
Safety Profile and Issues of Subcutaneous Immunotherapy in the Treatment of Children with Allergic Rhinitis


Abstract
:1. Introduction
Objective
2. Materials and Methods
2.1. Ethics Approval
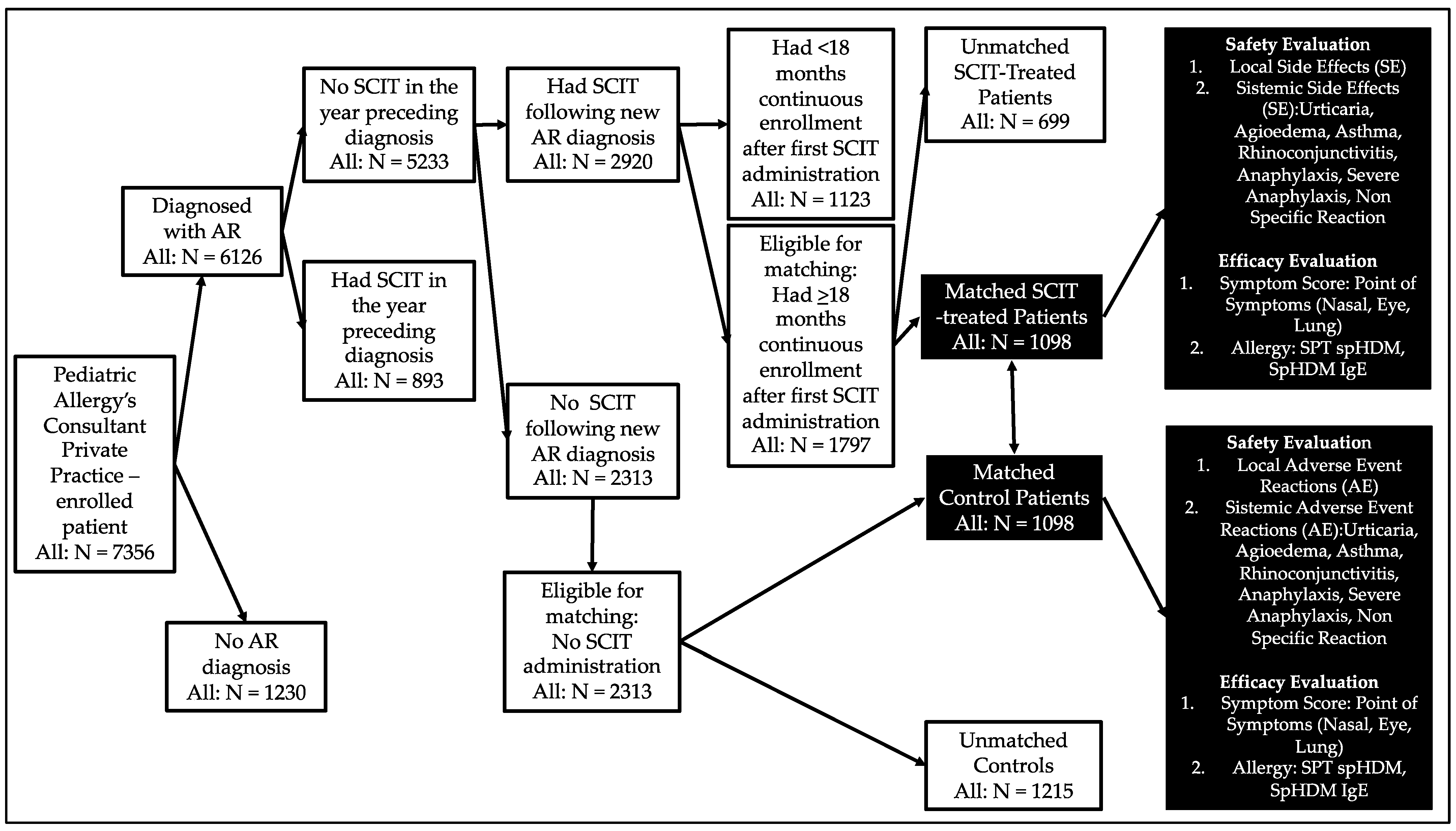
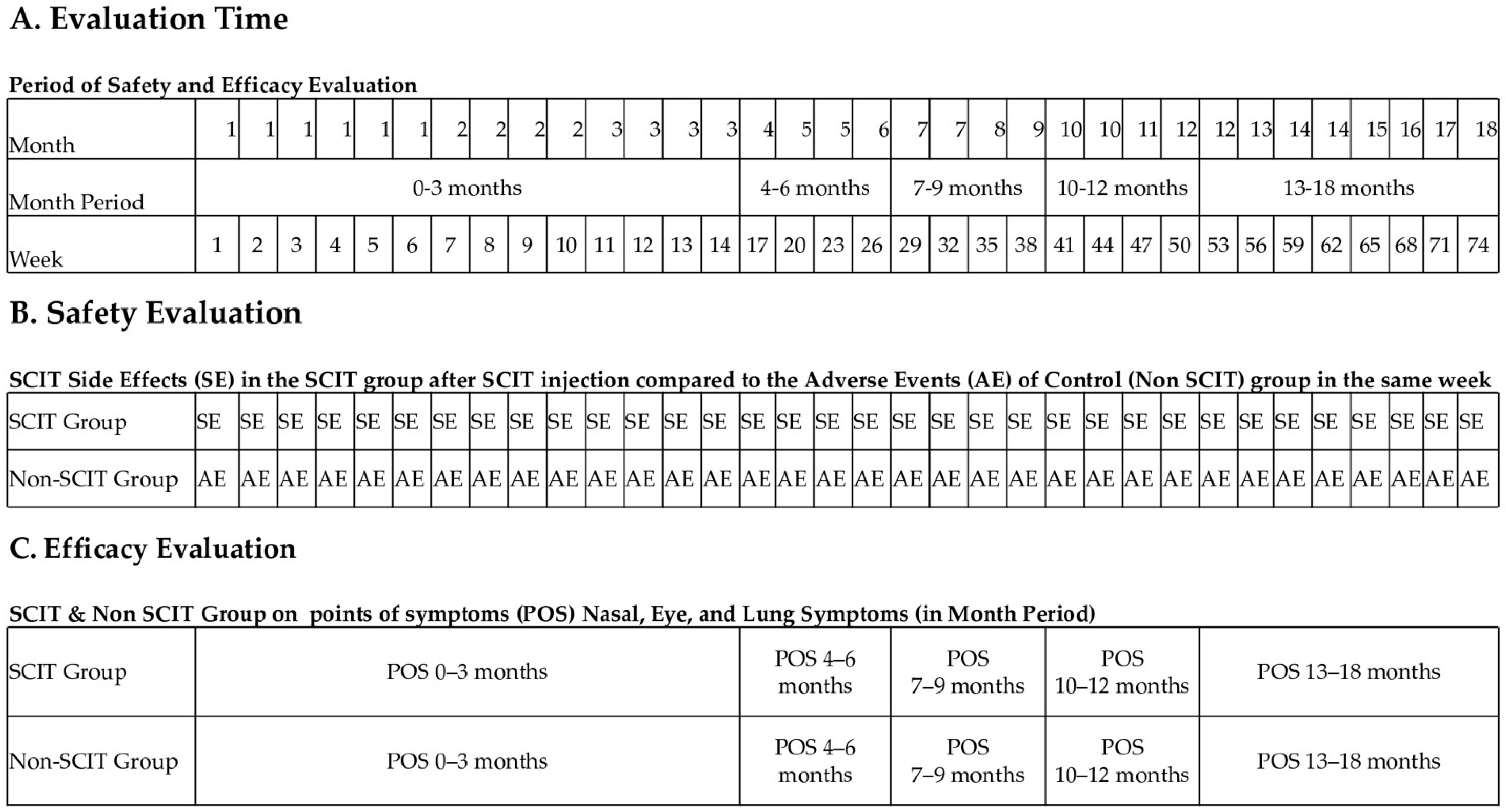
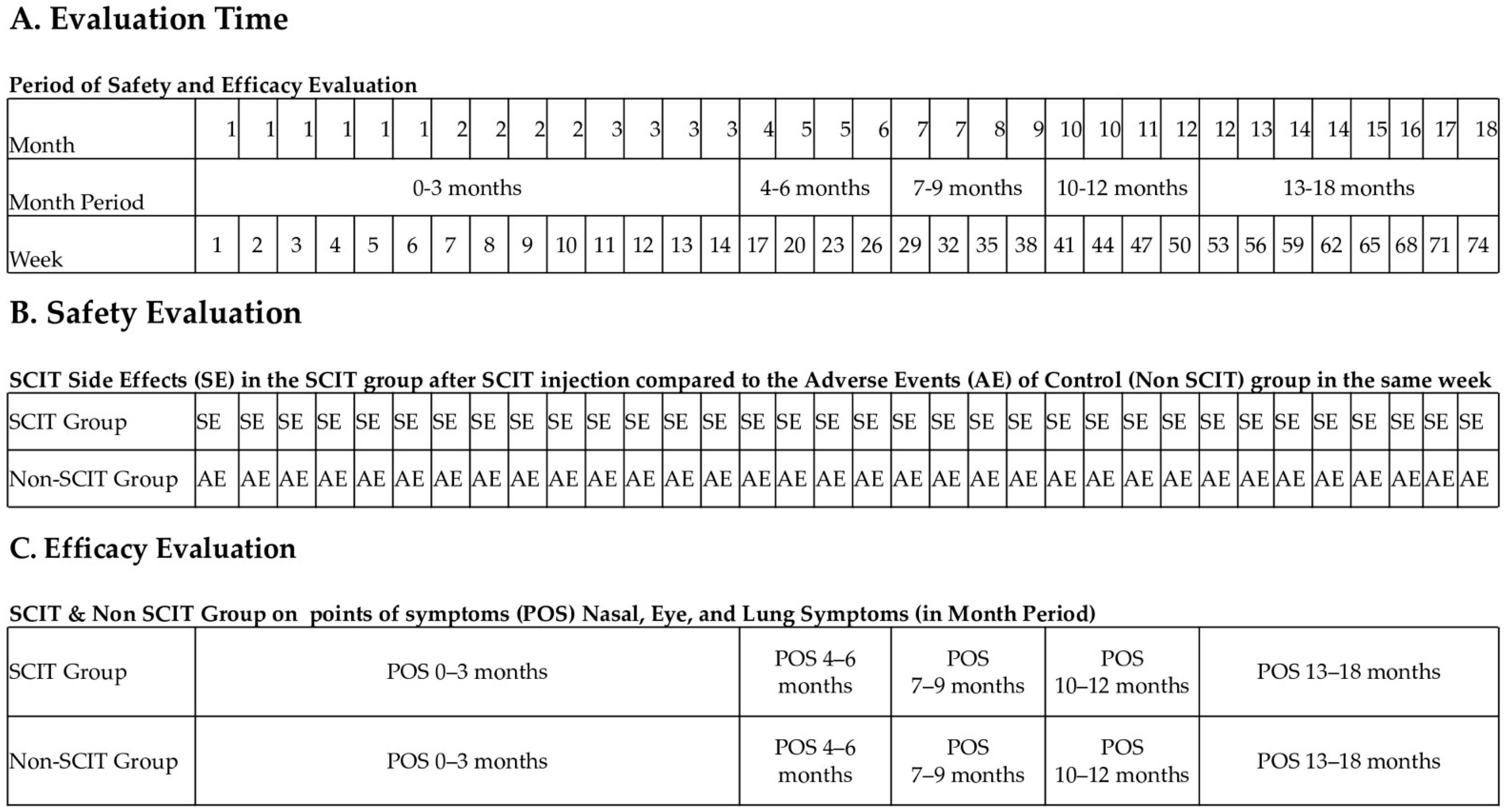
2.2. Study Design
2.3. Materials
2.4. Outcomes
2.5. Statistical Analysis
3. Results
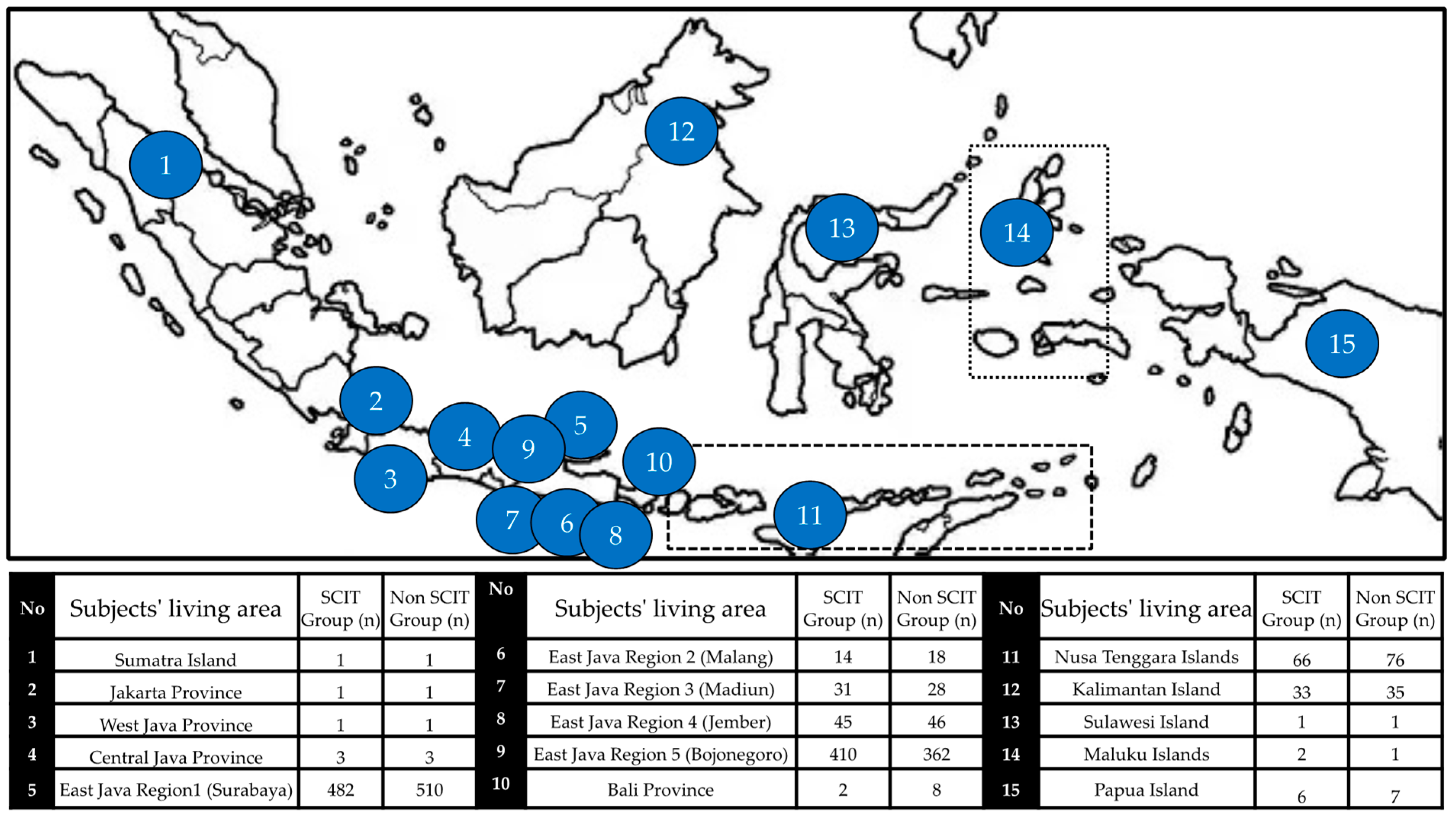
3.1. Baseline Characteristics
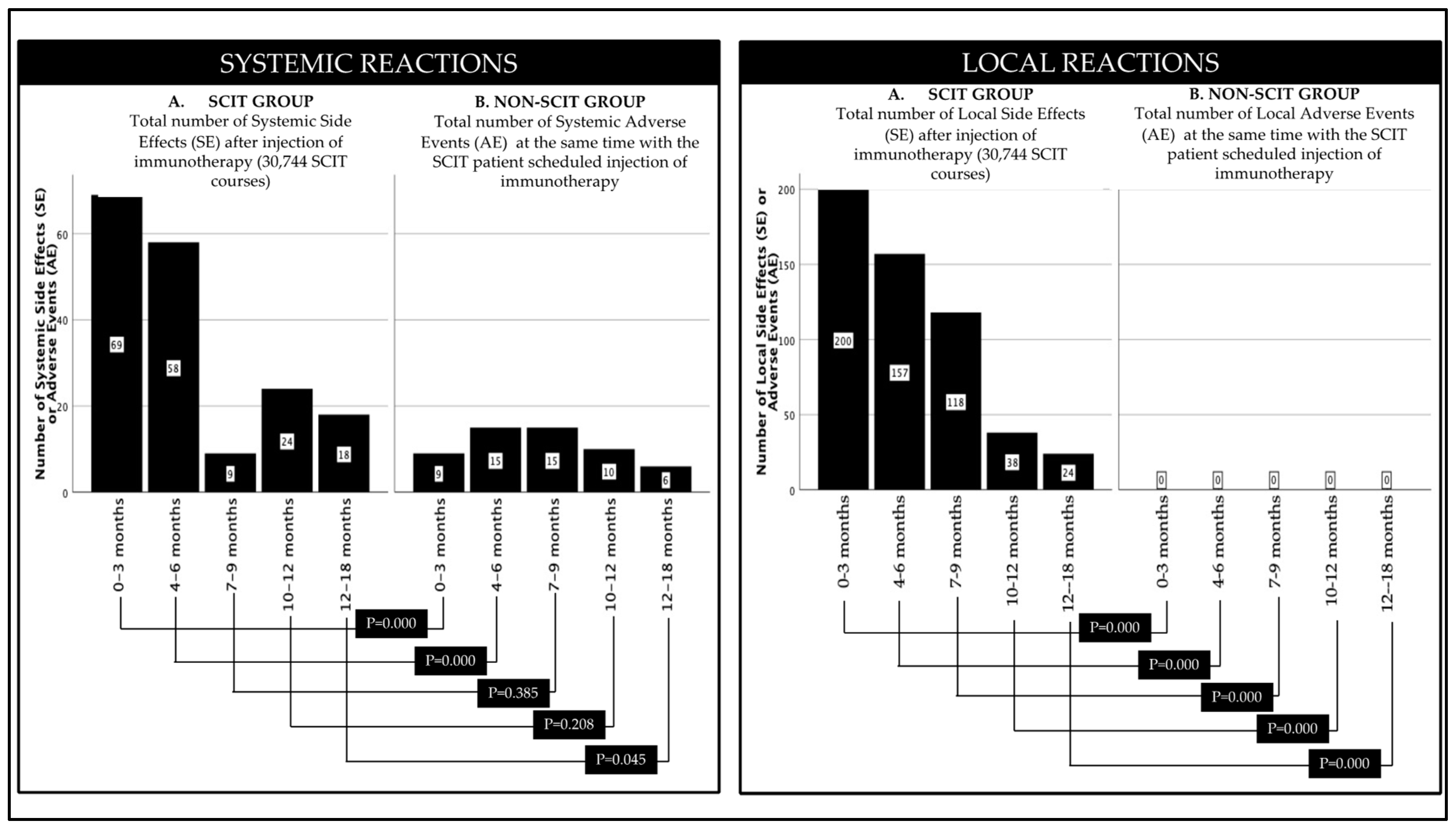
3.2. Safety
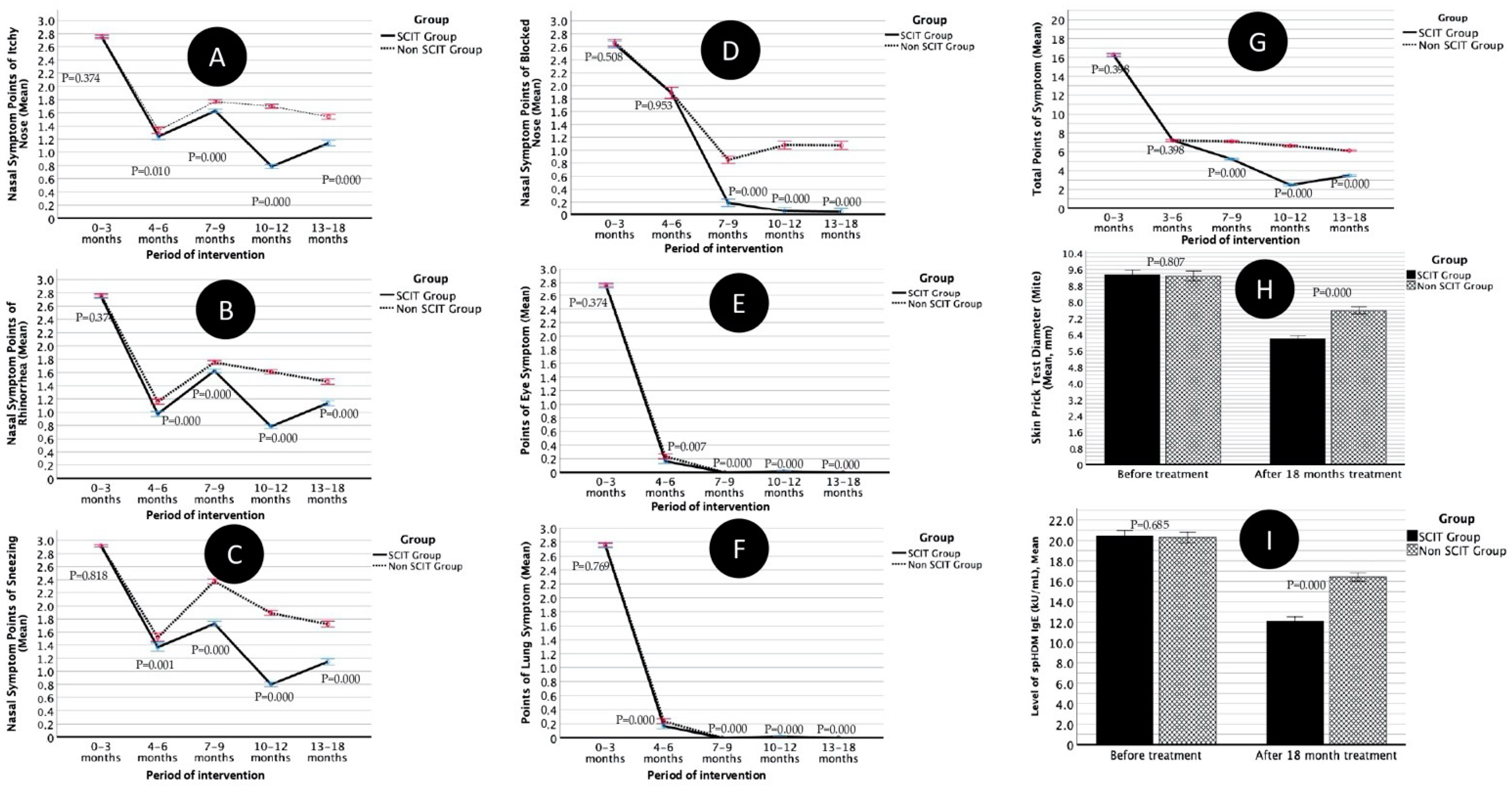
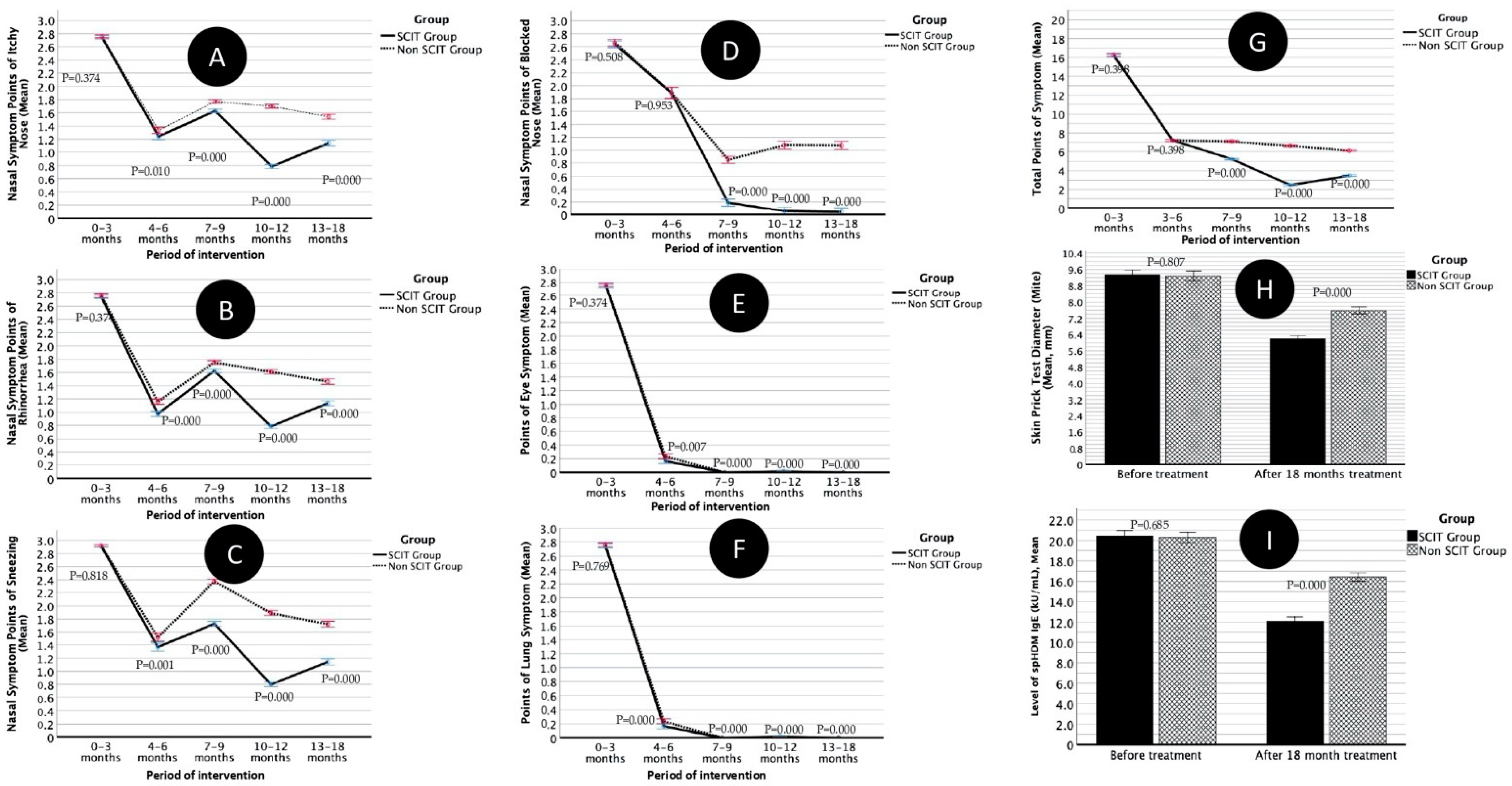
3.3. Efficacy
4. Discussion
Strength and Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Bona, D.; Paoletti, G.; Chu, D.K.; Pepys, J.; Macchia, L.; Heffler, E.; Canonica, G.W. Allergen immunotherapy for respiratory allergy: Quality appraisal of observational comparative effectiveness studies using the REal Life Evidence AssessmeNt Tool. An EAACI methodology committee analysis. Clin. Transl. Allergy 2021, 11, e12033. [Google Scholar] [CrossRef]
- Tosca, M.A.; Licari, A.; Olcese, R.; Castagnoli, R.; Marseglia, A.; Marseglia, G.L.; Miraglia Del Giudice, M.; Martelli, A.; Calvani, M.; Caffarelli, C.; et al. Allergen immunotherapy in children and adolescents with respiratory diseases. Acta Biomed. 2020, 91, e2020006. [Google Scholar] [CrossRef]
- Kim, J.Y.; Hwang, D.; Jang, M.; Rhee, C.S.; Han, D.H. Clinical effectiveness of house dust mite immunotherapy in mono- versus poly-sensitised patients with allergic rhinitis: A systematic review and meta-analysis. Rhinology 2021, 59, 352–359. [Google Scholar] [CrossRef]
- Chen, L.; Lei, L.; Cai, Y.; Li, T. Specific sublingual immunotherapy in children with perennial rhinitis: A systemic review and meta-analysis. Int. Forum Allergy Rhinol. 2020, 10, 1226–1235. [Google Scholar] [CrossRef]
- Roberts, G.; Pfaar, O.; Akdis, C.A.; Ansotegui, I.J.; Durham, S.R.; van Wijk, R.G.; Halken, S.; Larenas-Linnemann, D.; Pawankar, R.; Pitsios, C.; et al. EAACI guidelines on allergen immunotherapy: Allergic rhinoconjunctivitis. Allergy 2018, 73, 765–798. [Google Scholar] [CrossRef] [Green Version]
- Arasi, S.; Corsello, G.; Villani, A.; Pajno, G.B. The future outlook on allergen immunotherapy in children: 2018 and beyond. Ital. J. Pediatr. 2018, 44, 80. [Google Scholar] [CrossRef]
- Halken, S.; Larenas-Linnemann, D.; Roberts, G.; Calderon, M.A.; Angier, E.; Pfaar, O.; Pfaar, O.; Ryan, D.; Agache, I.; Ansotegui, I.J.; et al. EAACI guidelines on allergen immunotherapy: Prevention of allergy. Pediatr. Allergy Immunol. 2017, 28, 728–745. [Google Scholar] [CrossRef]
- Fiocchi, A.; Pajno, G.; La Grutta, S.; Pezzuto, F.; Incorvaia, C.; Sensi, L.; Marcucci, F.; Frati, F. Safety of sublingual-swallow immunotherapy in children aged 3 to 7 years. Ann. Allergy Asthma Immunol. 2005, 95, 254–258. [Google Scholar] [CrossRef] [Green Version]
- Agostinis, F.; Tellarini, L.; Canonica, G.W.; Falagiani, P.; Passalacqua, G. Safety of sublingual immunotherapy with a monomeric allergoid in very young children. Allergy 2005, 60, 133. [Google Scholar] [CrossRef]
- Cox, L.; Aaronson, D.; Casale, T.B.; Honsinger, R.; Weber, R. Allergy immunotherapy safety: Location matters! J. Allergy Clin. Immunol. Pract. 2013, 1, 455–457. [Google Scholar] [CrossRef]
- Sieber, J.; De Geest, S.; Shah-Hosseini, K.; Mosges, R. Medication persistence with long-term, specific grass pollen immunotherapy measured by prescription renewal rates. Curr. Med. Res. Opin. 2011, 27, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Egert-Schmidt, A.M.; Kolbe, J.M.; Mussler, S.; Thum-Oltmer, S. Patients’ compliance with different administration routes for allergen immunotherapy in Germany. Patient Prefer. Adherence 2014, 8, 1475–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiel, A.; Roder, E.; Gerth, R.; van Wijk, M.J.A.L.; Hop, W.C.; Rutten-van Molken, M.P. Real-life compliance and persistence among users of subcutaneous and sublingual allergen immunotherapy. J. Allergy Clin. Immunol. 2013, 132, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Brozek, J.L.; Bousquet, J.; Agache, I.; Agarwal, A.; Bachert, C.; Bosnic-Anticevich, S.; Brignardello-Petersen, R.; Canonica, G.W.; Casale, T.; Chavannes, N.H.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines—2016 revision. J. Allergy Clin. Immunol. 2017, 140, 950–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulet, L.-P.; Reddel, H.K.; Bateman, E.; Pedersen, S.; Fitzgerald, J.M.; O’Byrne, P.M. The Global Initiative for Asthma (GINA): 25 years later. Eur. Respir. J. 2019, 54, 1900598. [Google Scholar] [CrossRef]
- Sugiono, L.T.; Olivianto, E.; Nurdiana; Barlianto, W.; Kusuma, H. The effect of house dust mite immunotherapy, probiotic and Nigella sativa in the number of CD4+ IL-4+ cell, total IgE level and Asthma Control Test (ACT) score. J. Dent. Med. Sci. 2013, 7, 32–39. [Google Scholar]
- Putera, A.M.; Hikmah, Z.; Endaryanto, A.; Irwanto; Maramis, M.M. The role of house dust mite immunotherapy in Indonesian children with chronic rhinosinusitis allergy: A randomized control trial. Heliyon 2021, 7, e06510. [Google Scholar] [CrossRef]
- Putera, A.M.; Endaryanto, A.; Harsono, A. Effect of House Dust Mite Immunotherapy in Indonesian Children with Chronic Sinusitis. J. Int. Dent. Med. Res. 2020, 13, 1651–1658. [Google Scholar]
- Baratawidjaja, I.; Baratawidjaja, P.; Darwis, A.; Yi, F.; Chew, F.; Lee, B.; Baratawidjaja, K. Mites in Jakarta homes. Allergy 1998, 53, 1226–1227. [Google Scholar] [CrossRef]
- Ponggalunggu, W.F.; Pijoh, V.D.; Wahongan, G.J.P. Jenis dan kepadatan tungau debu rumah pada beberapa habitat di rumah penderita penyakit alergi. J. E-Biomedik 2015, 3, 254–260. [Google Scholar] [CrossRef]
- Sani, S.; Gupta, R.; Fonacier, L.; Aquino, M. Risk stratification of systemic reactions to subcutaneous immunotherapy: A retrospective study. Allergy Asthma Proc. 2019, 40, 338–342. [Google Scholar] [CrossRef]
- Muraro, A.; Roberts, G.; Worm, M.; Bilò, M.B.; Brockow, K.; Rivas, M.F.; Santos, A.F.; Zolkipli, Z.Q.; Bellou, A.; Beyer, K.; et al. Anaphylaxis: Guidelines from the European Academy of allergy and clinical Immunology. Allergy 2014, 69, 1026–1045. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Ma, D.; Huang, N.; Li, W.; Jiang, Q.; Wang, Y.; Wang, X.; Yang, L.; Zhu, R. Safety of house dust mite subcutaneous immunotherapy in preschool children with respiratory allergic diseases. Ital. J. Pediatr. 2021, 23, 101. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wu, Y.; Yang, Y.; Huang, N.; Li, W.; Zhang, S.; Jiang, Q.; Yang, L.; Zhu, R. The efficacy and safety of two commercial house dust mite extracts for allergic rhinitis: A head-to-head study. Int. Forum Allergy Rhinol. 2019, 9, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Di Bona, D.; Magistà, S.; Masciopinto, L.; Lovecchio, A.; Loiodice, R.; Bilancia, M.; Albanesi, M.; Caiaffa, M.F.; Nettis, E.; Macchia, L.; et al. Safety and treatment compliance of subcutaneous immunotherapy: A 30-year retrospective study. Respir Med. 2020, 161, 105843. [Google Scholar] [CrossRef] [Green Version]
- Rice, J.L.; Diette, G.B.; Suarez-Cuervo, C.; Brigham, E.P.; Lin, S.Y.; Ramanathan, M.J.; Robinson, K.A.; Azar, A. Allergen-specific immunotherapy in the treatment of pediatric asthma: A systematic review. Pediatrics 2018, 141, e20173833. [Google Scholar] [CrossRef] [Green Version]
- Coop, C.A.; Tankersley, M.S. Patient perceptions regarding local reactions from allergen immunotherapy injections. Ann. Allergy Asthma Immunol. 2008, 101, 96–100. [Google Scholar] [CrossRef]
- Nelson, B.L.; Dupont, L.A.; Reid, M.J. Prospective survey of local and systemic reactions to immunotherapy with pollen extracts. Ann. Allergy 1986, 56, 331–334. [Google Scholar] [CrossRef]
- Kartal, O.; Gulec, M.; Caliskaner, Z.; Musabak, U.; Sener, O. Safety of subcutaneous immunotherapy with inhalant allergen extracts: A single-center 30-year experience from Turkey. Immunopharmacol. Immunotoxicol. 2015, 37, 280–286. [Google Scholar] [CrossRef]
- Webber, C.M.; Calabria, C.W. Assessing the safety of subcutaneous immunotherapy dose adjustments. Ann. Allergy Asthma Immunol. 2010, 105, 369–375. [Google Scholar] [CrossRef]
- DaVeiga, S.P.; Liu, X.; Caruso, K.; Golubski, S.; Xu, M.; Lang, D.M. Systemic reactions associated with subcutaneous allergen immunotherapy: Timing and risk assessment. Ann. Allergy Asthma Immunol. 2011, 106, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, B.; Zhao, Y.; Zhang, Q.; Wan, L.; Liu, J.; Tian, X.; Li, J.; Zhou, G.; Zhang, L.; et al. A prospective multicenter study of systemic reactions in standardized specific immunotherapy for allergic rhinitis in China. Am. J. Rhinol. Allergy 2014, 28, e40–e44. [Google Scholar] [CrossRef] [PubMed]
- Tophof, M.A.; Hermanns, A.; Adelt, T.; Eberle, P.; Gronke, C.; Friedrichs, F.; Knecht, R.; Mönter, E.; Schöpfer, H.; Schwerk, N.; et al. Side effects during subcutaneous immunotherapy in children with allergic diseases. Pediatr. Allergy Immunol. 2018, 29, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Epstein, T.G.; Liss, G.M.; Murphy-Berendts, K.; Bernstein, D.I. Immediate and delayed-onset systemic reactions after subcutaneous immunotherapy injections: ACAAI/AAAAI surveillance study of subcutaneous immunotherapy: Year 2. Ann. Allergy Asthma Immunol. 2011, 107, 426–431. [Google Scholar] [CrossRef]
- Ragusa, F.V.; Passalacqua, G.; Gambardella, R.; Campanari, S.; Barbieri, M.M.; Scordamaglia, A.; Canonica, G.W. Nonfatal systemic reactions to subcutaneous immunotherapy: A 10-year experience. J. Investig. Allergol. Clin. Immunol. 1997, 7, 151–154. [Google Scholar]
- Ragusa, V.F.; Massolo, A. Non-fatal systemic reactions to subcutaneous immunotherapy: A 20-year experience comparison of two 10-year periods. Allerg. Immunol. 2004, 36, 52–55. [Google Scholar]
- Amin, H.S.; Liss, G.M.; Bernstein, D.I. Evaluation of near-fatal reactions to allergen immunotherapy injections. J. Allergy Clin. Immunol. 2006, 117, 169–175. [Google Scholar] [CrossRef]
- Phillips, J.F.; Lockey, R.F.; Fox, R.W.; Ledford, D.K.; Glaum, M.C. Systemic reactions to subcutaneous allergen immunotherapy and the response to epinephrine. Allergy Asthma Proc. 2011, 32, 288–294. [Google Scholar] [CrossRef]
- Epstein, T.G.; Liss, G.M.; Murphy-Berendts, K.; Bernstein, D.I. AAAAI and ACAAI surveillance study of subcutaneous immunotherapy, year 3: What practices modify the risk of systemic reactions? Ann. Allergy Asthma Immunol. 2013, 110, 274–278. [Google Scholar] [CrossRef]
- Epstein, T.G.; Liss, G.M.; Murphy-Berendts, K.; Bernstein, D.I. Risk factors for fatal and nonfatal reactions to subcutaneous immunotherapy: National surveillance study on allergen immunotherapy (2008–2013). Ann. Allergy Asthma Immunol. 2016, 116, 354–359. [Google Scholar] [CrossRef]
- Sánchez-Borges, M.; Bernstein, D.I.; Calabria, C. Subcutaneous Immunotherapy Safety. Immunol. Allergy Clin. N. Am. 2020, 40, 25–39. [Google Scholar] [CrossRef]
- Bernstein, D.I.; Wanner, M.; Borish, L.; Liss, G.M.; the Immunotherapy Committee of the American Academy of Allergy, Asthma and Immunology. Twelve-year survey of fatal reactions to allergen injections and skin testing: 1990–2001. J. Allergy Clin. Immunol. 2004, 113, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-L.; Ning, W.-X.; Li, S.-X.; Xu, Y.-C.; Wu, L.; Wang, Y.-S.; Xu, X.-F.; Jiang, Y.; Sheng, Y.-J.; Zhou, Y.-L.; et al. The safety profile of subcutaneous allergen immunotherapy in children with asthma in Hangzhou, East China. Allergol. Immunopathol. (Madr.) 2017, 45, 541–548. [Google Scholar] [CrossRef]
- Yu, C.L.; Huang, W.T.; Wang, C.M. Treatment of allergic rhinitis reduces acute asthma exacerbation risk among asthmatic children aged 2–18 years. J. Microbiol. Immunol. Infect. 2019, 52, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.; Nelson, H.; Lockey, R.; Calabria, C.; Chacko, T.; Finegold, I.; Nelson, M.; Weber, R.; Bernstein, D.I.; Blessing-Moore, J.; et al. Allergen immunotherapy: A practice parameter third update. J. Allergy Clin. Immunol. 2011, 127, S1–S55. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | SCIT Group (n = 1.098) | Control Group (n = 1.098) | p | ||
|---|---|---|---|---|---|
| Age (years), mean (SD) | 5.5 | (3.51) | 5.4 | (3.32) | 0.465 |
| Sex, n (%) | |||||
| Male | 696 | (63.4) | 704 | (64.1) | 0.722 |
| Female | 402 | (36.6) | 394 | (35.9) | |
| AR-associated conditions, n (%) | |||||
| Asthma, n (%) | 593 | (54.0) | 396 | (36.1) | 0.000 |
| Bronchitis, n (%) | 431 | (39.3) | 700 | (63.8) | 0.000 |
| Atopic dermatitis, n (%) | 100 | (9.1) | 85 | (7.7) | 0.249 |
| Sinusitis, n (%) | 12 | (1.1) | 106 | (9.7) | 0.000 |
| Conjunctivitis, n (%) | 3 | (0.3) | 0 | (0.0) | 0.083 |
| GI Problem, n (%) | 7 | (0.6) | 3 | (0.3) | 0.205 |
| Urticaria, n (%) | 14 | (1.3) | 20 | (1.8) | 0.300 |
| Nutrition Status | |||||
| BW (kgs), mean (SD) | 12.8 | (2.35) | 12.7 | (2.33) | 0.761 |
| BH (cm), mean (SD) | 84.7 | (19.84) | 84.2 | (19.24) | 0.530 |
| % BW/Age | 82.3 | (3.29) | 82.3 | (3.26) | 0.938 |
| % BH/Age | 77.9 | (4.11) | 77.9 | (4.07) | 0.938 |
| Geographic region, n (%) | |||||
| East Java Region 5 (Bojonegoro) | 410 | (37.3) | 362 | (32.9) | 0.325 |
| East Java Region 4 (Jember) | 45 | (4.1) | 46 | (4.2) | |
| East Java Region 3 (Madiun) | 31 | (2.8) | 28 | (2.5) | |
| East Java Region 2 (Malang) | 14 | (1.3) | 18 | (1.5) | |
| East Java Region 1 (Surabaya) | 482 | (43.9) | 510 | (46.4) | |
| Outer Geographic Region | 115 | (10.5) | 138 | (12.5) | |
| Symptom score (SS) before treatment, mean (SD) | 2.7 | (0.48) | 2.7 | (0.45) | 0.398 |
| Skin prick test diameter (mite) before treatment (mm), mean (SD) | 9.3 | (4.17) | 9.3 | (4.15) | 0.807 |
| spHDM IgE (kU/mL), mean (SD) before treatment (checked randomly by 10% of the total sample) | 20.5 | (8.75) | 20.3 | (8.66) | 0.685 |
| Side Effects (SE) | Total Number of Side Effects (SE) after Injection of Immunotherapy (30,744 SCIT Courses) | Total Patients with SE (N SCIT Group = 1098) | Mean of SE/Subject Who Experience SE | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0–3 Months | 4–6 Months | 7–9 Months | 10–12 Months | 13–18 Months | Total 0–18 Months | |||||
| n | % | n | % | |||||||
| 1. Local | 195 | 156 | 117 | 38 | 24 | 530 | 1.72 | 195 | 17.76 | 2.72 |
| 2. Urticaria | 27 | 3 | 0 | 24 | 0 | 54 | 0.18 | 27 | 2.46 | 2.00 |
| 3. Angioedema | 1 | 0 | 1 | 0 | 0 | 2 | 0.01 | 2 | 0.18 | 1.00 |
| 4. Asthma | 9 | 9 | 7 | 0 | 7 | 32 | 0.10 | 16 | 1.46 | 2.00 |
| 5. Rhinoconjungtivitis | 11 | 19 | 0 | 0 | 0 | 30 | 0.10 | 19 | 1.73 | 1.58 |
| 6. Nonspecific | 0 | 11 | 0 | 0 | 11 | 22 | 0.07 | 11 | 1.00 | 2.00 |
| 7. Anaphylaxis | 15 | 15 | 0 | 0 | 0 | 30 | 0.10 | 15 | 1.37 | 2.00 |
| 8. Severe anaphylaxis | 1 | 0 | 0 | 0 | 0 | 1 | 0.00 | 1 | 0.09 | 1.00 |
| 9. Local and systemic | 5 | 1 | 1 | 0 | 0 | 7 | 0.02 | 1 | 0.09 | 7.00 |
| 10. Total local | 200 | 157 | 118 | 38 | 24 | 537 | 1.75 | 196 | 17.85 | 2.74 |
| 11. Total systemic | 69 | 42 | 9 | 24 | 18 | 162 | 0.53 | 92 | 8.38 | 1.76 |
| Total Side Effects (SE) | 269 | 199 | 127 | 62 | 42 | 699 | 2.27 | 284 | 25.87 | 2.46 |
| Adverse Events (AE) | Total Number of Adverse Events (AE) of Non-SCIT Patients at the Same Time with the SCIT-Patient Scheduled Injection of Immunotherapy | Total Patients with AE (N Non-SCIT Group = 1098) | Mean of AE/Subject Who Experience AE | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0–3 Months | 4–6 Months | 7–9 Months | 10–12 Months | 13–18 Months | Total 0–18 Months | |||||
| n | % | n | % | |||||||
| 1. Local | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 2. Urticaria | 1 | 0 | 0 | 0 | 1 | 2 | 0.01 | 1 | 0.09 | 2 |
| 3. Angioedema | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 4. Asthma | 3 | 7 | 2 | 1 | 0 | 13 | 0.04 | 4 | 0.36 | 3.25 |
| 5. Rhinoconjungtivitis | 5 | 8 | 13 | 9 | 5 | 40 | 0.13 | 13 | 1.18 | 3.08 |
| 6. Nonspecific | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 7. Anaphylaxis | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 8. Severe anaphylaxis | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 9. Local and systemic | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 10. Total local | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 11. Total systemic | 9 | 15 | 15 | 1 | 6 | 46 | 0.15 | 18 | 1.64 | 2.56 |
| Total Adverse Events (AE) | 9 | 15 | 15 | 1 | 6 | 46 | 0.15 | 18 | 1.64 | 2.56 |
| Medication Score (MS), Mean (SD) | SCIT Group (n = 1.098) | Control Group (n = 1.098) | p | ||
|---|---|---|---|---|---|
| 0–3 months | 2.6 | (0.48) | 2.6 | (0.48) | 0.860 |
| 4–6 months | 1.7 | (0.53) | 2.4 | (0.48) | 0.000 |
| 7–12 months | 0.8 | (0.61) | 2.2 | (0.69) | 0.000 |
| 13–18 months | 0.4 | (0.59) | 2.2 | (0.69) | 0.000 |
| Difference Before-After | 2.3 | (0.59) | 0.4 | (0.49) | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Endaryanto, A.; Nugraha, R.A. Safety Profile and Issues of Subcutaneous Immunotherapy in the Treatment of Children with Allergic Rhinitis. Cells 2022, 11, 1584. https://doi.org/10.3390/cells11091584
Endaryanto A, Nugraha RA. Safety Profile and Issues of Subcutaneous Immunotherapy in the Treatment of Children with Allergic Rhinitis. Cells. 2022; 11(9):1584. https://doi.org/10.3390/cells11091584
Chicago/Turabian StyleEndaryanto, Anang, and Ricardo Adrian Nugraha. 2022. "Safety Profile and Issues of Subcutaneous Immunotherapy in the Treatment of Children with Allergic Rhinitis" Cells 11, no. 9: 1584. https://doi.org/10.3390/cells11091584
APA StyleEndaryanto, A., & Nugraha, R. A. (2022). Safety Profile and Issues of Subcutaneous Immunotherapy in the Treatment of Children with Allergic Rhinitis. Cells, 11(9), 1584. https://doi.org/10.3390/cells11091584