
Model Predictive Control of COVID-19 Pandemic with Social Isolation and Vaccination Policies in Thailand


Abstract
:1. Introduction
2. Mathematical Model
2.1. Invariant Region
2.2. The Equilibrium Points
- Disease-free equilibrium point :
- Endemic equilibrium point :whereand
2.3. The Basic Reproduction Number
3. Model Predictive Control (MPC)
3.1. Linearization and Discretization
3.2. Cost Function of the Model Predictive Control,
4. Results
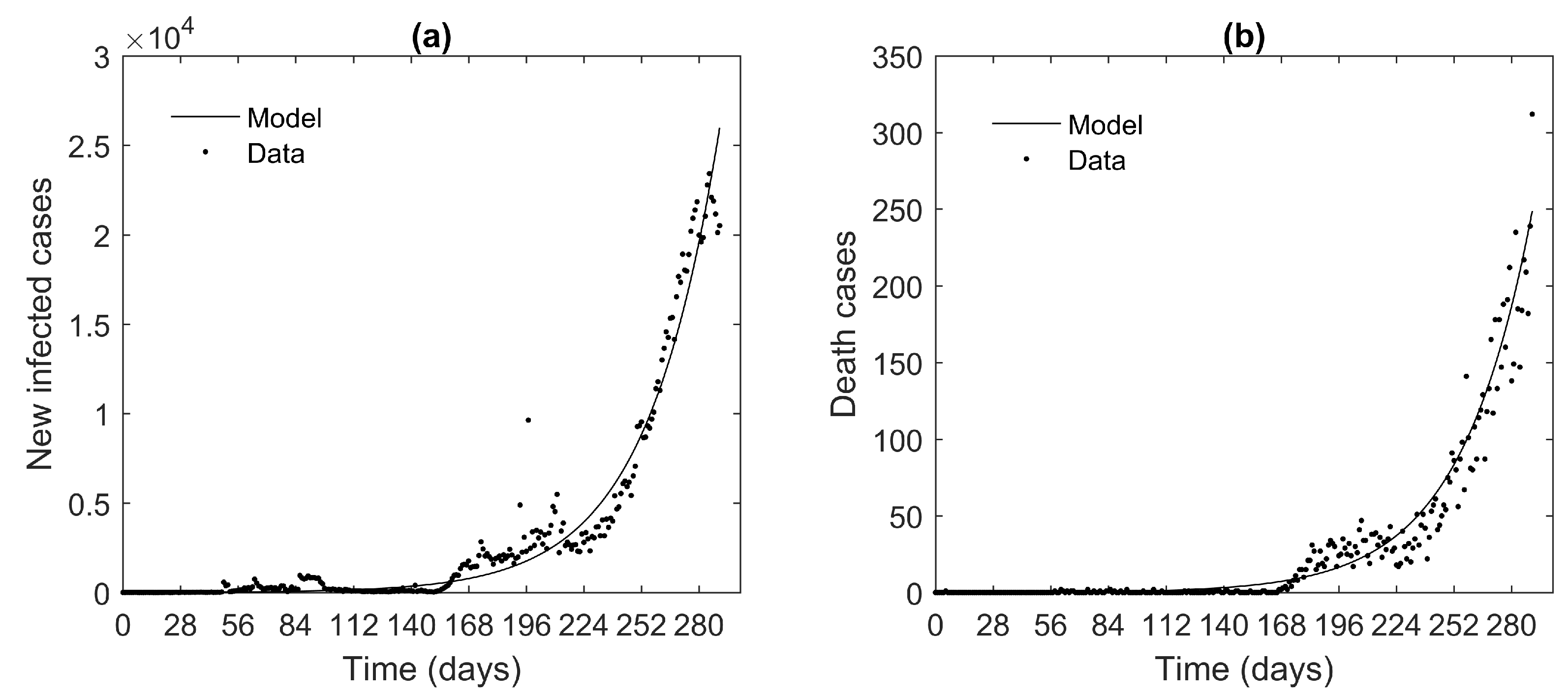
4.1. Mathematical Modeling of COVID-19 Pandemic in Thailand
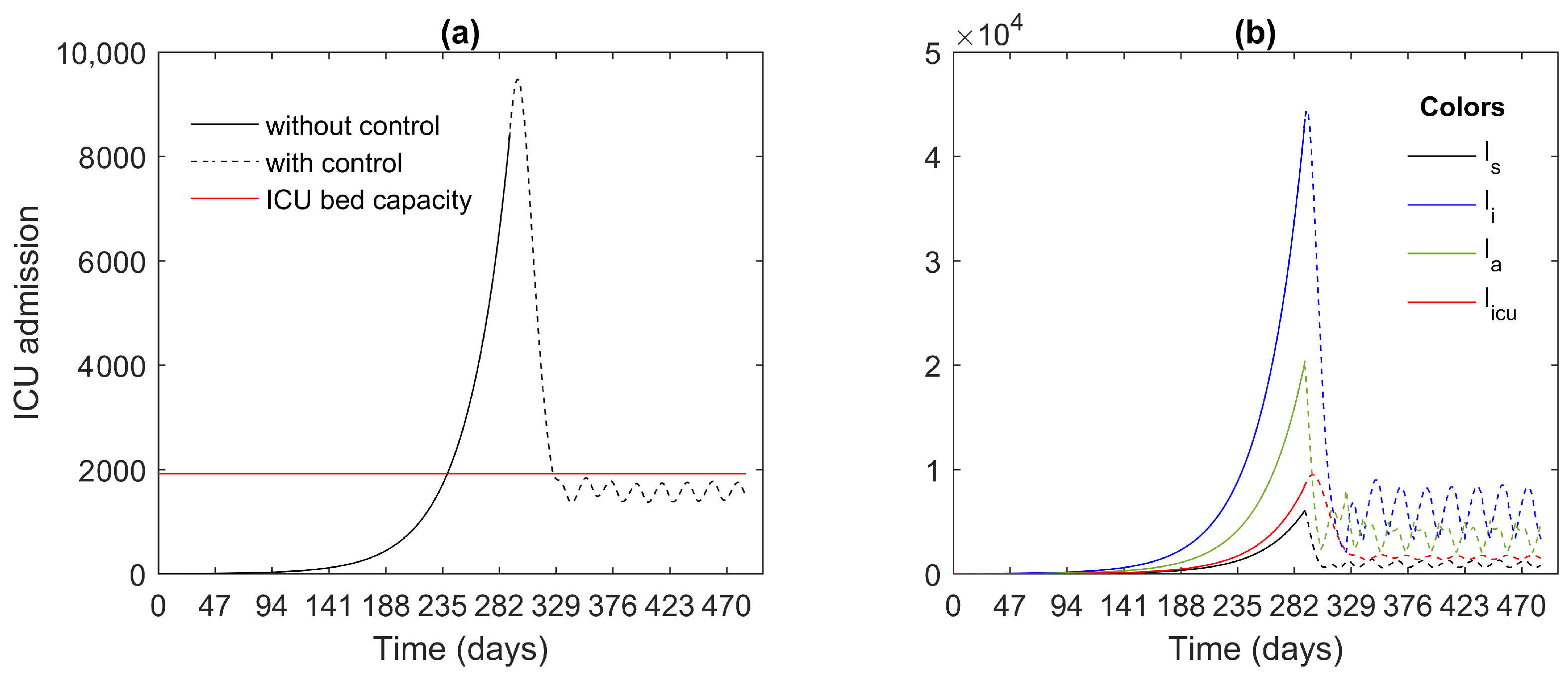
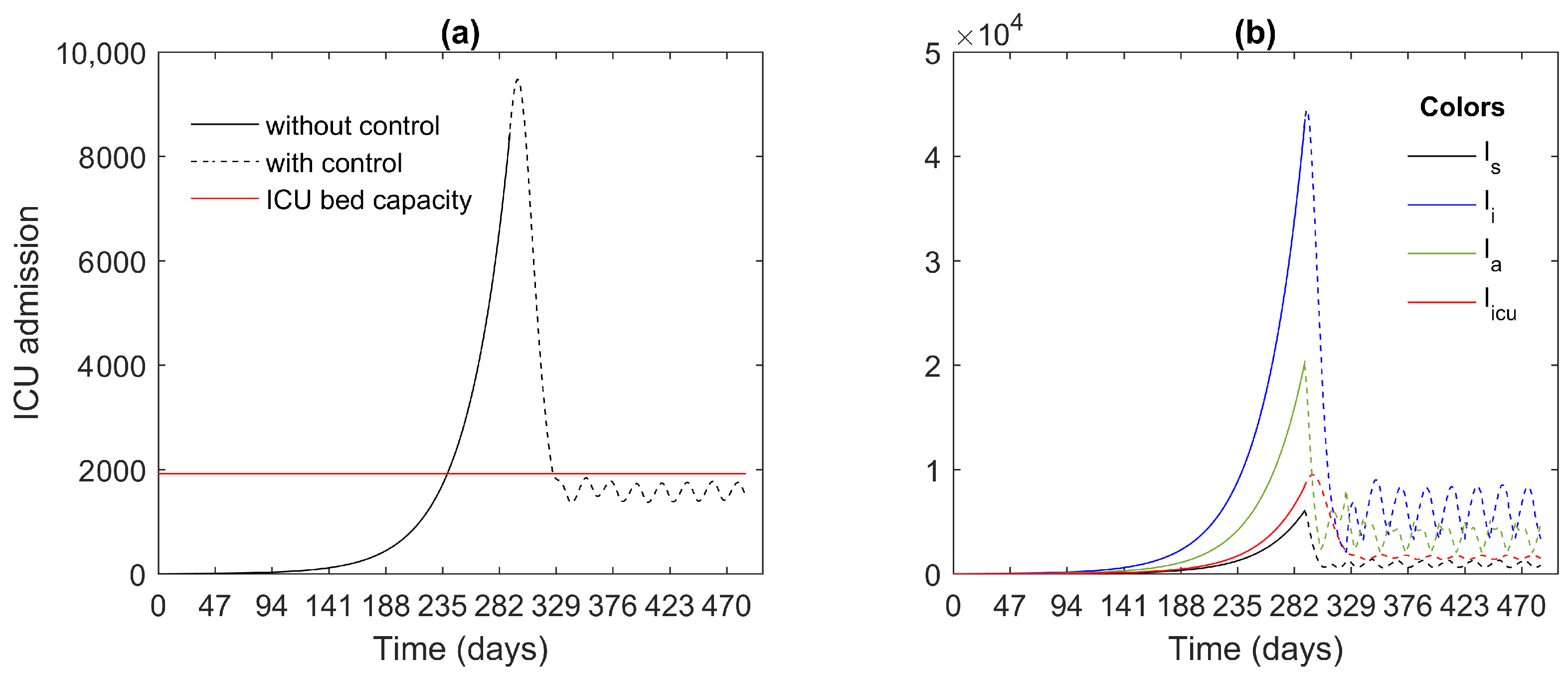
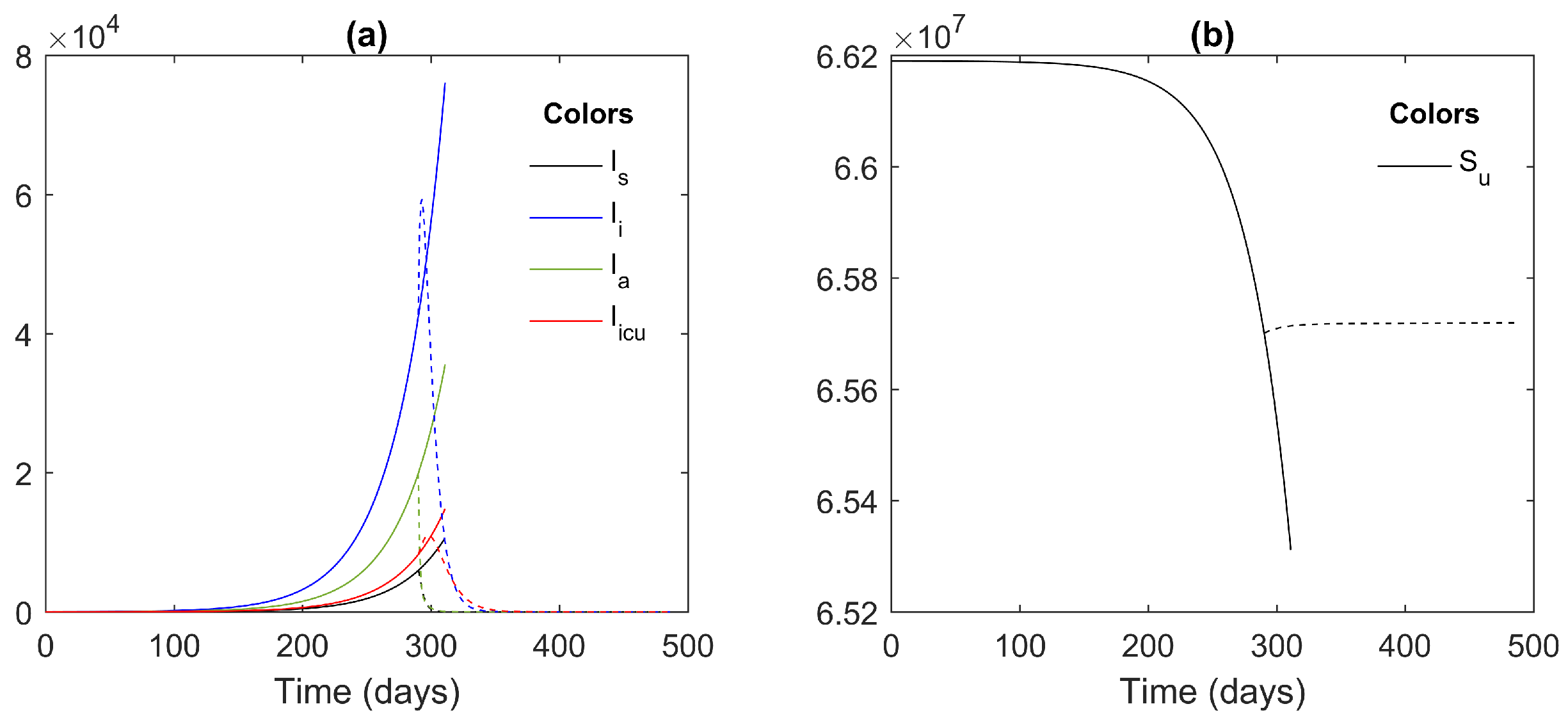
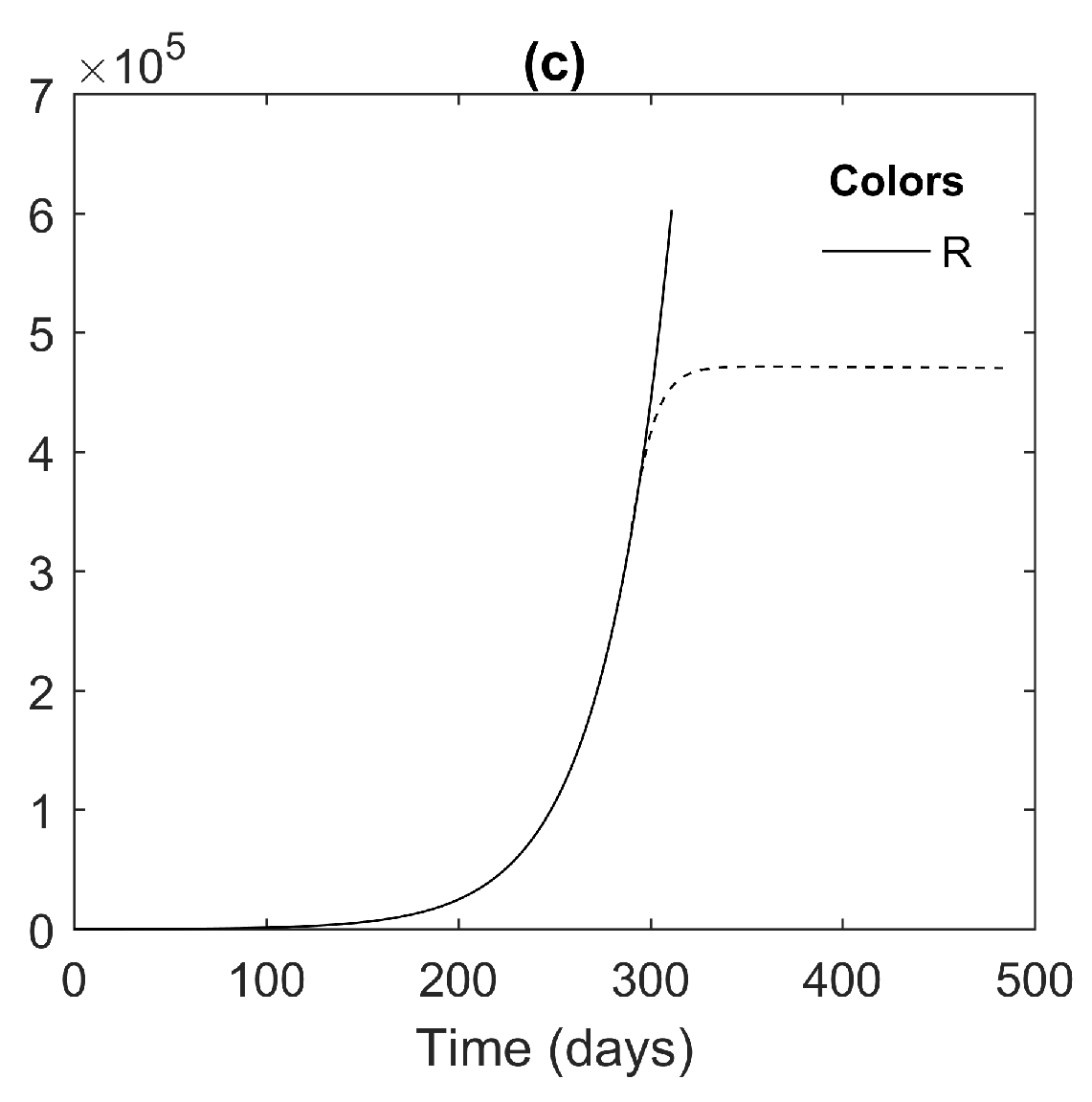
4.2. ICU Capacity Restriction and the Effectiveness of Social Isolation Strategies
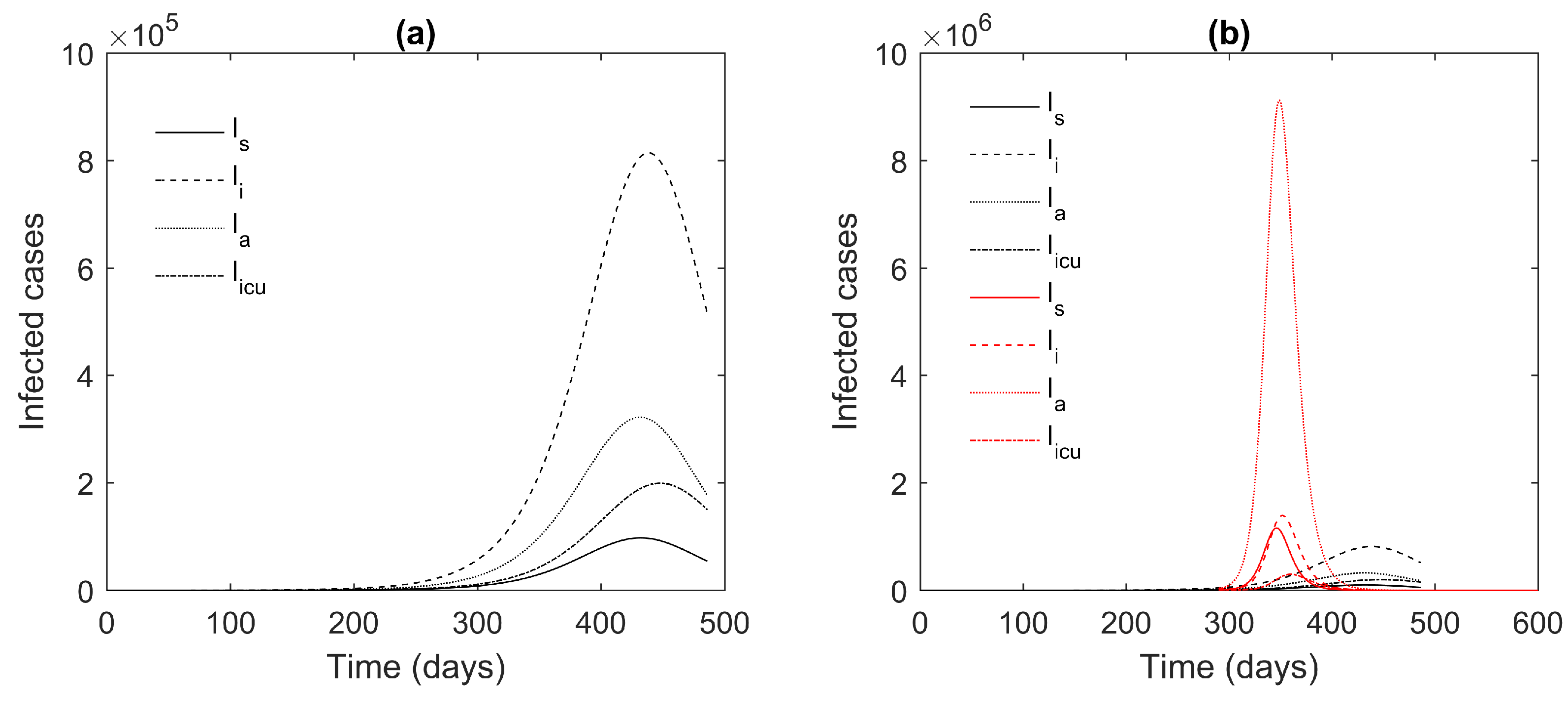
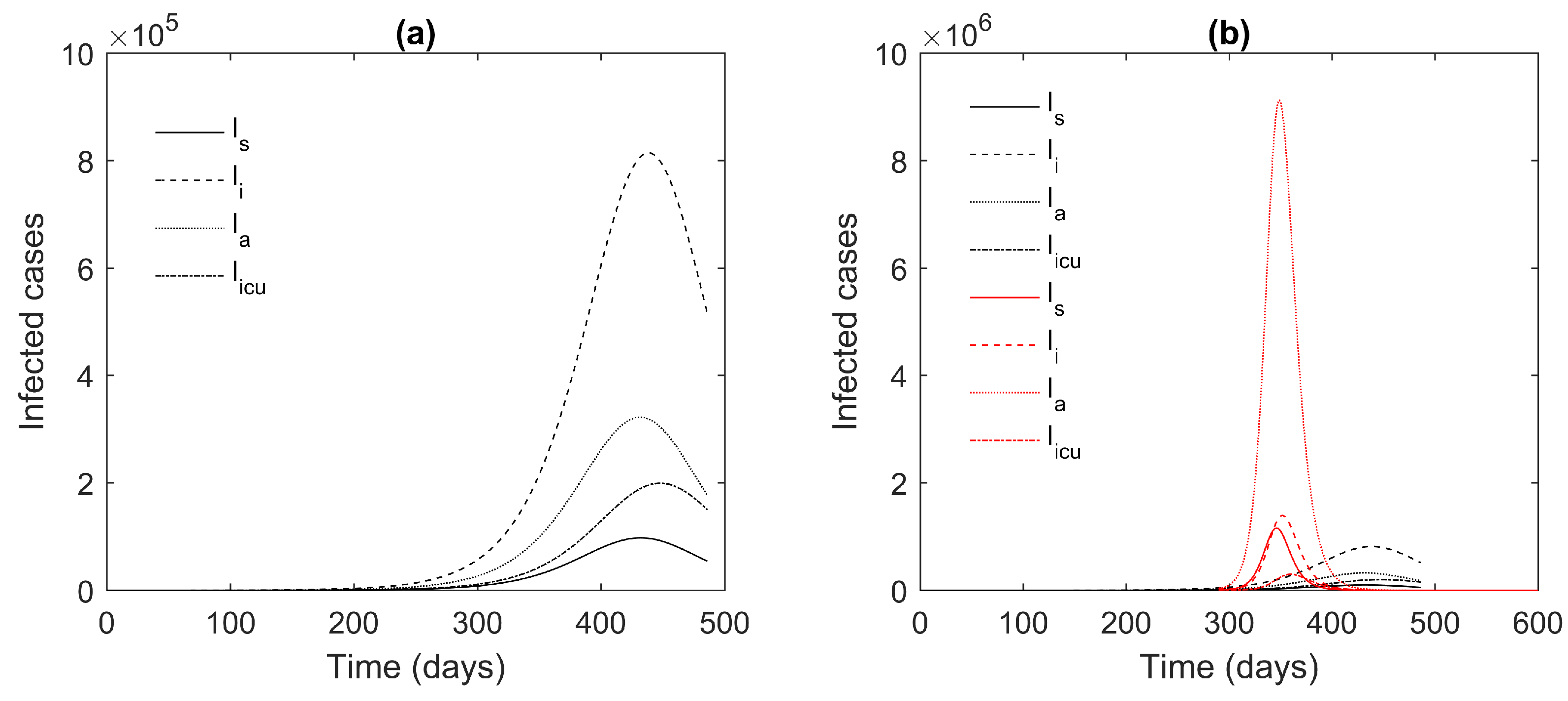
4.3. The Effectiveness of the Social Isolation Policy in Reducing COVID-19 Pandemic Transmission
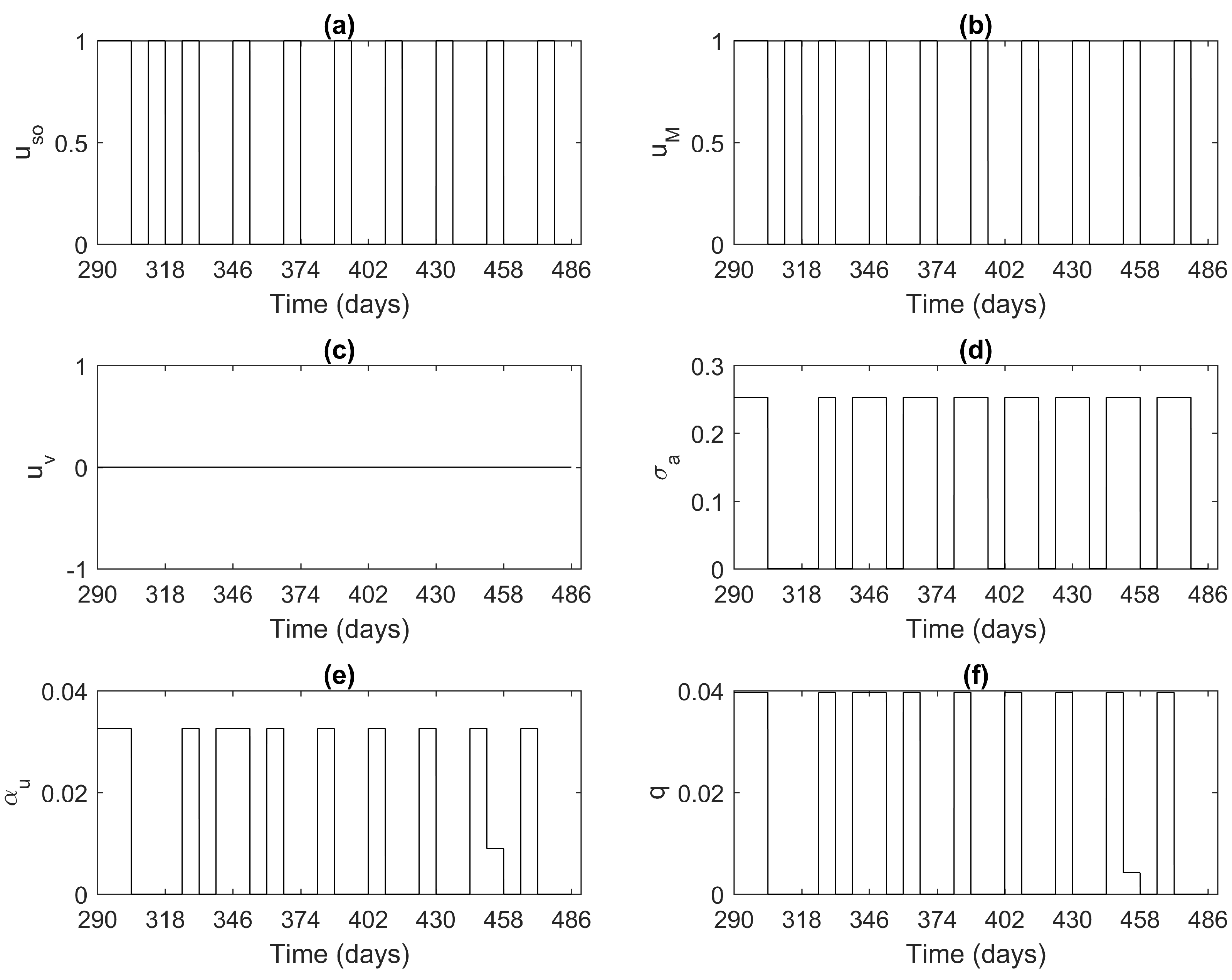
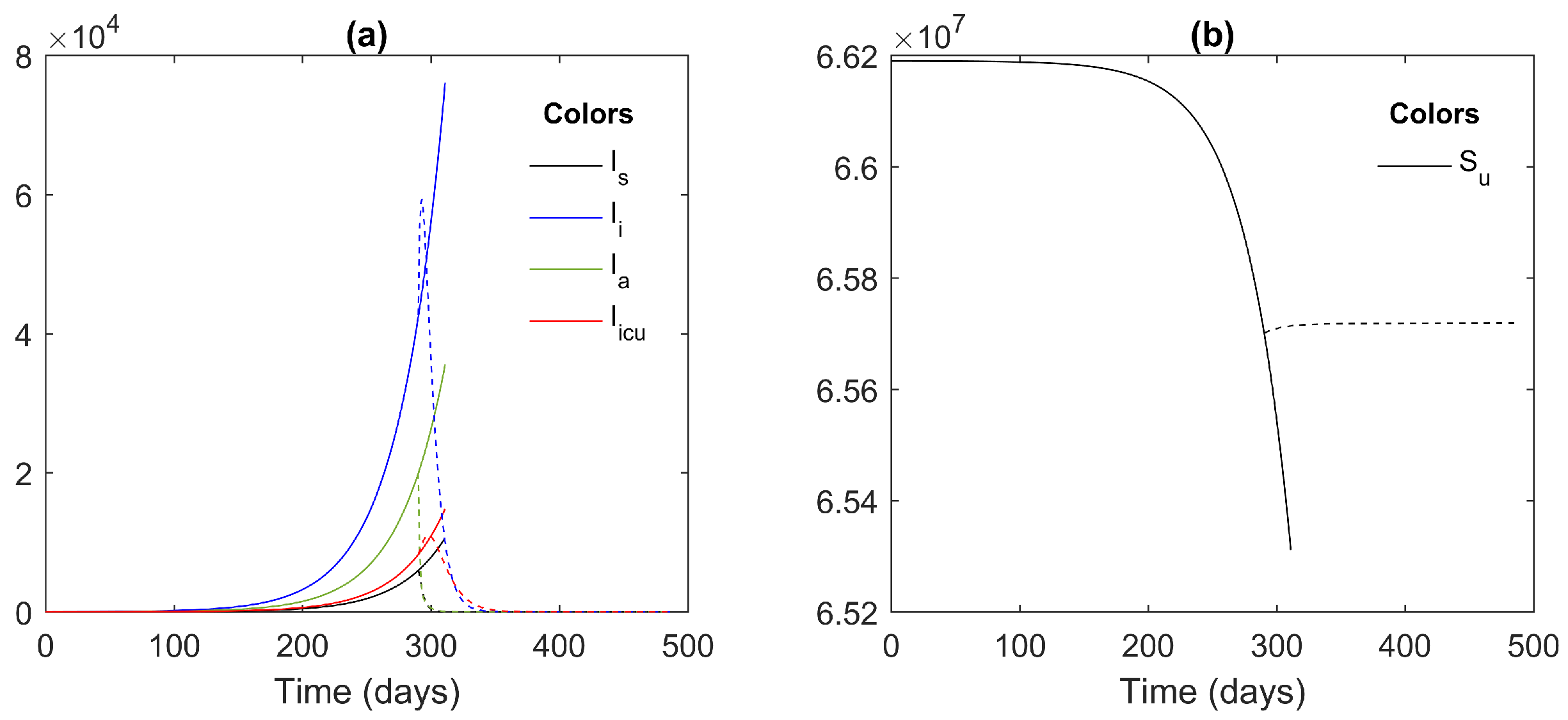
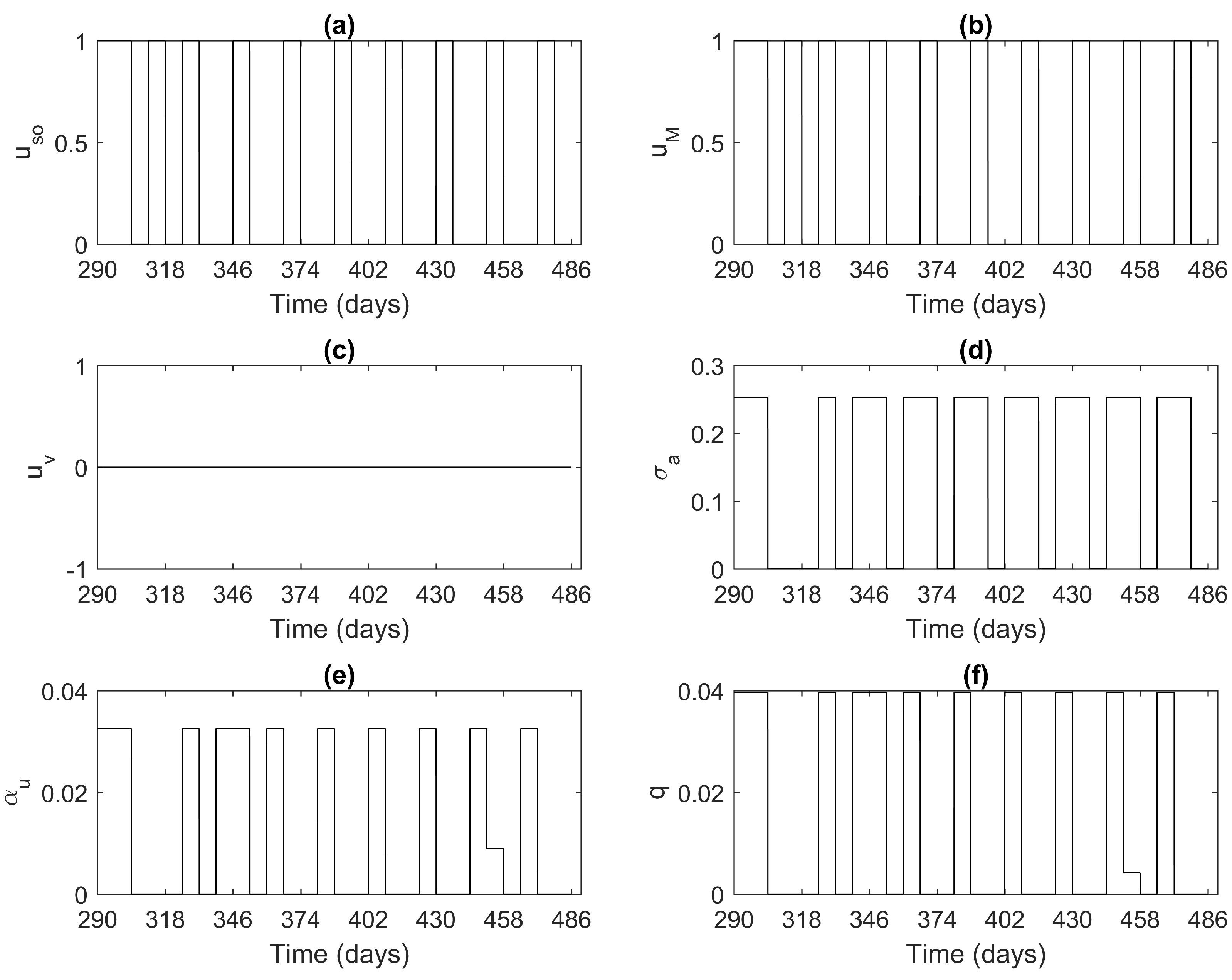
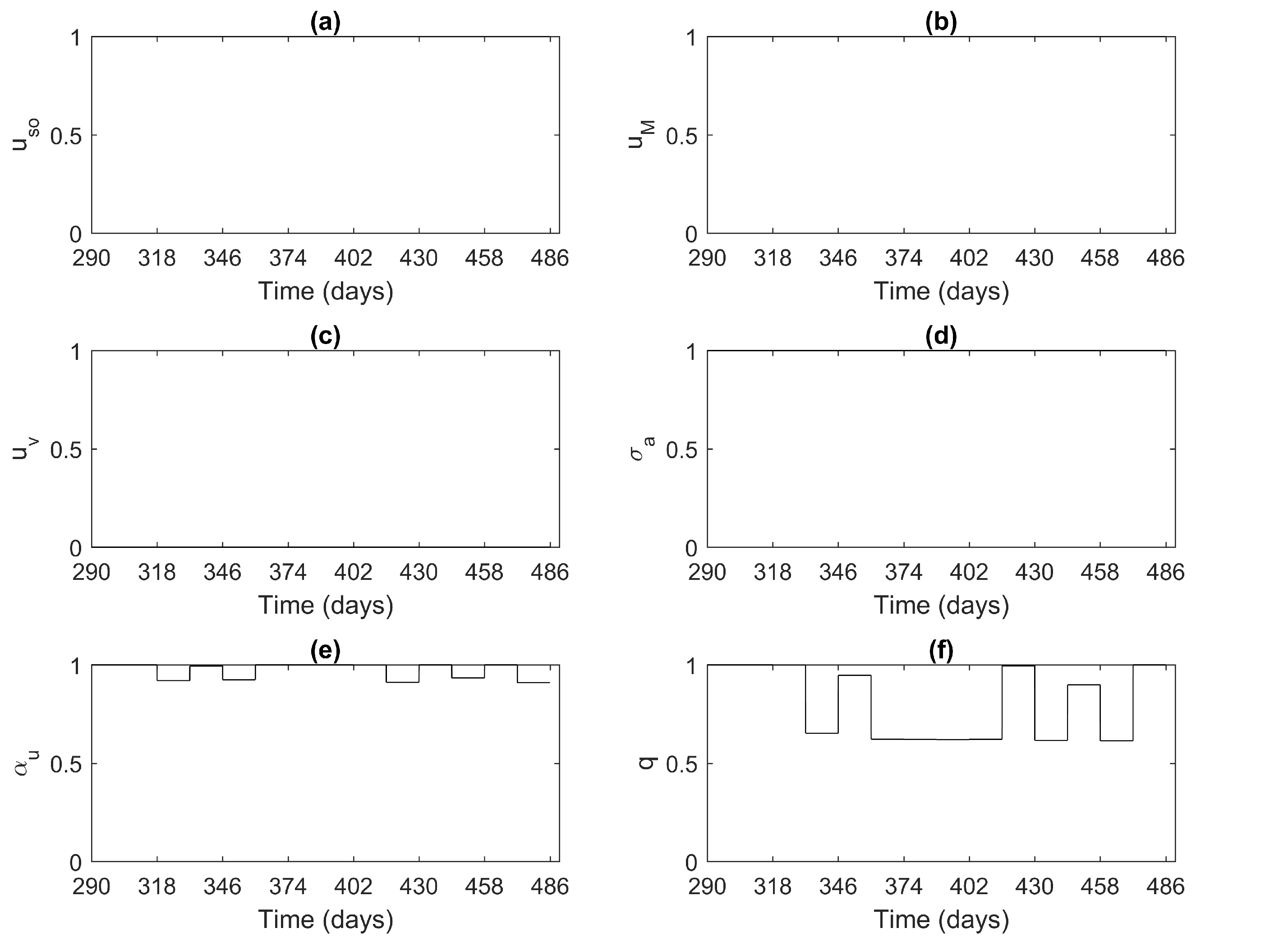
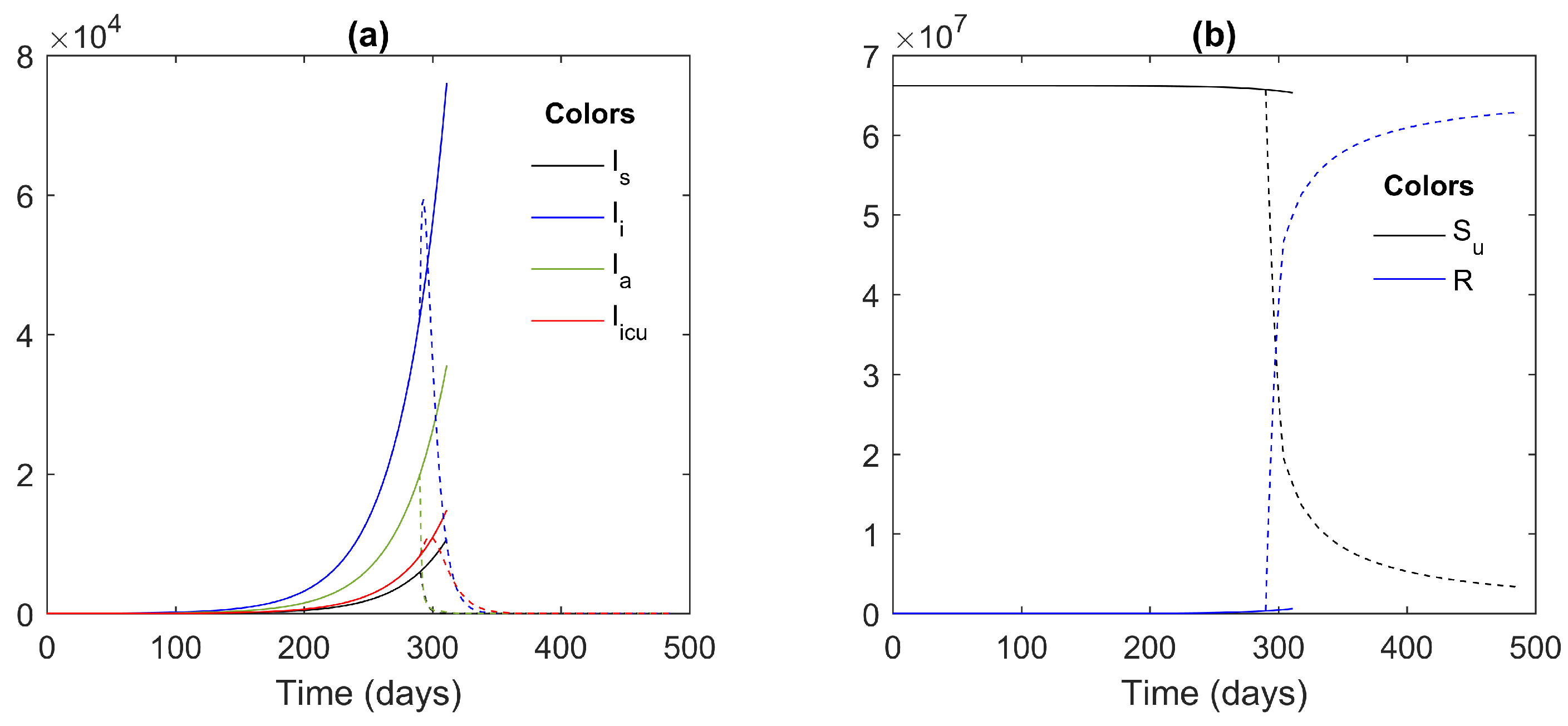
4.4. The Effectiveness of Social Isolation and Vaccination to Control the COVID-19 Pandemic
5. Discussion and Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, L.; Tuech, J.J. Is the use of laparoscopy in a COVID-19 epidemic free of risk? Br. J. Surg. 2020, 107, e188. [Google Scholar] [CrossRef]
- He, X.; Cheng, X.; Feng, X.; Wan, H.; Chen, S.; Xiong, M. Clinical symptom differences between mild and severe COVID-19 patients in China: A meta-analysis. Front. Public Health 2021, 8, 954. [Google Scholar] [CrossRef] [PubMed]
- Ngonghala, C.N.; Iboi, E.; Eikenberry, S.; Scotch, M.; MacIntyre, C.R.; Bonds, M.H.; Gumel, A.B. Mathematical assessment of the impact of non-pharmaceutical interventions on curtailing the 2019 novel Coronavirus. Math. Biosci. 2020, 325, 108364. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Disease (COVID-19): How Is It Transmitted? Available online: https://www.who.int/news-room/q-a-detail/coronavirus-disease-COVID-19-how-is-it-transmitted (accessed on 14 June 2021).
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.; Lau, E.H.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 13 June 2021).
- COVID-19 Situation Update Worldwide, as of Week 21, Updated 10 June 2021. Available online: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed on 13 June 2021).
- Wu, C.P.; Adhi, F.; Culver, D. Vaccination for COVID-19: Is it important and what should you know about it? Clevel. Clin. J. Med. 2021. [Google Scholar] [CrossRef]
- Kaplan, R.M.; Milstein, A. Influence of a COVID-19 vaccine’s effectiveness and safety profile on vaccination acceptance. Proc. Natl. Acad. Sci. USA 2021, 118. [Google Scholar] [CrossRef]
- Department of Disease Control. COVID-19 Infected Situation Reports. Available online: https://ddc.moph.go.th/viralpneumonia/eng/index.php (accessed on 11 May 2021).
- Coronavirus Disease 2019 (COVID-19) WHO Thailand Situation Report 197-19 August 2021 [EN/TH]-Thailand. Available online: https://reliefweb.int/report/thailand/coronavirus-disease-2019-COVID-19-who-thailand-situation-report-197-19-august-2021 (accessed on 30 August 2021).
- COVID-19 Pandemic in Thailand. Available online: https://en.wikipedia.org/w/index.php?title=COVID-19_pandemic_in_Thailand&oldid=1028455901 (accessed on 14 June 2021).
- Hussain, T.; Ozair, M.; Okosun, K.O.; Ishfaq, M.; Awan, A.U.; Aslam, A. Dynamics of swine influenza model with optimal control. Adv. Differ. Equ. 2019, 2019, 508. [Google Scholar] [CrossRef]
- Dénes, A.; Gumel, A.B. Modeling the impact of quarantine during an outbreak of Ebola virus disease. Infect. Dis. Model. 2019, 4, 12–27. [Google Scholar] [CrossRef]
- Chancharoenthana, W.; Leelahavanichkul, A.; Chinpraditsuk, S.; Pongpirul, K.; Kamolratanakul, S.; Phumratanaprapin, W.; Wilairatana, P.; Pitisuttithum, P. Social restriction versus herd immunity policies in the early phase of the SARS-CoV-2 pandemic: A mathematical modelling study. Asian Pac. J. Allergy Immunol. 2021. [Google Scholar] [CrossRef]
- Wilasang, C.; Jitsuk, N.; Sararat, C.; Modchang, C. Reconstruction of the transmission dynamics of the first COVID-19 epidemic wave in Thailand. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Frank, T.; Chiangga, S. SEIR order parameters and eigenvectors of the three stages of completed COVID-19 epidemics: With an illustration for Thailand January to May 2020. Phys. Biol. 2021, 18, 046002. [Google Scholar] [CrossRef] [PubMed]
- IHME COVID-19 Forecasting Team. Modeling COVID-19 Scenarios for the United States; Nature Publishing Group: Berlin, Germany, 2021; Volume 27, p. 94. [Google Scholar]
- Bastos, S.B.; Cajueiro, D.O. Modeling and forecasting the early evolution of the COVID-19 pandemic in Brazil. Sci. Rep. 2020, 10, 19457. [Google Scholar] [CrossRef]
- Iboi, E.; Richardson, A.; Ruffin, R.; Ingram, D.; Clark, J.; Hawkins, J.; McKinney, M.; Horne, N.; Ponder, R.; Denton, Z.; et al. Impact of public health education program on the novel coronavirus outbreak in the United States. Front. Public Health 2021, 9, 208. [Google Scholar] [CrossRef]
- Riyapan, P.; Shuaib, S.E.; Intarasit, A. A Mathematical Model of COVID-19 Pandemic: A Case Study of Bangkok, Thailand. Comput. Math. Methods Med. 2021, 2021, 6664483. [Google Scholar] [CrossRef]
- Akindeinde, S.O.; Okyere, E.; Adewumi, A.O.; Lebelo, R.S.; Fabelurin, O.O.; Moore, S.E. Caputo fractional-order SEIRP model for COVID-19 Pandemic. Alex. Eng. J. 2021, 61, 829–845. [Google Scholar] [CrossRef]
- Iyiola, O.; Oduro, B.; Zabilowicz, T.; Iyiola, B.; Kenes, D. System of Time Fractional Models for COVID-19: Modeling, Analysis and Solutions. Symmetry 2021, 13, 787. [Google Scholar] [CrossRef]
- Owusu-Mensah, I.; Akinyemi, L.; Oduro, B.; Iyiola, O.S. A fractional order approach to modeling and simulations of the novel COVID-19. Adv. Differ. Equ. 2020, 2020, 683. [Google Scholar] [CrossRef]
- Ndaïrou, F.; Area, I.; Nieto, J.J.; Torres, D.F. Mathematical modeling of COVID-19 transmission dynamics with a case study of Wuhan. Chaos Solitons Fractals 2020, 135, 109846. [Google Scholar] [CrossRef]
- Giordano, G.; Blanchini, F.; Bruno, R.; Colaneri, P.; Di Filippo, A.; Di Matteo, A.; Colaneri, M. A SIDARTHE model of COVID-19 epidemic in Italy. arXiv 2020, arXiv:2003.09861. [Google Scholar]
- Mahikul, W.; Chotsiri, P.; Ploddi, K.; Pan-Ngum, W. Evaluating the Impact of Intervention Strategies on the First Wave and Predicting the Second Wave of COVID-19 in Thailand: A Mathematical Modeling Study. Biology 2021, 10, 80. [Google Scholar] [CrossRef] [PubMed]
- Tantrakarnapa, K.; Bhopdhornangkul, B. Challenging the spread of COVID-19 in Thailand. ONE Health 2020, 11, 100173. [Google Scholar] [CrossRef] [PubMed]
- Giannari, A.G.; van Logtestijn, M.D.; Christodoulides, P.; Konishi, K.; Tanakal, R.J. Model predictive control for designing proactive therapy of atopic dermatitis. In Proceedings of the 2018 European Control Conference (ECC), Limassol, Cyprus, 12–15 June 2018; pp. 2387–2392. [Google Scholar]
- Wang, L. Model Predictive Control System Design and Implementation Using MATLAB®; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Maciejowski, J.M. Predictive Control: With Constraints; Pearson Education: London, UK, 2002. [Google Scholar]
- Yang, H.M. The basic reproduction number obtained from Jacobian and next generation matrices—A case study of dengue transmission modelling. Biosystems 2014, 126, 52–75. [Google Scholar] [CrossRef]
- Roberts, M.G.; Heesterbeek, J. Characterizing the next-generation matrix and basic reproduction number in ecological epidemiology. J. Math. Biol. 2013, 66, 1045–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, P.; Srivastava, S.K.; Arora, U. Stability of SEIR model of infectious diseases with human immunity. Glob. J. Pure Appl. Math. 2017, 13, 1811–1819. [Google Scholar]
- Tailor, M.R.; Bhathawala, P. Linearization of nonlinear differential equation by Taylor’s series expansion and use of Jacobian linearization process. Int. J. Theor. Appl. Sci. 2011, 4, 36–38. [Google Scholar]
- Bernal, J.L.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- BOI: The Board of Investment of Thailand. Available online: https://www.boi.go.th/ (accessed on 5 June 2021).
- Yokubol, B. Survey on Usage of Personal Protective Equipment in Known or Suspected COVID-19 Infected Patients during Anesthesia Practice in Early Pandemic 2020 in Thailand. Thai J. Anesthesiol. 2020, 46, 29–34. [Google Scholar]
- H Focus New. 80% of COVID-19 Cases Showing a Few Symptoms and 30% of These Groups Are Immune but Have No Symptoms. Available online: https://www.hfocus.org/content/2020/04/18886 (accessed on 11 May 2021).
- BANGKOKBIZ. Number of Intensive Care Unit (ICU) Beds. Available online: https://www.bangkokbiznews.com/news/detail/915139 (accessed on 11 May 2021).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | Source | Parameter | Value | Source |
|---|---|---|---|---|---|
| 0.9519 | Fitted [11] | 1/10 | [4] | ||
| p | 0.8891 | Fitted [11] | 1/8 | [4] | |
| 0.2533 | Fitted [11] | 0.13978 | [4] | ||
| 0.0326 | Fitted [11] | 1/10 | [4] | ||
| q | 0.0397 | Fitted [11] | 0.00011 | Fitted [11] | |
| 0.75 | [37] | 0.00011 | Fitted [11] | ||
| 0.000023 | [38] | 0.5 | [4] | ||
| N | 66,190,000 | [38] | 1.5 | [4] | |
| 1/5 | [4] | ||||
| 1/14 | [4] | 0.7 | [4] | ||
| 1/5.2 | [17] | 0.025 | [39] | ||
| 1/5.2 | [17] | 0.5 | [4] | ||
| 0.2 | [40] | 1.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jankhonkhan, J.; Sawangtong, W. Model Predictive Control of COVID-19 Pandemic with Social Isolation and Vaccination Policies in Thailand. Axioms 2021, 10, 274. https://doi.org/10.3390/axioms10040274
Jankhonkhan J, Sawangtong W. Model Predictive Control of COVID-19 Pandemic with Social Isolation and Vaccination Policies in Thailand. Axioms. 2021; 10(4):274. https://doi.org/10.3390/axioms10040274
Chicago/Turabian StyleJankhonkhan, Jatuphorn, and Wannika Sawangtong. 2021. "Model Predictive Control of COVID-19 Pandemic with Social Isolation and Vaccination Policies in Thailand" Axioms 10, no. 4: 274. https://doi.org/10.3390/axioms10040274
APA StyleJankhonkhan, J., & Sawangtong, W. (2021). Model Predictive Control of COVID-19 Pandemic with Social Isolation and Vaccination Policies in Thailand. Axioms, 10(4), 274. https://doi.org/10.3390/axioms10040274