

Spatial-Temporal Variation in Health Impact Attributable to PM2.5 and Ozone Pollution in the Beijing Metropolitan Region of China


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Data Collection
2.3. Health Impact Assessment
3. Results and Discussion
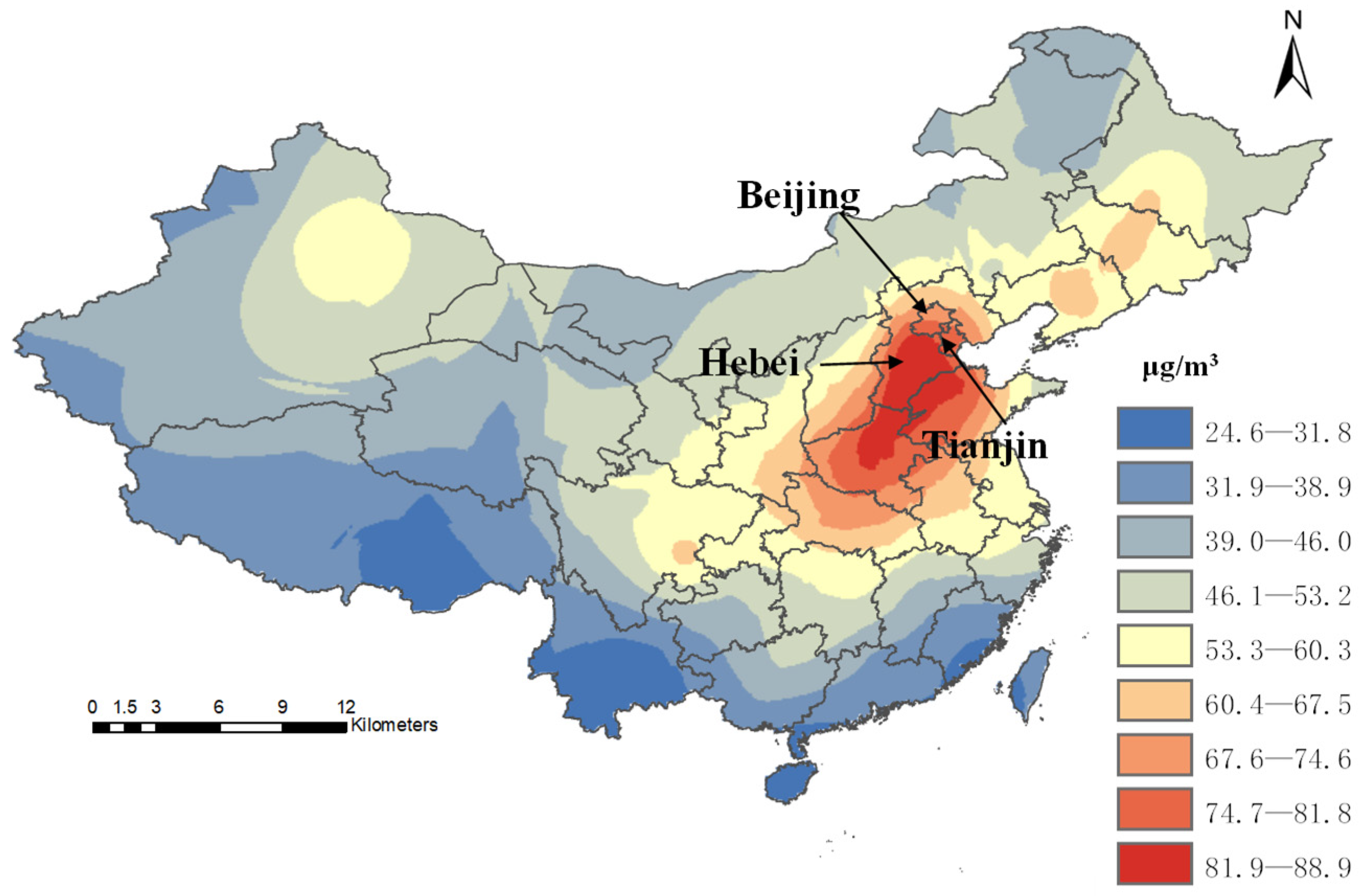
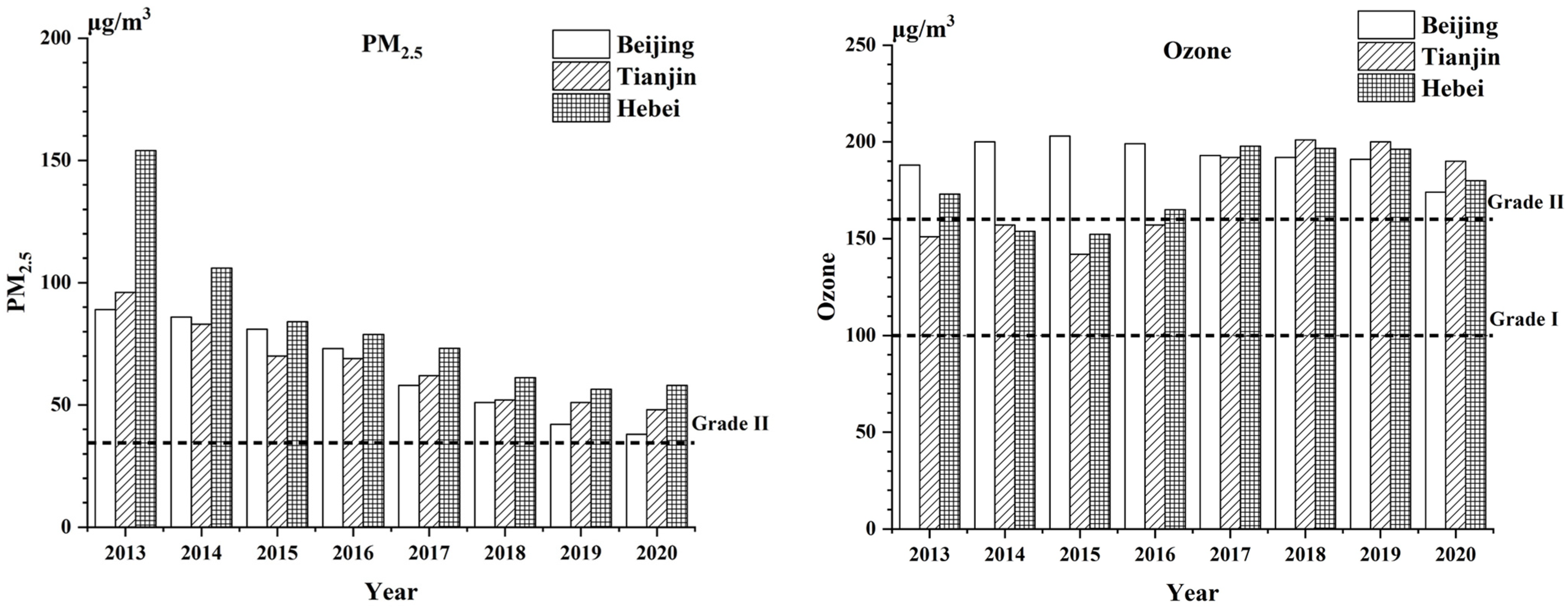
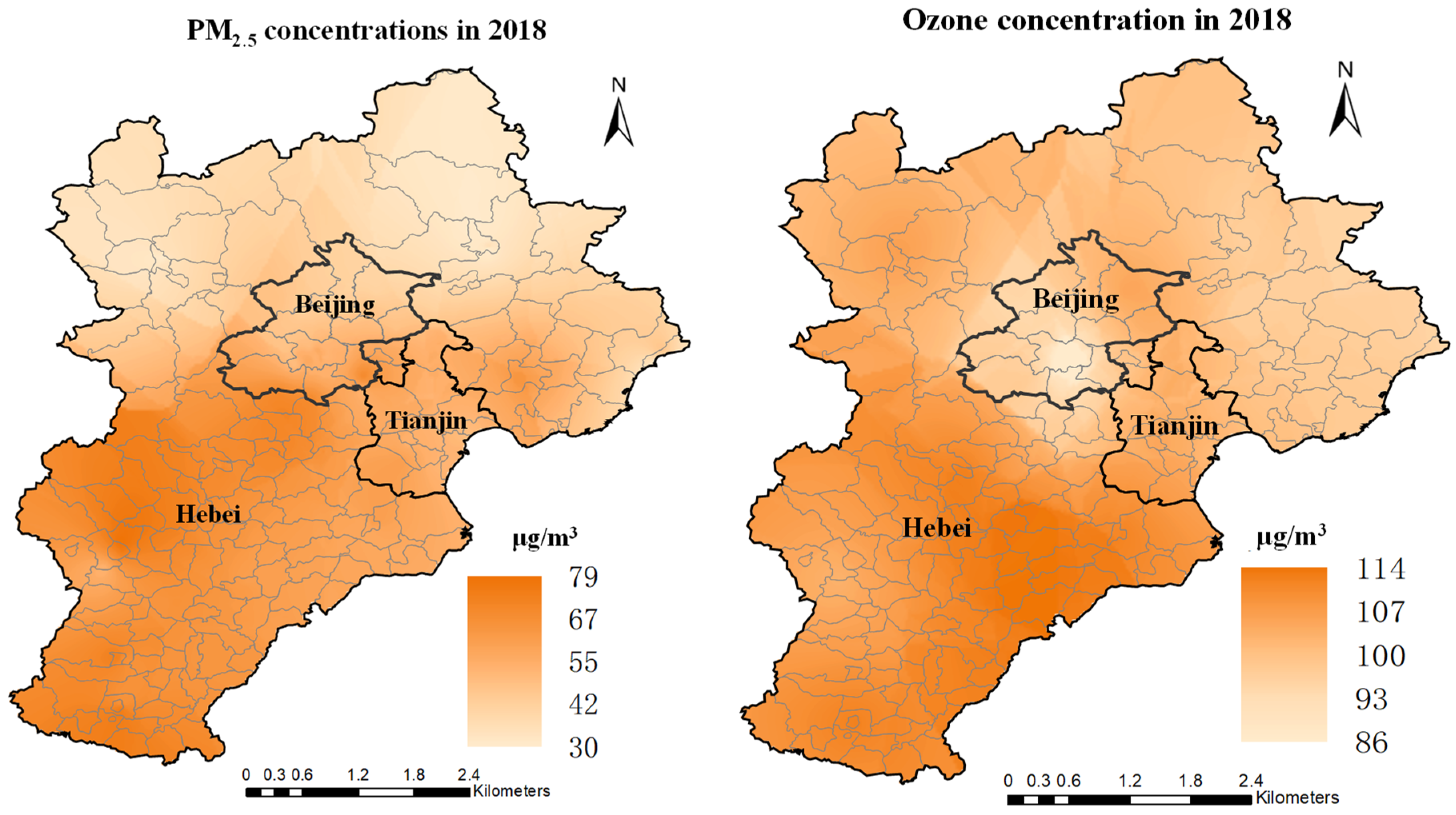
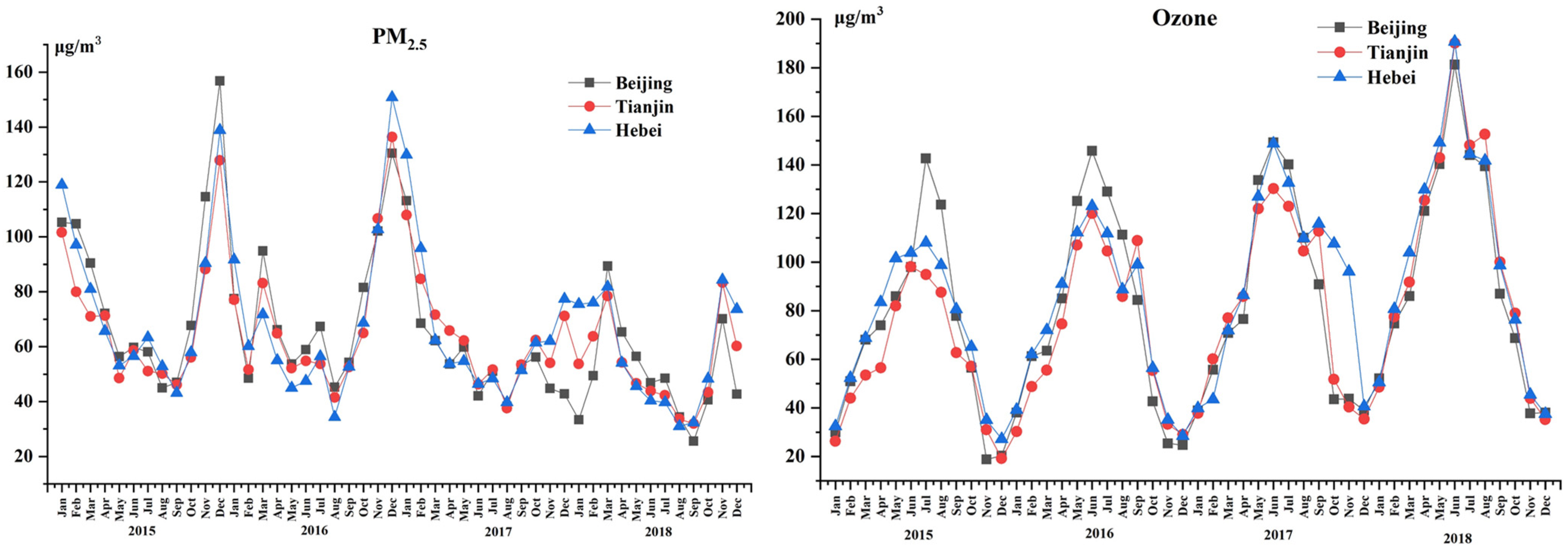
3.1. Spatial and Temporal Variation in PM2.5 and Ozone Concentrations
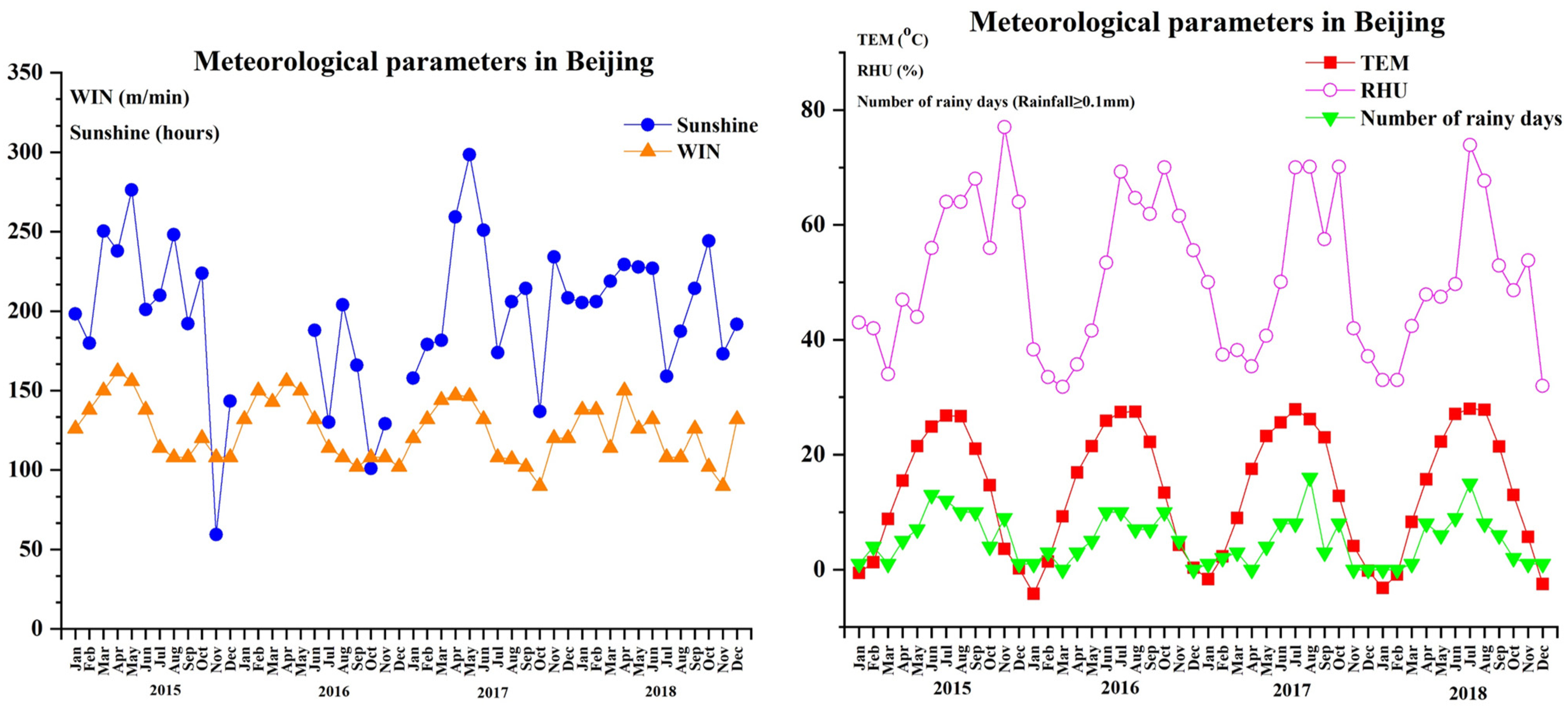
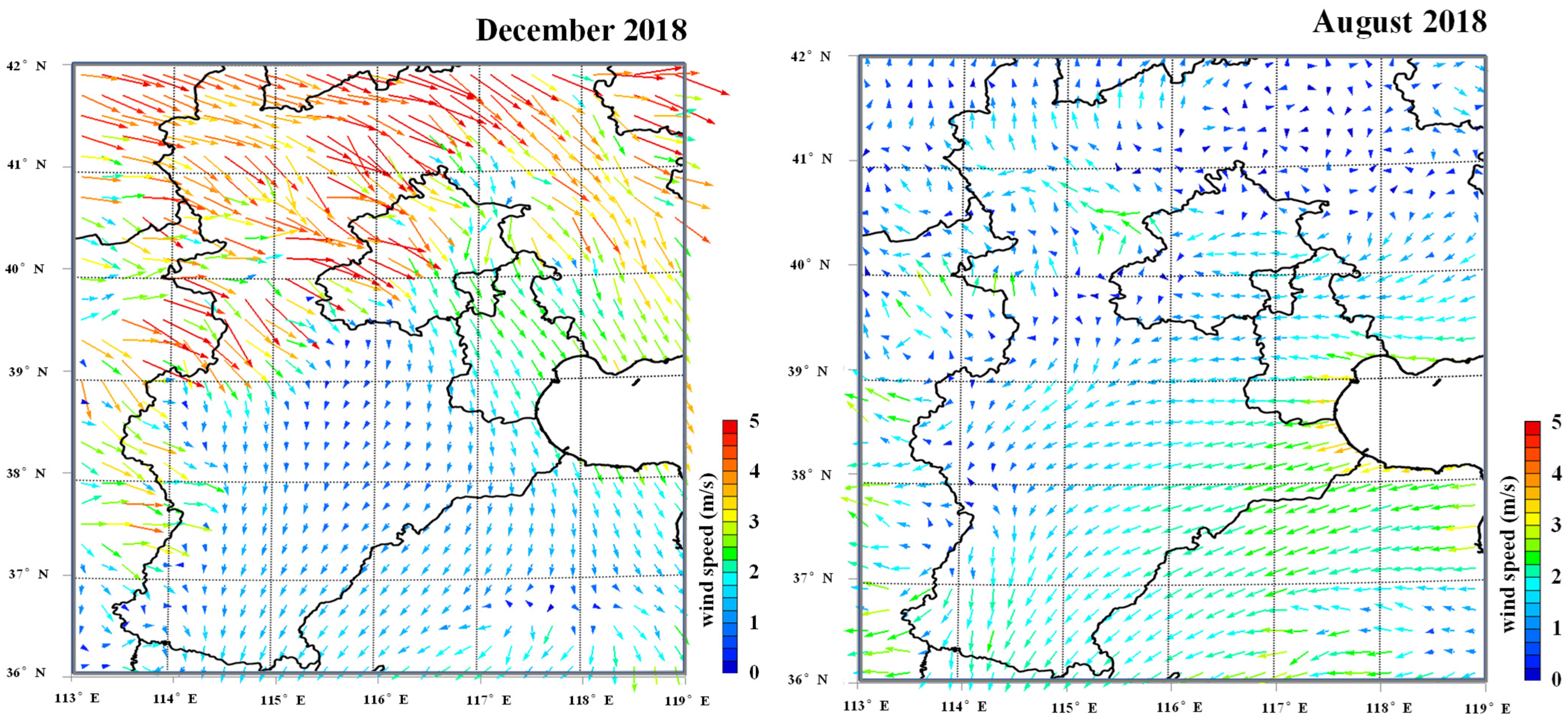
3.2. Relationship between Air Pollutants and Meteorological Parameters
3.3. Health Impact Attributable to PM2.5 and Ozone in the BTH Region
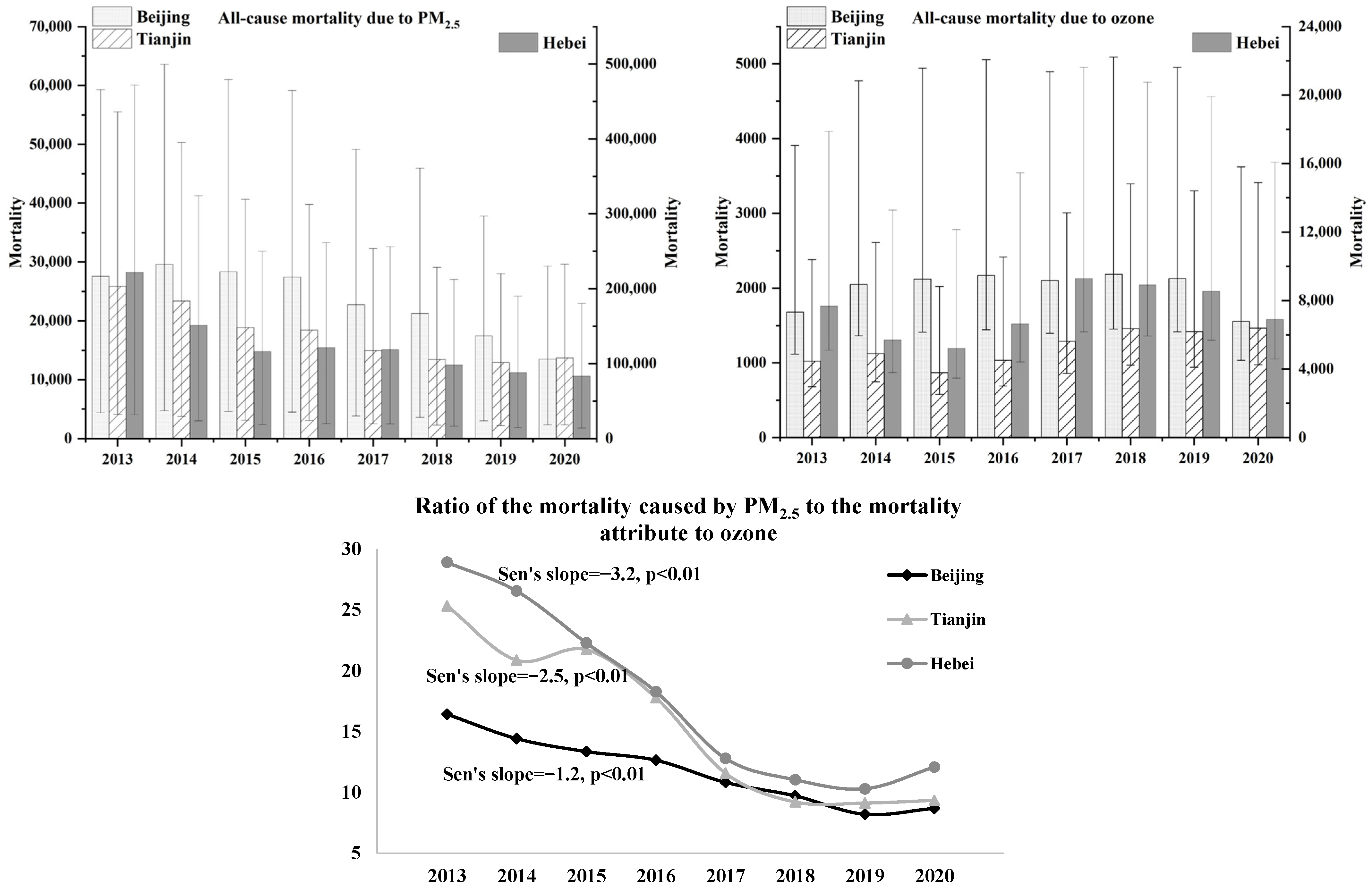
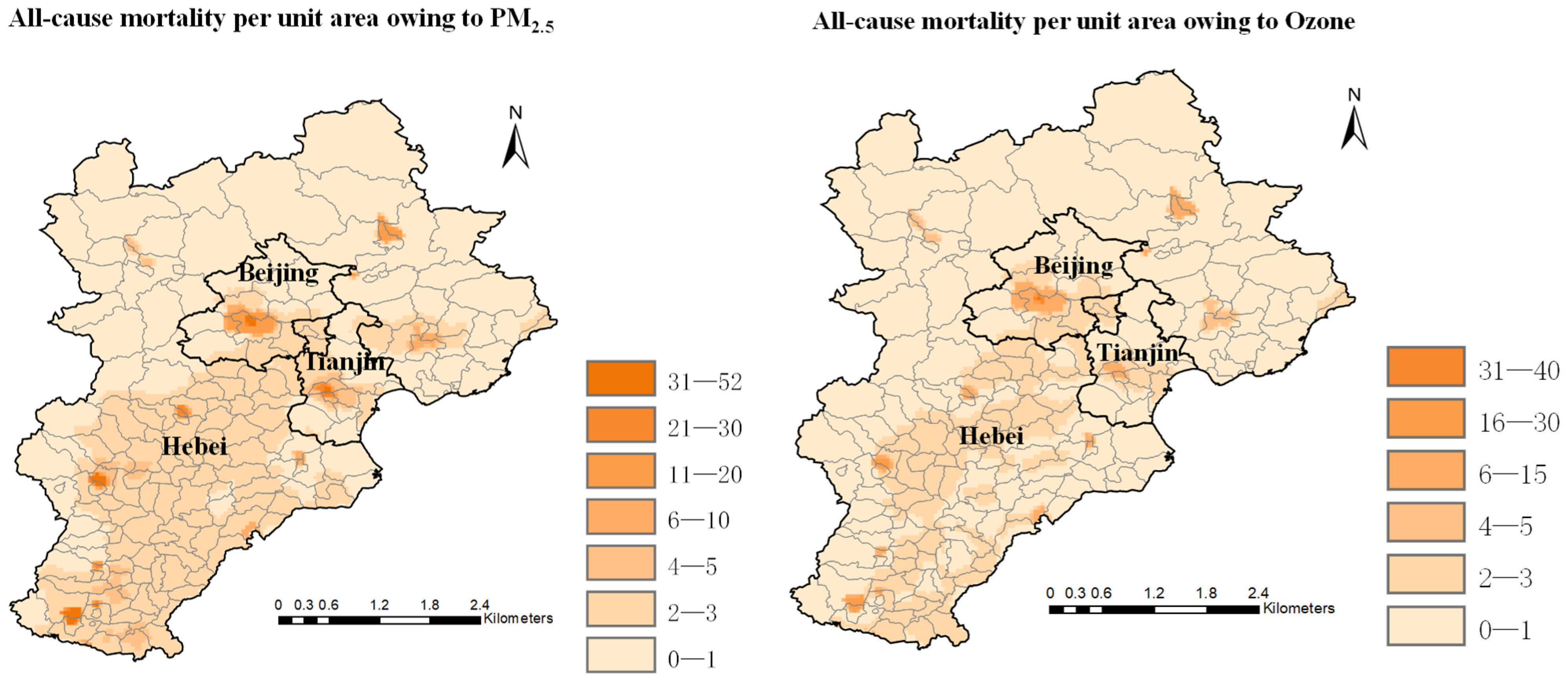
3.3.1. Heath Impact Attributable to the Concentration of PM2.5 and Ozone
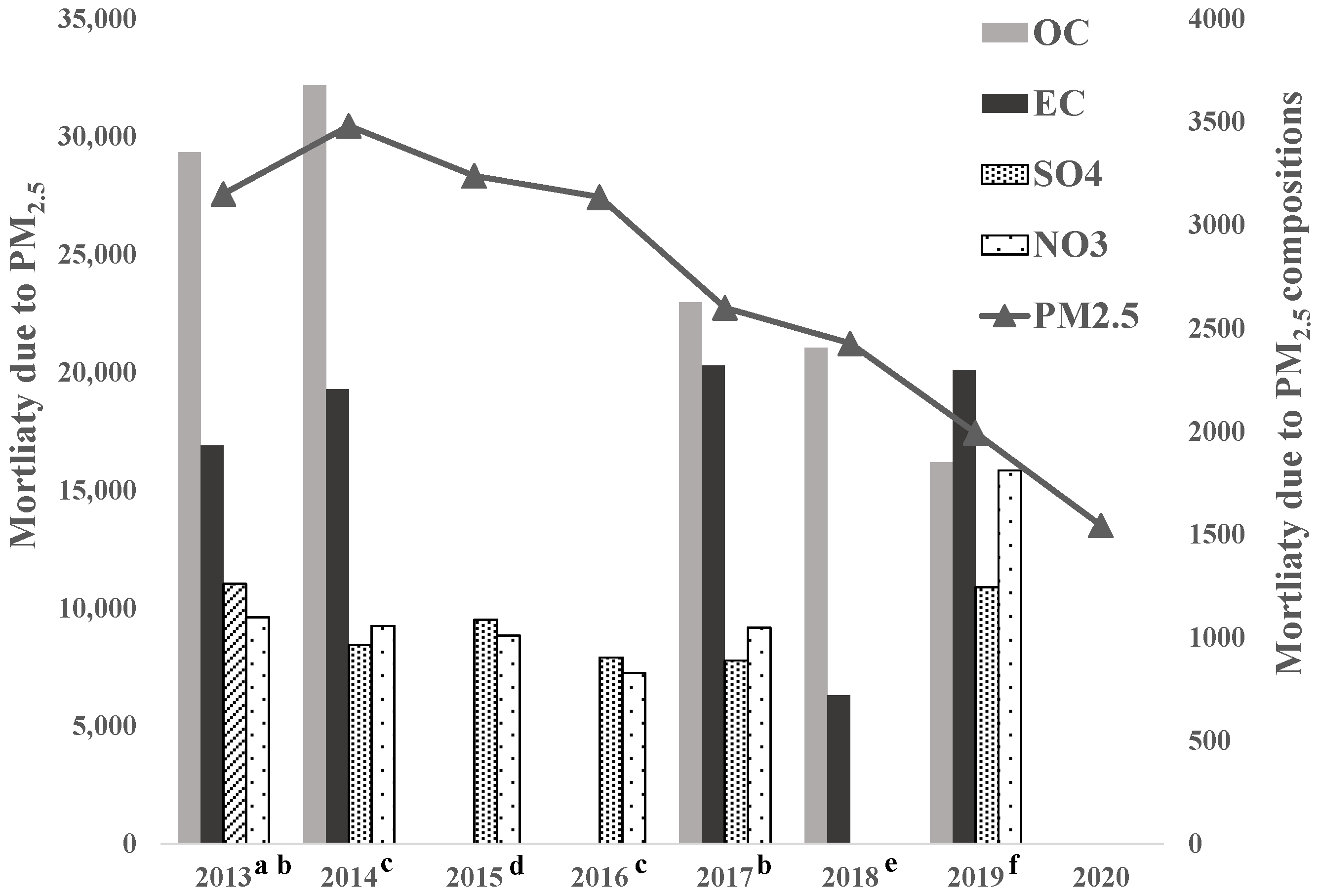
3.3.2. Health Effect Attributable to Main Compositions in PM2.5
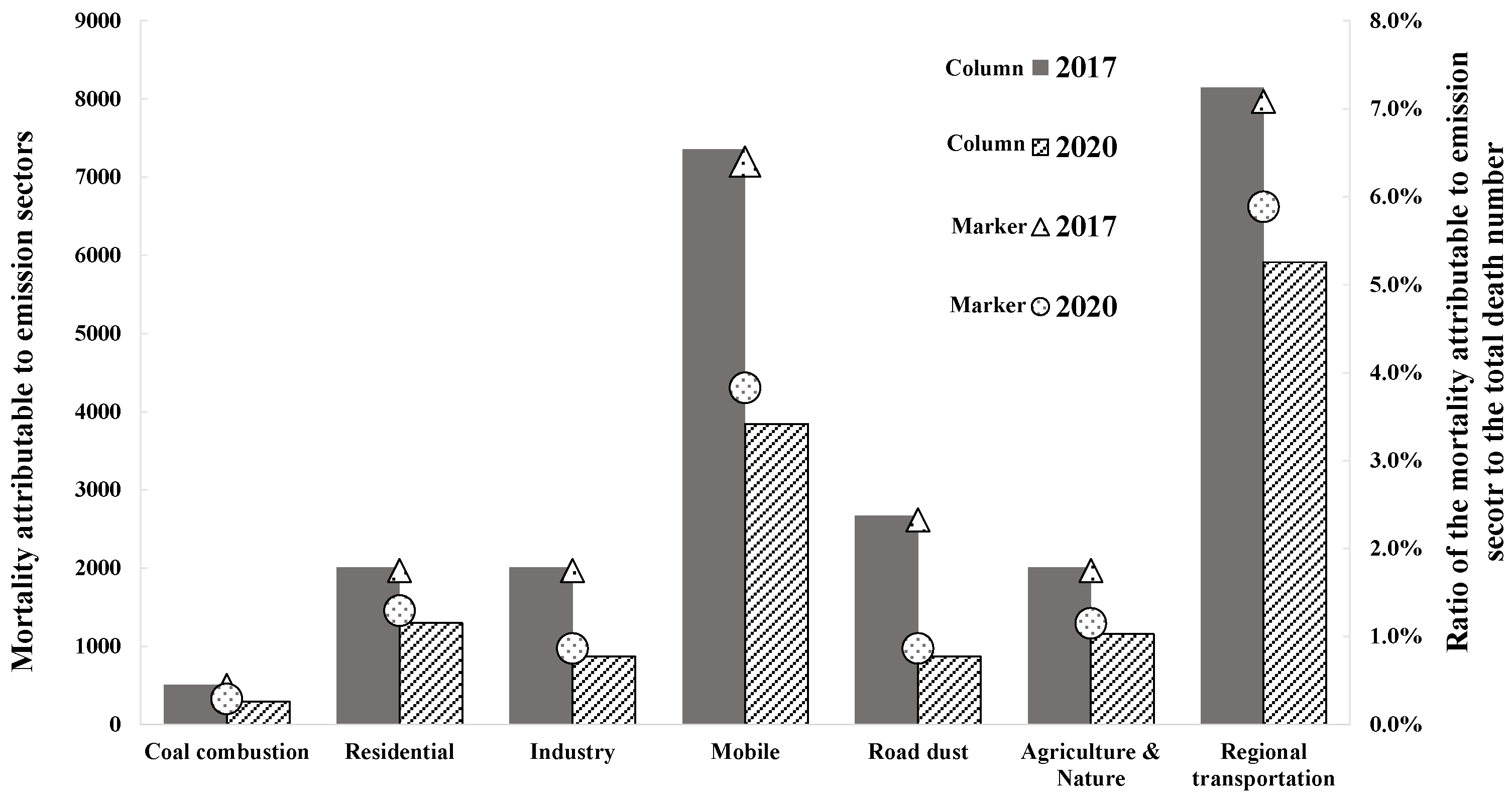
3.3.3. Health Effect Owing to Emission Sectors of PM2.5 in Beijing
4. Conclusions and Policy Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Faridi, S.; Shamsipour, M.; Krzyzanowski, M.; Künzli, N.; Amini, H.; Azimi, F.; Malkawi, M.; Momeniha, F.; Gholampour, A.; Hassanvand, M.S.; et al. Long-term trends and health impact of PM2.5 and O3 in Tehran, Iran, 2006–2015. Environ. Int. 2018, 114, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Atkinson, R.W.; Mills, I.C.; Walton, H.A.; Anderson, H.R. Fine particle components and health—A systematic review and meta-analysis of epidemiological time series studies of daily mortality and hospital admissions. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Nawahda, A.; Yamashita, K.; Ohara, T.; Kurokawa, J.; Yamaji, K. Evaluation of premature mortality caused by exposure to PM2.5 and ozone in East Asia: 2000, 2005, 2020. Water Air Soil Pollut. 2012, 223, 3445–3459. [Google Scholar] [CrossRef]
- Chen, F.; Yamashita, K.; Kurokawa, J.; Klimont, Z. Cost-benefit analysis of reducing premature mortality caused by exposure to ozone and PM2.5 in East Asia in 2020. Water Air Soil Pollut. 2015, 226, 1–17. [Google Scholar] [CrossRef]
- Song, C.; He, J.; Wu, L.; Jin, T.; Chen, X.; Li, R.; Ren, P.; Zhang, L.; Mao, H. Health burden attributable to ambient PM2.5 in China. Env. Pollut. 2017, 223, 575–586. [Google Scholar] [CrossRef]
- Ostro, B.; Spadaro, J.V.; Gumy, S.; Mudu, P.; Awe, Y.; Forastiere, F.; Peters, A. Assessing the recent estimates of the global burden of disease for ambient air pollution: Methodological changes and implications for low- and middle-income countries. Environ. Res. 2018, 166, 713–725. [Google Scholar] [CrossRef]
- Li, C.; Ma, X.; Fu, T.; Guan, S. Does public concern over haze pollution matter—Evidence from Beijing-Tianjin-Hebei region, China. Sci. Total Environ. 2021, 755, 142–397. [Google Scholar] [CrossRef]
- Conibear, L.; Butt, E.W.; Knote, C.; Arnold, S.R.; Spracklen, D.V. Residential energy use emissions dominate health impacts from exposure to ambient particulate matter in India. Nat. Commun. 2018, 9, 1–9. [Google Scholar] [CrossRef]
- Zhou, Q.; Cheng, L.; Zhang, Y.; Wang, Z.; Yang, S. Relationships between Springtime PM2.5, PM10, and O3 Pollution and the Boundary Layer Structure in Beijing, China. Sustainability 2022, 14, 9041. [Google Scholar] [CrossRef]
- Zhang, X.; Xiao, X.; Wang, F.; Brasseur, G.; Chen, S.; Wang, J.; Gao, M. Observed sensitivities of PM2.5 and O3 extremes to meteorological conditions in China and implications for the future. Environ. Int. 2022, 168, 107428. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.J.; Duan, F.K.; Su, H.; Ma, Y.L.; Cheng, Y.; Zheng, B.; Zhang, Q.; Huang, T.; Kimoto, T.; Chang, D.; et al. Exploring the severe winter haze in Beijing: The impact of synoptic weather, regional transport and heterogeneous reactions. Atmos. Chem. Phys. 2015, 15, 2969–2983. [Google Scholar] [CrossRef]
- Zheng, Y.; Xue, T.; Zhang, Q.; Geng, G.; Tong, D.; Xin, L.; He, K. Air quality improvements and health benefits from China’s clean air action since 2013. Environ. Res. Lett. 2017, 12, 114020. [Google Scholar] [CrossRef]
- China Statics Year Book 2014–2021. Available online: http://www.stats.gov.cn/english/ (accessed on 1 June 2022).
- Specifications and Test Procedures for Ambient Air Quality Continuous Monitoring System for PM10 and PM2.5; Ministry of Ecology and Environment the People’s Republic of China: Beijing, China, 2020. Available online: https://www.mee.gov.cn/xxgk2018/xxgk/xxgk06/202006/t20200630_786469.html (accessed on 1 June 2021).
- Ambient Air—Determination of Ozone—Ultraviolet Photometric Method; Ministry of Ecology and Environment the People’s Republic of China: Beijing, China, 2010. Available online: https://www.mee.gov.cn/ywgz/fgbz/bz/bzwb/jcffbz/201010/t20101026_196663.shtml (accessed on 1 June 2021).
- Calibration of Ambient Air Ozone Transfer Standard; Ministry of Ecology and Environment the People’s Republic of China: Beijing, China, 2020. Available online: https://www.mee.gov.cn/xxgk2018/xxgk/xxgk06/202006/t20200630_786469.html (accessed on 1 June 2021).
- Ji, D.; Gao, M.; Maenhaut, W.; He, J.; Wu, C.; Cheng, L.; Gao, W.; Sun, Y.; Sun, J.; Xin, J.; et al. The carbonaceous aerosol levels still remain a challenge in the Beijing-Tianjin-Hebei region of China: Insights from continuous high temporal resolution measurements in multiple cities. Environ. Int. 2019, 126, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wei, W.; Cheng, S.; Yao, S.; Zhang, H.; Zhang, C. Characteristics of PM2.5 and SNA components and meteorological factors impact on air pollution through 2013–2017 in Beijing, China. Atmos. Pollut. Res. 2019, 10, 1976–1984. [Google Scholar] [CrossRef]
- Jia, J.; Han, L.; Cheng, S.; Zhang, H.; Lv, Z. Pollution characteristic of PM2.5 and secondary inorganic ions in Beijing-Tianjin-Hebei region. China Environ. Sci. 2018, 38, 801–811. [Google Scholar]
- Ding, M.; Zhou, J.; Liu, B.; Wang, Y.; Zhang, B.; Shi, A.; Yang, D.; Chang, M. Pollution Characteristics of NH4+, NO3−, SO42− in PM2.5 and Their Precursor Gases During 2015 in an Urban Area of Beijing. Environ. Sci. 2017, 38, 1307–1315. [Google Scholar]
- Huang, X.; Tang, G.; Zhang, J.; Liu, B.; Liu, C.; Zhang, J.; Cong, L.; Cheng, M.; Yan, G.; Gao, W.; et al. Characteristics of PM2.5 pollution in Beijing after the improvement of air quality. J. Environ. Sci. 2021, 100, 1–10. [Google Scholar] [CrossRef]
- Luo, L.; Bai, X.; Liu, S.; Wu, B.; Liu, W.; Lv, Y.; Guo, Z.; Lin, S.; Zhao, S.; Hao, Y.; et al. Fine particulate matter (PM2.5/PM1.0) in Beijing, China: Variations and chemical compositions as well as sources. J. Environ. Sci. 2022, 121, 187–198. [Google Scholar] [CrossRef]
- Final Report Research Project on “A Study in Urban Air Pollution Improvement in Asia”; Japan International Cooperation Agency (JICA): Tokyo, Japan, 2017.
- Narita, D.; Oanh, N.T.K.; Sato, K.; Huo, M.; Permadi, D.A.; Chi, N.N.H.; Ratanajaratroj, T.; Pawarmart, I. Pollution characteristics and policy actions on fine particulate matter in a growing Asian economy: The case of Bangkok Metropolitan Region. Atmosphere 2019, 10, 227. [Google Scholar] [CrossRef]
- Song, Y.; Huang, B.; He, Q.; Chen, B.; Wei, J.; Mahmood, R. Dynamic assessment of PM2.5 exposure and health risk using remote sensing and geo-spatial big data. Env. Pollut. 2019, 253, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Yao, T.; Fung, J.C.H.; Lin, C. Estimation of health and economic costs of air pollution over the Pearl River Delta region in China. Sci. Total Environ. 2016, 566–567, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Shang, Y.; Sun, Z.; Cao, J.; Wang, X.; Zhong, L.; Bi, X.; Li, H.; Liu, W.; Zhu, T.; Huang, W. Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environ. Int. 2013, 54, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Achilleos, S.; Kioumourtzoglou, M.A.; Wu, C.D.; Schwartz, J.D.; Koutrakis, P.; Papatheodorou, S.I. Acute effects of fine particulate matter constituents on mortality: A systematic review and meta-regression analysis. Environ. Int. 2017, 109, 89–100. [Google Scholar] [CrossRef]
- World Health Organization. Health Risks of Ozone from Long-Range Transboundary Air Pollution; WHO Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- Center for International Earth Science Information Network—CIESIN—Columbia University (2018). Gridded Population of the World, Version 4 (GPWv4): Administrative Unit Center Points with Population Estimates; Revision 11; NASA Socioeconomic Data and Applications Center (SEDAC): Palisades, NY, USA, 2021. [Google Scholar] [CrossRef]
- China Air Quality Improvement Report (2013–2018); Ministry of Ecology and Environment of the People’s Republic of China: Beijing, China, 2019.
- Song, S.; Gao, M.; Xu, W.; Sun, Y.; Worsnop, D.R.; Jayne, J.T.; Zhang, Y.; Zhu, L.; Zhou, Z.; Cheng, C.; et al. Possible heterogeneous hydroxymethanesulfonate (HMS) chemistry in northern China winter haze. Atmos. Chem. Phys. 2019, 1357–1371. [Google Scholar] [CrossRef]
- Xue, T.; Liu, J.; Zhang, Q.; Geng, G.; Zheng, Y.; Tong, D.; Liu, Z.; Guan, D.; Bo, Y.; Zhu, T.; et al. Rapid improvement of PM2.5 pollution and associated health benefits in China during 2013–2017. Sci. China Earth Sci. 2019, 62, 1847–1856. [Google Scholar] [CrossRef]
- Huang, X.; Liu, Z.; Liu, J.; Hu, B.; Wen, T.; Tang, G.; Zhang, J.; Wu, F.; Ji, D.; Wang, L.; et al. Chemical characterization and source identification of PM2.5 at multiple sites in the Beijing–Tianjin–Hebei region, China. Atmos. Chem. Phys. 2017, 17, 12941–12962. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PM2.5 | Wind Speed | Relative Humidity | Air Temperature | Sunshine Hours | Air Pressure | Ozone | |
|---|---|---|---|---|---|---|---|
| PM2.5 | 1 | −0.578 ** | 0.823 ** | 0.255 ** | −0.560 ** | −0.402 ** | −0.538 ** |
| Wind speed | 1 | −0.620 ** | 0.051 | 0.462 ** | 0.172 | 0.713 ** | |
| Relative humidity | 1 | 0.17 | −0.672 ** | −0.366 ** | −0.672 ** | ||
| Air temperature | 1 | 0.013 | −0.641 ** | 0.119 | |||
| Sunshine hours | 1 | 0.218 * | 0.655 ** | ||||
| Air pressure | 1 | 0.195 * | |||||
| Ozone | 1 |
| PM2.5 | Wind Speed | Relative Humidity | Air Temperature | Sunshine Hours | Air Pressure | Ozone | |
|---|---|---|---|---|---|---|---|
| PM2.5 | 1 | −0.245 ** | 0.424 ** | 0.235 ** | −0.236 ** | −0.196 * | 0.474 ** |
| Wind speed | 1 | −0.134 | 0.015 | 0.079 | −0.003 | −0.161 | |
| Relative humidity | 1 | −0.243 ** | −0.676 ** | −0.124 | −0.189 * | ||
| Air temperature | 1 | 0.314 ** | −0.461 ** | 0.549 ** | |||
| Sunshine hours | 1 | −0.017 | 0.449 ** | ||||
| Air pressure | 1 | −0.155 | |||||
| Ozone | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huo, M.; Yamashita, K.; Chen, F.; Sato, K. Spatial-Temporal Variation in Health Impact Attributable to PM2.5 and Ozone Pollution in the Beijing Metropolitan Region of China. Atmosphere 2022, 13, 1813. https://doi.org/10.3390/atmos13111813
Huo M, Yamashita K, Chen F, Sato K. Spatial-Temporal Variation in Health Impact Attributable to PM2.5 and Ozone Pollution in the Beijing Metropolitan Region of China. Atmosphere. 2022; 13(11):1813. https://doi.org/10.3390/atmos13111813
Chicago/Turabian StyleHuo, Mingqun, Ken Yamashita, Fang Chen, and Keiichi Sato. 2022. "Spatial-Temporal Variation in Health Impact Attributable to PM2.5 and Ozone Pollution in the Beijing Metropolitan Region of China" Atmosphere 13, no. 11: 1813. https://doi.org/10.3390/atmos13111813
APA StyleHuo, M., Yamashita, K., Chen, F., & Sato, K. (2022). Spatial-Temporal Variation in Health Impact Attributable to PM2.5 and Ozone Pollution in the Beijing Metropolitan Region of China. Atmosphere, 13(11), 1813. https://doi.org/10.3390/atmos13111813