Analysis of Quality of Life and Nutritional Status in Elderly Patients with Dysphagia in Order to Prevent Hospital Admissions in a COVID-19 Pandemic

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
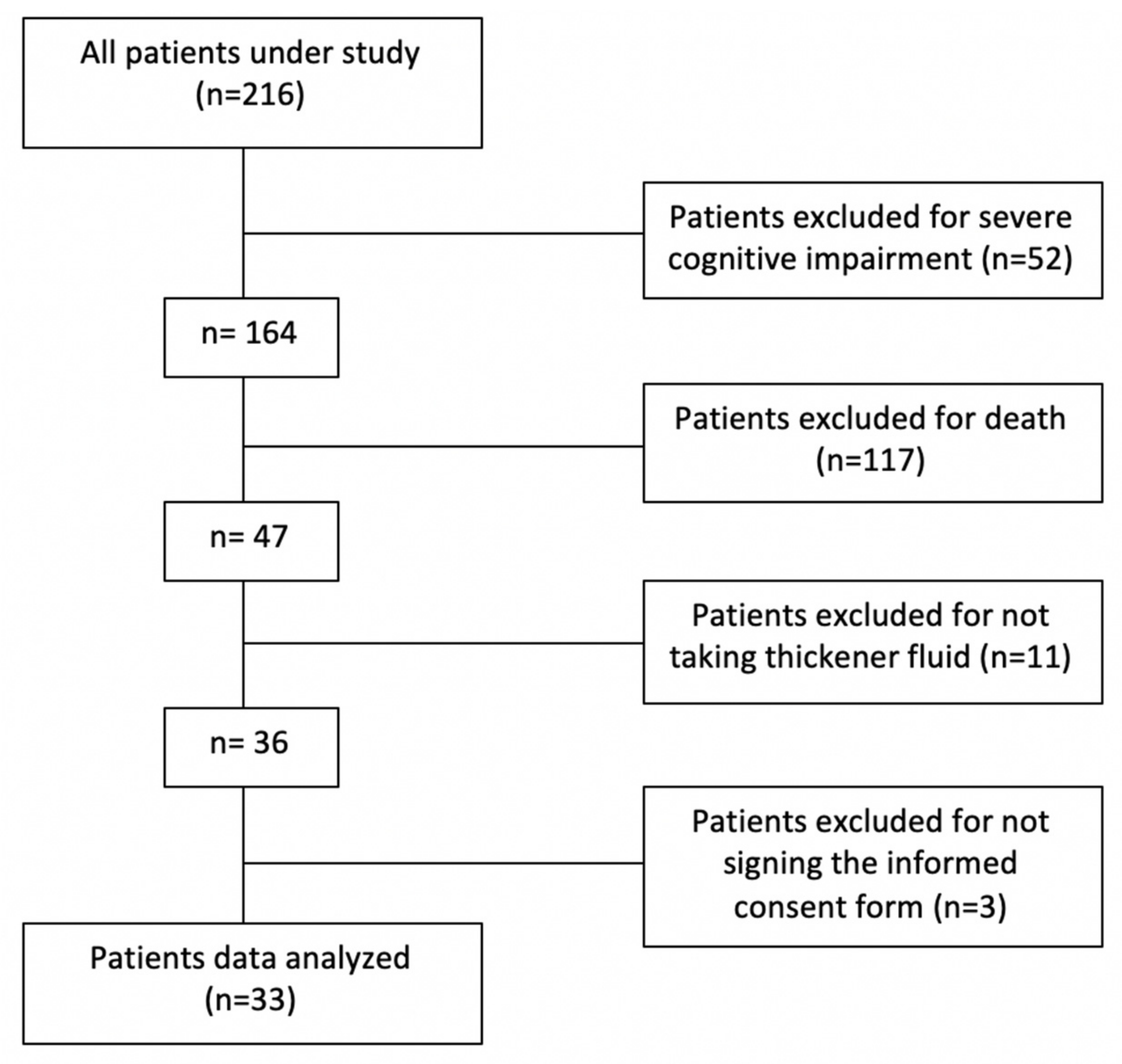
2.2. Study Design and Participants
2.3. Instruments and Measurement Procedure
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Study Population
3.2. Adaptation of Solid Texture and Liquid Viscosity
3.3. Nutritional Status
3.4. Quality of Life
3.5. Informal Caregiver Claudication (Zarit Questionnaire)
3.6. Efficiency of Telematic Consultation (Video Call)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Christmas, C.; Rogus-Pulia, N. Swallowing Disorders in the Older Population. J. Am. Geriatr. Soc. 2019, 67, 2643–2649. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferri, S.; Lauretani, F.; Pelá, G.; Meschi, T.; Maggio, M. The risk of dysphagia is associated with malnutrition and poor functional outcomes in a large population of outpatient older individuals. Clin. Nutr. 2019, 38, 2684–2689. [Google Scholar] [CrossRef] [PubMed]
- Byeon, H. Predicting the swallow-related quality of life of the elderly living in a local community using support vector machine. Int. J. Environ. Res. Public Health 2019, 16, 4269. [Google Scholar] [CrossRef] [PubMed]
- Michel, A.; Vérin, E.; Gbaguidi, X.; Druesne, L.; Roca, F.; Chassagne, P. Oropharyngeal dysphagia in community-dwelling older patients with dementia: Prevalence and relationship with geriatric parameters. J. Am. Med. Dir. Assoc. 2018, 19, 770–774. [Google Scholar] [CrossRef]
- Ortega, O.; Martín, A.; Clavé, P. Diagnosis and management of oropharyngeal dysphagia among older persons, state of the art. J. Am. Med. Dir. Assoc. 2017, 18, 576–582. [Google Scholar] [CrossRef]
- De Stefano, A.; Di Giovanni, P.; Kulamarva, G.; Gennachi, S.; Di Fonzo, F.; Sallustio, V.; Patrocinio, D.; Candido, S.; Lamarca, G.; Dispenza, F. Oropharyngeal dysphagia in elderly population suffering from mild cognitive impairment and mild dementia: Understanding the link. Am. J. Otolaryngol. 2020, 41, 102501. [Google Scholar] [CrossRef]
- De la Huerga Fernández-Bofill, T.; Hernández de las Heras, J.L.; Llamas Sandino, N.B. Prevalencia de disfagia orofaríngea en pacientes mayores de 65 años. Metas Enferm. 2015, 18, 49–55. [Google Scholar]
- Nimmons, D.; Michou, E.; Jones, M.; Pendleton, N.; Horan, M.; Hamdy, S. A longitudinal study of symptoms of oropharyngeal dysphagia in an elderly community-dwelling population. Dysphagia 2016, 31, 560–566. [Google Scholar] [CrossRef]
- Fırat Ozer, F.; Akın, S.; Soysal, T.; Gokcekuyu, B.M.; Erturk Zararsız, G. Relationship between dysphagia and sarcopenia with comprehensive geriatric evaluation. Dysphagia 2020, 27. [Google Scholar] [CrossRef]
- Espinosa-Val, M.C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O. Prevalence, risk factors, and complications of oropharyngeal dysphagia in older patients with dementia. Nutrients 2020, 12, 863. [Google Scholar] [CrossRef]
- Baijens, L.W.; Clavé, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders—European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [PubMed]
- Nawaz, S.; Tulunay-Ugur, O.E. Dysphagia in the older patient. Otolaryngol. Clin. N. Am. 2018, 51, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Attrill, S.; White, S.; Murray, J.; Hammond, S.; Doeltgen, S. Impact of oropharyngeal dysphagia on healthcare cost and length of stay in hospital: A systematic review. BMC Health Serv. Res. 2018, 18, 594. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Greene, M.; Sabido, I.; Stretton, M.; Miles, A. Economic costs of dysphagia among hospitalized patients. Laryngoscope 2020, 130, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Chebib, N.; Cuvelier, C.; Malézieux-Picard, A.; Parent, T.; Roux, X.; Fassier, T.; Müller, F.; Prendki, V. Correction to: Pneumonia prevention in the elderly patients: The other sides. Aging Clin. Exp. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zamora Mur, A.; Palacín Ariño, C.; Guardia Contreras, A.I.; Zamora Catevilla, A.; Clemente Roldán, E.; Santaliestra Grau, J. Importancia de la detección de la disfagia en pacientes geriátricos. Semergen 2018, 44, 168–173. [Google Scholar] [CrossRef]
- Nishida, T.; Yamabe, K.; Honda, S. Dysphagia is associated with oral, physical, cognitive and psychological frailty in Japanese community-dwelling elderly persons. Gerodontology 2020, 37, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Muhle, P.; Suntrup-Krueger, S.; Wirth, R.; Warnecke, T.; Dziewas, R. Swallowing in the elderly: Physiological changes, dysphagia, diagnostics and treatment. Z. Gerontol. Geriatr. 2019, 52, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Namasivayam-MacDonald, A.M.; Riquelme, L.F. Presbyphagia to dysphagia: Multiple perspectives and strategies for quality care of older adults. Semin. Speech Lang. 2019, 40, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Cantemir, S.; Laubert, A. Diagnostik und Therapie der Dysphagie. HNO 2017, 65, 347–356. [Google Scholar] [CrossRef]
- Kojima, K.; Mori, R.; Nishizawa, T.; Fujii, H. Problems of Home-Visiting Speech-Language-Hearing Therapists in Dysphagia Management. Gan Kagaku Ryoho 2018, 45, 18–20. [Google Scholar] [PubMed]
- Nakamura, T.; Amano, N. Proposal for preventing malnutrition in individuals on a texture-modified diet. Nutr. Health 2019, 25, 241–243. [Google Scholar] [CrossRef] [PubMed]
- Vellas, B.; Guigoz, Y.; Garry, P.J.; Nourhashemi, F.; Bennahum, D.; Lauque, S.; Albarede, J.L. The mini nutritional assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999, 15, 116–122. [Google Scholar] [CrossRef]
- Zaldibar-Barinaga, M.B.; Miranda-Artieda, M.; Zaldibar-Barinaga, A.; Pinedo-Otaola, S.; Erazo-Presser, P.; Tejada-Ezquerro, P. Versión española del Swallowing Quality of Life Questionnaire: Fase inicial de adaptación transcultural. Rehabilitación 2013, 47, 136–140. [Google Scholar] [CrossRef]
- Jaume, M.; Ballester Torralba, J.; Mariano de Miguel, A.M.; Gómez Gort, X.; Mazarico, S. Escala de Zarit reducida en cuidados paliativos. Med. Clín. 2005, 124, 651–653. [Google Scholar] [CrossRef]
- Rubio, M.A.; Salas-Salvadó, J.; Barbany, M.; Moreno, B.; Aranceta, J.; Bellido, D.; Blay, V.; Carraro, R.; Formiguera, M.F.; de Pablos, P.D. Comisión de redacción del documento “Consenso SEEDO 2007 para la evaluación del sobrepeso y la obesidad y el establecimiento de criterios de intervención terapéutica”. Rev. Esp. Obes. 2007, 128, 184–196. [Google Scholar]
- Martín, A.; Ortega, O.; Clavé, P. Disfagia orofaríngea, un nuevo síndrome geriátrico. Rev. Esp. Geriatr. Gerontol. 2018, 53, 3–5. [Google Scholar] [CrossRef]
- De Stefano, A.; Dispenza, F.; Kulamarva, G.; Lamarca, G.; Faita, A.; Merico, A.; Sardanelli, G.; Gabellone, S.; Antonaci, A. Predictive factors of severity and persistence of oropharyngeal dysphagia in sub-acute stroke. Eur. Arch. Otorhinolaryngol. 2020. [Google Scholar] [CrossRef]
- Pérez-Ros, P.; Martínez-Arnau, F.M. EQ-5D-3L for Assessing Quality of Life in Older Nursing Home Residents with Cognitive Impairment. Life (Basel) 2020, 10, 100. [Google Scholar] [CrossRef]
- Takizawa, C.; Gemmell, E.; Kenworthy, J.; Speyer, R. A systematic review of the prevalence of oropharyngeal dysphagia in stroke, Parkinson’s disease, Alzheimer’s disease, head injury, and pneumonia. Dysphagia 2016, 31, 434–441. [Google Scholar] [CrossRef]
- Rommel, N.; Hamdy, S. Oropharyngeal dysphagia: Manifestations and diagnosis. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 49–59. [Google Scholar] [CrossRef]
- Inui, A.; Takahashi, I.; Kurauchi, S.; Soma, Y.; Oyama, T.; Tamura, Y.; Noguchi, T.; Murashita, K.; Nakaji, S.; Kobayashi, W. Oral conditions and dysphagia in Japanese, community-dwelling middle- and older- aged adults, independent in daily living. Clin. Interv. Aging 2017, 12, 515–521. [Google Scholar] [CrossRef]
- Okabe, Y.; Takeuchi, K.; Izumi, M.; Furuta, M.; Takeshita, T.; Shibata, Y.; Kageyama, S.; Ganaha, S.; Yamashita, Y. Posterior teeth occlusion and dysphagia risk in older nursing home residents: A cross-sectional observational study. J. Oral Rehabil. 2017, 44, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.R.; Lawrence, J.; Williams, D., Jr.; Mainous, A., III. Population-Level Interest and Telehealth Capacity of US Hospitals in Response to COVID-19: Cross-Sectional Analysis of Google Search and National Hospital Survey Data. JMIR Public Health Surveill. 2020, 6, e18961. [Google Scholar] [CrossRef] [PubMed]
- Martín, A.; Ortega, O.; Roca, M.; Arús, M.; Clavé, P. Effect of a minimal-massive intervention in hospitalized older patients with oropharyngeal dysphagia: A proof of concept study. J. Nutr. Health Aging 2018, 22, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, W.V.; Arreola, V.; Sanz, P.; Necati, E.; Bolivar-Prados, M.; Michou, E.; Ortega, O.; Clavé, P. Pathophysiology of swallowing dysfunction in Parkinson disease and lack of dopaminergic impact on the swallow function and on the effect of thickening agents. Brain Sci. 2020, 10, 609. [Google Scholar] [CrossRef]
- Bolivar-Prados, M.; Rofes, L.; Arreola, V.; Guida, S.; Nascimento, W.V.; Martin, A.; Vilardell, N.; Ortega Fernández, O.; Ripken, D.; Lansink, M.; et al. Effect of a gum-based thickener on the safety of swallowing in patients with poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2019, 31, e13695. [Google Scholar] [CrossRef]
- Newman, R.; Vilardell, N.; Clavé, P.; Speyer, R. Effect of bolus viscosity on the safety and efficacy of swallowing and the kinematics of the swallow response in patients with oropharyngeal dysphagia: White Paper by the European Society for Swallowing Disorders (ESSD). Dysphagia 2016, 31, 232–249. [Google Scholar] [CrossRef]
- Mañas-Martínez, A.B.; Bucar-Barjud, M.; Campos-Fernández, J.; Gimeno-Orna, J.A.; Pérez-Calvo, J.; Ocón-Bretón, J. Association of positive screening for dysphagia with nutritional status and long-term mortality in hospitalized elderly patients. Endocrinol. Diabetes Nutr. 2018, 65, 402–408. [Google Scholar] [CrossRef]
- Huppertz, V.; Halfens, R.; van Helvoort, A.; de Groot, L.; Baijens, L.; Schols, J. Association between oropharyngeal dysphagia and malnutrition in dutch nursing home residents: Results of the national prevalence measurement of quality of care. J. Nutr. Health Aging 2018, 22, 1246–1252. [Google Scholar] [CrossRef]
- Fávaro-Moreira, N.C.; Krausch-Hofmann, S.; Matthys, C.; Vereecken, C.; Vanhauwaert, E.; Declercq, A.; Bekkering, G.E.; Duyck, J. Risk factors for malnutrition in older adults: A systematic review of the literature based on longitudinal data. Adv. Nutr. (Bethesda Md.) 2016, 7, 507–522. [Google Scholar] [CrossRef]
- Carrión, S.; Cabré, M.; Monteis, R.; Roca, M.; Palomera, E.; Serra-Prat, M.; Rofes, L.; Clavé, P. Oropharyngeal dysphagia is a prevalent risk factor for malnutrition in a cohort of older patients admitted with an acute disease to a general hospital. Clin. Nutr. (Edinb. Scotl.) 2015, 34, 436–442. [Google Scholar] [CrossRef]
- Zhang, Z.; Pereira, S.L.; Luo, M.; Matheson, E.M. Evaluation of blood biomarkers associated with risk of malnutrition in older adults: A systematic review and meta-analysis. Nutrients 2017, 9, 829. [Google Scholar] [CrossRef] [PubMed]
- Miao, J.P.; Quan, X.Q.; Zhang, C.T.; Zhu, H.; Ye, M.; Shen, L.Y.; Guo, Q.H.; Zhu, G.Y.; Mei, Q.J.; Wu, Y.X.; et al. Comparison of two malnutrition risk screening tools with nutritional biochemical parameters, BMI and length of stay in Chinese geriatric inpatients: A multicenter, cross-sectional study. BMJ Open 2019, 9, e022993. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Hu, H.Y.; Huang, N.; Chou, Y.C.; Li, C.P.; Chou, Y.J. Albumin levels and cause-specific mortality in community-dwelling older adults. Prev. Med. 2018, 112, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Ota, A.; Kondo, N.; Murayama, N.; Tanabe, N.; Shobugawa, Y.; Kondo, K.; Japan Gerontological Evaluation Study (JAGES) Group. Serum Albumin Levels and Economic Status in Japanese Older Adults. PLoS ONE 2016, 11, e0155022. [Google Scholar] [CrossRef] [PubMed]
- Cabrerizo, S.; Cuadras, D.; Gomez-Busto, F.; Artaza-Artabe, I.; Marín-Ciancas, F.; Malafarina, V. Serum albumin and health in older people: Review and meta analysis. Maturitas 2015, 81, 17–27. [Google Scholar] [CrossRef]
- Byun, S.E.; Kwon, K.B.; Kim, S.H.; Lim, S.J. The prevalence, risk factors and prognostic implications of dysphagia in elderly patients undergoing hip fracture surgery in Korea. BMC Geriatr. 2019, 19, 356. [Google Scholar] [CrossRef]
- Gyan, E.; Raynard, B.; Durand, J.P.; Lacau Saint Guily, J.; Gouy, S.; Movschin, M.L.; Khemissa, F.; Flori, N.; Oziel-Taieb, S.; Bannier Braticevic, C.; et al. Malnutrition in patients with cancer: Comparison of perceptions by patients, relatives, and physicians-results of the NutriCancer2012 Study. JPEN J. Parenter. Enter. Nutr. 2018, 42, 255–260. [Google Scholar] [CrossRef]
- Chen, P.H.; Golub, J.S.; Hapner, E.R.; Johns, M.M., 3rd. Prevalence of perceived dysphagia and quality-of-life impairment in a geriatric population. Dysphagia 2009, 24, 1–6. [Google Scholar] [CrossRef]
- Ghimire, S.; Baral, B.K.; Pokhrel, B.R.; Pokhrel, A.; Acharya, A.; Amatya, D.; Amatya, P.; Mishra, S.R. Depression, malnutrition, and health-related quality of life among Nepali older patients. BMC Geriatr. 2018, 18, 191. [Google Scholar] [CrossRef] [PubMed]
- Alvear, S.; Rodríguez, P.; Riveros, C.; Arenas, Á.; Canteros, J. Factores sociales del estado de salud autorreportado de personas mayores, en Chile. Rev. Med. Chile 2019, 147, 1407–1414. [Google Scholar] [CrossRef] [PubMed]
- Hale, M.D.; Santorelli, G.; Brundle, C.; Clegg, A. A cross-sectional study assessing agreement between self-reported and general practice-recorded health conditions among community dwelling older adults. Age Ageing 2019, 49, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Park, H.S.; Park, S.W.; Kim, J.H. The impact of dysphagia on quality of life in stroke patients. Medicine 2020, 99, e21795. [Google Scholar] [CrossRef]
- Reyes-Torres, C.A.; Castillo-Martínez, L.; Reyes-Guerrero, R.; Ramos-Vázquez, A.G.; Zavala-Solares, M.; Cassis-Nosthas, L.; Serralde-Zúñiga, A.E. Design and implementation of modified-texture diet in older adults with oropharyngeal dysphagia: A randomized controlled trial. Eur. J. Clin. Nutr. 2019, 73, 989–996. [Google Scholar] [CrossRef]
- O’Keeffe, S.T. Use of modified diets to prevent aspiration in oropharyngeal dysphagia: Is current practice justified? BMC Geriatr. 2018, 18, 167. [Google Scholar] [CrossRef]
- Beck, A.M.; Kjaersgaard, A.; Hansen, T.; Poulsen, I. Systematic review and evidence based recommendations on texture modified foods and thickened liquids for adults (above 17 years) with oropharyngeal dysphagia—An updated clinical guideline. Clin. Nutr. (Edinb. Scotl.) 2018, 37, 1980–1991. [Google Scholar] [CrossRef]
- Xiong, C.; Biscardi, M.; Astell, A.; Nalder, E.; Cameron, J.I.; Mihailidis, A.; Colantonio, A. Sex and gender differences in caregiving burden experienced by family caregivers of persons with dementia: A systematic review. PLoS ONE 2020, 15, e0231848. [Google Scholar] [CrossRef]
- Abdel-Malek, R.; Farag, D.E.; Shohdy, K.S.; Cox, S. Availability of Informal Caregivers for Palliative Care Patients with Cancer: Is there a Difference between Higher- and Lower-Income Settings. Indian J. Palliat. Care 2019, 25, 379–382. [Google Scholar] [CrossRef]
- Sakakibara, K.; Kabayama, M.; Ito, M. Experiences of “endless” caregiving of impaired elderly at home by family caregivers: A qualitative study. BMC Res. Notes 2015, 8, 827. [Google Scholar] [CrossRef]
- Jaul, E.; Barron, J.; Rosenzweig, J.P.; Menczel, J. An overview of co-morbidities and the development of pressure ulcers among older adults. BMC Geriatr. 2018, 18, 305. [Google Scholar] [CrossRef] [PubMed]
- Sieber, C.C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Ayres, A.; Jotz, G.P.; Rieder, C.R.; Schuh, A.F.; Olchik, M.R. The impact of dysphagia therapy on quality of life in patients with Parkinson’s disease as measured by the Swallowing Quality of Life Questionnaire (SWALQOL). Int. Arch. Otorhinolaryngol. 2016, 20, 202–206. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Biochemical Parameters | N | Minimum | Maximum | M ± SD |
|---|---|---|---|---|
| Glucose (mg/dL) | 33 | 62.00 | 225.00 | 119.4 ± 41.8 |
| Urea (mg/dL) | 33 | 17.00 | 82.00 | 44.5 ± 14.8 |
| Creatinine (mg/dL) | 33 | 0.51 | 62.00 | 2.9 ± 10.6 |
| Uric acid (mg/dL) | 32 | 2.00 | 10.50 | 5.3 ± 1.9 |
| Total proteins (g/dL) | 31 | 4.70 | 7.80 | 6.5 ± 0.7 |
| Albumin (g/dL) | 31 | 2.40 | 4.70 | 3.8 ± 0.5 |
| Calcium (mg/dL) | 30 | 7.20 | 10.20 | 9.1 ± 0.6 |
| Phosphorus (mg/dL) | 22 | 1.80 | 4.70 | 3.3 ± 0.8 |
| Bilirubin (mg/dL) | 32 | 0.14 | .86 | 0.4 ± 0.2 |
| Sodium (mEq/L) | 33 | 133.00 | 146.00 | 141 ± 3.0 |
| Potassium (mEq/L) | 33 | 3.60 | 5.60 | 4.5 ± 0.5 |
| Chloride (mEq/L) | 33 | 93.00 | 109.00 | 101.2 ± 3.8 |
| Iron (µg/dL) | 22 | 20.00 | 140.00 | 66.8 ± 31.3 |
| Ferritin (ng/mL) | 30 | 14.00 | 549.00 | 136.5 ± 133.3 |
| Transferrin (mg/dL) | 17 | 123.00 | 315.00 | 214.7 ± 54.0 |
| Transferrin saturation (%) | 16 | 7.30 | 45.60 | 19.4 ± 10.7 |
| Folate (ng/mL) | 18 | 3.20 | 23.00 | 9.9 ± 5.9 |
| Vitamin B12 (pg/mL) | 23 | 175.00 | 760.00 | 514.4 ± 188.2 |
| Triglycerides (mg/dL) | 31 | 43.00 | 526.00 | 141.0 ± 99.1 |
| Cholesterol (mg/dL) | 31 | 91.00 | 234.00 | 152.0 ± 36.2 |
| HDL-cholesterol (mg/dL) | 25 | 25.00 | 81.00 | 47.6 ± 16.3 |
| LDL-cholesterol (mg/dL) | 25 | 7.00 | 143.00 | 73.6 ± 31.7 |
| GGT (U/L) | 30 | 5.00 | 158.00 | 31.4 ± 35.5 |
| Alkaline phosphatase (U/L) | 32 | 45.00 | 190.00 | 86.2 ± 32.5 |
| Creatine kinase (U/L) | 25 | 14.00 | 292.00 | 65.5 ± 57.0 |
| GOT (AST) (U/L) | 33 | 10.00 | 33.00 | 17.7 ± 5.0 |
| GPT (ALT) (U/L) | 32 | 5.00 | 39.00 | 13.9 ± 8.0 |
| C-reactive protein (mg/dL) | 28 | 0.21 | 11.81 | 2.6 ± 3.3 |
| MDRD (mL/min/1.73 m2) | 26 | 40.82 | 182.52 | 69.7 ± 32.7 |
| CKD-EPI equation (mL/min/1.73 m2) | 30 | 34.74 | 99.34 | 62.9 ± 19.8 |
| TSH (µU/mL) | 29 | 0.93 | 6.80 | 2.24 ± 1.2 |
| Glycosylated hemoglobin (%) | 23 | 5.30 | 9.50 | 6.7 ± 1.2 |
| MNA_DX | Total | |||||
|---|---|---|---|---|---|---|
| NORMAL | RISK | MALNUT | ||||
| Subjective Malnutrition | NORMAL | Count | 4 | 17 | 6 | 27 |
| % within subjective malnutrition | 14.8% | 63.0% | 22.2% | 100.0% | ||
| % within MNA_DX | 100.0% | 85.0% | 66.7% | 81.8% | ||
| % of total | 12.1% | 51.5% | 18.2% | 81.8% | ||
| RISK | Count | 0 | 3 | 2 | 5 | |
| % within subjective malnutrition | 0.0% | 60.0% | 40.0% | 100.0% | ||
| % within MNA_DX | 0.0% | 15.0% | 22.2% | 15.2% | ||
| % of total | 0.0% | 9.1% | 6.1% | 15.2% | ||
| MALNUT | Count | 0 | 0 | 1 | 1 | |
| % within subjective malnutrition | 0.0% | 0.0% | 100.0% | 100.0% | ||
| % within MNA_DX | 0.0% | 0.0% | 11.1% | 3.0% | ||
| % of total | 0.0% | 0.0% | 3.0% | 3.0% | ||
| Total | Count | 4 | 20 | 9 | 33 | |
| % within subjective malnutrition | 12.1% | 60.6% | 27.3% | 100.0% | ||
| % within MNA_DX | 100.0% | 100.0% | 100.0% | 100.0% | ||
| % of total | 12.1% | 60.6% | 27.3% | 100.0% | ||
| DOMAINS | M ± SD |
|---|---|
| OVERLOAD | 3.4 ± 1.4 |
| It is very difficult for me to bear my swallowing problem | 3.4 ± 1.4 |
| My swallowing problem is a major concern in my life | 3.5 ± 1.4 |
| DURATION OF INTAKE | 3.4 ± 1.2 |
| I take longer to eat than others | 3.4 ± 1.3 |
| It takes me a long time to finish a meal | 3.5 ± 1.3 |
| APPETITE | 3.8 ± 1.3 |
| Most days, I don’t care whether I eat or not | 3.5 ± 1.3 |
| I no longer enjoy eating | 3.8 ± 1.4 |
| I am hardly ever hungry anymore | 3.8 ± 1.4 |
| FREQUENCY OF SYMPTOMS | 3.9 ± 0.9 |
| I cough | 3.6 ± 1.4 |
| Choking on solid food | 3.8 ± 1.4 |
| Choking on liquid food | 3.7 ± 1.3 |
| Saliva or thick phlegm | 3.7 ± 1.4 |
| I choke when I eat | 3.8 ± 1.3 |
| Excess saliva or phlegm | 3.4 ± 1.5 |
| Having to clear my throat (throat clearing) | 3.6 ± 1.5 |
| Drooling | 4.1 ± 1.4 |
| Problems when chewing | 2.6 ± 1.8 |
| Food residues in the throat | 4.2 ± 1.1 |
| Food residues in the mouth | 4.4 ± 1.1 |
| Solids and liquids coming out of the mouth | 4.4 ± 1.1 |
| Solids and liquids coming out of the nose | 4.4 ± 1.1 |
| Coughing up food or liquid | 4.5 ± 0.9 |
| SELECTION OF FOOD | 4.5 ± 1.1 |
| I have a problem thinking about what I can eat | 4.5 ± 1.1 |
| It is difficult to find foods that I like and can eat | 4.5 ± 1.1 |
| COMMUNICATION | 3.4 ± 1.5 |
| Others find it difficult to understand me when I speak | 3.5 ± 1.5 |
| I find it difficult to speak clearly | 3.4 ± 1.5 |
| FEARS | 4.0 ± 1.4 |
| I am afraid of choking when I eat | 3.9 ± 1.3 |
| I am worried about having pneumonia | 4.0 ± 1.3 |
| I am afraid to choke when I drink | 4.0 ± 1.3 |
| I never know when I am going to choke | 4.0 ± 1.2 |
| MENTAL HEALTH | 3.5 ± 1.4 |
| My swallowing problem depresses me | 3.5 ± 1.4 |
| My swallowing problem irritates me | 3.5 ± 1.4 |
| It bothers me to have to take so many precautions when eating or drinking | 3.5 ± 1.4 |
| My swallowing problem frustrates me | 3.5 ± 1.4 |
| I am discouraged because of my swallowing problem | 3.5 ± 1.4 |
| SOCIAL | 3.6 ± 1.3 |
| I do not go out to eat because of my swallowing | 3.6 ± 1.3 |
| My swallowing problem makes my social life difficult | 3.6 ± 1.3 |
| My usual activities have changed due to my swallowing problem | 3.7 ± 1.3 |
| I do not enjoy social gatherings because of my swallowing problem | 3.7 ± 1.3 |
| My role with my family and friends has changed due to my swallowing problem | 3.7 ± 1.4 |
| FATIGUE | 3.5 ± 1.0 |
| I feel weak | 3.3 ± 1.1 |
| I feel tired | 3.6 ± 1.1 |
| I feel exhausted | 3.6 ± 1.1 |
| SLEEP | 3.9 ± 1.1 |
| I have trouble sleeping | 3.9 ± 1.1 |
| I have trouble keeping asleep | 3.9 ± 1.1 |
| D1 | D2 | D3 | D4 | D5 | D6 | D7 | D8 | D9 | D10 | D11 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| D1 | Pearson correlation | 1 | 0.286 | 0.444 ** | 0.580 ** | 0.251 | 0.401 * | 0.398 * | 0.701 ** | 0.426 * | 0.381 * | −0.116 |
| Sig. (2-tailed) | 0.106 | 0.010 | 0.000 | 0.159 | 0.021 | 0.022 | 0.000 | 0.013 | 0.029 | 0.520 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D2 | Pearson correlation | 0.286 | 1 | 0.723 ** | 0.274 | 0.292 | 0.371 * | 0.344 * | 0.142 | 0.311 | 0.317 | 0.147 |
| Sig. (2-tailed) | 0.106 | 0.000 | 0.122 | 0.099 | 0.034 | 0.050 | 0.430 | 0.078 | 0.072 | 0.415 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D3 | Pearson correlation | 0.444 ** | 0.723 ** | 1 | 0.470 ** | 0.493 ** | 0.221 | 0.428 * | 0.357 * | 0.383 * | 0.381 * | −0.002 |
| Sig. (2-tailed) | 0.010 | 0.000 | 0.006 | 0.004 | 0.217 | 0.013 | 0.041 | 0.028 | 0.029 | 0.992 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D4 | Pearson correlation | 0.580 ** | 0.274 | 0.470 ** | 1 | 0.364 * | 0.342 | 0.763 ** | 0.714 ** | 0.558 ** | 0.466 ** | −0.026 |
| Sig. (2-tailed) | 0.000 | 0.122 | 0.006 | 0.037 | 0.051 | 0.000 | 0.000 | 0.001 | 0.006 | 0.888 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D5 | Pearson correlation | 0.251 | 0.292 | 0.493 ** | 0.364 * | 1 | −0.199 | 0.262 | 0.473 ** | 0.217 | 0.071 | −0.002 |
| Sig. (2-tailed) | 0.159 | 0.099 | 0.004 | 0.037 | 0.267 | 0.141 | 0.005 | 0.224 | 0.695 | 0.990 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D6 | Pearson correlation | 0.401 * | 0.371 * | 0.221 | 0.342 | −0.199 | 1 | 0.448 ** | 0.345 * | 0.496 ** | 0.328 | 0.345 * |
| Sig. (2-tailed) | 0.021 | 0.034 | 0.217 | 0.051 | 0.267 | 0.009 | 0.049 | 0.003 | 0.062 | 0.049 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D7 | Pearson correlation | 0.398 * | 0.344 * | 0.428 * | 0.763 ** | 0.262 | 0.448 ** | 1 | 0.648 ** | 0.687 ** | 0.135 | −0.014 |
| Sig. (2-tailed) | 0.022 | 0.050 | 0.013 | 0.000 | 0.141 | 0.009 | 0.000 | 0.000 | 0.453 | 0.938 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D8 | Pearson correlation | 0.701 ** | 0.142 | 0.357 * | 0.714 ** | 0.473 ** | 0.345 * | 0.648 ** | 1 | 0.731 ** | 0.301 | 0.061 |
| Sig. (2-tailed) | 0.000 | 0.430 | 0.041 | 0.000 | 0.005 | 0.049 | 0.000 | 0.000 | 0.089 | 0.734 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D9 | Pearson correlation | 0.426 * | 0.311 | 0.383 * | 0.558 ** | 0.217 | 0.496 ** | 0.687 ** | 0.731 ** | 1 | 0.363 * | 0.152 |
| Sig. (2-tailed) | 0.013 | 0.078 | 0.028 | 0.001 | 0.224 | 0.003 | 0.000 | 0.000 | 0.038 | 0.399 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D10 | Pearson correlation | 0.381 * | 0.317 | 0.381 * | 0.466 ** | 0.071 | 0.328 | 0.135 | 0.301 | 0.363 * | 1 | 0.144 |
| Sig. (2-tailed) | 0.029 | 0.072 | 0.029 | 0.006 | 0.695 | 0.062 | 0.453 | 0.089 | 0.038 | 0.425 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | |
| D11 | Pearson correlation | −0.116 | 0.147 | −0.002 | −0.026 | −0.002 | 0.345* | −0.014 | 0.061 | 0.152 | 0.144 | 1 |
| Sig. (2-tailed) | 0.520 | 0.415 | 0.992 | 0.888 | 0.990 | 0.049 | 0.938 | 0.734 | 0.399 | 0.425 | ||
| N | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 | 33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Ruiz, V.E.; Paredes-Ibáñez, R.; Armero-Barranco, D.; Sánchez-Romera, J.F.; Ferrer, M. Analysis of Quality of Life and Nutritional Status in Elderly Patients with Dysphagia in Order to Prevent Hospital Admissions in a COVID-19 Pandemic. Life 2021, 11, 22. https://doi.org/10.3390/life11010022
Fernández-Ruiz VE, Paredes-Ibáñez R, Armero-Barranco D, Sánchez-Romera JF, Ferrer M. Analysis of Quality of Life and Nutritional Status in Elderly Patients with Dysphagia in Order to Prevent Hospital Admissions in a COVID-19 Pandemic. Life. 2021; 11(1):22. https://doi.org/10.3390/life11010022
Chicago/Turabian StyleFernández-Ruiz, Virginia E., Rocío Paredes-Ibáñez, David Armero-Barranco, Juan Francisco Sánchez-Romera, and Mercedes Ferrer. 2021. "Analysis of Quality of Life and Nutritional Status in Elderly Patients with Dysphagia in Order to Prevent Hospital Admissions in a COVID-19 Pandemic" Life 11, no. 1: 22. https://doi.org/10.3390/life11010022
APA StyleFernández-Ruiz, V. E., Paredes-Ibáñez, R., Armero-Barranco, D., Sánchez-Romera, J. F., & Ferrer, M. (2021). Analysis of Quality of Life and Nutritional Status in Elderly Patients with Dysphagia in Order to Prevent Hospital Admissions in a COVID-19 Pandemic. Life, 11(1), 22. https://doi.org/10.3390/life11010022