



Discrepancies in Embryonic Staging: Towards a Gold Standard

Abstract
1. Introduction
2. Background: Historical Beginnings of Embryonic Staging
3. Embryonic Age
4. Embryonic Length
5. Carnegie Stages: Academic Discrepancies and Nonuniformity
The Importance of Concise Embryonic Staging Systems
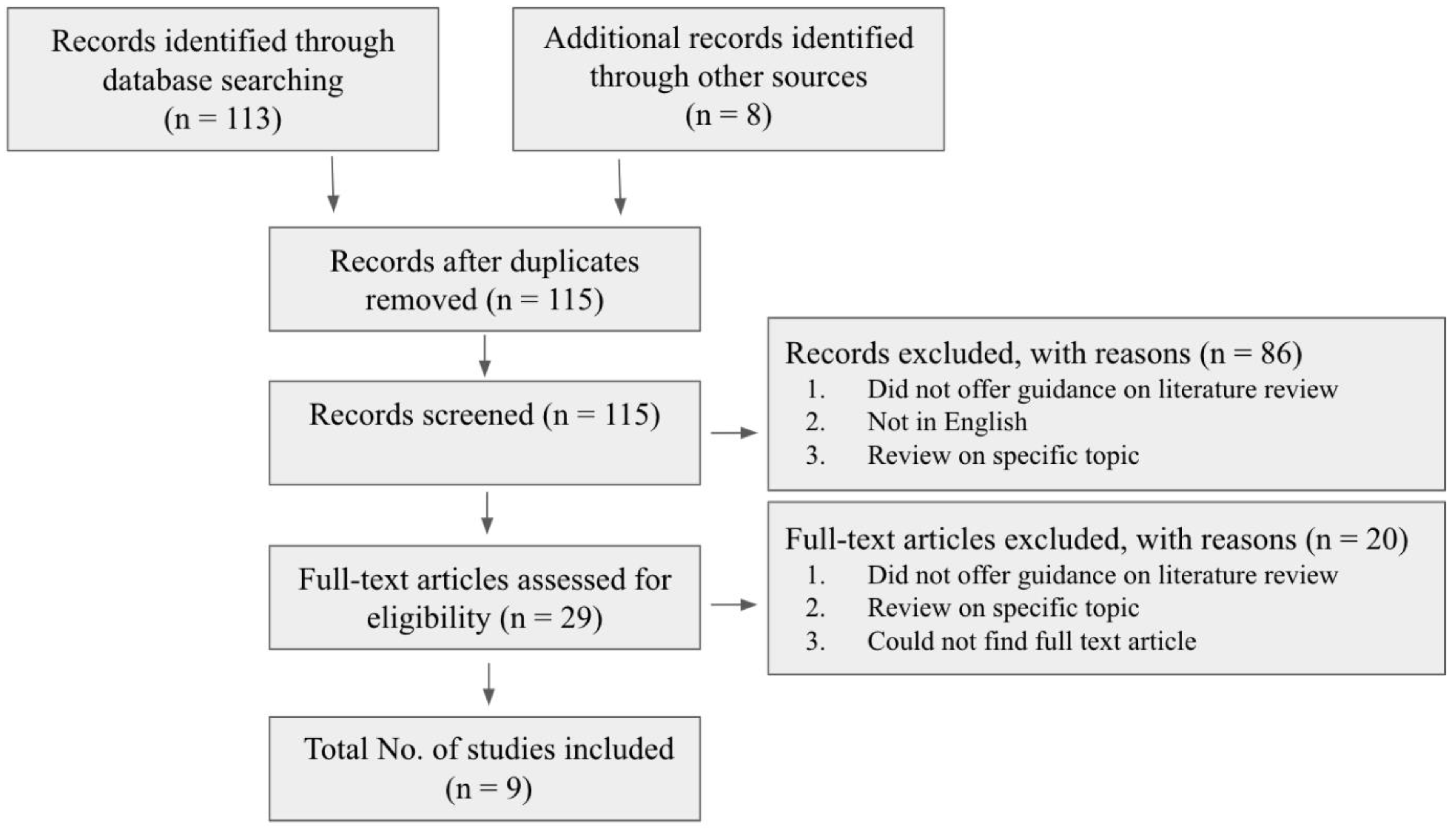
6. Methods
7. Results
8. Discussion
8.1. Staging Differences: A Matter of Sampling?

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
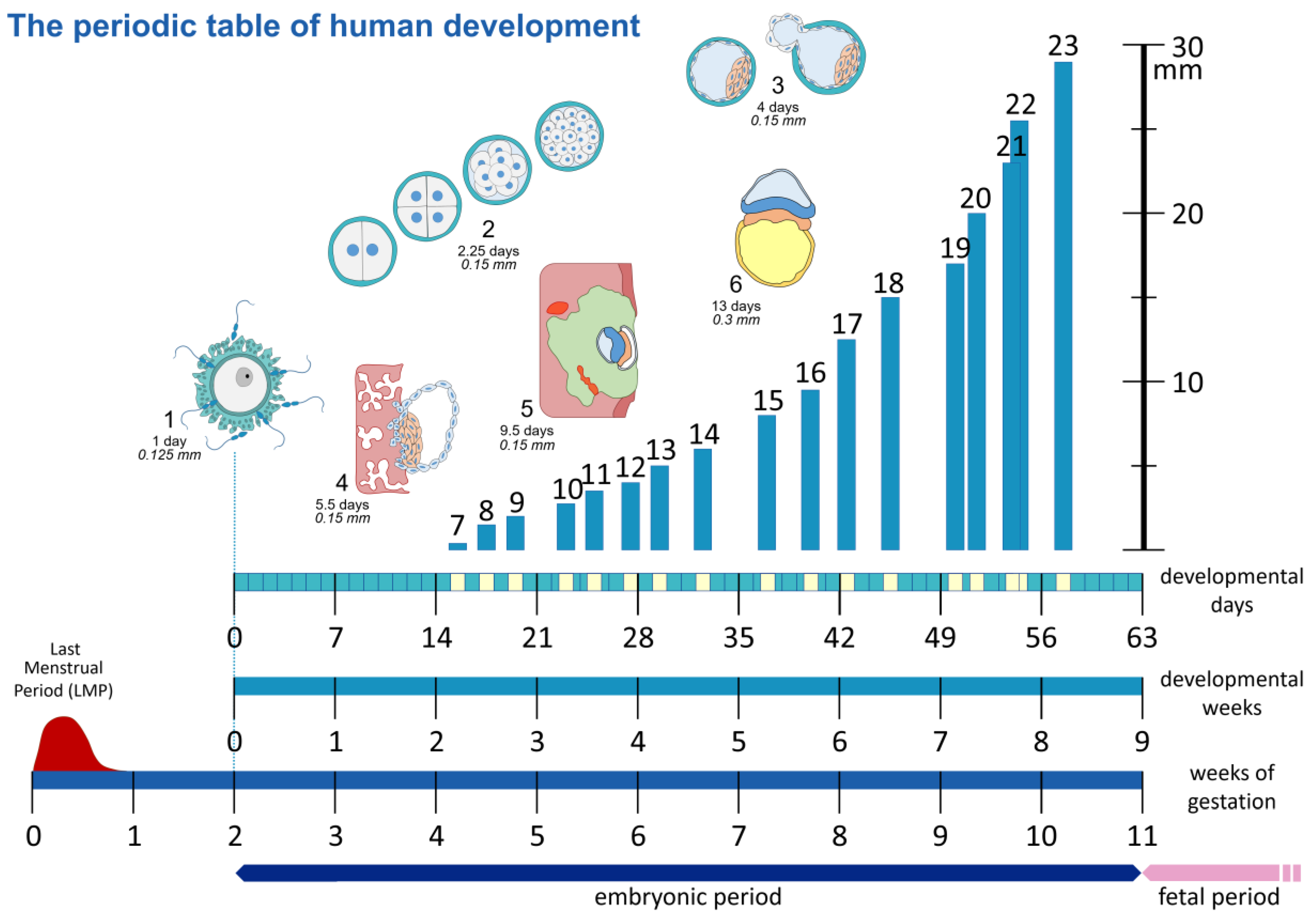
| Carnegie Stage | P.O. Days | Size (mm) | Characteristics | Carnegie Stage | P.O. Days | Size (mm) | Characteristics |
|---|---|---|---|---|---|---|---|
| 1 | 1 | 0.125 | Unicellular | 13 | 28 | 5 | Lower limb buds appear as bulges Caudal neuropore closed Lens placodes Otic vesicles Left and right lung buds discernable Septum primum and foramen primum |
| 2 | 1.5–3 | 0.15 | More than one cell presentNo blastocystic cavity present | 14 | 32 | 6 | Longer upper limbs Lower limbs clearly visible Nasal pits Optic cups |
| 3 | 4 | 0.15 | Blastocyst | 15 | 33 | 8 | Handplate Lower limbs elongate Future cerebral hemispheres distinct Foramen secundum in the heart |
| 4 | 5–6 | 0.15 | Zona pellucida dissolved Blastocyst attachment to uterine epithelium | 16 | 37 | 9.5 | Slight rotation upper limbs Footplate Pigment in the retina |
| 5 | 7–12 | 0.15 | Solid trophoblast Trophoblastic lacunae Primary umbilical vesicle Mesoblastic crests Lacunar vascular circle | 17 | 41 | 12.5 | Digital rays in hand plate Slight rotation of lower limbs Cerebral vesicles clearly visible Semilunar cusps visible in the heart Foramen primum obliterated |
| 6 | 13 | 0.2 | Chorionic villi Primitive streak Secondary umbilical vesicle Cloacal membrane | 18 | 44 | 15 | Longer and straighter trunk, toe rays Scalloping hand plate, start digits 4th ventricle larger than lateral ventr. Elbow region visible Membran. region interventr. septum Septum secundum |
| 7 | 16 | 0.4 | Cranial prolongation primitive streak (notoch. process) Primitive node Secondary villi Cloacal membrane Allantoic diverticulum | 19 | 47.5 | 18.5 | Elongation and straightening of trunk Upper limbs slightly bent in elbow Limbs extend ventrally Hands far apart, short fingers Midgut herniation |
| 8 | 18 | 1.25 | Primitive node Notochordal process Prechordal plate Primitive pit Notochordal canal | 20 | 50.5 | 22 | Longer upper limbs, bent in elbow, hands slightly flexed Toes separated 4th ventr. still larger than lateral ventr. Scalp vascular plexus visible |
| 9 | 20 | 2 | Head fold Somite pairs | 21 | 52 | 23 | Hands and feet turned inward Longer fingers Toes distinct but webbed Bending of knees, toes may touch Trunk straight and longer Stubby tail visible |
| 10 | 22 | 2.25 | Neural tube closing Looped heart tube | 22 | 54 | 26 | Eyelids visible Fingers may overlap Lower limbs rotated, touching feet Very straight trunk 4th ventricle smaller than lateral ventr. Hemispheres recognizable |
| 11 | 24 | 3.5 | Rostral neuropore closing Otic placodes Optic vesicles 1st and 2nd phar. arches Meson. duct and tubules Sinus venosus | 23 | 56.5 | 29 | Rounded head Limbs increased in length Rotation of lower limbs Forearm ascends to shoulder level Scalp vascular plexus at vertex |
| 12 | 26 | 4 | Rostral neuropore closed Caudal neuropore closing Upper limb buds 3rd pharyngeal arch Otic pits Lung bud Interventricular septum formation | Characteristics of Stages 1–8 were taken from O’Rahilly’s study (1987) [4], and the characteristics of Stages 9–23 were acquired through a combination of sources, including the HDBR atlas, O’Rahilly (1987), Hill (2007), and Pietersma (2023) [4,5,22,29]. P.O days and embryonic size data utilized within the table were taken from O’Rahilly’s study (1987) [4]. | |||
8.2. Technological Advances: A Cause for Discrepancies?
8.3. Staging Differences: A Matter of Data Collection?
8.4. Embryonic Diapause: A Novel Theory
8.5. Limitations
8.6. Future Perspectives
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Britannica, T. Editors of Encyclopaedia (17 February 2019). Embryology. Encyclopedia Britannica. Available online: https://www.britannica.com/science/embryology (accessed on 12 December 2022).
- Wilens, S.R.G. Harrison Organization and Development of the Embryo Yale Univ. Press, Yale University. Science 1969, 168, 724–725. [Google Scholar] [CrossRef]
- Oppenheimer, J. Developmental Stages in Human Embryos. Including a Revision of Streeter’s “Horizons” and a Survey of the Carnegie Collection. Ronan O’Rahilly, Fabiola Muller. Q. Rev. Biol. 1991, 66, 79. [Google Scholar] [CrossRef]
- O’Rahilly, R.; Muller, F.; Streeter, G.L. Developmental Stages in Human Embryos: Including a Revision of Streeter’s “Horizons” and a Survey of the Carnegie Collection; Carnegie Institution of Washington: Washington, DC, USA, 1987. [Google Scholar]
- Hill, M.A. Early Human Development. Clin. Obstet. Gynecol. 2007, 50, 2–9. [Google Scholar] [CrossRef] [PubMed]
- De Bakker, B.S.; de Jong, K.H.; Hagoort, J.; de Bree, K.; Besselink, C.T.; de Kanter, F.E.C.; Veldhuis, T.; Bais, B.; Schildmeijer, R.; Ruijter, J.M.; et al. An interactive three-dimensional digital atlas and quantitative database of human development. Science 2010, 354, aag0053. [Google Scholar] [CrossRef] [PubMed]
- Hill, M. Two Web Resources Linking Major Human Embryology Collections Worldwide. Cells Tissues Organs 2018, 205, 293–302. [Google Scholar] [CrossRef]
- Sabin, F.R. Franklin Paine Mall. 1862–1917. Anat. Record. 1918, 14, 1–17. [Google Scholar] [CrossRef]
- Streeter, G.L. Developmental Horizons in Human Embryos. Age Groups XI to XXIII; Carnegie Institution of Washington: Washington, DC, USA, 1951. [Google Scholar]
- De Bakker, B.S. 3D Atlas of Human Embryology: New Insights in Human Development. 2018. Available online: https://dare.uva.nl/search?identifier=cfb70f9b-ebc4-4dda-b1cf-421e78cbd612 (accessed on 12 December 2022).
- De Beer, G. Embryos and Ancestors by Sir Gavin De Beer (3 December 1958); Clarendon Press: Oxford, UK, 1958. [Google Scholar]
- O’Rahilly, R.; Muller, F. Prenatal ages and stages? Measures and errors. Teratology 2000, 61, 382–384. [Google Scholar] [CrossRef]
- Tanner, J.M. A History of the Study of Human Growth; Cambridge University Press: Cambridge, UK, 1981. [Google Scholar]
- O’Rahilly, R. Early human development and the chief sources of information on staged human embryos. Eur. J. J. Obstet. Gynecol. Reprod. Biol. 1979, 9, 273–280. [Google Scholar] [CrossRef]
- Pexsters, A.; Daemen, A.; Bottomley, C.; Van Schoubroeck, D.; De Catte, L.; De Moor, B.; D’Hooghe, T.; Lees, C.; Timmerman, D.; Bourne, T. New crown-rump length curve based on over 3500 pregnancies. Ultrasound Obs. Obstet. Gynecol. 2010, 35, 650–655. [Google Scholar] [CrossRef]
- Nishimura, H.; Takano, K.; Tanimura, T.; Yasuda, M. Normal and abnormal development of human embryos: First report of the analysis of 1,213 intact embryos. Teratology 1968, 1, 281–290. [Google Scholar] [CrossRef]
- Jirásek, J.E. Development of the Genital System and Male Pseudohermaphroditism; Johns Hopkins Press: Baltimore, MD, USA; London, UK, 1972; Volume 136. [Google Scholar]
- Hill, M.A. Developing the Digital Kyoto Collection in Education and Research. Anat. Rec. 2018, 301, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Hill, M.; Takakuwa, T. Human Embryology. In New Discoveries in Embryology; IntechOpen: London, UK, 2015. [Google Scholar] [CrossRef]
- Nishimura, H.; Tanimura, T.; Semba, R.; Uwabe, C. Normal development of early human embryos: Observation of 90 specimens at Carnegie stages 7 to 13. Teratology 1974, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Harkness, L. Morphological and molecular characteristics of living human fetuses between Carnegie stages 7 and 23: Developmental stages in the post-implantation embryo. Hum. Human. Reprod. Updat. 1997, 3, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Human Developmental Biology Resource. HDBR Atlas Carnegie Staging Criteria. HDBR Atlas. 2010. Available online: https://hdbratlas.org/staging-criteria/carnegie-staging.html (accessed on 12 December 2022).
- Heirloom Collection. Heirloom Collection. 2006. [Google Scholar]
- O’Rahilly, R.; Müller, F. Developmental Stages in Human Embryos: Revised and New Measurements. Cells Tissues Organs 2010, 192, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Linskens, I.H.; Pajkrt, E. Protocol Datering Van de Zwangerschap, Nederlandse Vereniging Voor Obstetrie en Gynaecologie. 29 August 2018. Available online: https://www.nvog.nl/wp-content/uploads/2018/09/Datering-van-de-zwangerschap-2.0-update-aug-2018.pdf (accessed on 24 October 2022).
- Salomon, L.; Alfirevic, Z.; Bilardo, C.M.; Chalouhi, G.E.; Ghi, T.; Kagan, K.O.; Lau, T.S.; Papageorghiou, A.T.; Raine-Fenning, N.; Stirnemann, J.; et al. ISUOG Practice Guidelines: Performance of first-trimester fetal ultrasound scan. Ultrasound Obs. Obstet. Gynecol. 2013, 41, 102–113. [Google Scholar] [CrossRef]
- Rousian, M.; Koning, A.H.; van Oppenraaij, R.H.; Hop, W.C.; Verwoerd-Dikkeboom, C.M.; van der Spek, P.J.; Exalto, N.; Steegers, E.A. An innovative virtual reality technique for automated human embryonic volume measurements. Hum. Reprod. 2010, 25, 2210–2216. [Google Scholar] [CrossRef]
- Digital Embryology Consortium. Available online: https://human-embryology.org (accessed on 18 August 2022).
- Pietersma, C.S.; Mulders, A.G.M.G.J.; Willemsen, S.P.; Graafland, N.; Altena, A.C.; Koning, A.H.J.; Rousian, M.; Steegers-Theunissen, R.P.M.; Steegers, E.A.P.; de Bakker, B.S. Embryonic morphological development is delayed in pregnancies ending in a spontaneous miscarriage. Hum. Reprod. 2023. accepted for publication. [Google Scholar] [CrossRef]
- Dawood, Y.; Buijtendijk, M.F.J.; Shah, H.; Smit, J.A.; Jacobs, K.; Hagoort, J.; Oostra, R.J.; Bourne, T.; van den Hoff, M.J.B.; de Bakker, B.S. Imaging fetal anatomy. Semin. Cell. Dev. Biol. 2022, 131, 78–92. [Google Scholar] [CrossRef]
- Rousian, M.; Groenenberg, I.A.L.; Hop, W.C.; Koning, A.H.J.; van der Spek, P.J.; Exalto, N.; Steegers, E.A.P. Human Embryonic Growth and Development of the Cerebellum Using 3-Dimensional Ultrasound and Virtual Reality. Reprod. Sci. 2013, 20, 899–908. [Google Scholar] [CrossRef]
- Rousian, M.; Verwoerd-Dikkeboom, C.M.; Koning, A.H.; Hop, W.C.; van der Spek, P.J.; Steegers, E.A.; Exalto, N. First trimester umbilical cord and vitelline duct measurements using virtual reality. Early Hum. Human. Dev. 2011, 87, 77–82. [Google Scholar] [CrossRef]
- Baken, L.; Rousian, M.; Koning, A.H.; Bonsel, G.J.; Steegers, E.; Exalto, N. First trimester detection of structural abnormalities; a comparison of 2D/3D ultrasound and virtual embryoscopy. Ultrasound Obs. Obstet. Gyneco. 2012, 40, 180–181. [Google Scholar] [CrossRef]





| Carnegie | Mean Days | |||||
|---|---|---|---|---|---|---|
| stage | Heirloom collection (2006) [23] | O’Rahilly (1987) [4] | O’Rahilly (2010) [24] | Hill image (2018) [18] | Hill (2007) [5] | Harkness (1997) [21] |
| 1 | 1 | 1 | 1 | 1 | - | - |
| 2 | 2.5 | 2.25 | 2.5 | 3 | - | - |
| 3 | 4.5 | 4 | 4.5 | 4 | - | - |
| 4 | 6 | 5.5 | 6 | - | - | - |
| 5 | 9.5 | 9.5 | 9.5 | - | - | - |
| 6 | 17 | 13 | 17 | - | - | - |
| 7 | 19 | 16 | 19.5 | 16 | 16 | - |
| 8 | 23 | 18 | 23 | 18 | 18 | 25.5 |
| 9 | 25 | 20 | 26 | 20 | 20 | 31 |
| 10 | 28 | 22 | 29 | 22 | 22.5 | 31.2 |
| 11 | 29 | 24 | 29 | 24.5 | 24.5 | 30 |
| 12 | 30 | 26 | 30 | 28 | 28 | 35.5 |
| 13 | 32 | 28 | 31.5 | 30 | 30 | 36.2 |
| 14 | 33 | 32 | 34 | 33 | 33 | 37.9 |
| 15 | 36 | 33 | 36 | 36.5 | 36.5 | 38.2 |
| 16 | 39 | 37 | 38.5 | 39.5 | 39.5 | 40.3 |
| 17 | 41 | 41 | 40.5 | 43 | 43 | 40.8 |
| 18 | 44 | 44 | 43.5 | 46 | 46 | 41.9 |
| 19 | 46 | 47.5 | 46 | 49.5 | 49.5 | 44.3 |
| 20 | 49 | 50.5 | 48.5 | 52 | 52 | 43.9 |
| 21 | 51 | 52 | 50.5 | 53.5 | 53.5 | 45 |
| 22 | 53 | 54 | 53.5 | 56 | 55 | 50 |
| 23 | 56 | 56.5 | 55.5 | 58 | 58 | 49.9 |
| Carnegie | Mean Length (mm) | ||||
|---|---|---|---|---|---|
| Stage | Heirloom collection (2006) [23] | O’Rahilly (1987) [4] | O’Rahilly (2010) [24] | Hill (2007) [5] | Harkness (1997) [21] |
| 1 | 0.125 | 0.125 | 0.125 | - | - |
| 2 | 0.15 | 0.15 | 0.15 | - | - |
| 3 | 0.15 | 0.15 | 0.15 | - | - |
| 4 | 0.15 | 0.15 | 0.15 | - | - |
| 5 | 0.15 | 0.15 | 0.15 | - | - |
| 6 | 0.2 | 0.2 | 0.3 | - | - |
| 7 | 0.4 | 0.4 | 0.6 | 0.4 | - |
| 8 | 1.25 | 1.25 | 1.1 | 1.5 | 2.5 |
| 9 | 2 | 2 | 1.4 | 2 | 2.5 |
| 10 | 2.75 | 2.25 | 2.1 | 2.75 | 2.9 |
| 11 | 3.5 | 3.5 | 3.2 | 3.5 | 3.2 |
| 12 | 4 | 4 | 3.9 | 4 | 4.2 |
| 13 | 5 | 5 | 4.9 | 5 | 5.6 |
| 14 | 6 | 6 | 6.5 | 6 | 7.2 |
| 15 | 8 | 8 | 7.8 | 8 | 8.7 |
| 16 | 9.5 | 9.5 | 9.6 | 9.5 | 10 |
| 17 | 12.5 | 12.5 | 12.2 | 12.5 | 12.2 |
| 18 | 15 | 15 | 14.9 | 15 | 14.8 |
| 19 | 17 | 18.5 | 18.2 | 17 | 16.9 |
| 20 | 20 | 22 | 20.7 | 20 | 18.1 |
| 21 | 23 | 23 | 22.9 | 23 | 22.3 |
| 22 | 25.5 | 26 | 25.5 | 25.5 | 22.8 |
| 23 | 29 | 29 | 28.8 | 29 | 23.7 |
| Collection | Place | Number | Characteristics | Establishment |
|---|---|---|---|---|
| Carnegie | Washington, DC, USA | ~10,000 | Human histology and fixed specimens | 1887 |
| Madrid | Madrid, Spain | ~120 | Human histology | 1935 |
| Blechschmidt | Göttingen, Germany | 100 | Human histology | 1950s |
| Kyoto | Kyoto, Japan | ~44,000 | Human histology and fixed specimens | 1961 |
| Author | Publication Year | Title |
|---|---|---|
| Harkness, L. | 1997 | “Morphological and molecular characteristics of living human fetuses between Carnegie stages 7 and 23: developmental stages in the post-implantation embryo.” |
| HDBR Atlas | 2010 | Human Developmental Biology Resource. |
| Heirloom Collection | 2006 | Human embryo imaging and reconstruction, Library of Online media collection. |
| Hill, M. A. | 2007 | Early Human Development. |
| Hill, M. A. | 2018 | “Developing the Digital Kyoto Collection in Education and Research” |
| Jirásek, J. E. | 1972 | Development of the genital system and male pseudohermaphroditism. |
| Nishimura, H.; Takano, K.; Tanimura, T.; and Yasuda, M. | 1968 | “Normal and abnormal development of human embryos: First report of the analysis of 1213 intact embryos.” |
| O’Rahilly, R.; Muller, F.; and Streeter, G. L. | 1987 | “Developmental stages in human embryos: Including a revision of Streeter’s “Horizons” and a survey of the Carnegie collection.” |
| O’Rahilly, R.; and Müller, F. | 2010 | “Developmental Stages in Human Embryos: Revised and New Measurements.” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flierman, S.; Tijsterman, M.; Rousian, M.; de Bakker, B.S. Discrepancies in Embryonic Staging: Towards a Gold Standard. Life 2023, 13, 1084. https://doi.org/10.3390/life13051084
Flierman S, Tijsterman M, Rousian M, de Bakker BS. Discrepancies in Embryonic Staging: Towards a Gold Standard. Life. 2023; 13(5):1084. https://doi.org/10.3390/life13051084
Chicago/Turabian StyleFlierman, Sander, Melanie Tijsterman, Melek Rousian, and Bernadette S. de Bakker. 2023. "Discrepancies in Embryonic Staging: Towards a Gold Standard" Life 13, no. 5: 1084. https://doi.org/10.3390/life13051084
APA StyleFlierman, S., Tijsterman, M., Rousian, M., & de Bakker, B. S. (2023). Discrepancies in Embryonic Staging: Towards a Gold Standard. Life, 13(5), 1084. https://doi.org/10.3390/life13051084