|
| Study | Published | Study Sample | Software | Main Findings | Study Limitations |
|---|---|---|---|---|---|
| Sampaio et al. [33] | 2013 | 109 patients, 18 controls | VVI | GLS lower in patients 19.99% vs. 22.02%, p = 0.003 | Only apical 4 and 2 chamber view used |
| Nazar et al. [58] | 2014 | 50 patients | EchoPAC | GLS not associated with the grade DD or prognosis | Only apical 4 and 2 chamber views used No control group |
| Altekin et al. [34] | 2014 | 38 patient, 37 controls | EchoPAC | GLS lower in patients 20.6% vs. 28.75, p < 0.001 GLS lower for MELD > 10.5 19.4% vs. 21.7%, p < 0.001 | Value for patients within normal limits, value in controls supranormal Patients with alcoholic cirrhosis excluded |
| Pagourelias et al. [36] | 2015 | 77 patients and 20 controls | EchoPAC | GLS higher in patients 20.9% vs. 19.0% p = 0.03 | Only male patients included |
| Chen et al. [35] | 2016 | 103 patients, 48 controls | EchoPAC | GLS lower in patients 18.6% vs. 20.1%, p < 0.01 GLS improvement with LT | More than 60% of patients had viral etiology |
| Jansen et al. [59] | 2018 | 168 patients | TomTec | GLS lower than reference values Higher GLS associated with worse outcome | no control group, GLS associated with earlier LT may be a confounder |
| Rimbas et al. [38] | 2018 | 46 patients, 46 controls | EchoPac | GLS non-different between patients and controls 20.9% vs. 20.7%, p > 0.05 | No patients with NASH cirrhosis included Percentage of Child-Pugh C patients low |
| Huang et al. [40] | 2019 | 80 patients, 29 controls | EchoPAC | GLS non-different between patients and controls 21.5% vs. 20.2%, p > 0.05 GLS lower in alcoholic than in HBV cirrhosis | No patients with NASH included Patients with hypotension, common in CCM excluded from the study |
| Inci et al. [37] | 2019 | 40 patients, 26 controls | VVI | GLS lower in patients 16.0% vs. 17.6%, p = 0.002 | Only 4 and 2 chamber apical views used |
| Zamirian et al. [45] | 2019 | 20 patients and 10 controls | Not stated | GLS higher in patients 22.6% vs. 19.2%, p < 0.001 Inability to improve GLS with dobutamine | Low sample size, no detailed description of the methodology |
| Jansen et al. [60] | 2019 | 114 patients | TomTEC | Lower GLS associated with worse prognosis after TIPS | Retrospective study, many echo studies excluded for low quality lack of control group |
| Kim et al. [43] | 2020 | 33 patients and 17 controls | TomTec | GLS higher in patients 24.2% vs. 18.6%, p < 0.001 | Low sample size |
| Mechelinck et al. [56] | 2020 | 117 patients | TomTec | GLS higher in patients with decompensated LC or portal hypertension | Retrospective study No control group |
| Köckritz et al. [44] | 2021 | 80 patients and 30 controls | EchoPAC | GLS higher in patients 21.4% vs. 18.7, p < 0.001 | Patients with abnormal LVEF excluded Study included only patients referred for LT |
| Cesari et al. [62] | 2021 | 83 patients and 46 controls | EchoPAC | GLS non-different between patients and controls 20% vs. 20%, p > 0.05 | Retrospective study |
| Soulaidopoulos et al. [47] | 2021 | 130 patients | EchoPAC | Patients with hepatopulmonary syndrome had lower GLS | No control group included |
| Poojary et al. [41] | 2022 | 70 patients and 60 controls | EchoPAC | GLS non-different between patients and controls 22.4% vs. 21.8% GLS higher for MELD >15.5 | Only Child Pugh A and B patients included |
| Razpotnik et al. [61] | 2022 | 122 patients | EchoPAC | GLS < 18% in 10% of patients GLS > 22% in 41% of patients | No control group |
| Meucci et al. [64] | 2022 | 129 patients | EchoPAC | 15% of patients had GLS < 18% GLS not associated with prognosis | No control group Study included only patients referred for TIPS |
| Dimitroglou et al. [63] | 2023 | 72 patients and 18 controls | QLAB | Higher GLS associated with increased disease severity | Data for control group not presented |
| Skouloudi [55] | 2023 | 135 patients | QLAB | Higher GLS associated with higher MELD score | No control group |
| Cao et al. [42] | 2023 | 90 patients and 30 controls | EchoPAC | GLS lower in patients Lower GLS associated with increased disease severity | Retrospective study Only patients with HBV cirrhosis included |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimitroglou, Y.; Aggeli, C.; Alexopoulou, A.; Tsartsalis, D.; Patsourakos, D.; Koukos, M.; Tousoulis, D.; Tsioufis, K. The Contemporary Role of Speckle Tracking Echocardiography in Cirrhotic Cardiomyopathy. Life 2024, 14, 179. https://doi.org/10.3390/life14020179
Dimitroglou Y, Aggeli C, Alexopoulou A, Tsartsalis D, Patsourakos D, Koukos M, Tousoulis D, Tsioufis K. The Contemporary Role of Speckle Tracking Echocardiography in Cirrhotic Cardiomyopathy. Life. 2024; 14(2):179. https://doi.org/10.3390/life14020179
Chicago/Turabian StyleDimitroglou, Yannis, Constantina Aggeli, Alexandra Alexopoulou, Dimitrios Tsartsalis, Dimitrios Patsourakos, Markos Koukos, Dimitris Tousoulis, and Konstantinos Tsioufis. 2024. "The Contemporary Role of Speckle Tracking Echocardiography in Cirrhotic Cardiomyopathy" Life 14, no. 2: 179. https://doi.org/10.3390/life14020179
APA StyleDimitroglou, Y., Aggeli, C., Alexopoulou, A., Tsartsalis, D., Patsourakos, D., Koukos, M., Tousoulis, D., & Tsioufis, K. (2024). The Contemporary Role of Speckle Tracking Echocardiography in Cirrhotic Cardiomyopathy. Life, 14(2), 179. https://doi.org/10.3390/life14020179