
Cerebral Biomarkers and Blood-Brain Barrier Integrity in Preeclampsia

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Collection
2.3. Biomarker Assay
2.4. hCMEC/D3 In Vitro Model
2.5. Statistical Analyses
3. Results
3.1. Background Characteristics
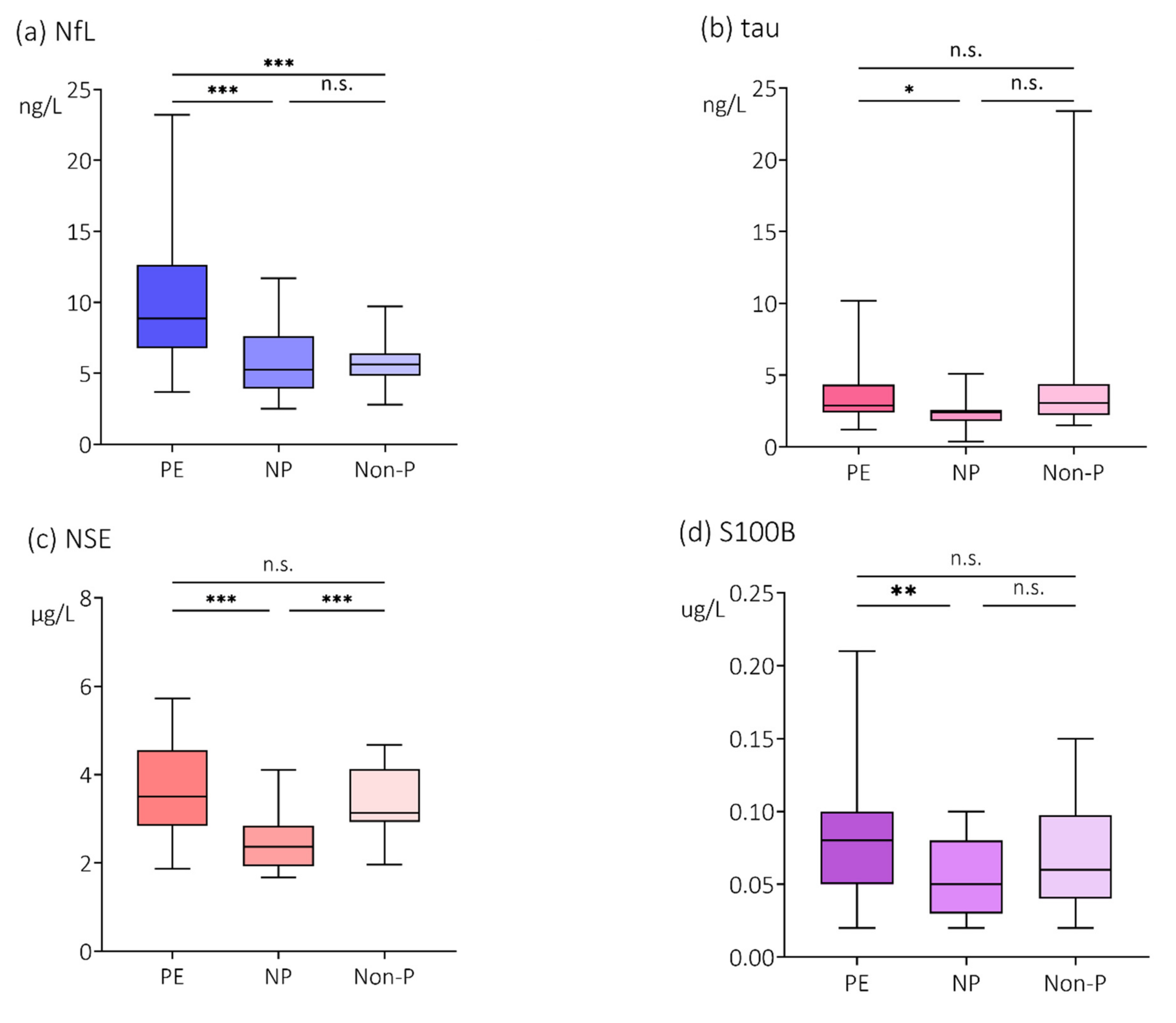
3.2. Plasma Concentrations of NfL, Tau, NSE and S100B
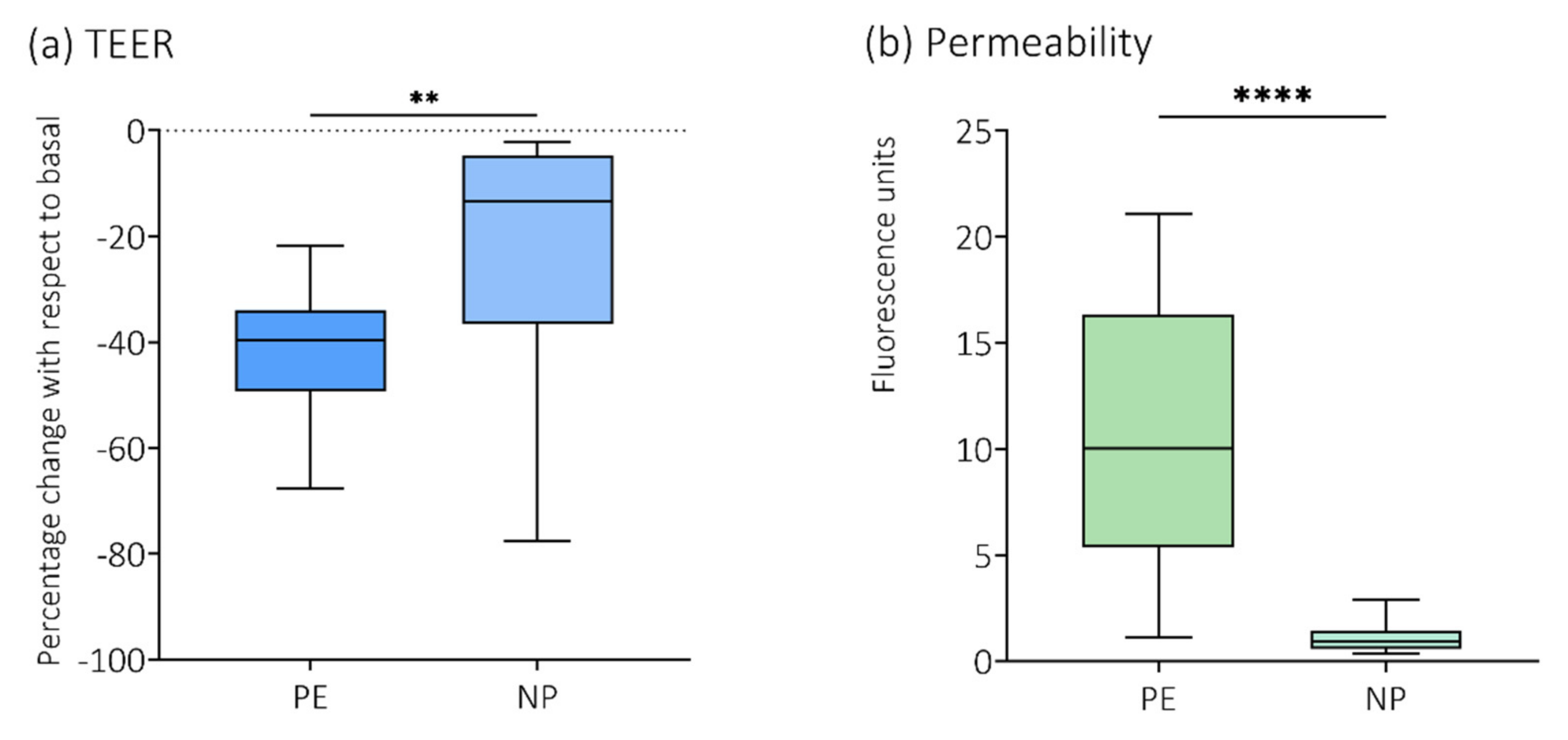
3.3. Effects of Plasma on TEER in an In Vitro BBB Model
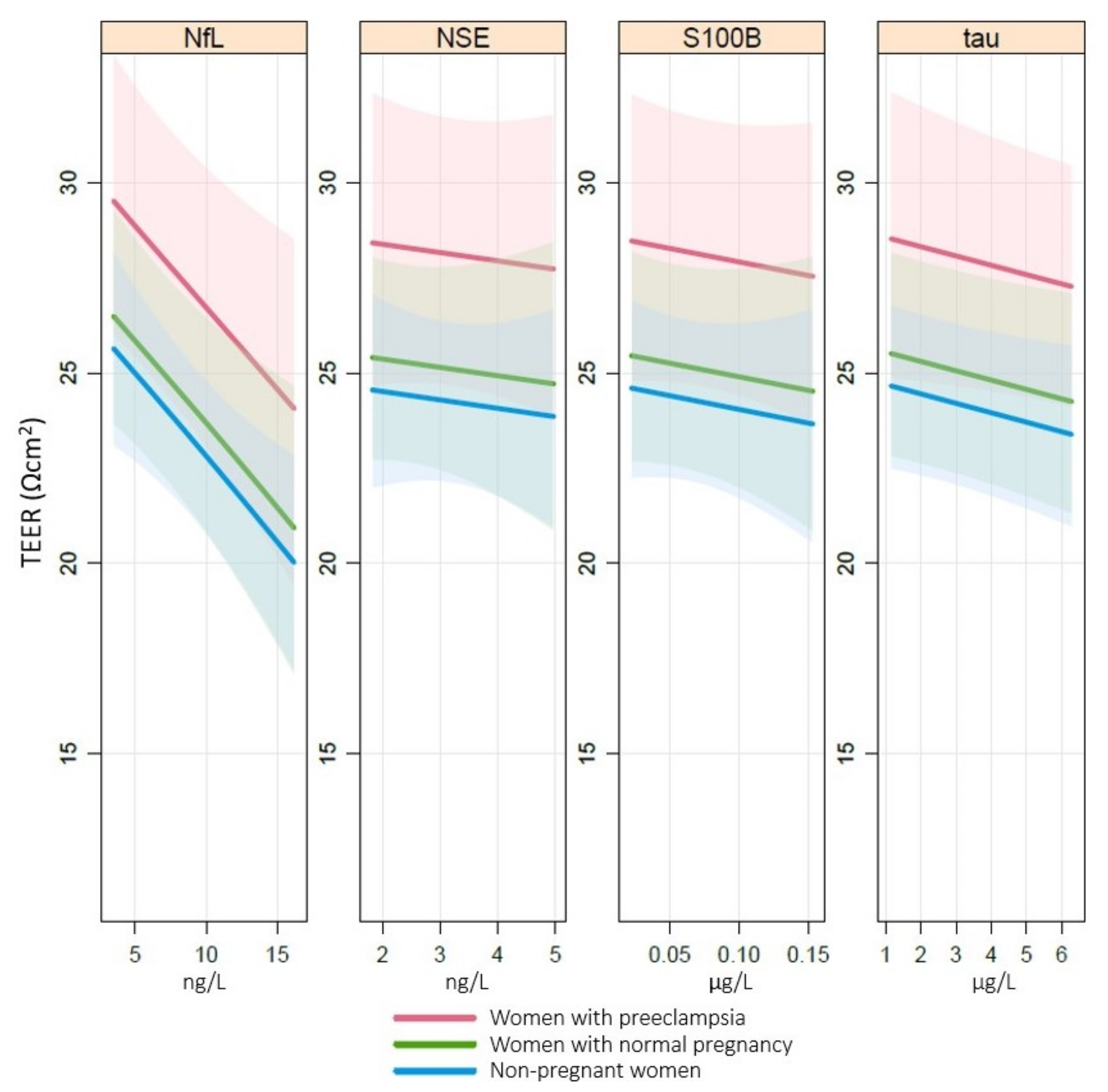
3.4. Association of NfL, Tau, NSE and S100B with TEER
3.5. Subgroup Analyses of Neurological Symptoms in the Women with Preeclampsia
4. Discussion
4.1. Main Findings
4.2. Research Implications
4.3. Strengths and Limitations
4.4. Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chappell, L.C.; Cluver, C.A.; Kingdom, J.; Tong, S. Pre-eclampsia. Lancet 2021, 398, 341–354. [Google Scholar] [CrossRef]
- Tranquilli, A.L.; Dekker, G.; Magee, L.; Roberts, J.; Sibai, B.M.; Steyn, W.; Zeeman, G.G.; Brown, M.A. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens. 2014, 4, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S.; et al. Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations for International Practice. Hypertension 2018, 72, 24–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKay, A.P.; Berg, C.J.; Atrash, H.K. Pregnancy-related mortality from preeclampsia and eclampsia. Obstet. Gynecol. 2001, 97, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Say, L.; Chou, D.; Gemmill, A.; Tuncalp, O.; Moller, A.B.; Daniels, J.; Gulmezoglu, A.M.; Temmerman, M.; Alkema, L. Global causes of maternal death: A WHO systematic analysis. Lancet Glob. Health 2014, 2, e323–e333. [Google Scholar] [CrossRef] [Green Version]
- Hastie, R.; Brownfoot, F.C.; Cluver, C.A.; Walker, S.P.; Hesselman, S.; Tong, S.; Bergman, L. Predictive Value of the Signs and Symptoms Preceding Eclampsia: A Systematic Review. Obstet. Gynecol. 2019. [Google Scholar] [CrossRef]
- Donato, R.; Cannon, B.R.; Sorci, G.; Riuzzi, F.; Hsu, K.; Weber, D.J.; Geczy, C.L. Functions of S100 proteins. Curr. Mol. Med. 2013, 13, 24–57. [Google Scholar] [CrossRef] [Green Version]
- Rohrer, J.D.; Woollacott, I.O.; Dick, K.M.; Brotherhood, E.; Gordon, E.; Fellows, A.; Toombs, J.; Druyeh, R.; Cardoso, M.J.; Ourselin, S.; et al. Serum neurofilament light chain protein is a measure of disease intensity in frontotemporal dementia. Neurology 2016, 87, 1329–1336. [Google Scholar] [CrossRef] [Green Version]
- Avila, J.; Lucas, J.J.; Perez, M.; Hernandez, F. Role of tau protein in both physiological and pathological conditions. Physiol. Rev. 2004, 84, 361–384. [Google Scholar] [CrossRef]
- Bogoslovsky, T.; Gill, J.; Jeromin, A.; Davis, C.; Diaz-Arrastia, R. Fluid Biomarkers of Traumatic Brain Injury and Intended Context of Use. Diagnostics 2016, 6, 37. [Google Scholar] [CrossRef]
- Marchi, N.; Rasmussen, P.; Kapural, M.; Fazio, V.; Kight, K.; Mayberg, M.R.; Kanner, A.; Ayumar, B.; Albensi, B.; Cavaglia, M.; et al. Peripheral markers of brain damage and blood-brain barrier dysfunction. Restor. Neurol. Neurosci. 2003, 21, 109–121. [Google Scholar] [PubMed]
- Chou, S.H.; Robertson, C.S.; the Participants in the International Multi-disciplinary Consensus Conference on the Multimodality Monitoring. Monitoring biomarkers of cellular injury and death in acute brain injury. Neurocrit. Care 2014, 21 (Suppl. S2), S187–S214. [Google Scholar] [CrossRef] [PubMed]
- Randall, J.; Mortberg, E.; Provuncher, G.K.; Fournier, D.R.; Duffy, D.C.; Rubertsson, S.; Blennow, K.; Zetterberg, H.; Wilson, D.H. Tau proteins in serum predict neurological outcome after hypoxic brain injury from cardiac arrest: Results of a pilot study. Resuscitation 2013, 84, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Stefanovic, B.; Duric, O.; Stankovic, S.; Mijatovic, S.; Doklestic, K.; Stefanovic, B.; Jovanovic, B.; Marjanovic, N.; Kalezic, N. Elevated Serum Protein S100B and Neuron Specific Enolase Values as Predictors of Early Neurological Outcome After Traumatic Brain Injury. J. Med. Biochem. 2017, 36, 314–321. [Google Scholar] [CrossRef] [Green Version]
- Marchi, N.; Cavaglia, M.; Fazio, V.; Bhudia, S.; Hallene, K.; Janigro, D. Peripheral markers of blood-brain barrier damage. Clin. Chim. Acta 2004, 342, 1–12. [Google Scholar] [CrossRef]
- Evers, K.S.; Atkinson, A.; Barro, C.; Fisch, U.; Pfister, M.; Huhn, E.A.; Lapaire, O.; Kuhle, J.; Wellmann, S. Neurofilament as Neuronal Injury Blood Marker in Preeclampsia. Hypertension 2018, 71, 1178–1184. [Google Scholar] [CrossRef]
- Bergman, L.; Zetterberg, H.; Kaihola, H.; Hagberg, H.; Blennow, K.; Akerud, H. Blood-based cerebral biomarkers in preeclampsia: Plasma concentrations of NfL, tau, S100B and NSE during pregnancy in women who later develop preeclampsia—A nested case control study. PLoS ONE 2018, 13, e0196025. [Google Scholar] [CrossRef]
- Bergman, L.; Akerud, H. Plasma Levels of the Cerebral Biomarker, Neuron-Specific Enolase, are Elevated During Pregnancy in Women Developing Preeclampsia. Reprod. Sci. 2016, 23, 395–400. [Google Scholar] [CrossRef]
- Bergman, L.; Akhter, T.; Wikstrom, A.K.; Wikstrom, J.; Naessen, T.; Akerud, H. Plasma levels of S100B in preeclampsia and association with possible central nervous system effects. Am. J. Hypertens. 2014, 27, 1105–1111. [Google Scholar] [CrossRef] [Green Version]
- Vettorazzi, J.; Torres, F.V.; de Avila, T.T.; Martins-Costa, S.H.; Souza, D.O.; Portela, L.V.; Ramos, J.G. Serum S100B in pregnancy complicated by preeclampsia: A case-control study. Pregnancy Hypertens. 2012, 2, 101–105. [Google Scholar] [CrossRef]
- Bergman, L.; Akerud, H.; Wikstrom, A.K.; Larsson, M.; Naessen, T.; Akhter, T. Cerebral Biomarkers in Women With Preeclampsia Are Still Elevated 1 Year Postpartum. Am. J. Hypertens. 2016, 29, 1374–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, A.P.; Tort, A.B.; Amaral, O.B.; Schmidt, A.P.; Walz, R.; Vettorazzi-Stuckzynski, J.; Martins-Costa, S.H.; Ramos, J.G.; Souza, D.O.; Portela, L.V. Serum S100B in pregnancy-related hypertensive disorders: A case-control study. Clin. Chem. 2004, 50, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Artunc-Ulkumen, B.; Guvenc, Y.; Goker, A.; Gozukara, C. Maternal Serum S100-B, PAPP-A and IL-6 levels in severe preeclampsia. Arch. Gynecol Obs. 2015, 292, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Cipolla, M.J. Cerebrovascular function in pregnancy and eclampsia. Hypertension 2007, 50, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Hammer, E.S.; Cipolla, M.J. Cerebrovascular Dysfunction in Preeclamptic Pregnancies. Curr. Hypertens. Rep. 2015, 17, 64. [Google Scholar] [CrossRef] [Green Version]
- Amburgey, O.A.; Chapman, A.C.; May, V.; Bernstein, I.M.; Cipolla, M.J. Plasma from preeclamptic women increases blood-brain barrier permeability: Role of vascular endothelial growth factor signaling. Hypertension 2010, 56, 1003–1008. [Google Scholar] [CrossRef] [Green Version]
- Weksler, B.; Romero, I.A.; Couraud, P.O. The hCMEC/D3 cell line as a model of the human blood brain barrier. Fluids Barriers CNS 2013, 10, 16. [Google Scholar] [CrossRef] [Green Version]
- Rahman, N.A.; Rasil, A.; Meyding-Lamade, U.; Craemer, E.M.; Diah, S.; Tuah, A.A.; Muharram, S.H. Immortalized endothelial cell lines for in vitro blood-brain barrier models: A systematic review. Brain Res. 2016, 1642, 532–545. [Google Scholar] [CrossRef]
- Deli, M.A.; Abraham, C.S.; Kataoka, Y.; Niwa, M. Permeability studies on in vitro blood-brain barrier models: Physiology, pathology, and pharmacology. Cell. Mol. Neurobiol. 2005, 25, 59–127. [Google Scholar] [CrossRef]
- Bergman, L.; Acurio, J.; Leon, J.; Gatu, E.; Friis, T.; Nelander, M.; Wikstrom, J.; Larsson, A.; Lara, E.; Aguayo, C.; et al. Preeclampsia and increased permeability over the blood brain barrier—A role of vascular endothelial growth receptor 2. Am. J. Hypertens. 2020. [Google Scholar] [CrossRef]
- León, J.; Acurio, J.; Bergman, L.; López, J.; Wikström, A.-K.; Torres-Vergara, P.; Troncoso, F.; Castro, F.O.; Vatish, M.; Escudero, C. Disruption of the Blood-Brain Barrier by Extracellular Vesicles From Preeclampsia Plasma and Hypoxic Placentae: Attenuation by Magnesium Sulfate. Hypertension 2021. [Google Scholar] [CrossRef]
- Tranquilli, A.L.; Brown, M.A.; Zeeman, G.G.; Dekker, G.; Sibai, B.M. The definition of severe and early-onset preeclampsia. Statements from the International Society for the Study of Hypertension in Pregnancy (ISSHP). Pregnancy Hypertens. 2013, 3, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Marsal, K.; Persson, P.H.; Larsen, T.; Lilja, H.; Selbing, A.; Sultan, B. Intrauterine growth curves based on ultrasonically estimated foetal weights. Acta Paediatr. 1996, 85, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Nelander, M.; Weis, J.; Bergman, L.; Larsson, A.; Wikstrom, A.K.; Wikstrom, J. Cerebral Magnesium Levels in Preeclampsia; A Phosphorus Magnetic Resonance Spectroscopy Study. Am. J. Hypertens. 2017, 30, 667–672. [Google Scholar] [CrossRef]
- Mattsson, N.; Zetterberg, H.; Janelidze, S.; Insel, P.S.; Andreasson, U.; Stomrud, E.; Palmqvist, S.; Baker, D.; Tan Hehir, C.A.; Jeromin, A.; et al. Plasma tau in Alzheimer disease. Neurology 2016, 87, 1827–1835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Q.; Shepherd, B.E.; Li, C.; Harrell, F.E., Jr. Modeling continuous response variables using ordinal regression. Stat. Med. 2017, 36, 4316–4335. [Google Scholar] [CrossRef] [PubMed]
- R: A Language and Environment for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 26 December 2021).
- Harrell, F.E., Jr. rms: Regression Modeling Strategies. R Package Version 6.2-0. Available online: https://CRAN.R-project.org/package=rms (accessed on 26 December 2021).
- Simani, L.; Sadeghi, M.; Ryan, F.; Dehghani, M.; Niknazar, S. Elevated Blood-Based Brain Biomarker Levels in Patients with Epileptic Seizures: A Systematic Review and Meta-analysis. ACS Chem. Neurosci. 2020, 11, 4048–4059. [Google Scholar] [CrossRef]
- Kalm, M.; Bostrom, M.; Sandelius, A.; Eriksson, Y.; Ek, C.J.; Blennow, K.; Bjork-Eriksson, T.; Zetterberg, H. Serum concentrations of the axonal injury marker neurofilament light protein are not influenced by blood-brain barrier permeability. Brain Res. 2017, 1668, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Uher, T.; McComb, M.; Galkin, S.; Srpova, B.; Oechtering, J.; Barro, C.; Tyblova, M.; Bergsland, N.; Krasensky, J.; Dwyer, M.; et al. Neurofilament levels are associated with blood-brain barrier integrity, lymphocyte extravasation, and risk factors following the first demyelinating event in multiple sclerosis. Mult. Scler. 2021, 27, 220–231. [Google Scholar] [CrossRef]
- Andersson, M.; Oras, J.; Thorn, S.E.; Karlsson, O.; Kalebo, P.; Zetterberg, H.; Blennow, K.; Bergman, L. Signs of neuroaxonal injury in preeclampsia-A case control study. PLoS ONE 2021, 16, e0246786. [Google Scholar] [CrossRef]
- Burwick, R.M.; Togioka, B.M.; Speranza, R.J.; Gaffney, J.E.; Roberts, V.H.J.; Frias, A.E.; Rincon, M. Assessment of blood-brain barrier integrity and neuroinflammation in preeclampsia. Am. J. Obs. Gynecol. 2019, 221, 269.e1–269.e8. [Google Scholar] [CrossRef] [PubMed]
- Helms, H.C.; Abbott, N.J.; Burek, M.; Cecchelli, R.; Couraud, P.O.; Deli, M.A.; Forster, C.; Galla, H.J.; Romero, I.A.; Shusta, E.V.; et al. In vitro models of the blood-brain barrier: An overview of commonly used brain endothelial cell culture models and guidelines for their use. J. Cereb. Blood Flow Metab. 2016, 36, 862–890. [Google Scholar] [CrossRef] [PubMed]
- van Veen, T.R.; Panerai, R.B.; Haeri, S.; Singh, J.; Adusumalli, J.A.; Zeeman, G.G.; Belfort, M.A. Cerebral autoregulation in different hypertensive disorders of pregnancy. Am. J. Obs. Gynecol. 2015, 212, 513.e1–513.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, A.C.; Tremble, S.M.; Chan, S.L.; Moseley, J.; LaMarca, B.; Nagle, K.J.; Cipolla, M.J. Magnesium sulfate treatment reverses seizure susceptibility and decreases neuroinflammation in a rat model of severe preeclampsia. PLoS ONE 2014, 9, e113670. [Google Scholar] [CrossRef]
- Uwamori, H.; Ono, Y.; Yamashita, T.; Arai, K.; Sudo, R. Comparison of organ-specific endothelial cells in terms of microvascular formation and endothelial barrier functions. Microvasc. Res. 2019, 122, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Haseloff, R.F.; Dithmer, S.; Winkler, L.; Wolburg, H.; Blasig, I.E. Transmembrane proteins of the tight junctions at the blood-brain barrier: Structural and functional aspects. Semin. Cell Dev. Biol. 2015, 38, 16–25. [Google Scholar] [CrossRef]
- Keaney, J.; Campbell, M. The dynamic blood-brain barrier. FEBS J. 2015, 282, 4067–4079. [Google Scholar] [CrossRef]
- Koval, M. Claudins—Key pieces in the tight junction puzzle. Cell Commun. Adhes. 2006, 13, 127–138. [Google Scholar] [CrossRef]
- Krause, G.; Winkler, L.; Mueller, S.L.; Haseloff, R.F.; Piontek, J.; Blasig, I.E. Structure and function of claudins. Biochim. Biophys. Acta 2008, 1778, 631–645. [Google Scholar] [CrossRef] [Green Version]
- Angelow, S.; Ahlstrom, R.; Yu, A.S. Biology of claudins. Am. J. Physiol. Ren. Physiol. 2008, 295, F867–F876. [Google Scholar] [CrossRef]
- Wen, H.; Watry, D.D.; Marcondes, M.C.; Fox, H.S. Selective decrease in paracellular conductance of tight junctions: Role of the first extracellular domain of claudin-5. Mol. Cell Biol. 2004, 24, 8408–8417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marra, A.; Vargas, M.; Striano, P.; Del Guercio, L.; Buonanno, P.; Servillo, G. Posterior reversible encephalopathy syndrome: The endothelial hypotheses. Med. Hypotheses. 2014, 82, 619–622. [Google Scholar] [CrossRef] [PubMed]
- Clayton, A.M.; Shao, Q.; Paauw, N.D.; Giambrone, A.B.; Granger, J.P.; Warrington, J.P. Postpartum increases in cerebral edema and inflammation in response to placental ischemia during pregnancy. Brain Behav. Immun. 2018, 70, 376–389. [Google Scholar] [CrossRef]
- Warrington, J.P.; Fan, F.; Murphy, S.R.; Roman, R.J.; Drummond, H.A.; Granger, J.P.; Ryan, M.J. Placental ischemia in pregnant rats impairs cerebral blood flow autoregulation and increases blood-brain barrier permeability. Physiol. Rep. 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- Nelander, M.; Hannsberger, D.; Sundström-Poromaa, I.; Bergman, L.; Weis, J.; Åkerud, H.; Wikström, J.; Wikström, A.-K. Assessment of cerebral perfusion and edema in preeclampsia with intravoxel incoherent motion MRI. AOGS 2018. [Google Scholar] [CrossRef] [Green Version]
- Nelander, M.; Wikström, A.-K.; Weis, J.; Bergman, L.; Larsson, A.; Sundström-Poromaa, I.; Wikström, J. Cerebral Osmolytes and Plasma Osmolality in Pregnancy and Preeclampsia: A Proton Magnetic Resonance Spectroscopy Study. Am. J. Hypertens. 2018, 31, 847–853. [Google Scholar] [CrossRef]
- Hatherell, K.; Couraud, P.O.; Romero, I.A.; Weksler, B.; Pilkington, G.J. Development of a three-dimensional, all-human in vitro model of the blood-brain barrier using mono-, co-, and tri-cultivation Transwell models. J. Neurosci. Methods 2011, 199, 223–229. [Google Scholar] [CrossRef]
- Cucullo, L.; Couraud, P.O.; Weksler, B.; Romero, I.A.; Hossain, M.; Rapp, E.; Janigro, D. Immortalized human brain endothelial cells and flow-based vascular modeling: A marriage of convenience for rational neurovascular studies. J. Cereb. Blood Flow Metab. 2008, 28, 312–328. [Google Scholar] [CrossRef] [Green Version]
- Vigh, J.P.; Kincses, A.; Ozgür, B.; Walter, F.R.; Santa-Maria, A.R.; Valkai, S.; Vastag, M.; Neuhaus, W.; Brodin, B.; Dér, A. Transendothelial Electrical Resistance Measurement across the Blood–Brain Barrier: A Critical Review of Methods. Micromachines 2021, 12, 685. [Google Scholar] [CrossRef]
- Escudero, C.; Bertoglia, P.; Hernadez, M.; Celis, C.; Gonzalez, M.; Aguayo, C.; Acurio, J. Impaired A2A adenosine receptor/nitric oxide/VEGF signaling pathway in fetal endothelium during late- and early-onset preeclampsia. Purinergic Signal. 2013, 9, 215–226. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Preeclampsia (n = 28) | Normal Pregnancy (n = 28) | Non-Pregnant (n = 16) | p-Values |
|---|---|---|---|---|
| Maternal age (years) | 28 (25–32) | 33 (29–35) | 27 (24–36) | n.s. |
| Nulliparous | 23 (82%) | 10 (36%) | 9 (56%) | <0.001 |
| BMI | 26 (23–29) | 24 (22–26) | 22 (20–25) | <0.001 |
| At inclusion | ||||
| Gestational week | 35 (29–37) | 35 (27–38) | n.s. | |
| Blood pressure (mmHg) | ||||
| Systolic | 150 (140–160) | 110 (110–120) | 110 (110–118) | <0.001 |
| Diastolic | 98 (86–100) | 70 (60–75) | 70 (65–70) | <0.001 |
| MAP | 113 (107–120) | 83 (77–90) | 83 (80–86) | <0.001 |
| Neurological symptoms (yes) | ||||
| Headache | 18 (64%) | 4 (14%) | 3 (19%) | <0.001 |
| Severe headache (VAS ≥ 5) | 10 (36%) | 0 | 0 | <0.001 |
| Visual disturbances | 10 (36%) | 0 | 0 | <0.001 |
| Headache & visual disturbances | 10 (36%) | 0 | 0 | <0.001 |
| Any neurological symptom | 20 (71%) | 4 (14%) | 3 (19%) | <0.001 |
| TEER (Ωcm2) | ||||
| Baseline value | 34.9(29.7–38.8) | 33.7 (29.7–42.6) | 29.2 (25.4–38.8) | n.s. |
| After plasma exposure | 22.9 (18.1–27.5) | 27.1 (18.8–35.5) | 23.8 (21.6–29.3) | n.s. |
| Δ-TEER | 11.9 (8.5–14.8) | 7.6 (3.7–11.9) | 5.8 (2.0–8.0) | <0.001 |
| Clinical Characteristics | Preeclampsia (n = 28) |
|---|---|
| Gestational week at preeclampsia diagnosis | 35 (22–41) |
| Severe preeclampsia at inclusion, n | 10 (36%) |
| Blood pressure medication at inclusion, n | 22 (79%) |
| Magnesium treatment, n | 0 (0%) |
| Gestational week at delivery | 35 (25–41) |
| Severe preeclampsia at delivery, n | 16 (57%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friis, T.; Wikström, A.-K.; Acurio, J.; León, J.; Zetterberg, H.; Blennow, K.; Nelander, M.; Åkerud, H.; Kaihola, H.; Cluver, C.; et al. Cerebral Biomarkers and Blood-Brain Barrier Integrity in Preeclampsia. Cells 2022, 11, 789. https://doi.org/10.3390/cells11050789
Friis T, Wikström A-K, Acurio J, León J, Zetterberg H, Blennow K, Nelander M, Åkerud H, Kaihola H, Cluver C, et al. Cerebral Biomarkers and Blood-Brain Barrier Integrity in Preeclampsia. Cells. 2022; 11(5):789. https://doi.org/10.3390/cells11050789
Chicago/Turabian StyleFriis, Therese, Anna-Karin Wikström, Jesenia Acurio, José León, Henrik Zetterberg, Kaj Blennow, Maria Nelander, Helena Åkerud, Helena Kaihola, Catherine Cluver, and et al. 2022. "Cerebral Biomarkers and Blood-Brain Barrier Integrity in Preeclampsia" Cells 11, no. 5: 789. https://doi.org/10.3390/cells11050789
APA StyleFriis, T., Wikström, A.-K., Acurio, J., León, J., Zetterberg, H., Blennow, K., Nelander, M., Åkerud, H., Kaihola, H., Cluver, C., Troncoso, F., Torres-Vergara, P., Escudero, C., & Bergman, L. (2022). Cerebral Biomarkers and Blood-Brain Barrier Integrity in Preeclampsia. Cells, 11(5), 789. https://doi.org/10.3390/cells11050789