
Evaluation of Whole Brain Radiotherapy among Lung Cancer Patients with Brain Metastases in Relation to Health Care Level and Survival

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Patient Characteristics
2.2. Outcome Information
2.3. Statistical Analyses
3. Results
3.1. Clinical Characteristics of the Cohort
3.2. Brain Metastases and WBRT
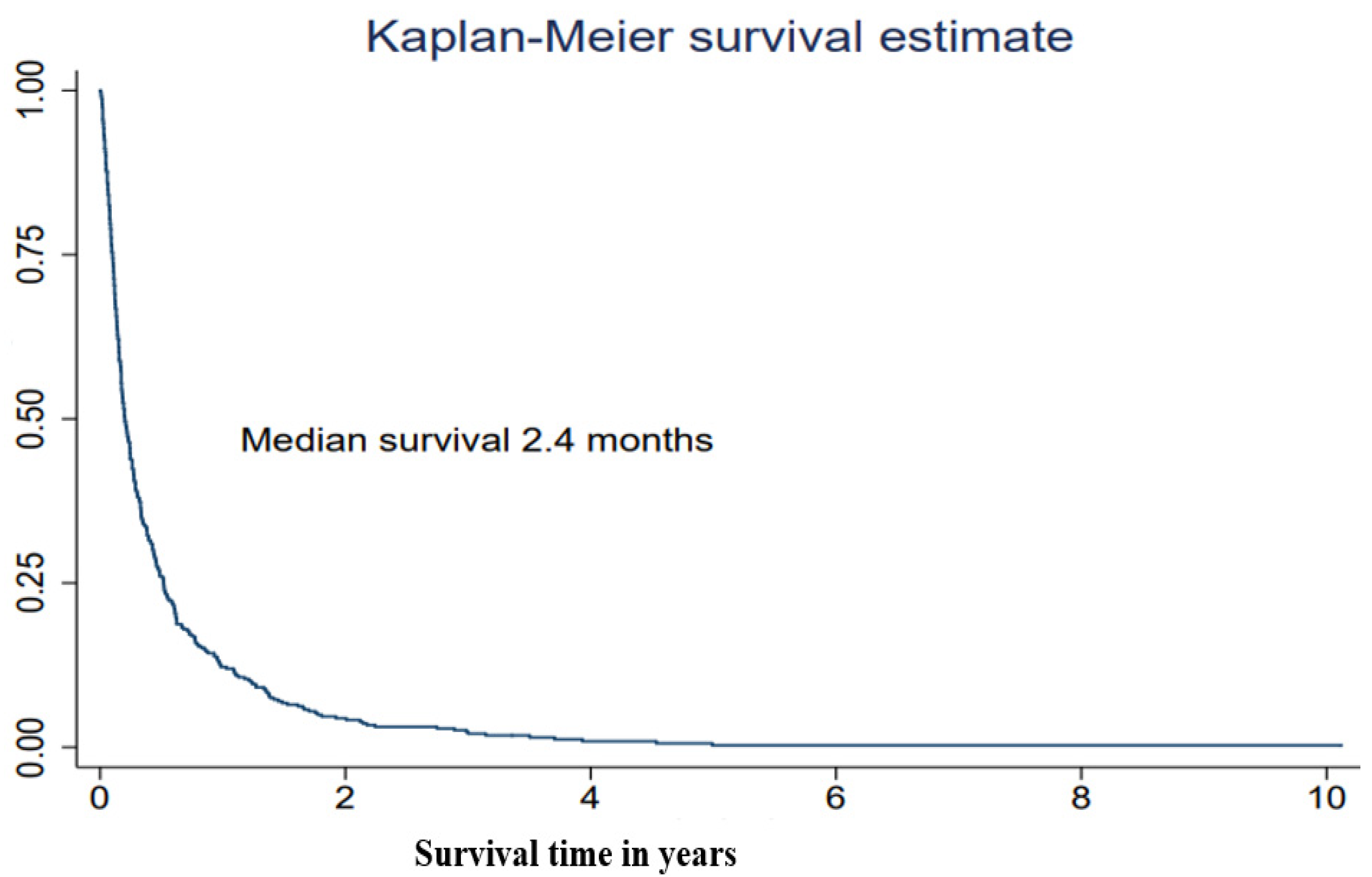
3.3. Overall Survival
3.4. Health Care Level after Treatment with WBRT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamba, N.; Wen, P.Y.; Aizer, A.A. Epidemiology of brain metastases and leptomeningeal disease. Neuro Oncol. 2021, 23, 1447–1456. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, M.; Bahrami, T.; Salmaninejad, A.; Nosrati, R.; Ghaffari, P.; Ghaffari, S.H. Lung cancer-associated brain metastasis: Molecular mechanisms and therapeutic options. Cell Oncol. 2017, 40, 419–441. [Google Scholar] [CrossRef] [PubMed]
- Gavrilovic, I.T.; Posner, J.B. Brain metastases: Epidemiology and pathophysiology. J. Neurooncol. 2005, 75, 5–14. [Google Scholar] [CrossRef]
- Steindl, A.; Berghoff, A.S. Brain metastases in metastatic cancer: A review of recent advances in systemic therapies. Expert Rev. Anticancer Ther. 2021, 21, 325–339. [Google Scholar] [CrossRef] [PubMed]
- Rodin, D.; Banihashemi, B.; Wang, L.; Lau, A.; Harris, S.; Levin, W.; Dinniwell, R.; Millar, B.A.; Chung, C.; Laperriere, N.; et al. The Brain Metastases Symptom Checklist as a novel tool for symptom measurement in patients with brain metastases undergoing whole-brain radiotherapy. Curr. Oncol. 2016, 23, e239–e247. [Google Scholar] [CrossRef] [Green Version]
- Le Rhun, E.; Guckenberger, M.; Smits, M.; Dummer, R.; Bachelot, T.; Sahm, F.; Galldiks, N.; de Azambuja, E.; Berghoff, A.S.; Metellus, P.; et al. EANO-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours. Ann. Oncol. 2021, 32, 1332–1347. [Google Scholar] [CrossRef]
- Suh, J.H.; Kotecha, R.; Chao, S.T.; Ahluwalia, M.S.; Sahgal, A.; Chang, E.L. Current approaches to the management of brain metastases. Nat. Rev. Clin. Oncol. 2020, 17, 279–299. [Google Scholar] [CrossRef]
- Osmani, L.; Askin, F.; Gabrielson, E.; Li, Q.K. Current WHO guidelines and the critical role of immunohistochemical markers in the subclassification of non-small cell lung carcinoma (NSCLC): Moving from targeted therapy to immunotherapy. Semin. Cancer Biol. 2018, 52, 103–109. [Google Scholar] [CrossRef]
- Arbour, K.C.; Riely, G.J. Systemic Therapy for Locally Advanced and Metastatic Non-Small Cell Lung Cancer: A Review. JAMA 2019, 322, 764–774. [Google Scholar] [CrossRef]
- Page, S.; Milner-Watts, C.; Perna, M.; Janzic, U.; Vidal, N.; Kaudeer, N.; Ahmed, M.; McDonald, F.; Locke, I.; Minchom, A.; et al. Systemic treatment of brain metastases in non-small cell lung cancer. Eur. J. Cancer 2020, 132, 187–198. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Mesko, S.; Li, J.; Cagney, D.; Aizer, A.; Lin, N.U.; Nesbit, E.; Kruser, T.J.; Chan, J.; Braunstein, S.; et al. Survival in Patients With Brain Metastases: Summary Report on the Updated Diagnosis-Specific Graded Prognostic Assessment and Definition of the Eligibility Quotient. J. Clin. Oncol. 2020, 38, 3773–3784. [Google Scholar] [CrossRef] [PubMed]
- Sperduto, P.W.; Kased, N.; Roberge, D.; Xu, Z.; Shanley, R.; Luo, X.; Sneed, P.K.; Chao, S.T.; Weil, R.J.; Suh, J.; et al. Summary report on the graded prognostic assessment: An accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J. Clin. Oncol. 2012, 30, 419–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperduto, P.W.; Yang, T.J.; Beal, K.; Pan, H.; Brown, P.D.; Bangdiwala, A.; Shanley, R.; Yeh, N.; Gaspar, L.E.; Braunstein, S.; et al. Estimating Survival in Patients With Lung Cancer and Brain Metastases: An Update of the Graded Prognostic Assessment for Lung Cancer Using Molecular Markers (Lung-molGPA). JAMA Oncol. 2017, 3, 827–831. [Google Scholar] [CrossRef] [PubMed]
- Suh, J.H. Association of Molecular Marker Status With Graded Prognostic Assessment of Lung Cancer With Brain Metastases. JAMA Oncol. 2017, 3, 831–832. [Google Scholar] [CrossRef]
- Gaspar, L.; Scott, C.; Rotman, M.; Asbell, S.; Phillips, T.; Wasserman, T.; McKenna, W.G.; Byhardt, R. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 745–751. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1960 patients in the RTOG database. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 510–514. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Yang, T.J.; Beal, K.; Pan, H.; Brown, P.D.; Bangdiwala, A.; Shanley, R.; Yeh, N.; Gaspar, L.E.; Braunstein, S.; et al. The Effect of Gene Alterations and Tyrosine Kinase Inhibition on Survival and Cause of Death in Patients With Adenocarcinoma of the Lung and Brain Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 406–413. [Google Scholar] [CrossRef] [Green Version]
- Nieder, C.; Norum, J.; Dalhaug, A.; Aandahl, G.; Pawinski, A. Radiotherapy versus best supportive care in patients with brain metastases and adverse prognostic factors. Clin. Exp. Metastasis 2013, 30, 723–729. [Google Scholar] [CrossRef]
- Ernani, V.; Stinchcombe, T.E. Management of Brain Metastases in Non-Small-Cell Lung Cancer. J. Oncol. Pract. 2019, 15, 563–570. [Google Scholar] [CrossRef]
- Mulvenna, P.; Nankivell, M.; Barton, R.; Faivre-Finn, C.; Wilson, P.; McColl, E.; Moore, B.; Brisbane, I.; Ardron, D.; Holt, T.; et al. Dexamethasone and supportive care with or without whole brain radiotherapy in treating patients with non-small cell lung cancer with brain metastases unsuitable for resection or stereotactic radiotherapy (QUARTZ): Results from a phase 3, non-inferiority, randomised trial. Lancet 2016, 388, 2004–2014. [Google Scholar] [CrossRef] [Green Version]
- Tsakonas, G.; Hellman, F.; Gubanski, M.; Friesland, S.; Tendler, S.; Lewensohn, R.; Ekman, S.; de Petris, L. Prognostic factors affecting survival after whole brain radiotherapy in patients with brain metastasized lung cancer. Acta Oncol. 2018, 57, 231–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsao, M.N.; Rades, D.; Wirth, A.; Lo, S.S.; Danielson, B.L.; Gaspar, L.E.; Sperduto, P.W.; Vogelbaum, M.A.; Radawski, J.D.; Wang, J.Z.; et al. Radiotherapeutic and surgical management for newly diagnosed brain metastasis(es): An American Society for Radiation Oncology evidence-based guideline. Pract. Radiat. Oncol. 2012, 2, 210–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glatzer, M.; Faivre-Finn, C.; De Ruysscher, D.; Widder, J.; Van Houtte, P.; Troost, E.G.C.; Slotman, B.J.; Ramella, S.; Pottgen, C.; Peeters, S.T.H.; et al. Role of radiotherapy in the management of brain metastases of NSCLC—Decision criteria in clinical routine. Radiother. Oncol. 2021, 154, 269–273. [Google Scholar] [CrossRef]
- Kraft, J.; Mayinger, M.; Willmann, J.; Brown, M.; Tanadini-Lang, S.; Wilke, L.; Guckenberger, M.; Andratschke, N. Management of multiple brain metastases: A patterns of care survey within the German Society for Radiation Oncology. J. Neurooncol. 2021, 152, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Vårdprogram Lungcancer 2021. Available online: Nationellt vårdprogram lungcancer (cancercentrum.se) (accessed on 1 February 2022).
- Nilsson, J.; Blomberg, C.; Holgersson, G.; Carlsson, T.; Bergqvist, M.; Bergstrom, S. End-of-life care: Where do cancer patients want to die? A systematic review. Asia Pac. J. Clin. Oncol. 2017, 13, 356–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radbruch, L.; De Lima, L.; Knaul, F.; Wenk, R.; Ali, Z.; Bhatnaghar, S.; Blanchard, C.; Bruera, E.; Buitrago, R.; Burla, C.; et al. Redefining Palliative Care-A New Consensus-Based Definition. J. Pain Symptom. Manag. 2020, 60, 754–764. [Google Scholar] [CrossRef]
- Statistiska Centralbyrån (SCB). Available online: https://www.scb.se/ (accessed on 21 January 2022).
- Ramstrom, L.; Borland, R.; Wikmans, T. Patterns of Smoking and Snus Use in Sweden: Implications for Public Health. Int. J. Environ. Res. Public Health 2016, 13, 1110. [Google Scholar] [CrossRef]
- Cancerfonden-Statistik. Available online: https://www.cancerfonden.se/om-cancer/statistik?gclid=EAIaIQobChMIi4vfuN7C9QIVGRkGAB0yIQcEEAAYASAAEgKCwvD_BwE (accessed on 21 January 2022).
- Statistikdatabas för Cancer. Available online: https://sdb.socialstyrelsen.se/if_can/resultat.aspx (accessed on 28 January 2022).
- VISS. Available online: https://viss.nu/ (accessed on 21 January 2022).
- Eden, M.; Harrison, S.; Griffin, M.; Lambe, M.; Pettersson, D.; Gavin, A.; Brewster, D.H.; Lin, Y.; Johannesen, T.B.; Milne, R.L.; et al. Impact of variation in cancer registration practice on observed international cancer survival differences between International Cancer Benchmarking Partnership (ICBP) jurisdictions. Cancer Epidemiol. 2019, 58, 184–192. [Google Scholar] [CrossRef] [Green Version]
- Strang, P.; Furst, P.; Hedman, C.; Bergqvist, J.; Adlitzer, H.; Schultz, T. Chronic obstructive pulmonary disease and lung cancer: Access to palliative care, emergency room visits and hospital deaths. BMC Pulm. Med. 2021, 21, 170. [Google Scholar] [CrossRef]
- Young, J.; Badgery-Parker, T.; Dobbins, T.; Jorgensen, M.; Gibbs, P.; Faragher, I.; Jones, I.; Currow, D. Comparison of ECOG/WHO performance status and ASA score as a measure of functional status. J. Pain Symptom. Manag. 2015, 49, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, A.T.; Hjermstad, M.J.; Omdahl, T.; Aass, N.; Skovlund, E.; Hellebust, T.P.; Johansen, S.; Kaasa, S.; Yri, O.E. Overall survival after initial radiotherapy for brain metastases; a population based study of 2140 patients with non-small cell lung cancer. Acta Oncol. 2021, 60, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Ullgren, H.; Fransson, P.; Olofsson, A.; Segersvard, R.; Sharp, L. Health care utilization at end of life among patients with lung or pancreatic cancer. Comparison between two Swedish cohorts. PLoS ONE 2021, 16, e0254673. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, L.E.; Troost, E.G.; Steward, A.; Bootsma, G.P.; De Jaeger, K.; van den Borne, B.E.; Dingemans, A.M. Patient selection for whole brain radiotherapy (WBRT) in a large lung cancer cohort: Impact of a new Dutch guideline on brain metastases. Acta Oncol. 2014, 53, 945–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasch-Westin, M.; Helde-Frankling, M.; Bjorkhem-Bergman, L. Death at home: Predictive factors in a medical home care unit. BMJ Support. Palliat. Care 2019. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variable | N (%) |
|---|---|
| Gender | |
| Women | 211 (54.8) |
| Men | 173 (45.1)) |
| Marital status | |
| Cohabitation, no children at home | 204 (53.3) |
| Cohabitation with children at home | 15 (3.9) |
| Alone with children at home | 3 (0.26) |
| Alone | 161 (42.0) |
| Missing | 1 |
| Stage M (Stage IV) | |
| M0 | 88 (22.9) |
| M1 | 291 (75.8) |
| Histology | |
| SCLC | 63 (16.4) |
| Adenocarcinoma | 265 (69.0) |
| Squamous cell | 26 (6.8) |
| Large cell | 11 (2.9) |
| NOS/Mixed | 4 (1.0) |
| Sarcoma | 1 (0.3) |
| Unclassified | 9 (2.3) |
| Missing | 5 (1.3) |
| EGFR status | |
| Positive | 35 (9.1) |
| Negative | 135 (35.2) |
| Missing | 214 (55.7) |
| ALK status | |
| Positive | 12 (3.1) |
| Negative | 78 (20.3) |
| Missing | 294 (76.6) |
| KRAS status | |
| Positive | 18 (4.7) |
| Negative | 35 (9.1) |
| Missing | 331 (86.2) |
| Adjuvant treatment (radio, chemo, or both) | |
| Yes | 56 (14.6) |
| No | 328 (85.4) |
| Brain metastases at time of diagnosis | |
| Yes | 177 (46.1) |
| No | 207 (53.9) |
| Palliative medical oncological treatment | |
| Yes | 264 (68.8) |
| No | 120 (31.3) |
| No of palliative medical oncological treatments (min-max) | 0–6 |
| No of palliative medical oncological treatments | |
| 0–2 | 329 (85.7) |
| 3–6 | 55 (16.7) |
| Treatment of brain metastases in the medical history before WBRT | |
| Surgery | 14 (3.7) |
| SRT | 38 (9.9) |
| Systemic treatment | 9 (2.3) |
| Surgery + SRT | 9 (2.3) |
| None | 311 (81.0) |
| Year of WBRT treatment | |
| 2008–2010 | 96 (25.0) |
| 2011–2013 | 175 (45.6) |
| 2014–2016 | 88 (22.9) |
| 2017–2019 | 25 (6.5) |
| Age at time of WBRT treatment (range 36–91) | |
| -49 | 19 (4.9) |
| 50–69 | 223 (58.1) |
| 70- | 142(40.0) |
| Dose of WBRT | |
| 4 Gy x 5 | 356 (92.7) |
| 3 Gy x 10 | 22 (5.7) |
| Other | 6 (1.6) |
| Performance status at the start of WBRT (WHO) | |
| 0 | 82 (21.4) |
| 1 | 157 (40.9) |
| 2 | 101 (26.3) |
| 3 | 39 (10.2) |
| 4 | 5 (1.3) |
| Finished WBRT treatment | |
| Yes | 365 (95.0) |
| No | 19 (4.9) |
| Health care level one week before WBRT | |
| Home | 276 (71.9) |
| Hospital | 70 (18.2) |
| Palliative ward | 37 (9.6) |
| Nursing home | 1 (0.3) |
| Health care level during WBRT | |
| Home | 272 (70.8) |
| Hospital | 64 (16.7) |
| Palliative ward | 46 (12.0) |
| Nursing home | 1 (0.3) |
| Health care level one week after WBRT | |
| Home | 275 (70.3) |
| Hospital | 25 (6.5) |
| Palliative ward | 80 (20.8) |
| Nursing home | 2 (0.5) |
| Ever home after WBRT treatment | |
| Yes | 298 (77.6) |
| No | 84 (21.9) |
| Characteristics | Median Survival Months (Range) | Adjusted HR 1 (95% CI) | Adjusted HR 2 (95% CI) |
|---|---|---|---|
| Gender Women Men At the time of treatment with WBRT Age (years) -49 50–69 70+ | 2.2 (0.1–60.8) 2.6 (0.1–55.2) | 1.0 (ref) 0.94 (0.77–1.16) | 1.0 (ref) 0.85 (0.69–1.05) |
3.6 (0.7–47.9) 2.8 (0.1–123.1) 2.0 (0.1–55.2) | 1.0 (ref) 1.09 (0.68–1.75) 1.59 (0.98–2.57) | 1.0 (ref) 1.00 (0.63–1.63) 1.33 (0.82–2.18) | |
| Marital status Alone Alone with children at home Cohabitation with no childern at home Cohabitation with children at home Calendar year 2008–2010 2011–2013 2014–2016 2017–2019 | 2.1 (0.1–123.1) 1.6 (0.7–47.9) 2.8 (0.1–60.8) 2.9 (0.1–22.0) | 1.0 (ref) 0.47 (0.13–1.68) 0.82 (0.66–1.01) 0.98 (0.53–1.79) | 1.0 (ref) 0.39 (0.11–1.39) 0.83 (0.66–1.04) 0.90 (0.48–1.67) |
2.2 (0.1–123.1) 2.5 (0.1–60.8) 2.8 (0.1–47.9) 2.6 (0.3–40.8) | 1.0 (ref) 0.85 (0.66–1.09) 1.00 (0.75–1.35) 0.75 (0.48–1.18) | 1.0 (ref) 0.86 (0.67–1.11) 1.14 (0.85–1.53) 0.90 (0.57–1.41) | |
| WBRT dose 4 Gy x 5 3 Gy x 10 WHO performance status score 0–1 2 3–4 Health care level one week before WBRT Home Hospital Palliative ward At primary lung cancer diagnosis | 2.4 (0.1–123.1) 3.5 (0.8–36.4) | 1.0 (ref) 0.84 (0.55–1.29) | 1.0 (ref) 0.89 (0.58–1.37) |
3.7 (0,1–123.1) 1.6 (0.1–16.5) 1.0 (0.1–5.5) | 1.0 (ref) 2.33 (1.82–3.00) 4.69 (3.31–6.64) | -- -- -- | |
3.45 (0.1–60.8) 1.38 (0.1–123.1) 0.85 (0.1–7.5) | 1.0 (ref) 2.25 (1.70–2.98) 3.66 (2.54–5.27) | 1.0 (ref) 1.56 (1.15–2.12) 2.26 (1.53–3.34) | |
| Stage M0 M1 EGFR Positive Negative | 2.0 (0.1–55.2) 2.6 (0.1–123.1) | 1.0 (ref) 1.07 (0.84–1.37) | 1.0 (ref) 1.14 (0.89–1.46) |
3.4 (0.1–60.8) 3.2 (0.4–55.2) | 1.0 (ref) 1.05 (0.70–1.56) | 1.0 (ref) 1.12 (0.75–1.69) | |
| Palliative treatments before WBRT | |||
| Palliative medical oncological treatment No Yes | 1.8 (0.1–40.8) 2.9 (0.1–123.1) | 1.0 (ref) 0.74 (0.58–0.93) | 1.0 (ref) 0.92 (0.72–1.16) |
| No of palliative chemotherapy regimens 0–2 2–6 | 2.3 (0.1–123.1) 3.4 (0.3–47.9) | 1.0 (ref) 0.71 (0.52–0.96) | 1.0 (ref) 0.84 (0.61–1.14) |
| Patients That Ever Came Home after WBRT | |||
|---|---|---|---|
| Yes | No | Total | |
| Total | 298 (77.6%) | 84 (21.9%) | 384 (100%) |
| Health care level one week before WBRT | |||
| Home | 257 (93.1%) | 18 (6.5%) | 276 (100%) |
| Hospital/Specialized palliative ward | 41 (38.0%) | 66 (61.1%) | 108 (100%) |
| Performance status WHO score before WBRT | |||
| 0–1 | 217 (90.8%) | 22 (9.2%) | 239 (100%) |
| 2 | 65 (64.4%) | 34 (33.6%) | 101 (100%) |
| 3–4 | 16 (36.4%) | 28 (63.6%) | 44 (100%) |
| Clinical and Biological Characteristics | N (%) of Lung Cancer Patients Not Coming Home | Adjusted OR 1 (95% CI) | Adjusted OR 2 (95% CI) |
|---|---|---|---|
| Gender Women Men | 57 (27.0) 27 (15.8) | 1.0 (ref) 0.51 (0.30–0.85) | 1.0 (ref) 0.37 (0.20–0.68) |
| At the time of treatment with WBRT | |||
| Age (years) -49 50–69 70+ | 4 (21.1) 45 (20.3) 35 (24.8) | 1.0 (ref) 0.92 (0.29–2.94) 1.30 (0.39–4.16) | 1.0 (ref) 0.92 (0.23–3.63) 1.04 (0.26–4.21) |
| Marital status Alone Alone with children at home Cohabitation with no childern at home Cohabitation with children at home | 54 (33.5) 1 (33.3) 27 (13.3) 2 (13.3) | 1.0 (ref) 1.25 (0.09–17.59) 0.32 (0.19–1.54) 0.31 (0.05–1.73) | 1.0 (ref) 0.70 (0.04–13.29) 0.29 (0.16–0.53) 0.15 (0.02–1.21) |
| Calendar year 2008–2010 2011–2013 2014–2016 2017–2019 | 23 (24.5) 46 (26.3) 12 (13.6) 3 (12.0) | 1.0 (ref) 1.10 (0.62–1.96) 0.47 (0.21–1.01) 0.42 (0.12–1.55) | 1.0 (ref) 1.07 0.43 (0.18–1.01) 0.52 (0.13–2.10) |
| WBRT dose 4 Gy x 5 3 Gy x 10 | 79 (22.0) 5 (21.7) | 1.0 (ref) 1.01 (0.36–2.88) | 1.0 (ref) 1.61 (0.53–4.89) |
| Performance status WHO score 0–1 2 3–4 | 22 (9.2) 34 (34.3) 28 (63.6) | 1.0 (ref) 5.10 (2.75–9.45) 17.48 (8.08–37.84) | -- -- -- |
| Health care level one week before WBRT Home Hospital Palliative ward | 18 (6.6) 37 (52.9) 29 (78.4) | 1.0 (ref) 16.06 (8.08–31.93) 60.32 (22.70–160.31) | 1.0 (ref) 10.56 (5.10–21.85) 37.15 (13.46–102.52) |
| At primary lung cancer diagnosis | |||
| Stage M0 M1 | 20 (23.0) 64 (22.1) | 1.0 (ref) 1.00 (0.56–1.80) | 1.0 (ref) 1.14 (0.59–2.19) |
| EGFR Negative Positive | 23 (17.0) 7 (20.0) | 1.0 (ref) 1.12 (0.41–3.02) | 1.0 (ref) 0.95 (0.28–3.24) |
| Palliative treatments before WBRT | |||
| Palliative medical oncological treatment Yes No | 45 (17.1) 39 (32.8) | 1.0 (ref) 0.44 (0.26–0.74) | 1.0 (ref) 0.61 (0.34–1.09) |
| Number of palliative oncological treatments 0–2 2–6 | 75 (22.9) 9 (16.7) | 1.0 (ref) 0.72 (0.33–1.57) | 1.0 (ref) 1.04 (0.44–2.49) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frisk, G.; Helde Frankling, M.; Warnqvist, A.; Björkhem-Bergman, L.; Hedman, M. Evaluation of Whole Brain Radiotherapy among Lung Cancer Patients with Brain Metastases in Relation to Health Care Level and Survival. Life 2022, 12, 525. https://doi.org/10.3390/life12040525
Frisk G, Helde Frankling M, Warnqvist A, Björkhem-Bergman L, Hedman M. Evaluation of Whole Brain Radiotherapy among Lung Cancer Patients with Brain Metastases in Relation to Health Care Level and Survival. Life. 2022; 12(4):525. https://doi.org/10.3390/life12040525
Chicago/Turabian StyleFrisk, Gabriella, Maria Helde Frankling, Anna Warnqvist, Linda Björkhem-Bergman, and Mattias Hedman. 2022. "Evaluation of Whole Brain Radiotherapy among Lung Cancer Patients with Brain Metastases in Relation to Health Care Level and Survival" Life 12, no. 4: 525. https://doi.org/10.3390/life12040525
APA StyleFrisk, G., Helde Frankling, M., Warnqvist, A., Björkhem-Bergman, L., & Hedman, M. (2022). Evaluation of Whole Brain Radiotherapy among Lung Cancer Patients with Brain Metastases in Relation to Health Care Level and Survival. Life, 12(4), 525. https://doi.org/10.3390/life12040525