High Dose Ifosfamide in Relapsed and Unresectable High-Grade Osteosarcoma Patients: A Retrospective Series

 ,
,  , , ,
, , , 
 , and
, and
Abstract
1. Introduction
2. Patients and Methods
3. Results
3.1. Response
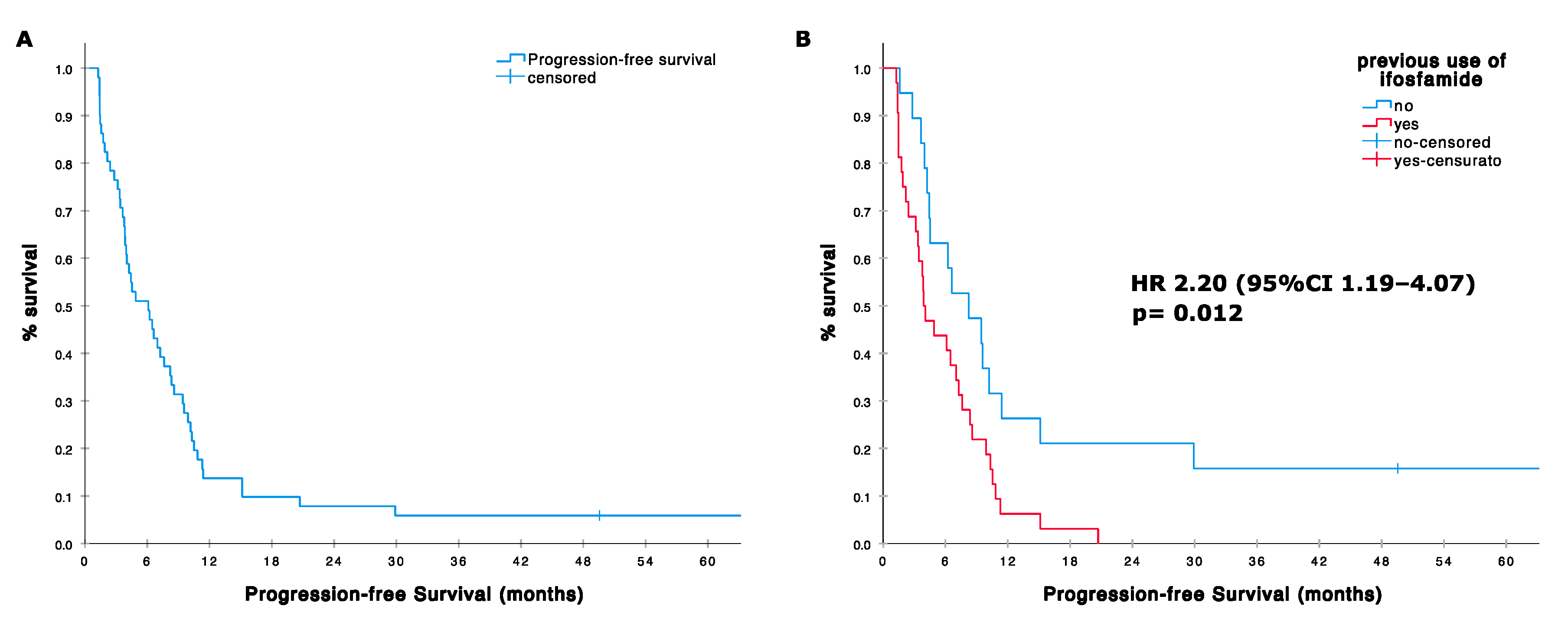
3.2. Progression Free Survival (PFS)
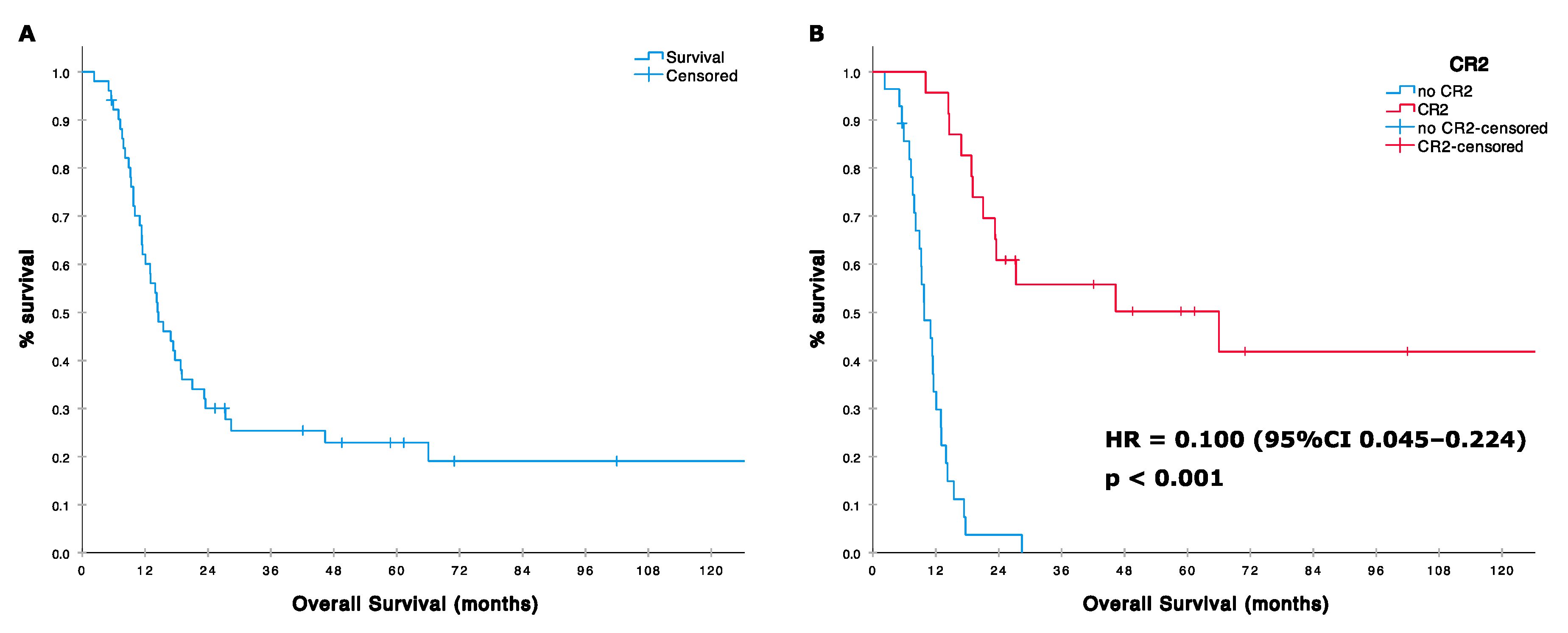
3.3. Overall Survival (OS) Post HDIFO
3.4. PFS and OS Multivariate Analysis
3.5. Toxicity
3.6. PARP1 Expression and Mutational Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Campanacci, M. Bone and Soft Tissue Tumors. In Clinical Features, Imaging, Pathology and Treatment, 2nd ed.; Springer: New York, NY, USA, 1999; pp. 463–557. [Google Scholar]
- Fletcher, C.D.M.; Bridge, J.A.; Hogendoorn, P.C.W.; Mertens, F. WHO Classification of Tumours of Soft Tissue and Bone, 4th ed.; IARC Press: Lyon, France, 2013. [Google Scholar]
- Casali, P.G.; Bielack, S.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brennan, B.; et al. Bone sarcomas: ESMO-PaedCan-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv79–iv95. [Google Scholar] [CrossRef] [PubMed]
- Bielack, S.S.; Kempf-Bielack, B.; Delling, G.; Exner, G.U.; Flege, S.; Helmke, K.; Kotz, R.; Salzer-Kuntschik, M.; Werner, M.; Winkelmann, W.; et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J. Clin. Oncol. 2002, 20, 776–790. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.; Palmerini, E. Adjuvant and neoadjuvant combination chemotherapy for osteogenic sarcoma. Curr. Opin. Oncol. 2007, 19, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; van den Berg, H.; Brennan, B.; et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): An open-label, international, randomised controlled trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef]
- Ferrari, S.; Briccoli, A.; Mercuri, M.; Bertoni, F.; Picci, P.; Tienghi, A.; del Prever, A.B.; Fagioli, F.; Comandone, A.; Bacci, G. Postrelapse survival in osteosarcoma of the extremities: Prognostic factors for long-term survival. J. Clin. Oncol. 2003, 21, 710–715. [Google Scholar] [CrossRef]
- Kempf-Bielack, B.; Bielack, S.S.; Jurgens, H.; Branscheid, D.; Berdel, W.E.; Exner, G.U.; Göbel, U.; Helmke, K.; Jundt, G.; Kabisch, H.; et al. Osteosarcoma relapse after combined modality therapy: An analysis of unselected patients in the Cooperative Osteosarcoma Study Group (COSS). J. Clin. Oncol. 2005, 23, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Kung, F.H.; Pratt, C.B.; Vega, R.A.; Jaffe, N.; Strother, D.; Schwenn, M.; Nitschke, R.; Homans, A.C.; Holbrook, C.T.; Golembe, B.; et al. Ifosfamide/etoposide combination in the treatment of recurrent malignant solid tumors of childhood. A Pediatric Oncology Group Phase II study. Cancer 1993, 71, 1898–1903. [Google Scholar] [CrossRef]
- Miser, J.S.; Kinsella, T.J.; Triche, T.J.; Tsokos, M.; Jarosinski, P.; Forquer, R.; Wesley, R.; Magrath, I. Ifosfamide with mesna uroprotection and etoposide: An effective regimen in the treatment of recurrent sarcomas and other tumors of children and young adults. J. Clin. Oncol. 1987, 5, 1191–1198. [Google Scholar] [CrossRef]
- Rodríguez-Galindo, C.; Daw, N.C.; Kaste, S.C.; Dome, J.S.; Pappo, A.S.; Rao, B.N.; Pratt, C.B. Treatment of refractory osteosarcoma with fractionated cyclophosphamide and etoposide. J. Pediatr. Hematol. Oncol. 2002, 24, 250–255. [Google Scholar] [CrossRef]
- Berger, M.; Grignani, G.; Ferrari, S.; Biasin, E.; del Prever, A.B.; Aliberti, S.; Saglio, F.; Aglietta, M.; Fagioli, F. Phase 2 trial of two courses of cyclophosphamide and etoposide for relapsed high-risk osteosarcoma patients. Cancer 2009, 115, 2980–2987. [Google Scholar] [PubMed]
- Fox, E.; Patel, S.; Wathen, J.K.; Schuetze, S.; Chawla, S.; Harmon, D.; Reinke, D.; Chugh, R.; Benjamin, R.S.; Helman, L.J. Phase II study of sequential gemcitabine followed by docetaxel for recurrent Ewing sarcoma, osteosarcoma, or unresectable or locally recurrent chondrosarcoma: Results of Sarcoma Alliance for Research Through Collaboration Study 003. Oncologist 2012, 17, 321. [Google Scholar] [CrossRef]
- Navid, F.; Willert, J.R.; McCarville, M.B.; Furman, W.; Watkins, A.; Roberts, W.; Daw, N.C. Combination of gemcitabine and docetaxel in the treatment of children and young adults with refractory bone sarcoma. Cancer 2008, 113, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Song, B.S.; Seo JKim, D.H.; Lim, J.S.; Yoo, J.Y.; Lee, J.A. Gemcitabine and docetaxel for the treatment of children and adolescents with recurrent or refractory osteosarcoma: Korea Cancer Center Hospital experience. Pediatr. Blood Cancer 2014, 61, 1376–1381. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, E.; Jones, R.L.; Marchesi, E.; Paioli, A.; Cesari, M.; Longhi, A.; Meazza, C.; Coccoli, L.; Fagioli, F.; Asaftei, S.; et al. Gemcitabine and docetaxel in relapsed and unresectable high-grade osteosarcoma and spindle cell sarcoma of bone. BMC Cancer 2017, 16, 280. [Google Scholar] [CrossRef] [PubMed]
- Chou, A.J.; Merola, P.R.; Wexler, L.H.; Gorlick, R.G.; Vyas, Y.M.; Healey, J.H.; LaQuaglia, M.P.; Huvos, A.G.; Meyers, P.A. Treatment of osteosarcoma at first recurrence after contemporary therapy: The Memorial Sloan-Kettering Cancer Center experience. Cancer 2005, 104, 2214–2221. [Google Scholar] [CrossRef]
- Verschoor, A.J.; Speetjens, F.M.; Dijkstra, P.D.S.; Fiocco, M.; van de Sande, M.A.J.; Bovée, J.V.M.G.; Gelderblom, H. Single-Center Experience with Ifosfamide Monotherapy as Second-Line Treatment of Recurrent/Metastatic Osteosarcoma. Oncologist 2020, 25, e716–e721. [Google Scholar] [CrossRef]
- Patel, S.R.; Vadhan-Raj, S.; Papadopolous, N.; Plager, C.; Burgess, M.A.; Hays, C.; Benjamin, R.S. High-dose ifosfamide in bone and soft tissue sarcomas: Results of phase II and pilot studies--dose-response and schedule dependence. J. Clin. Oncol. 1997, 15, 2378–2384. [Google Scholar] [CrossRef]
- Harris, M.B.; Cantor, A.B.; Goorin, A.M.; Shochat, S.J.; Ayala, A.G.; Ferguson, W.S.; Holbrook, T.; Link, M.P. Treatment of osteosarcoma with ifosfamide: Comparison of response in pediatric patients with recurrent disease versus patients previously untreated: A Pediatric Oncology Group study. Med. Pediatr. Oncol. 1995, 24, 87–92. [Google Scholar] [CrossRef]
- Berrak, S.G.; Pearson, M.; Berberoğlu, S.; Ilhan, I.E.; Jaffe, N. High-dose ifosfamide in relapsed pediatric osteosarcoma: Therapeutic effects and renal toxicit. Pediatr. Blood Cancer 2005, 44, 215–219. [Google Scholar] [CrossRef]
- Ferrari, S.; Zolezzi, C.; Cesari, M.; Fasano, M.C.; Lamanna, G.; Bacci, G. Prospective evaluation of high-dose ifosfamide-related nephrotoxicity in young adult patients with recurrent osteosarcoma previously treated with cisplatin, methotrexate and standard-dose ifosfamide. Anticancer Drugs 1999, 10, 25–31. [Google Scholar] [CrossRef]
- Grignani, G.; Palmerini, E.; Dileo, P.; Asaftei, S.D.; D’Ambrosio, L.; Pignochino, Y.; Mercuri, M.; Picci, P.; Fagioli, F.; Casali, P.G.; et al. A phase II trial of sorafenib in relapsed and unresectable high-grade osteosarcoma after failure of standard multimodal therapy: An Italian Sarcoma Group study. Ann. Oncol. 2012, 23, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, N.; Sirvent, J.B.; Venkatramani, R.; Longhi, A.; Lervat, C.; Casanova, M.; Aerts, I.; Bielack, S.S.; Entz-Werle, N.; Strauss, S.; et al. Phase I combination dose-finding/phase II expansion cohorts of lenvatinib + etoposide + ifosfamide in patients (pts) aged 2 to ≤ 25 years with relapsed/refractory (r/r) osteosarcoma. Ann. Oncol. 2019, 30, v688. [Google Scholar] [CrossRef]
- Duffaud, F.; Mir, O.; Boudou-Rouquette, P.; Piperno-Neumann, S.; Penel, N.; Bompas, E.; Delcambre, C.; Kalbacher, E.; Italiano, A.; Collard, O.; et al. Efficacy and safety of regorafenib in adult patients with metastatic osteosarcoma: A non-comparative, randomised, double-blind, placebo-controlled, phase 2 study. Lancet Oncol. 2019, 20, 120–133. [Google Scholar] [CrossRef]
- Davis, L.E.; Bolejack, V.; Ryan, C.W.; Ganjoo, K.N.; Loggers, E.; Chawla, S.; Agulnik, M.; Livingston, M.B.; Reed, D.; Keedy, V.; et al. Randomized Double-Blind Phase II Study of Regorafenib in Patients with Metastatic Osteosarcoma. J. Clin. Oncol. 2019, 37, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Italiano, A.; Mir, O.; Mathoulin-Pelissier, S.; Penel, N.; Piperno-Neumann, S.; Bompas, E.; Chevreau, C.; Duffaud, F.; Entz-Werle, N.; Saâda, E.; et al. Cabozantinib in patients with advanced Ewing sarcoma or osteosarcoma (CABONE): A multicentre, single-arm, phase 2 trial. Lancet Oncol. 2020, 21, 446–455. [Google Scholar] [CrossRef]
- Le Cesne, A.; Antoine, E.; Spielmann, M.; Fumagalli, E.; Pilotti, S.; Morosi, C.; Messina, A.; Tos, A.P.D.; Gronchi, A.; Casali, P.G. High-dose ifosfamide: Circumvention of resistance to standard-dose ifosfamide in advanced soft tissue sarcomas. J. Clin. Oncol. 1995, 13, 1600–1608. [Google Scholar] [CrossRef]
- Pelgrims, J.; De Vos, F.; Van den Brande, J.; Schrijvers, D.; Prové, A.; Vermorken, J.B. Methylene blue in the treatment and prevention of ifosfamide-induced encephalopathy: Report of 12 cases and a review of the literature. Br. J. Cancer 2000, 82, 291–294. [Google Scholar] [CrossRef]
- Pignochino, Y.; Capozzi, F.; D’Ambrosio, L.; Dell’Aglio, C.; Basiricò, M.; Canta, M.; Lorenzato, A.; Vignolo Lutati, F.; Aliberti, S.; Palesandro, E.; et al. PARP1 expression drives the synergistic antitumor activity of trabectedin and PARP1 inhibitors in sarcoma preclinical models. Mol. Cancer 2017, 16, 86. [Google Scholar] [CrossRef]
- Grignani, G.; D’Ambrosio, L.; Pignochino, Y.; Palmerini, E.; Zucchetti, M.; Boccone, P.; Aliberti, S.; Stacchiotti, S.; Bertulli, R.; Piana, R.; et al. Trabectedin and olaparib in patients with advanced and non-resectable bone and soft tissue sarcomas (TOMAS trial): A phase 1b study from the Italian Sarcoma Group. Lancet Oncol. 2018, 19, 1360–1371. [Google Scholar] [CrossRef]
- Bertucci, F.; Finetti, P.; Monneur, A.; Perrot, D.; Chevreau, C.; Le Cesne, A.; Blay, J.Y.; Mir, O.; Birnbaum, D. PARP1 expression in soft tissue sarcomas is a poor-prognosis factor and a new potential therapeutic target. Mol. Oncol. 2019, 13, 1577–1588. [Google Scholar] [CrossRef]
- Lønning, P.; Knappskog, S. Mapping genetic alterations causing chemoresistance in cancer: Identifying the roads by tracking the drivers. Oncogene 2013, 32, 5315–5330. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Pleasance, E.; Zhao, E.Y.; Ng, T.; Grewal, J.K.; Mohammad, N.; Taylor, S.K.; Simmons, C.; Srikanthan, A.; Rassekh, S.R. Therapeutic Implication of Genomic Landscape of Adult Metastatic Sarcoma. JCO Precis. Oncol. 2019, 3, 1–25. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Drugs | No | CR + PR | ORR | Authors |
|---|---|---|---|---|
| IFO 2 g/m2/day 1–3 ETO 100 mg/m2/day 1–3 | 32 | 2/3 | 16 | Kung FH, Cancer 1992 [9] |
| IFO 2 g/m2/day 1–3 ETO 100 mg/m2/day 1–3 | 8 | 0/3 | 37 | Miser JS, J Clin Onc 1997 [10] |
| CTX 500 mg/m2/day 1–5 ETO 100 mg/m2/day 1–5 | 14 | 1/3 | 28 | Rodriguez-Galindo C, JPHO 2002 [11] |
| CTX 4000 mg/m2/day ETO 200 mg/m2/day 1–3 | 26 | 2/3 | 19 | Berger M, Cancer, 2009 [12] |
| GEM 900 mg/m2/day, d1,8 TAXO 80–100 mg/m2, d1 | 14 | 0/1 | 7 | Fox E. SARC 003, Oncologist 2012 [13] |
| GEM 675 mg/m2, d 1,8 TAXO 75–100 mg/m2, d1 | 10 | 0/3 | 30 | Navid F, Cancer 2008 [14] |
| GEM 675–900 mg/m2, d 1,8 TAXO 100 mg/m2, d1 | 17 | 3/1 | 24 | Song BS, Pediatr Blood Cancer 2014 [15] |
| GEM 675–900 mg/m2 d1,8 TAXO 75 mg/m2 d1 | 34 | 0/5 | 15 | Palmerini E, BMC Cancer 2017 [16] |
| IFO 2.8 g/m2/day 1–5 | 23 | nr | nr | Chou AJ, Cancer 2005 [17] |
| IFO 2.5 gr/m2 1–2 or IFO 3 gr/m2 1–3 | 26 36 | 6 13 | 23 36 | Verschoor AJ, Oncologist, 2019 [18] |
| IFO 14 g/m2 CI d 1–14 | 19 | 2/6 | 42 | Patel SR, JCO, 1997 [19] |
| IFO 14 g/m2 CI d 1–14 | 16 | 6/4 | 62 | Berrak SG, Ped Blood Cancer 2005 [20] |
| IFO 12 g/m2 CI d 1–14 | 30 | 1/2 | 10 | Harris MB, Med Ped Oncol 1995 [21] |
| n | % | |
|---|---|---|
| All | 51 | 100 |
| Age median, range (years) | 19 (7–68) | |
| ≥18 years | 30 | 59 |
| <18 years | 21 | 41 |
| Sex | ||
| male | 33 | 65 |
| female | 18 | 53 |
| ECOG | ||
| 0 | 47 | 92 |
| 1 | 4 | 8 |
| Line at HDIFO | ||
| 1 | 46 | 90 |
| ≥2 | 5 | 10 |
| Histology | ||
| Osteoblatstic | 38 | 74 |
| Chondroblastic | 6 | 12 |
| Other | 7 | 14 |
| Metastases at diagnosis or relapse | ||
| Diagnosis | 5 | 90 |
| Relapse | 46 | 10 |
| Median time from diagnosis to HD-IFO | ||
| <24 months | 29 | 57 |
| ≥24 months | 22 | 43 |
| Pattern of metastases | ||
| Lung | 35 | 68 |
| Bone | 3 | 6 |
| Multiple sites | 13 | 26 |
| Ifosfamide in pretreatment | ||
| yes | 32 | 63 |
| no | 19 | 37 |
| Previous metastasectomy | ||
| yes | 26 | 51 |
| no | 25 | 49 |
| Primary tumor histologic response | ||
| <90% | 23 | 45 |
| ≥90% | 24 | 47 |
| Not available | 4 | 8 |
| All (n = 51) n (%) | <18 yrs (n = 21) n (%) | ≥18 yrs (n = 30) n (%) | p | |
|---|---|---|---|---|
| CR PR | 10 (20) | 6 (28) | 4 (13) | 0.186 |
| SD | 29 (57) | 10 (48) | 19 (63) | |
| PD | 12 (23) | 5 (24) | 7 (23) |
| n (%) | Median Months (95%CI) | HR (95%CI) | p Value | |
|---|---|---|---|---|
| All | 51 (100) | 6.1 (3.7–8.5) | ||
| Age median, range (years) | 19 (7–68) | 0.540 | ||
| ≥18 years | 30 (59) | 6.1 (3.1–9.1) | 0.835 (0.468–1488) | |
| <18 years | 21 (41) | 4.9 (0.47–9.3) | ||
| Sex | 0.789 | |||
| male | 33 (65) | 4.9 (2–7.7) | 1.086 (0.594–1.983) | |
| female | 18 (53) | 6.1 (1.5–10.7) | ||
| ECOG | 0.671 | |||
| 0 | 47 (92) | 6.1 (3.4–8.8) | 1.291 (0.397–4.196) | |
| 1 | 4 (8) | 7.3 (0.2–14.4) | ||
| Line of CT | 0.042 | |||
| 1° line | 46 (90) | 6.1 (3.0–9.2) | 0.369 (0.141–0.966) | |
| ≥2° line | 5 (10) | 3.1 (0–6.8) | ||
| Pattern of metastases | 0.890 | |||
| Lung | 35 (69) | 6.5 (3.7–9.2) | 0.957 (0.515–1.780) ** | |
| Bone | 3 (6) | 1.3 (NE) | ||
| Multiple sites | 13 (25) | 3.8 (3.2–4.4) | ||
| Ifosfamide in pretreatment | 0.012 | |||
| yes | 32 (63) | 3.9 (2.3–5.4) | 2.20 (1.19–4.07) | |
| no | 19 (37) | 8.2 (3.7–12.7) | ||
| Histologic response for | 0.833 | |||
| primary * | ||||
| good | 24 (51) | 6.2 (2.9–9.5) | 1.065 (0.592–1.918) | |
| poor | 23 (49) | 6.1 (2.8–9.4) |
| n (%) | Median Months (95%CI) | HR | p Value | |
|---|---|---|---|---|
| All | 51 (100) | 14.5 (10.1–18.9) | ||
| Age median, range (years) | 19 (7–68) | 0.626 | ||
| ≥18 years | 30 (59) | 16.8 (11.8–21.9) | 0.852 | |
| <18 years | 21 (41) | 11.0 (5.4–16.6) | (0.448–1.620) | |
| Sex | 0.721 | |||
| male | 33 (65) | 15.4 (10.9–20.0) | 0.885 | |
| female | 18 (53) | 11.3 (10.4–12.2) | (0.454–1.728) | |
| ECOG | 0.86 | |||
| 0 | 47 (92) | 15.4 (10.6–20.3) | 1.137 | |
| 1 | 4 (8) | 13.0 (1.6–24.4) | (0.272–4.749) | |
| Line of CT | 0.21 | |||
| 1° line | 46 (90) | 14.4 (10.2–18.6) | 0.51 | |
| ≥2° line | 5 (10) | 9.3 (0–19.5) | (0.177–1.464) | |
| Response to CT | <0.001 | |||
| CR/PR | 10 (20) | 14.4 2–26.8) | ||
| SD | 29 (57) | 18.8 (8.6–29.0) | 0.223 | |
| PD | 12 (23) | 7.6 (3.4–11.9) | (0.106–0.470) ** | |
| Pattern of metastases | 0.484 | |||
| Lung | 35 (69) | 16.8 (12.6–21.1) | ||
| Bone | 3 (6) | 17.7 (NE) | 0.788 | |
| Multiple sites | 13 (25) | 9.8 (6.9–12.7) | (0.404–1.537) *** | |
| Prior ifosfamide | 0.018 | |||
| no | 19 (37) | 23.5 (0–62.4) | 0.428 | |
| yes | 32 (63) | 12.1 (.0–18.1) | (0.212–0.863) | |
| Histologic response for | 0.059 | |||
| Primary * | ||||
| good | 24 (51) | 18.8 (15.4–22.2) | 0.527 | |
| poor | 23 (49) | 13.0 (8.6–17.5) | (0.271–1.025) | |
| CR2 | <0.001 | |||
| yes | 23(45) | 66.0 (1.7–130.4) | 0.100 | |
| no | 28 (55) | 9.8 (7.0–12.6) | (0.045–0.224) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmerini, E.; Setola, E.; Grignani, G.; D’Ambrosio, L.; Comandone, A.; Righi, A.; Longhi, A.; Cesari, M.; Paioli, A.; Hakim, R.; et al. High Dose Ifosfamide in Relapsed and Unresectable High-Grade Osteosarcoma Patients: A Retrospective Series. Cells 2020, 9, 2389. https://doi.org/10.3390/cells9112389
Palmerini E, Setola E, Grignani G, D’Ambrosio L, Comandone A, Righi A, Longhi A, Cesari M, Paioli A, Hakim R, et al. High Dose Ifosfamide in Relapsed and Unresectable High-Grade Osteosarcoma Patients: A Retrospective Series. Cells. 2020; 9(11):2389. https://doi.org/10.3390/cells9112389
Chicago/Turabian StylePalmerini, Emanuela, Elisabetta Setola, Giovanni Grignani, Lorenzo D’Ambrosio, Alessandro Comandone, Alberto Righi, Alessandra Longhi, Marilena Cesari, Anna Paioli, Rossella Hakim, and et al. 2020. "High Dose Ifosfamide in Relapsed and Unresectable High-Grade Osteosarcoma Patients: A Retrospective Series" Cells 9, no. 11: 2389. https://doi.org/10.3390/cells9112389
APA StylePalmerini, E., Setola, E., Grignani, G., D’Ambrosio, L., Comandone, A., Righi, A., Longhi, A., Cesari, M., Paioli, A., Hakim, R., Pierini, M., Marchesi, E., Vanel, D., Pignochino, Y., Donati, D. M., Picci, P., & Ferrari, S. (2020). High Dose Ifosfamide in Relapsed and Unresectable High-Grade Osteosarcoma Patients: A Retrospective Series. Cells, 9(11), 2389. https://doi.org/10.3390/cells9112389