
How to Seek a Site for Forest Health Care Development—A Case Study in Hainan Tropical Rainforest National Park, China


Abstract
1. Introduction
2. Materials and Methods
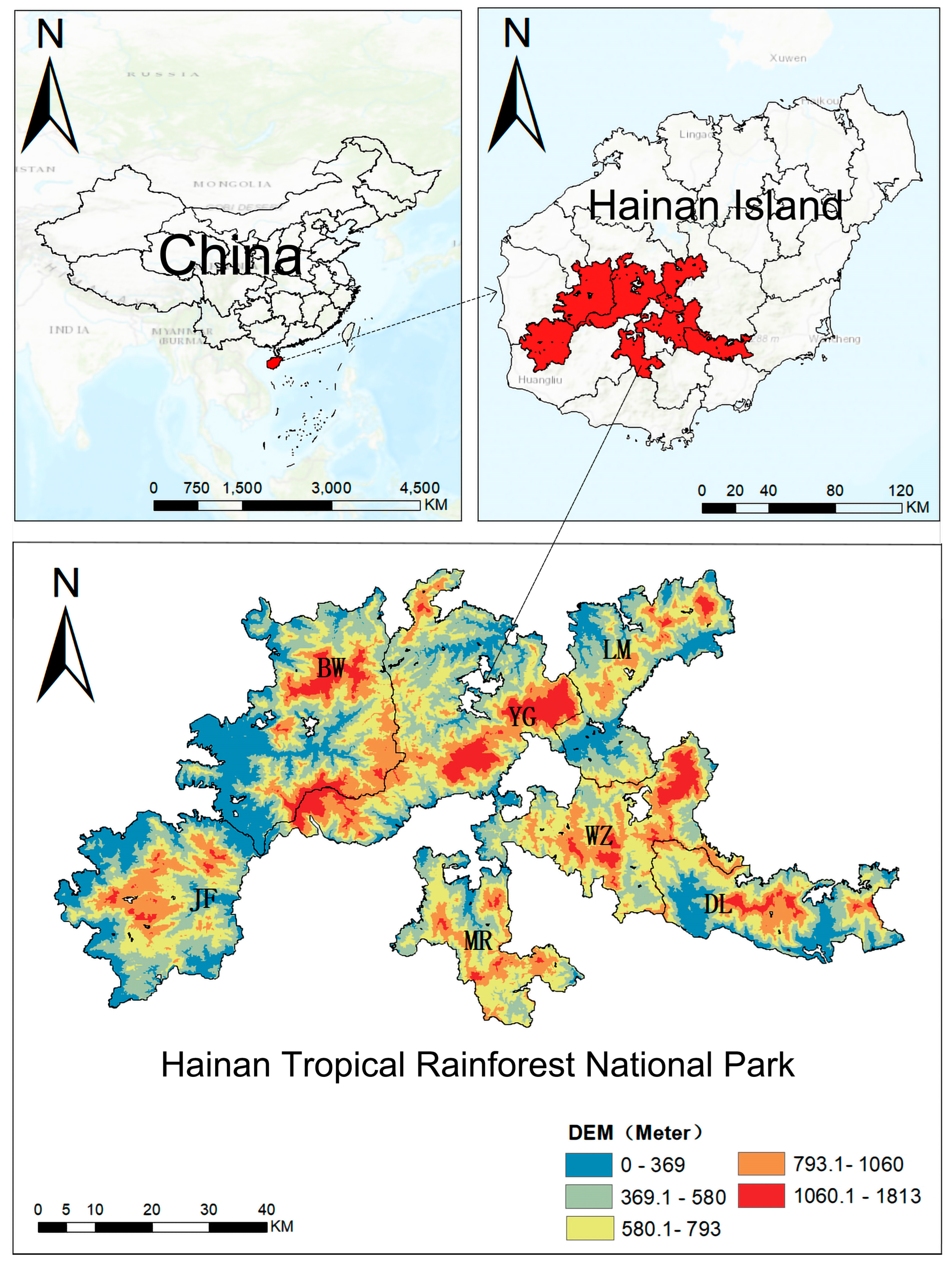
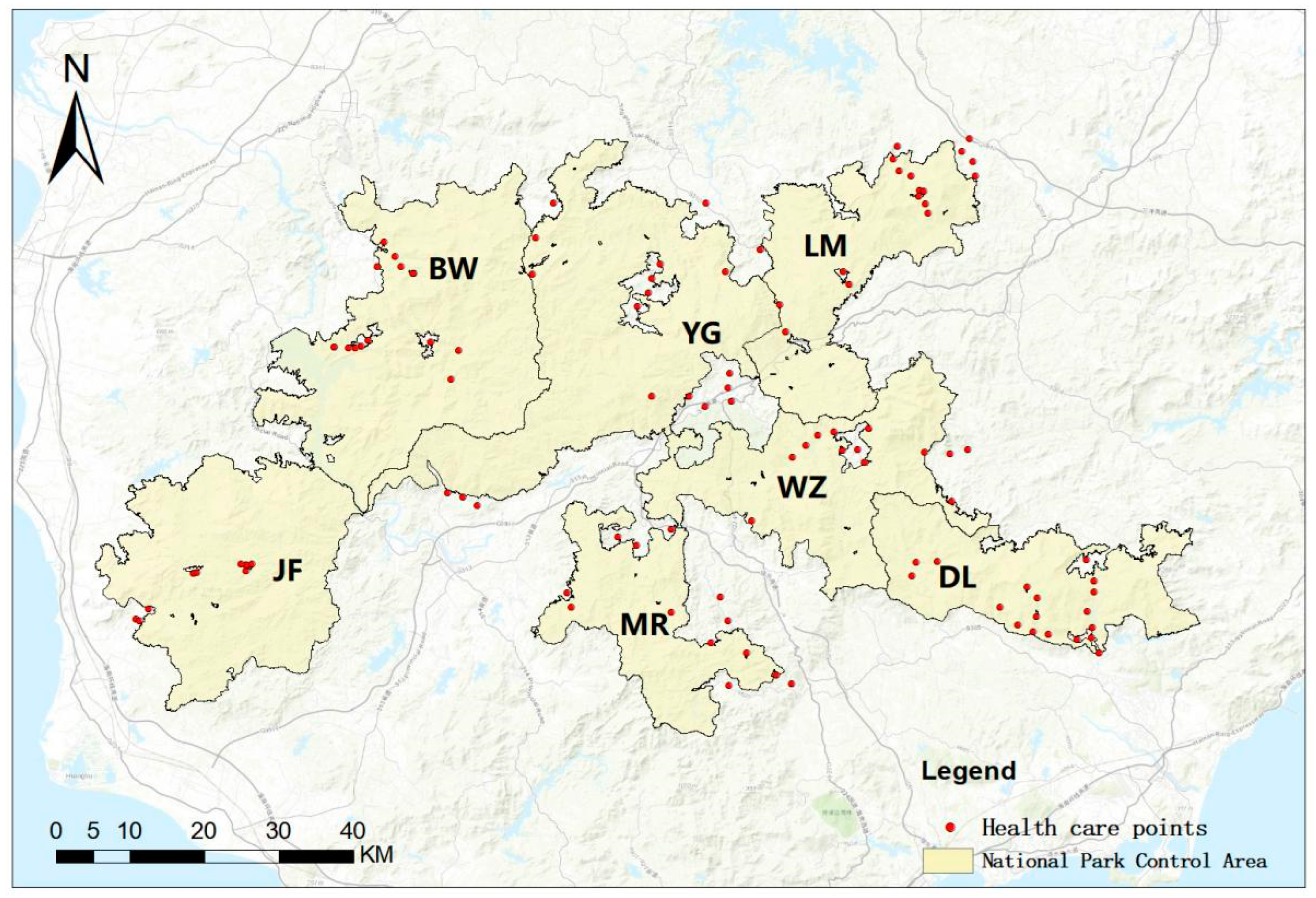
2.1. Study Area
2.2. Data Sources
2.3. Research Methods and Data Analysis
2.3.1. Indicator Selection and Scoring
2.3.2. Data Normalization and Weight Assignment
2.3.3. Construction of Health Care Evaluation System
2.3.4. Multi-Factor Superposition Analysis
3. Results
3.1. Evaluation Results of Health Care Points
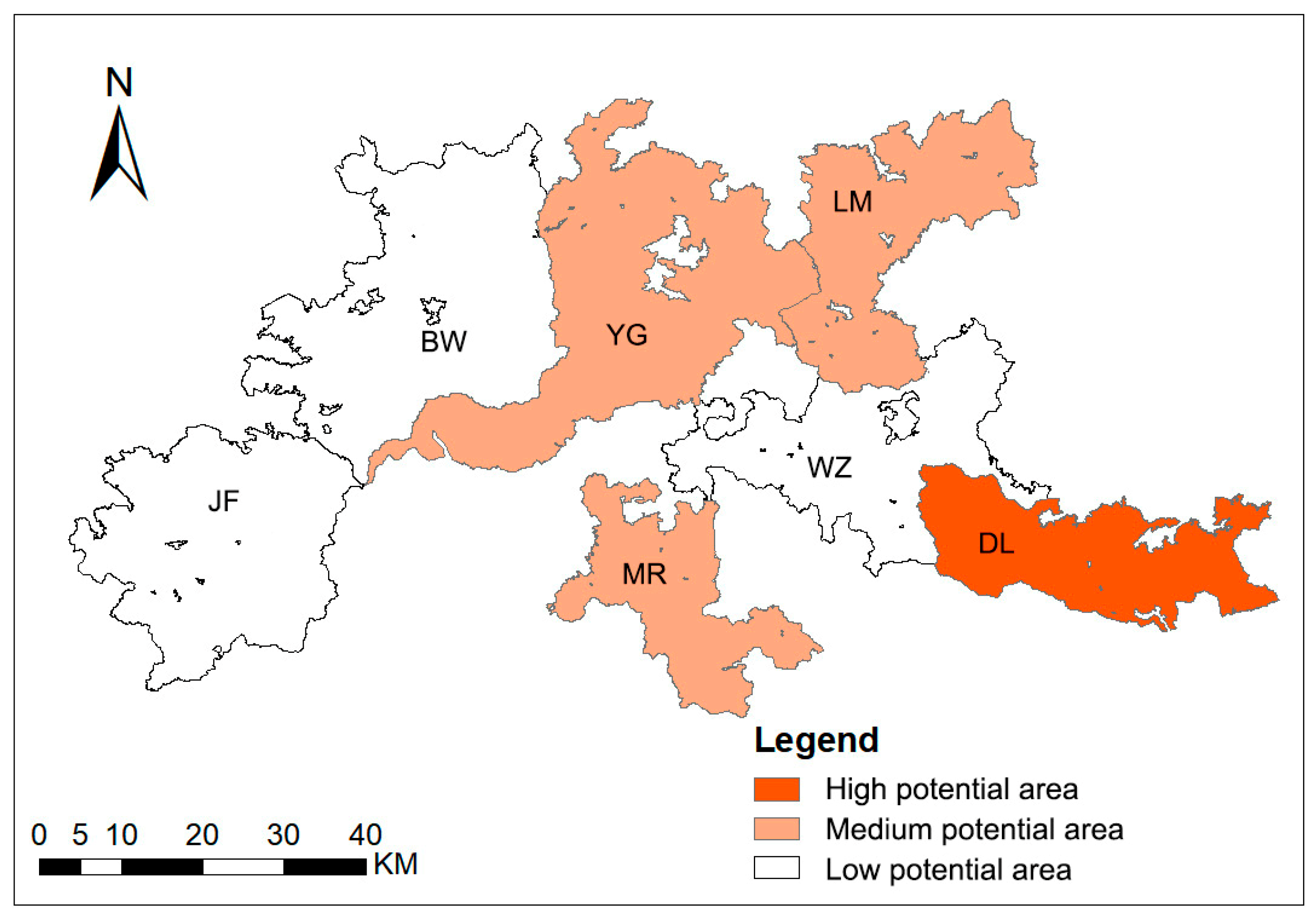
3.2. Results of Overlay Analysis
4. Discussion
4.1. Results Analysis
4.2. Significance and Suggestions
4.3. Limitations and Prospects
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Deng, S.L. Theoretic Research and Practices of Forest Health. World For. Res. 2016, 29, 1–6. [Google Scholar] [CrossRef]
- Guo, S.Y.; Wang, Y.Y.; Chen, X.G.; Wang, Y.; Jin, T.W. Research Progress in Forest Therapy and Forest Established for Healthcare. World For. Res. 2022, 35, 28–33. [Google Scholar] [CrossRef]
- Xu, G.F.; Yu, Y.W.; Xu, M.L.; Zhang, W.F. What is forest health regimen? Thinking on the integration between forest multi-function and related business models. For. Econ. 2018, 40, 58–60. [Google Scholar] [CrossRef]
- Liu, Q. Necessity, feasibility and path selection of development of forest health industry. China Econ. 2021, 2, 36–39. [Google Scholar]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef]
- Rajoo, K.S.; Karam, D.S.; Abdullah, M.Z. The physiological and psychosocial effects of forest therapy, A systematic review. Urban For. Urban Green. 2020, 54, 126744. [Google Scholar] [CrossRef]
- Zhou, Q.; Wang, J.; Wu, Q.; Chen, Z.; Wang, G. Seasonal dynamics of VOCs released from Cinnamomun camphora forests and the associated adjuvant therapy for geriatric hypertension. Ind. Crops Prod. 2021, 174, 114131. [Google Scholar] [CrossRef]
- Qin, F.K.; Liu, L.G.; Deng, T.; Chen, H.; Li, J. Investigation on Effects of Short-term Forest Health Rehabilitation on Lung Function of the Middle-aged and Elderly. Prev. Med. Inf. 2019, 35, 1172–1177. [Google Scholar]
- Quan, W.; Yu, S.; Huang, Q.; Ying, M. The effect of forest-based health and wellness on the stress-relieve of middle-aged people. Front. Public Health 2024, 12, 1366339. [Google Scholar] [CrossRef]
- Fan, X. Policy evolution and enlightenment of Japan’s forest healthcare industry. EDP Sci. 2024, 395, 01079. [Google Scholar] [CrossRef]
- Han, J.-W.; Choi, H.; Jeon, Y.-H.; Yoon, C.-H.; Woo, J.-M.; Kim, W. The effects of forest therapy on coping with chronic widespread pain, Physiological and psychological differences between participants in a forest therapy program and a control group. Int. J. Environ. Res. Public Health 2016, 13, 255. [Google Scholar] [CrossRef]
- Im, S.G.; Choi, H.; Jeon, Y.-H.; Song, M.-K.; Kim, W.; Woo, J.-M. Comparison of effect of two-hour exposure to forest and urban environments on cytokine, anti-oxidant, and stress levels in young adults. Int. J. Environ. Res. Public Health 2016, 13, 625. [Google Scholar] [CrossRef] [PubMed]
- Anundi, H.; Dolling, A.; Palsdottir, A.M. Forest Therapy for Women with Gynaecological Cancer—A Feasibility Study to Find New Alternatives in Cancer Rehabilitation. Forests 2023, 14, 333. [Google Scholar] [CrossRef]
- Lee, M.M.; Park, B.J. Effects of forest healing program on depression, stress and cortisol changes of cancer patients. J. People Plants Environ. 2020, 23, 245–254. [Google Scholar] [CrossRef]
- Muro, A.; Feliu-Soler, A.; Canals, J.; Parrado, E.; Sanz, A. Psychological benefits of Forest Bathing during the COVID-19 pandemic, A pilot study in a Mediterranean forest close to urban areas. J. For. Res. 2022, 27, 71–75. [Google Scholar] [CrossRef]
- He, S.X.; Kong, B.; Wan, Y. The Research Progress of Forest Bathing at Home and Abroad. Shaanxi For. Sci. Technol. 2024, 52, 94–104. [Google Scholar]
- Li, Q.; Kawada, T. Effect of forest therapy on the human psycho-neuro-endocrino-immune network. Nihon Eiseigaku Zasshi Jpn. J. Hyg. 2011, 66, c645–c650. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Nie, X. Investigation and analysis of the influence of forest bath on sleep quality of military pilots during convalescence. Chin. J. Conval. Med. 2014, 23, 75–76. [Google Scholar] [CrossRef]
- Pan, Y.L.; Zeng, J.; Liu, Y.Q.; Wen, Y.; Yan, Q.; Gu, X.R. Research on the evaluation of different forest recuperation types. Issues For. Econ. 2018, 38, 83–88. [Google Scholar] [CrossRef]
- Zhang, Z.Q. Study on the Forest Therapy Base Planning and Design Based on Therapy Factors. Master’s Thesis, Hunan University of Technology, Zhuzhou, China, 2018. [Google Scholar]
- Li, J.R.; Xu, D. Evaluation on exploitation potential of forest health tourism based on AHP and fuzzy synthetic evaluation, a case study of Liaodong Mountain area. Chin. J. Agric. Resour. Reg. Plan. 2018, 39, 135–142. [Google Scholar]
- Li, J.R.; Xu, D. Study on the construction of forest health tourism evaluation index system. For. Econ. 2018, 40, 28–34. [Google Scholar] [CrossRef]
- Liu, Z.; Wang, P. The forest health care re-search progress at home and abroad. Hubei For. Sci. Technol. 2017, 46, 53–58. [Google Scholar]
- Li, D. The Master Plan of Hunan Huayanxi National Park Based on Forest Health Care Theory. Master’s Thesis, Central South University of Forestry Technology, Changsha, China, 2018. [Google Scholar]
- Zhang, H.Q.; Zhai, X.J.; He, D. Research on innovative development of forest based health and wellness industry based on industrial integration, taking Heilongjiang Province as an example. For. Econ. 2019, 41, 56–61. [Google Scholar] [CrossRef]
- Cong, L.; Zhang, Y.J. Thoughts on scientific research of forest health tourism. Tour. Trib. 2016, 31, 6–8. [Google Scholar]
- Ling, H.J.; Zhang, Y.F.; Shao, J.M.; Ding, M.H.; Yu, J. Spatial Distribution Characteristics and Influencing Factors of Forest Health Resources in Jiangxi Province. Jiangxi Sci. 2024, 42, 85–92. [Google Scholar] [CrossRef]
- Yu, P.; Zhang, C.S.; Chen, Y.; Li, B.; Ma, J.J.; Guan, X.C.; Wang, K. Research Progress on The Effects of Environmental Factors on Red Claw Crayfish. FSTInfo 2024, 51, 125–132. [Google Scholar]
- Lin, S.L.; Zhou, X.J.; Xing, A.; Jiang, H.X.; Yao, D.D.; Qin, J.; Feng, Z.Y.; Guo, C.; Wang, Y. Relationship between rodent community structure and environmental factors in the southern part of the northeast agro-pastoral ecotone. Plant Prot. 2024, 50, 126–134. [Google Scholar]
- Tang, S.Q. Study on the relationship between ground cover plant community succession and environmental factors in Tongling Wetland Park. Mod. Gard. 2024, 47, 33–37. [Google Scholar] [CrossRef]
- Qian, N.P.; Gao, H.X.; Song, C.J.; Dong, C.C.; Liu, Q.J. Seasonal dynamics of radial growth of Betula platyphylla and its response to environmental factors in Changbai Mountain. Chin. J. Plant Ecol. 2024, 48, 1001–1010. [Google Scholar] [CrossRef]
- Tomar, S.; Thakur, S.; Thapliyal, N.; Kanwal, K.S.; Bhatt, I.D.; Nautiyal, S.; Puri, S. Understanding the influence of environmental factors on forest composition along the vertical gradient of Northwestern Himalaya. Trees For. People 2024, 17, 100631. [Google Scholar] [CrossRef]
- Zhang, Z.Y.; Ye, B.; Yang, J.; He, Q.J.; Dong, J.H. Research Progress in Studies of Health Functions of Urban Forests. World For. Res. 2014, 27, 27–33. [Google Scholar] [CrossRef]
- Li, X.Y.; Li, J.J.; Kang, L.G. Evaluation of forest health care bases in Beijing-Tianjin-Hebei region based on the eight-factor model and Chengde strategy. Econ. Res. Rev. 2017, 47, 71–79. [Google Scholar] [CrossRef]
- Han, M.C.; Liang, Y.L.; Ye, B.; Yu, S.F. Research on composite evaluation index of urban forest health effects of Beigong National Forest Park. Guangdong Agric. Sci. 2012, 39, 185–188. [Google Scholar] [CrossRef]
- Lan, Y.; Wang, J.; Huang, Y.; Tang, Y.; Liu, Z.; Zheng, J.; Yao, X.; Zhu, Z.; Dong, J.; Chen, Y. The Combined Effects of the Thermal Environment and Air Quality at health care Places on the Physiology and Psychology of People in Urban Parks. Forests 2024, 15, 1640. [Google Scholar] [CrossRef]
- Sun, M.T. Research on the Evaluation of Health Care Function of Forest Parks in Alshan Region Based on Environmental Factors. Master’s Thesis, Northeast Forestry University, Harbin, China, 2023. [Google Scholar] [CrossRef]
- Liu, J.L.; Hou, J.X.; Zou, R.M.; Sun, J.; Wu, C.; Wang, R. Assessment of Forest Health Value, A Case Study in Sanming City, Fujian Province, China. Pol. J. Environ. Stud. 2022, 31, 2709–2715. [Google Scholar] [CrossRef]
- Wu, S.Y.; Deng, X.J. Evaluation of Hainan’s forest tourism resources based on analytic hierarchy process. China Trop. Agric. 2016, 12, 84–89. [Google Scholar]
- Lin, R.X.; Yan, Q.L.; Zeng, D.Q. Status Quo and Countermeasures of Forest Health Industry Development in Hainan Province. Trop. For. 2023, 51, 95–100. [Google Scholar]
- Wang, W.X.; Zhang, W.; Bai, M.M.; Lin, X.; Yang, H. Analysis on the development dilemma and optimization strategy of Hainan’s forest health care industry. West. Tour. 2023, 21, 8–10. [Google Scholar]
- Zhang, C.D.; Ma, L.B.; Yao, N.J.; Lin, X.; Yang, H. Research on the evaluation of the facilities of the forest health care base in Hainan Tropical Rainforest National Park, Taking Diaoluoshan area as an example. Trop. For. 2024, 52, 82–87. [Google Scholar]
- Wang, Q.Y.; Chen, P.F.; Li, X.D.; Feng, Y.; Song, X.Y.; Fu, L.Y. Review of forest health assessment methods. J. Nanjing For. Univ. 2018, 42, 177. [Google Scholar] [CrossRef]
- Gao, Z.L.; Yu, X.X.; Yue, Y.J.; Bian, Z.; Yang, B.Q.; Cao, B.; Qin, Y.S. Study on forest health evaluation of Songshan Nature Reserve in Beijing. J. Beijing For. Univ. 2008, 30, 127–131. [Google Scholar] [CrossRef]
- Ruan, Z.Q. Study on Forest Ecosystem Health Assessment. Master’s Thesis, South China Normal University, Guangzhou, China, 2007. [Google Scholar]
- Gan, J.; Zhu, J.G.; Zhang, G.Z.; Yu, X.X. Establishment of forest health evaluation index based on BP neural network. For. Sci. 2007, 43, 1–7. [Google Scholar]
- GB 3096-2008; Environmental Quality Standard for Noise. Standardization Administration of China: Beijing, China, 2007.
- Lu, D.H.; Cui, S.; Li, C.H. Suitability of Summer Micro Climatic Conditions for Human Beings in Urban Greening in Beijing, Proceedings of Forestry Meteorology; Meteorological Press: Beijing, China, 1984; pp. 144–152. [Google Scholar]
- GB 3838-2002; Environmental Quality Standard for Surface Water. Standardization Administration of China: Beijing, China, 2002.
- Wang, H.J. Effects of Structure of Urban Forestry on Aero-anion Concentration. J. Nanjing For. Univ. 2004, 28, 96–98. [Google Scholar]
- Li, Q.Y.; Chen, N.N.; Yu, Z.X.; Qin, H.; Qiao, X.; Yan, W. Spatial Distribution Characteristics and Driving Factors of Forest Health Care Resources in Guizhou Province. J. Nanjing For. Univ. 2023, 43, 175–182. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Source |
|---|---|
| Road, water system data | OSM, https://openmaptiles.org/ (accessed on 13 October 2023) |
| The DEM data | Geospatial Data Cloud Platform https://www.gscloud.cn/ (accessed on 20 March 2024) |
| Village sites data | China National Bureau of Statistics, https://www.stats.gov.cn/ (accessed on 15 October 2023) |
| Environmental factors data | Data from on-site monitoring |
| Grade | A | B | C | D | E1 | E2 | E3 |
|---|---|---|---|---|---|---|---|
| Air cleanliness | Cleanest | Clean | Moderately Clean | Allowed | Slightly Polluted | Moderately Polluted | Severely Polluted |
| CI | >1.00 | 1.00~0.70 | 0.69~0.50 | 0.49~0.30 | 0.29~0.20 | 0.19~0.10 | <0.10 |
| Serial Number | Health Care Point Name | Microclimate Comfort | Air Quality | Sound Pressure | Water Quality |
|---|---|---|---|---|---|
| 1 | BW01 | 5 | 5 | 5 | 3 |
| 2 | BW1703 | 4 | 5 | 5 | 5 |
| 3 | BW0301 | 4 | 4 | 5 | 4 |
| 4 | BW0302 | 4 | 5 | 5 | 4 |
| 5 | DL01 | 4 | 5 | 4 | 5 |
| 6 | DL03 | 5 | 5 | 1 | 5 |
| 7 | DL04 | 4 | 5 | 4 | 5 |
| 8 | DL06 | 4 | 5 | 3 | 5 |
| … | …… | … | … | … | … |
| 107 | MR057 | 5 | 5 | 3 | 5 |
| Indicators | Average Value | Standard Deviation | CV Coefficient | Weight (%) |
|---|---|---|---|---|
| Noise score | 0.715 | 0.309 | 0.432 | 37 |
| Surface water quality score | 0.785 | 0.255 | 0.324 | 28 |
| Air quality score | 0.986 | 0.119 | 0.12 | 11 |
| Human comfort score | 0.859 | 0.242 | 0.281 | 24 |
| Evaluation Content | Evaluation Score | Level | Evaluation Standards |
|---|---|---|---|
| Evaluation of forest health care functions | N ≥ 0.80 | I | The forest environment is very comfortable and very suitable for forest health care activities |
| 0.65 ≤ N < 0.80 | II | The forest environment is very comfortable and suitable for forest health care activities | |
| 0.50 ≤ N < 0.65 | III | The forest environment is relatively comfortable and relatively suitable for forest health care activities | |
| 0.35 ≤ N < 0.50 | IV | The forest environment is uncomfortable and not suitable for forest health care activities | |
| N < 0.35 | V | The forest environment is very uncomfortable and extremely unsuitable for forest health care activities |
| Serial Number | Health Care Point Name | F1 | F2 | F3 | F4 | N | Health Care Point Level |
|---|---|---|---|---|---|---|---|
| 1 | BW01 | 1 | 1 | 1 | 0.6 | 0.888 | Level 1 |
| 2 | BW1703 | 0.75 | 1 | 1 | 1 | 0.94 | Level 1 |
| 3 | BW0301 | 0.75 | 0.75 | 1 | 0.8 | 0.8565 | Level 1 |
| 4 | BW0302 | 0.75 | 1 | 1 | 0.8 | 0.884 | Level 1 |
| 5 | DL01 | 0.75 | 1 | 0.8 | 1 | 0.866 | Level 1 |
| 6 | DL04 | 0.75 | 1 | 0.8 | 1 | 0.866 | Level 1 |
| 7 | DL08 | 1 | 1 | 0.8 | 1 | 0.926 | Level 1 |
| 8 | DL09 | 1 | 1 | 0.8 | 1 | 0.926 | Level 1 |
| … | …… | … | … | .. | .. | … | … |
| 67 | MR057 | 1 | 1 | 0.6 | 1 | 0.852 | Level 1 |
| Number of Health Care Points | |||
|---|---|---|---|
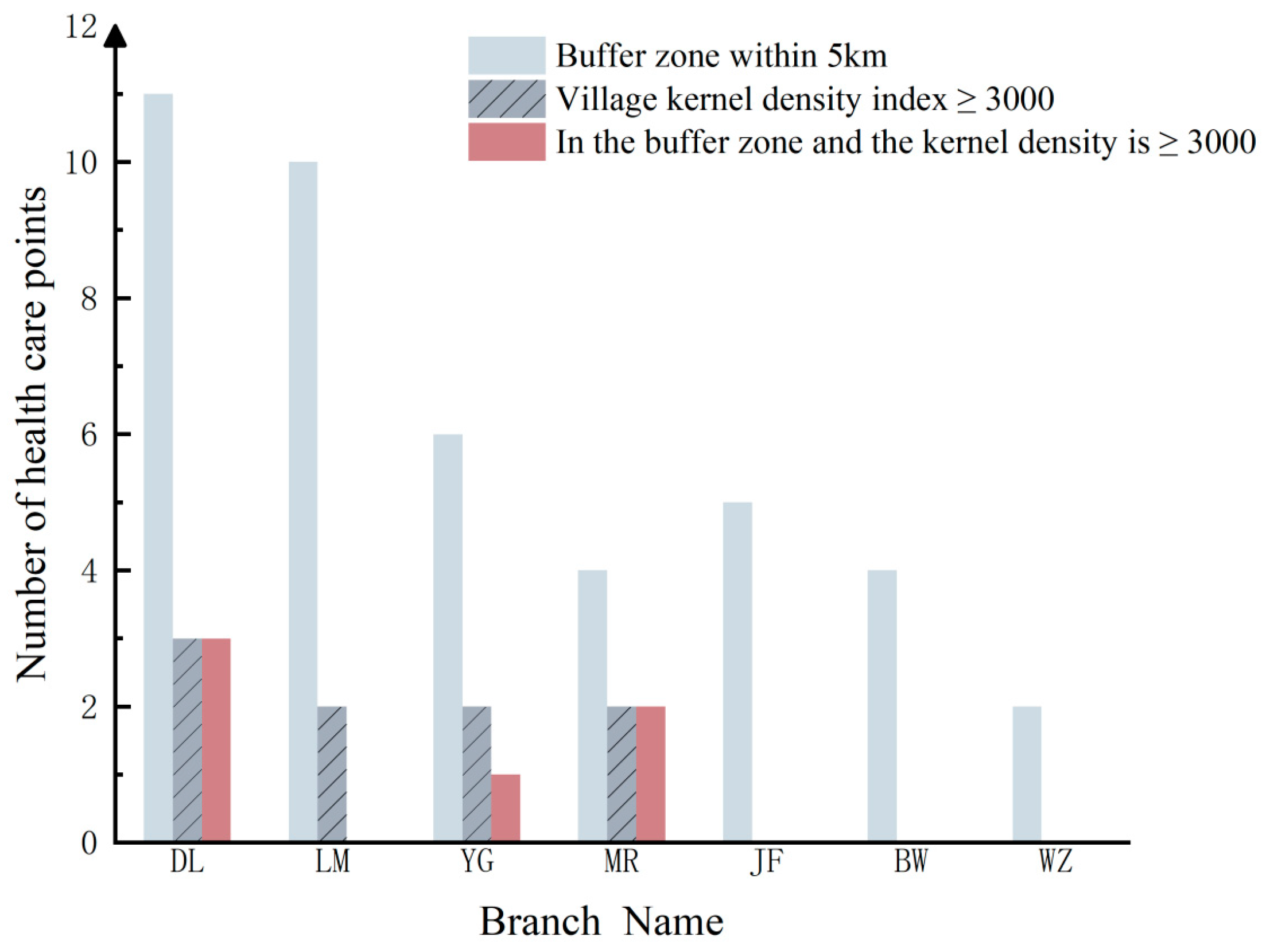
| Branch Name | Buffer Zone Within 5 km | Village Kernel Density Index ≥ 3000 | In the Buffer Zone and the Kernel Density is ≥3000 |
| JF | 5 | 0 | 0 |
| BW | 4 | 0 | 0 |
| YG | 6 | 2 | 1 |
| MR | 4 | 2 | 2 |
| WZ | 2 | 0 | 0 |
| LM | 10 | 2 | 0 |
| DL | 11 | 3 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, Z.; Chu, J.; Fu, G.; Fu, H.; Xu, T.; Li, S. How to Seek a Site for Forest Health Care Development—A Case Study in Hainan Tropical Rainforest National Park, China. Land 2025, 14, 1076. https://doi.org/10.3390/land14051076
Zheng Z, Chu J, Fu G, Fu H, Xu T, Li S. How to Seek a Site for Forest Health Care Development—A Case Study in Hainan Tropical Rainforest National Park, China. Land. 2025; 14(5):1076. https://doi.org/10.3390/land14051076
Chicago/Turabian StyleZheng, Ziqi, Jieling Chu, Guang Fu, Hui Fu, Tao Xu, and Shuling Li. 2025. "How to Seek a Site for Forest Health Care Development—A Case Study in Hainan Tropical Rainforest National Park, China" Land 14, no. 5: 1076. https://doi.org/10.3390/land14051076
APA StyleZheng, Z., Chu, J., Fu, G., Fu, H., Xu, T., & Li, S. (2025). How to Seek a Site for Forest Health Care Development—A Case Study in Hainan Tropical Rainforest National Park, China. Land, 14(5), 1076. https://doi.org/10.3390/land14051076